BONE TUMOURS - I & II - 2015.pptx

of 113
-
Upload
nur-atiqah-mohd-azli -
Category
Documents
-
view
224 -
download
0
Transcript of BONE TUMOURS - I & II - 2015.pptx
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
1/113
BONETUMOURSPROFESSOR.NYAN HTAIN
LINN
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
2/113
Learning outcomes
At the end of the lecture the studentmust !e a!le to" E#$lain the $athogenesis of !one tumors and
tumor%li&e conditions.
'lassif( ma)or $rimar( tumors in*ol*ing!ones.
+escri!e the mor$holog( of !one tumors.
+escri!e the clinical course and distinctradiological features of !one tumors.
+iscuss the diagnosis and management !onetumors.
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
3/113
Parts of a long bone
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
4/113
BONE TUMOURS
Gross and morphologic appearances diverse.
Natural history varies from innocuous to rapidly fatal.
Classification mostly according to the normal cell or
tissue type they recapiculate.
Benign tumours greatly out number their malignant
counterparts and greatest frequency
in the first decade of life.Specific typesof tumours target certain age groups
and anatomic sites.
Location provides important diagnostic information.
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
5/113
CLASSIFICATION OF BONETUMORS
Cartilage tumorsOsteocon!roma Con!romas Enchondroma
Periosteal chondroma Con!roblastoma Con!rom"#oi! $broma Con!rosarcoma +edi,erentiated
-esench(mal
'lear cell
Periosteal
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
6/113
Osteogenic tumors
Osteoi! osteoma Osteoblastoma Osteosarcoma
'on*entional Teleangiectatic
Small cell
Lo grade central
Secondar( Parosteal
Periosteal
High grade surface
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
7/113
Fibrogenic tumors Non%ossif"ing $broma Fibrous cortical !efect
Fibrosarcoma
Primiti&e Neuroecto!ermalTumor E'ing sarcoma
(iant Cell Tumor (iant cell tumor Malignant (iant cell tumor
Miscellaneous lesions
Aneur"smal bone c"st Fibrous !"s)lasia
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
8/113
on!ar" bone neo)lasia is associated ith "
!one infarctschronic osteom(elitis
Pagets diseaseradiation
metal $rostheses
ndary neoplasms account for only a small fra
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
9/113
CLINICAL FEATURES
)resentation &aries /benign lesions /0 fre1uentl(
as(mtomatic. incidental2nding. many /0%$roduce $ain. %slo groing mass. %
sudden $athologicfracture.
-limitation of mo*ement.
-general s(m$toms fe*er e#hausioneight% loss etc.
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
10/113
BONE FORMIN( TUMOURS
$roduction ofbone!( the neo$lastic cells tumour !one usuall( de$osited as 'o&en
trabeculae *aria!l( minerali*e!
OSTEOMAS !osselated round to o*al sessile.
$ro)ect from sub)eriosteal surface ofcorte#+
most often arise on or insides,ulland
facial bones+
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
11/113
multiple osteomas are seen in Gardnerssyndrome+
generall( slo' gro'ing tumours of littleclinicalsigni2cance.
the( consist of a com$osite of 'o&enand
lamellar !one fre1uentl( de$osited in cortical$attern.some *ariants contain a com$onent of
tra!ecular !one.
COMPLICATIONS . o!struction of a sinus ca*it(.
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
12/113
OSTEOMA OF T/E S0ULL
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
13/113
OSTEOMA
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
14/113
OSTEOI1 OSTEOMA
benign!one tumour. less than2cm in greatest diameter. usuall( occur in teensand 23s3456 7
25"rs4 men " omen 5 2.8 can arise in any bone. )re!election/ a$$endicular s&eleton. $osterior elements of
s$ine. 536 of cases% femur orti!ia.
commonl( arise in corte#.
less fre1uentl( arise ithin medullar(
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
15/113
Painis caused !( e#cessprostaglandin E2$roduced
!( $roliferating osteo!lasts.
MORP/OLO(:(ross
ell circumscri!ed round to o*al masses ofgritt( tan tissue.Microsco)iccom$osed of randoml( interconnecting
tra!eculae of 'o&en bone $redominentl(rimmed !( osteoblasts+surrounded !( loose connecti*e tissue
stroma
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
16/113
uall( elicit a tremendous amount of reacti*ene formation that encircles the lesion.
