Bone Scan Pp

of 49
-
Upload
deti-paridlah -
Category
Documents
-
view
222 -
download
1
Transcript of Bone Scan Pp
-
7/31/2019 Bone Scan Pp
1/49
Nuclear Medicinein Musculoskeletal system
-
7/31/2019 Bone Scan Pp
2/49
-
7/31/2019 Bone Scan Pp
3/49
Introduction
Nuclear medicine is defined as a medical
speciality which uses the nuclear properties
of the matter to investigatephysiology andanatomy, diagnose diseases, and to treat
with unsealed sources of radionuclide
-
7/31/2019 Bone Scan Pp
4/49
Introduction
Characteristic:
Used Radiation from Nuclear desintegration
Physiologic process and change of function
from the organbiochemistric process in
celluler or moleculer levels.
Non-invasif, sensitivity >>>, specificity
-
7/31/2019 Bone Scan Pp
5/49
Introduction
A wide variety of musculoskeletal disorders can beinvestigated by nuclear medicine techniques,particularly through Bone scintigraphy/Bone Scan
The principal conditions that can be imaged are :
- metastatic bone disease- osteomyelitis
- variety of benign conditions (fractures,
avascular necrosis, inflammatories arthro-
pathies, metabolic bone disease, etc).
-
7/31/2019 Bone Scan Pp
6/49
Bone scan is commonly performed withTc99m-biphosphonates.
Bone scanning is performed with the
gamma camera.
Bone scan is more sensitive thanradiography in detecting skeletal disease.
-
7/31/2019 Bone Scan Pp
7/49
Pathophysiology of Biphosphonate Uptake
The bone scan provides information that reflectsskeletal metabolic activity.
The mechanism involved in biphosphonate uptakeis thought by chemiabsorption onto the calcium ofhidroxyapatite in bone, i.e. the biphosphonatemolecule is adsorbed onto the surface of bone.
The major factors which affect this adsorption :- osteoblastic activity
- skeletal vascularity.
-
7/31/2019 Bone Scan Pp
8/49
The bone scan therefore reflects the metabolic
reaction to a disease process.
Because its ability to detect functional
change, the bone scan can often be strongly
positive, well before the structural X-ray
changes occur.
-
7/31/2019 Bone Scan Pp
9/49
The Normal Bone Scan
The most important : symmetry.
There should be uniform uptake, greater activity atsites ofhighest metabolic activity (joint margins)& areas rich in trabecular bone (the spinal
vertebral bodies).
Biphosphonate not taken up by the skeleton isexcreted via the urinary tract tracer is
visualized in kidney & bladder.
Uptake of bone scanning agents can also occur insoft tissues significant abnormalities.
-
7/31/2019 Bone Scan Pp
10/49
-
7/31/2019 Bone Scan Pp
11/49
Three-Phase Bone Scan
Provide additional valuable info regardingthe vascularity of a lesion.
This involves :o Initial dynamic flow study (1st phase)
o A blood pool image (2nd phase)
o Delayed static images (3rd phase) can beobtained between 2 & 4 hours.
For the diagnosis ofosteomyelitis, thethree-phase bone scan is typically used.
-
7/31/2019 Bone Scan Pp
12/49
-
7/31/2019 Bone Scan Pp
13/49
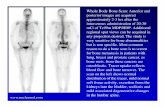
Bone Scan in Malignancy
The detection ofmetastatic skeletal diseaseremains the most important indication forperforming a bone scan.
The common cancers that metastasise to the boneare those of the prostate, breast & lung.
The most characteristic feature of metastases isirregular focal lesions in a pattern that does notcorrespond to any single anatomical structure.
-
7/31/2019 Bone Scan Pp
14/49
Bone Scan in Malignancy
In general, metastases must generate anosteoblastic response in order to be detectedon the bone scan.
Metastases can on occasion produce an areaof decreased uptake (cold lesion) reflectingbone destruction & failure to stimulate ahealing response. This is most often seen inmyeloma or renal carcinoma.