1IO(RAP/ICALL:/ tumor manifests as smaln! lucenc" that ma( !e centrall" minerali*e!
i!us41uentl( treated !(ra!ioablation+
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
17/113
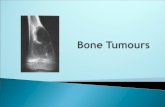
Osteoi!osteoma
shoing randoml(oriented tra!eculae ofo*en !one rimmed
!( $rominentosteo!lasts.
The intertra!ecular
s$aces are 2lled !(*ascular looseconnecti*e tissue.
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
18/113
OSTEOI1 OSTEOMA
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
19/113
OSTEOBLASTOMA benign!one tumour si*e% larger than 2cm. in*ol*es the spinemore fre1uentl(.
CL9F/ dull aching $ain not res$onsi*e tosalic(lates.
/ISTOLO(IC FEATURES / identical to osteoidosteoma !ut usuall( does notinduce
mar&ed !on(reaction.
T9M% usuall( curetted or e#cised en!loc in aconser*ati*e fashion.
$ossi!ilit( of malignant change / remote
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
20/113
OSTEOBLASTOMA
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
21/113
OSTEOSARCOMA
malignant mesench(mal tumor inhich thecancerous cells produce bone
matrix.
6most common $rimar( malignant tumorof
!one.3
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
22/113
SITE % usuall( arise in the meta)"sealregion of
long bones of e#tremities.
almost 536 occur about te ,nee an" bone can !e in*ol*ed. in $ersons 0 25"rs/ incidence in 8at!ones
and long !ones is almost e1ual.
PAT/O(ENESIS
!asic mechanisms that cause thede*elo$ment of osteosarcoma are still un&non.a$$ro#imatel( 436 ha*e ac1uired genetic
a!nor%
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
23/113
tinoblastoma gene ?RB (ENE!" (ENE
defects in rband )5< $la( im$ortant roles.
!normalities inIN9:A hich encodes$;< 3 a cell(cle regulator4 and$;:3hich aids and a!ets $=>unction4are also seen in osteosarcoma.
steosarcomas tend to occur at sites of bone
rowth !ecause $roliferation ma&es osteo!las%c cells $rone to ac1uire mutations that couldad to malignant transformation.
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
24/113
Maor sites of origins of Osteosarcomas
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
25/113
MORP/OLO(:SUBT:PESare grouped according to"@SITE OF ORIGIN 3intramedullar( intracorticalor
surface4@DEGREE OF DIFFERENTIATION.@MUTIENTRIIT!3s(nchronous metachronous4@"RIMAR!3 underl(ing !one is unremar&a!le4 or SEONDAR! to $ree#isting disorders such as!enign tumours $aget disease !one infarcts
$re*ious radiation.@HISTOLO?I' FEAT@RES 3osteo!lasticchondro!lastic
2!ro!lastic telangiectatic small cell and
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
26/113
(ROSSL: big b#l$y tumors. gritty% gray white% often contain areas of
haemorrhage and &ysti& 'egeneration. fre1uentl( destro(s surrounding cortices and $roduce soft tiss#e masses. s(rea' e)tensi*ely in the me'#llary &anal
in2l% trating and re$lacing the marrosurrounding
the $ree#isting !one tra!eculae. infre1uentl( (enetrate e(i(hyseal (late orenter
the +oint.
gros into it along tendoligamentous
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
27/113
/ISTOLO(: tumour cells *ar( in si7e and sha$e. fre1uentl( ha*e large h($erchromatic
nuclei. !i77are tumor giant cells and mitosesarecommon.
t#e formation of bone by t#e tumorcells isc#aracteristic.
neo$lastic !one / usuall( coarse lace%li&e
archi% tecture. %ma( also !e !roadsheets or
$rimiti*e tra!eculae.
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
28/113
&ascular in&asion /% usuall( cons$icious.
necrosis% % ma( !e $resent in536 to >36of indi*idual
tumour.
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
29/113
Osteosarcoma+ A--ass in*ol*ing the
u$$er end of the ti!ia.
The tan%hite tumor 2llsmost of the medullar(
ca*it( of the meta$h(sisand $ro#imal dia$h(sis.
It has in2ltrated throughthe corte# lifted the
$eriosteum and formedsoft tissue masses on!oth sides of the !one
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
30/113
B-/istologica))earance-
ith coarse laceli&e
$attern of neo$lastic!one 3arrow4 $roduced !(ana$lastic tumor cells.
Note the ildl( a!errantmitotic 2gures3arrowhea's,
CLINICAL COURSE
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
31/113
CLINICAL COURSEt")ical )resentation / $ainful$rogressi*el( en%
largingmasses.sudden fractureof the !one% 3sometimes isthe
2rst s(m$tom4.
RA1IOLO(:large destructi&e mixed lytic andblastic mass 'it#
inltrati&e margins.the tumor !rea&s through the corte# and liftsthe $eriosteum resulting in reacti*e $eriosteal!one
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
32/113
OSTEOSARCOMA
a tumor -T,in thefemoral dia$h(sisith a Co!mantriangle
Co!man triangle &hara&teristi& b#t
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
33/113
Co!man triangle / &hara&teristi&% b#tnot
'iagnosti& of this
t#mor.SPREA1%mainl( aematogenousat the time of diagnosis 836 to 236ha*e
(#lmonarymetastases.in those ho die of this neo$lasm 36ha*e metastases to l#ngs% bones%
brain etc.
TREATMENT/ m#ltimo'ality a$$roach
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
34/113
CARTILA(E ? FORMIN( TUMOU
tilage tumors account for the ma)orit(ofr( !one tumors and are c#aracteried byormation of #yaline or myxoid cartilage.
igncartilage tumors are much more common
malignant ones.
OSTEOC/ON1ROMA
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
35/113
OSTEOC/ON1ROMA Benigncartilage *capped tumor that
is attached
to the underl(ing s&eleton !( a bonystalk. %also &non as E+,S-,SS
%most common benign bone tumora!out 56 are solitary./0-E ERE3-4R5 E+,S-,SSS563R,/E
autosomal dominant hereditar( disease.caused !( germline loss%of%functionmutations in either the ext1 or ext2genes+
inacti*ation of onl(ext1 has !een
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
36/113
E% SOLITARY% usuall( 2rst diagnosed in latea'oles&en&e an' early a'#lthoo'.
-@LTIPLE3hereditar(4% !ecome a$$arentduring &hil'hoo'.
% men # >0 omen.E% de*elo$ onl( in !ones ofendochondral
origin and arise from the meta(hysis near the growth (late of long t#b#lar bones es$eciall( a!out the &nee. OASIONA!/ !ones of sca$ula $el*isand ri!s.% in these sites% sessile short stal&s. RARE! / short tu!ular !ones of the hands and feet.
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
37/113
RP/OLO(:ssile or musroomsa)e!+
% range from 8 to 23cm+
nign "aline cartilage ca) *ar(ing in thic&ness.
$ is co*ered $eri$herall( !( )ericon!rium+
corte# of the stal& merges ith the corte# ofe host !one so that medullar( ca*it( of theteochondroma and !one are in continuit(.
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
38/113
OSTEOC/ON1ROMA
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
39/113
OSTEOC/ON1ROMA
CLINICAL FEATURES
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
40/113
CLINICAL FEATURES $resent as slo groing masses. $ainful if im$inge on a ner*e or if the stal&
isfractured.
man( cases% incidental 2nding.
hereditar( e#ostosis / underl(ing !ones ma(!e!oed and shortened.
osteochondromas sto$$ed groingat timeof
groth $late closure.
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
41/113
C/ON1ROMAS
Benign tumors of #yaline cartilage t#atusually
occurs in bones of enc#ondral origin.
if arise ithin the me!ullar" ca&it" / &nonas
E67,63R,/4S+
if arise on the surface of bone% &non as S0B8ER,S-E4 or90+-47,R-747,63R,/4S
3i i ll i 23 3 3 4
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
42/113
3iagnosis/ usuall( in 23sto 3s+ 3(ears4.resentith solitar( meta$h(seal lesions oftu!ular !ones.
fa*ored sites% short tu!ular !ones of hands and feet.S(ndrome of multi)le encon!romas or
encon!romatosis is &non asOLLIER1ISEASE
Encon!romatosis associate! 'it soft%tissue
aemangiomas is called MAFFUCCIS:N1ROME
MORP/OLO(:% /
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
43/113
/ISTOLO(:/ com$osed of ell%circumscri!ednodulesof c(tologicall( !enign h(alinecartilage. Peri$heral $ortions of nodules ma(
undergo enchondral ossi2cation and centercan
calcif( and die.In Ollier disease and -a,ucci s(ndrome /chondromas are more cellular and e#hi!itc(tologic at($ia.
CLINICAL FEATURES-ost enchondromas are as(mtomatic andare detected incidentall(.Occasionall( $ainful.
Encon!romatosis / tumors ma( !e numerous
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
44/113
Encon!romatosis tumors ma( !e numerousand large $roducing se*ere deformities.