-
7/31/2019 Bone Scan Pp
15/49
-
7/31/2019 Bone Scan Pp
16/49
Important variant to recognise : Superscanof malignancyextensive focal lesions.
Therenal images are not visualizeddue to
less tracer is excreted via the renal tract.should be followed by more specific
investigation directed to the site of
abnormality.
-
7/31/2019 Bone Scan Pp
17/49
Bone Scanning In The Management ofMalignancy
For staging for a malignancy at presentation.
Metastases may be present in an asymptomatic
individual & even in patient with a suspectedmetastasis because of bone pain, moreextensive disease may be found when the bonescan is undertaken.
-
7/31/2019 Bone Scan Pp
18/49
Bone Scanning In The Management of Malignancy
The bone scan can be helpful in monitoringresponse to therapy. The use of the bonescan to assess the response to therapy is notalways straightforward.
Flare response : transient worsening of scanfindings in response to treatment in the firstfew months after therapy.
-
7/31/2019 Bone Scan Pp
19/49
Breast Cancer
An important part ofstaging in breast cancer patients.
In early breast cancer, the pick-up rate of metastases islow, about 3% in stage II. However, bone scan has a
useful role as a baseline study In more advances disease, at presentation the pick-up
rate of metastases is high ( 28%).
An abnormal bone scan carries a mean survival of 2-3
years, and is clearly of prognostic importance
-
7/31/2019 Bone Scan Pp
20/49
Prostate Cancer
Higher incidence of metastases (around 38% ) &increases in more advanced disease good case for
bone scan in all patients for staging.
Prostate-specific antigen (PSA) is used to detect
metastases. Although patients with an elevated PSA
should have bone scan.
It is common to find patients with normal PSA but
who have skeletal metastase.
-
7/31/2019 Bone Scan Pp
21/49
-
7/31/2019 Bone Scan Pp
22/49
Lung Cancer
Most patients with lung cancer have a poor
prognostic at presentation. The bone scanimportant in such patients where surgery is
considered to exclude skeletal metastase.
-
7/31/2019 Bone Scan Pp
23/49
Primary Bone Tumours
A wide variety of benign & malignanttumours can be investigated with bone
scintigraphy.Of malignant tumours : osteosarcomas,
Ewings tumours, & giant cell tumoursusually show increased tracer uptakeon both blood pool & delayed images.
-
7/31/2019 Bone Scan Pp
24/49
Primary Bone Tumours
Among benign tumours, bone scan in most usefulfor detecting osteoid osteoma, as radiographs arecommonly normal & the bone scan has a
characteristic appearance
Osteoblastomas & chondroblastomas also showincreased activity on both blood pool & delayedimages but have characteristic X-ray appearances.
-
7/31/2019 Bone Scan Pp
25/49
Osteomyelitis
The use of bone scan for osteomyelitis has
become an established routine procedure.
Uptake in osteomyelitis is usually focal &present in all three phases.
A bone scan will often show increased
activity about 2 weeks before an X-raybecomes positive.
-
7/31/2019 Bone Scan Pp
26/49
Metabolic Bone Disease
Increased uptake in axial skeleton
Increased uptake in long bones
Increased uptake in periarticular area Faint or absent kidney images
Prominent calvaria and mandible
Beading of costochondral junction
Tie sternum
-
7/31/2019 Bone Scan Pp
27/49
Avascular Necrosis
Bony infarction complication offracture
Bone scanreduced uptake due todiminished blood supply.