RA1IO(RAP/:
@nminerali7ed nodules of cartilage $roduce ell% circumscri!ed o*al lucencies that are
surrounded !( a thin rim of radiodense !one. ;7 or , ring signif matri# calci2es / irregular o$acities de*elo$.tumor nodules scallo$ the endosteum !ut
lea*e the corte# intact.
TREATMENT%+O /clinical situation. usuall( o!ser*ationor curettageencon!romatosis% Ris& of malignant
change.
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
45/113
AFFUCCI S:N1ROME / ris& of de*elo$ing othermalignancies including o*arian &ar&inomas
and brain gliomas.
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
46/113
ENC/ON1ROMA
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
47/113
C/ON1ROMA
C/ON1ROBLASTOMA
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
48/113
C/ON1ROBLASTOMA rare benign tumorC 7 86 of $rimar( !onetumors
A(E / usuall( (oung $atient in their teens SE % male" female 5 2.8 SITE % most / a!out the$nee.
in older $atients /(el*is an' ribs.
stri&ing $redelection for epip#ysesandapop#yses.
MORP/OLO(: com$osed of sheetsof com$act $ol(hedralchon% dro!lasts that ha*e ell%de2ned c(to$lasmic
!orders moderate amounts of $in& c(to$lasm
and nucleithat are h($erlo!ulatedith longi%
mour cells are surrounded !( scant #yaline
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
49/113
mour cells are surrounded !( scant #yalinetrix- de$osited in a lace%li&e con2guration.
hen matri# calci2es it $roduces a character%
ticc#icken8'ire$attern of minerali7ation.attered non%neo$lastic osteoclast8type giantells$resent.ccasionall( undergo haemorrhagic c(stic
egeneration.
INICAL FEATURES
suall( $ainful.int e,usions.stricted )oint mo!ilit(.
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
50/113
A1IO(RAP/:
ell%de2nedgeogra$hic lucenc( that commonl(has s$ott( calci2cations.
ecurrences/ not uncommon after curettage
arel(% $ulmonar(3 haemotogenous4metastases occur.
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
51/113
C/ON1ROBLASTOMA
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
52/113
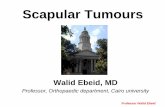
Con!roblast
oma+ There is alarge destructi*ecalci2ed lesion ofthe $ro#imalhumeral e$i$h(sis
C/ON1ROM:OI1 FIBROMA
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
53/113
C/ON1ROM:OI1 FIBROMArarestof cartilage tumors.can !e mista&en for sarcoma.
A(E % teensand 23s+ male$re$onderance.SITE% can in*ol*e an( !one of the !od(C most fre1entl( arise in the meta(hysisof
long t#b#lar bones.
(ROSS
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
54/113
" C $ $aremost cellular.in cartilaginous regions / tumor cells aresituated in lacunaeCin m"#oi! areas / cells are stellate.*ar(ing degrees of c(tologic at($ia.
small foci of calci2cation.scattered non%neo$lastic osteoclast%t($egiant cells.
CLINICAL FEATURES / lo&ali/e' '#ll a&hy(ain.RA1IO(RAP/:/ eccentric geogra$hicl#&en&ythatis ell delineated from the ad)acent !one !(
a
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
55/113
EATMENTof choice / sim)le curettage+ The( ma( recur !ut no threat for malignant
tranformation or metastasis.
C/ON1ROM:OI1 FIBROMA
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
56/113
C/ON1ROM:OI1 FIBROMA
C/ON1ROSARCOMA
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
57/113
C/ON1ROSARCOMA?rou$ of tumors that s$an a !road s$ectrumof
clinical and $athologic 2ndings.'ommon feature to all is% production of neoplastic cartilageS@B'LASSIFIE+according to"%SITE % central 3intramedullar(4
perip#eral3)u#tacortical andsurface4
HISTOLO?Y/ con&entional3h(aline andorm(#oid4 0clear cell
%dedi%erentiated
the second most common malignant matri#
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
58/113
the second most common malignant matri# $roducing tumor of !one. A(E% clear cell and mesench(mal *ariants"%
occur in teensor 23s others / usuall( 3sor older.% male #20 female)856 of con*entional 3$eri$heral4chondro%
sarcomas arise from a $ree#isting enchondroma or osteochondroma
SITE/ commonl( arise in the central)ortions of te s,eleton including(el*issho#l'er and ribs.
The clear cell &ariant originates in
MORP/OLO(:
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
59/113
MORP/OLO(:
(ROSS/ large bulky tumors: made up ofnodules of gray8'#ite translucentglistening tissue.
in m"#oi! &ariants the tumors are *iscousand gelatinousand the matri# oo7es from the cut
surface.s$ott( calci2cations% t($icall( $resent.central necrosiscreate c(stic s$aces.ad)acent corte#is thic&ened or eroded.
tumor gros ith !road $ushing fronts into
MICROSCOPICALL: ?
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
60/113
C OSCO CCONGENTIONAL(RA1E 8 ;LOH (RA1E / mild
h($ercellularit(.'hondroc(tes / $lum$ *esicular nuclei ithsmall nucleoli.
Binucleate cells / s$arseC mitotic 2gures% fePortions of matri# fre1uentl( minerali7eC'artilage ma( undergo endochondralossi2cation.
(RA1E < % mar&ed h($ercellularit(D e#treme $leomor$hism ith!i77arre
tumor giant cells and mitoses.
CLEAR CELL C/ON1ROSARCOMA%
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
61/113
CLEAR CELL C/ON1ROSARCOMAsheets of largemalignant chondroc(tes ith abundant clear
cytoplasm numerous osteoclast8type giantcellsand intralesional reacti&e bone formation.
MESENC/:MAL C/ON1ROSARCOMA /islands of 'ell8di%erentiated #yaline cartilagesurrounded !(sheets of small round cells.
CLINICAL FEATURES / $ainful $rogressi*el(enlarging masses.RA1IOLO(:/ $rominent endosteal scallo$ing.
foci of 8occulent densities 3calci2cations4
PRO(NOSIS
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
62/113
PRO(NOSIS ?-(RA1E9$&e "ear sur&i&al / gra!e 85 36- gra!e 25 86- gra!e E7-Sel( common.
in 56G >BR,/4S / !e&elo)e! from
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
69/113
,SS>56G >BR,/4S !e&elo)e! fromal !efectsthat gro to 5 or >cm in si7e.re usuall( not detected until adolescence.
P/OLO(:consist of gra( to (ello%!ron cellular
ns containing $broblastsand macro)agestioc(tes4.blastsare fre1uentl( arranged in a
iform 3$inheel4 $attern.
oc(tes are either multinucleated giant cellslusters of foam( macro$hages.
RA1IOLO(ICALL:/ $roduce elongated
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
70/113
shar$l(demarcated radiolucenciesthat are
surrounded!( a thin rim of sclerosis.
CLINICAL FEATURES>BR,0S 7,R-74 3E>E7-S /
as"mtomatic usuall(detected radiologicall( as inci!ental2nding.
-ost / limited groth $otentialand undergos)ontaneous resolution ithin se*eral
(ears
to !e re$laced !( normal cortical !one.
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
71/113
Fibrous cortical!efect=
Nonossif"ing$broma.
7#aracteristic
storiform pattern ofspindle cellsinterspersed 'it#scatteredosteoclast8typegiant cells.
NON OSSIF:IN( FIBROMA
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
72/113
NON%OSSIF:IN( FIBROMA
FIBROUS 1:SPLASIA
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
73/113
FIBROUS 1:SPLASIA Benign tumor li&ened to a localied
de&elopmental arrest
All the components of normal bone are$resent !ut the( do not di%erentiate into theirmature structures.Lesions arise during s&eletal groth andde*elo$ment.
T/REE CLINICAL PATTERNS"%
;8 monostotic"% in*ol*ement of single!one. ;2 )ol"ostotic "% in*ol*ement of multi$le!ones
;
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
74/113
geneduring em!r(ogenesis.
MONOSTOTIC FIBROUS1:SPLASIA436 of all cases.occurse1uall( in !o(s and girls.usuallyin earl( adolescence and often sto$s enlarging at time of groth $late closure.
femur ti!ia ri!s )a !ones cal*aria andhumerus are most commonly a,ected.fre@uentlyas(m$tomatic and usuall(
disco*ered
can cause mar&ed enlargement and distortionf !
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
75/113
of !one.craniofacial s,eleton in&ol&ementse*ere
dis2gurementcan occur.monostotic dAs does not e&ol&e intopolyostotic dAs.
POL:OSTOTIC FIBROUS 1:SPLASIAHIT/OUTEN1OCRINE 1:SFUNCTION246 of all casesmanifests at a slightl( earlier age than the monostotic t($e.femur s&ull ti!ia humerus ri!s 2!ula
radius
craniofacial in&ol&ement / $resent in 536to8336
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
76/113
to8336+se*ere sometimes cri$$ling deformities3she$herd%croo& deformit( of $ro#imal femur4
and s$ontaneousand often recurrentfractures.
POL:OSTOTIC FIBROUS 1:SPLASIA
HIT/ CAFJ%AU%LAIT S0IN PI(MENTATION AN1EN1OCRINOPAT/IES
&non as /ccune84lbrig#t syndrome.account for
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
77/113
usuall( limited to same side of !od(.Dclassicall( large.dar& to caf%au%lait.ha*e irregular ser$iginous !orders. 3 coastline of maine4found $rimaril( on the nec& chest !ac&
shoulder and $el*ic region.
MORP/OLO(:ell circumscri!ed intramedullar(.*ar( greatl( insi7e larger lesions e#$and and
distort the !one.
tan%hitein color and gritt(.
MICROSCOPICcom$osed of cur*ilinear tra!eculae of o*en
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
78/113
com$osed of cur*ilinear tra!eculae of o*en !one surrounded !( a moderatel( cellular
2!ro% !lastic $roliferation. sha$es of tra!eculaemimicchinese letters.
the !one lac&s $rominent osteo!lasticrimming.nodules of h(aline cartilage ith a$$earanceof
disorgani7ed groth $late are also $resent+;236c(stic degeneration haemorrhage andfoam(
macro ha es are common.
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
79/113
%RA1IOLO(:
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
80/113
RA1IOLO(:T($ical ground%glass a$$earance and ell%de2ned margins.
$ol(ostotic disease is fre1uentl( associatedith $rogressi*e disease.
%SEGERE S0ELETAL COMPLICATIONS /recurring fractures long%!one deformities$ersistent $ain
distortion of craniofacial !ones.
%MALI(NANT TRANSFORMATION / rarecom$lication
usuall( from $ol(ostotic disease.
Fibrous
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
81/113
Fibrous!"s)lasia+
'ur*ed tra!eculae ofo*en !one arising in
a 2!rous tissue.
Note the a!sence ofosteo!lasts rimming
the !ones.
FIBROUS 1:SPLASIA
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
82/113
FIBROUS 1:SPLASIA
FIBROUS 1:SPLASIA
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
83/113
FIBROUS 1:SPLASIA
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
84/113
The u$$er left leg ith
t($ical osseous changesconsistent ith $brous!"s)lasia and se)er!Kscroo, !eformit"
FIBROSARCOMA GARIANTS
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
85/113
ma( occur at an( age.mostl( middle%ageand elderl(.
nearl( e1ual se# distri!ution.usuall( arise de no*o !ut fe de*elo$ in $re%e#isting !enign tumors !one infarcts Pagetic!one and irradiated tissue.
MORP/OLO(:(ROSSL:% large haemorrhagic tan%hitemasses that destro(the underl(ing!one and
fre1uentl( e#tendsinto soft tissues.MICROSCOPIC% c(tologicall( malignant2!ro!lastsarranged in a herring!one storiform $attern.
FIBROSARCOMA-alignant s$indl( neo$lastic cells forming
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
86/113
-alignant s$indl( neo$lastic cells forming/ERRIN(%BONE- STORIFORM$attern.
ICAL FEATURES ?
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
87/113
rging $ainful mass.ll( arises in meta$h(sis of long !ones and
ic 8at !ones.ologic fracture is a fre1uent com$lication.
IO(RAP/: ? it is(ermeati*eandlyti&and oftdsinto the ad)acent soft tissue.
(NOSIS ?en!son / si/e lo&ation stage and gra'e of tumor.
MISCELLANEOUS TUMORSEHIN( SARCOMA9PRIMITIGE
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
88/113
EHIN( SARCOMA9PRIMITIGENEUROECTO1ERMAL
TUMOR ;PNET$rimar( malignant small round8celltumors
of !one and soft tissue.share an identical chromosome translocation.to *ariants of the same tumor that di,er onl( in their degree of neural di,erentiation.
PNETs/ demonstrate neuraldi%erentiation.
EHIN( SARCOMA / undi%erentiated.
cond most common !one sarcomas in children.ungest a*erage age at $resentation%
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
89/113
ungest a*erage age at $resentation%ost/ 83 to85"rs old- 36% (ounger than 23(rs
(s slightl(0 girlsi&ing $redilection for hitesC !lac&s are rarel( aist ha*e atranslocation in*ol*ing theSgeneon C/ROMOSOME 22 and a gene
co!ing an ETS famil" transcri)tion factor=ost common E-S geneis>11.
RP/OLO(:ft tan%hite and fre1uentl( contains areas of
morrhageand necrosis.risesin the medullar( ca*it(C usuall( in&a!estherte) (erioste#mand soft tiss#e.
ROSCOPICALL:/ com$osed of sheets of unifol ro#n' &ells slightl( larger than
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
90/113
l ro#n' &ells slightl( larger thanhoc(tes. ith scant( clear c(to$lasm 3due to
gen4ER%HRI(/T rosettes3t#mor &ells arrange' in at a &entral 1brillary s(a&e4 is indicati*e of neuralrentiation.
or contains little stroma.rosis ma( !e $rominent.ti*el( fe mitotic 2gures.
ICAL FEATURESall( arise in dia$h(sisof long tu!ular !oneseciall( femurand 8at !ones of $el*is.ent as $ainful enlarging masses.
cted site is tender arm and sollen
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
91/113
cted site is tender arm and sollen.temic $n!ings / fe*er ele*ated ESR anaemia&oc(tosis ma( !e $resent.
1IO(RAP/:% destructi*e l(tic tumor $ermeati*e margins
e#tension into surrounding soft tisiosteal reaction $roduces la(ers of reacti*ene in onion8skinfashion.
ATMENT/ chemothera$h( surgical e#cision ith or ithout irradiation.
(NOSIS/ a$$ro#imatel( 456 . 5%"rsur*i*alC at least 536 ha*e long%term cures.
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
92/113
E'ing
sarcoma+
Sheets of small roundcells ith scant clearedc(to$lasm.
EHIN( SARCOMA
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
93/113
EHIN( SARCOMA
EHIN( SARCOMA
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
94/113
EHIN( SARCOMA
(IANT%CELL TUMOR
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
95/113
containsa mi#ture of mononuclear cells and a$rofusion of multinucleated osteoclast%t($e
giant cells. s(non(m / osteoclastomarelati*el( uncommon.benign !ut locall" aggressi&e neo$lasm.age/ 23"rs to 3"rs+the mononuclear cells in the tumor e#$ress
R46C.3 Re&e(tor a&ti*ator of n#&lear fa&tor$a((a02 ligan'
also $nown as osteo&last 'i3erentiationfa&tor,
MORP/OLO(:(ROSS% large red%!ron tumors that fre1uentl(
undergo c(stic degeneration.MICROSCOPIC% com$osed mostl( of uniform o*al
mononuclear cells that
scatteredithin this !ac&ground are numerous osteoclast%t($e giant cells ha*ing833 or more
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
96/113
nuclei that resem!le those of the mononuclear cells.
necrosis haemorrhage haemosiderinde$osition and reacti*e !one formation are common.
CLINICAL FEATURESA1ULTS % in*ol*e !oth thee$i$h(ses and themeta$h(ses.
A1OLESCENTS% con2ned $ro#imall( !( thegroth $late and are limited tometa$h(sisMAORIT:% arise around the &nee3 distal femurand
$ro#imal ti!ia4.
fre1uentl( causes arthritis%li&e s(m$toms.
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
97/113
1 ( ( $occasionall( / $athologic fractures.most are solitar(C
multi$lemulticentric tumors occur es$eciall( in the e#tremities.often erode into su!chondral !one $lateC destro( o*erl(ing corte#C $roduce !ulging soft
tissue massdelineated !( a thin shell of reacti*e !one.
TREATMENT
curettage/ associated ith a 36 to >36recurrence rate.u$ to 6 metastasi7e to the lungs.
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
98/113
Benign giant%cell
tumor shoing a!undant
multinucleated giant cells
and a !ac&ground ofmononuclear cells.
(IANT CELL TUMOR OF BONE
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
99/113
ANEUR:SMAL BONE C:STA benign tumor of !one characteri7ed !( multi
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
100/113
A benign tumor of !one characteri7ed !( multi8 loculated blood8lled cystic spacesthat ma( $resent as a ra$idl( groing e#$ansile tumor. associated ith distincti*e 84)8 adeu!i1uitinating
en7(me.MORP/OLO(:(ROSS% multiple blood8lled cystic spacesseperated
by t#in$ tan8'#ite septa.Microsco)icall"Hallsare com$osed of $lum$ uniform 2!ro!lastsmultinucleated osteoclast%li&e giant cells and
reacti*e o*en !one.
a$$ro#imatel( one tir! of cases contain acartilage%li&e matri#called blue bone+
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
101/113
necrosis is uncommon.
CLINICAL FEATURESa,ects all age grou$s.generall( occurs during $rst 2 !eca!es of life.
no se# $redilection.
most fre1uentl( de*elo$s in meta$h(ses of long!onesand the $osterior elements of *erte!ral
!odies.most common s9s % )ainand s'elling+
&ertebral in&ol&ementcom$ress ner*es neurologic s(m$toms.
rel( $athologic fractures occur.
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
102/113
( $ g
1IO(RAP/:/ aneccentric e)(ansilelesion ithl% de2ned margins. -ost lesions are com$letel(cand contain a thin shell of reacti*e !one at$eri$her(andMRIma( demonstrate internal se$ta and
aracteristic 8uid le*els.
EATMENT% surgical C curettage or en !loc resection
currence rate is loContaneous regression ma( occur folloingcom$lete remo*al.
ANEUR:SMAL BONE C:ST
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
103/113
-@LTIPLE BLOO+%FILLE+ 'YSTI' SPA'ESSEPERATE+ BY THINFIBRO@S SEPTA
ANEUR:SMAL BONE C:ST
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
104/113
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
105/113
METASTATIC TUMORS
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
106/113
most common s&eletal malignanc(.usuall( occur in late stages of tumor.
PAT/HA:Sof s$read include" ;.3RE7- EGTENSION . 5/4-7OR 4E/4-,GE6,0S+ISSE-INATION >. 6-R4S64 SEE+LIN? 3*ia Batson$le#us of *eins4
INADUTS" more than 456 originate from"% cancers of prostate- breast- kidneyandlung.
IN 4IDREN" originate from"%
icall( multifocal 3e#ce$t&idne( and th(roidduce solitar( lesions4
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
107/113
duce solitar( lesions4.( occur in any boneCmostin*ol*e0 a)ial s$eleton-*ertebrall#mn% (el*is% ribs% s$#ll% stern#m,% (ro)imal
#raand h#mer#s in descending order.tastasis to small bones of han' an' feet areommonand usuall( from cancer of l#ng
eyand &olon.
IO(RAP/:%( !e $urel(L:TIC $urel( BLASTIC or MIE1
TIC AN1 BLASTIC.cinoma of kidney$ lung$ G.. tract$ malignantelanoma$ producelyticlesions+
prostatea!enocarcinoma%elicit scleroticres$onse.
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
108/113
res$onse.most oter metastases induce ami#e!l(ticand
!lastic reaction inl"ticlesions/ metastatic cells secrete
su!stances such as"prostaglandins-cytokines and-8relatedproteinthat stimulate osteoclastic !one resor$% tionC the tumor cells themsel*es do not directl( resor! !one.
l"tic bone tissue /0 rich in groth factors*i7. T(F%b- I(F%i- F(F- P1(F and bonemor)ogenetic
)roteins% hel$ create an en*ironment
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
109/113
Radiogra$h shosa dis$laced
fracture through anosteolytic lesionin the distal femurof a =>%(ear%old
oman ith lungcarcinoma
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
110/113
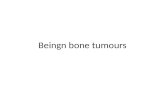
Pel*ic radiogra$h
shos ides$readosteoblastic$scleroticmetastases from
$rostate cancer
!NC!"ENCE O# BONE C$NCER
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
111/113
%&O bone sarcoma account for '()* of all
neoplasms. (2006)
!"#$ %&'"% appro*imately'(+ ne+ cases
per ,00-000 population and
year
%rgentina and ra/il higher incidence
'1% (34) (2005) &%1' , -() . /''0''' 7'&%1'1 2(' . /''0'''
O# $LL M$L!GN$NT 3R!M$R4 BONE TUMORS 1
osteosarcoma , 25* chondrosarcoma1 )5*
e+ing sarcoma /6*
fibrosarcoma , 5*
( S''" 8rogramme ,9:;
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
112/113
BONE C$NCER !N M$L$4S!$
N$T!ON$L C$NCER REG!STR4 7M$L$4S!$8C$NCER !NC!"ENCE !N M$L$4S!$ 7)''29)''58
M$LE 1 22' C$SES: /(/ . /''0'''
#EM$LE 1 )'' C$SES: '(5 . /''0'''
-
7/25/2019 BONE TUMOURS - I & II - 2015.pptx
113/113
THAN9 YO@