-
7/31/2019 Bone Scan Pp
28/49
Imaging infection/inflammation
Inflammation reaction of the body to any
kind of injury
Infection simply means contaminationwith microorganism
-
7/31/2019 Bone Scan Pp
29/49
Radiopharmaceuticals for image infection
Non specific : Ga-67 citrate
increased blood supply, vascular
permeability and enhanced transudation
Specific : specific processes of accumulation
comprise a number of possible interaction
between the radiopharmaceuticals and thetarget
-
7/31/2019 Bone Scan Pp
30/49
Leucocytes : HMPAO, cytokines,
interleukin-1, 2 and 8, platelet factors 4
Antibiotics : ciprofloxacin , peptides
FDG-PET
-
7/31/2019 Bone Scan Pp
31/49
Imaging with Tc99m-Ciprofloxacin(Infecton)
-
7/31/2019 Bone Scan Pp
32/49
Introduction
Ciprofloxacin is an antibiotic with theproperty of binding to actively dividingbacteria. It binds to the DNA-gyrase
enzyme.A study showed that it binds to a widerange of bacteria, particularlystaphylococciappropriate for imaginginfection.
-
7/31/2019 Bone Scan Pp
33/49
Introduction
Imaging is undertaken at 1 hour & 4 hourafter injection. In particular circumstances,
a 24 hour imaging is essential.
-
7/31/2019 Bone Scan Pp
34/49
Normal Features
Vascular, renal & urine activity are visible becauseinfecton is renally excreted.
Decrease of liver,spleen & blood pool activity with time.
No bone marrow uptake the problem of bone marrow
interference in the interpretation of inflammatory changdoes not arrise.
Symmetrical uptake in bone epiphyses in growing
children is a normal variant.
-
7/31/2019 Bone Scan Pp
35/49
-
7/31/2019 Bone Scan Pp
36/49
Clinical Advantages
The main indication : when there is a need tolocalise the site of bacterial infection, example :in patient with a fever of unknown origin.
Its particular use in distinguishing activebacterial infectionfrom inflammatory particularlyin orthopaedic conditions : osteomyelitis, septic
arthritis, evaluation of prostheses, vertebralabscess or infection in the sternum after
coronary bypass surgery.
-
7/31/2019 Bone Scan Pp
37/49
-
7/31/2019 Bone Scan Pp
38/49
In the diabetic foot, is it skin & bone that is
infected or skin alone ?
In the knee, is it aseptic inflammation or septicarthritis ?
In the hip prosthesis, does it have asepticinflammation or is it infected ?
It aids the management of patients with suspectedor known bacterial infection, particularly with
regard to key issue of when to stop antibiotictherapy.
-
7/31/2019 Bone Scan Pp
39/49
-
7/31/2019 Bone Scan Pp
40/49
Acute Inflammation Vs Active
Infection
In typical acute inflammatory joint due to
rheumatoid or other arthropathy, theuptake at 1 h & 4 h is visible, but at 24 h ithas fadednot infected
-
7/31/2019 Bone Scan Pp
41/49
Acute Inflammation Vs Active Infection
Infecton is a small molecule which rapidly
diffuses in & out of sites of inflammation.Itdiffuses in rapidly because of the extrapermeability of an inflammatory lesion. Itdiffuses out because there is no specific
binding & as the blood level of infectonfalls, so the level in the inflammation willfall.
-
7/31/2019 Bone Scan Pp
42/49
Acute Inflammation Vs Active Infection
If there is specific binding, then Infecton
will remain bound to that site because of thedividing bacteria.
-
7/31/2019 Bone Scan Pp
43/49
-
7/31/2019 Bone Scan Pp
44/49
As well as its specificity for bacteria, there
is a dynamic specificity, which helps to
differentiate active bacterial infection fromacute or active non-bacterial inflammation.
-
7/31/2019 Bone Scan Pp
45/49
The key to the success of this agent is
not only that it binds to bacteria, but
that it clears quickly from sites of non-infected inflammation 24 h image is
essential.
-
7/31/2019 Bone Scan Pp
46/49
-
7/31/2019 Bone Scan Pp
47/49
-
7/31/2019 Bone Scan Pp
48/49
References
1. Maisey MN, Britton KE and Collier BD
(1998). Clinical Nuclear Medicine. 3rd
edition. Chapman & Hall Medical.London.
-
7/31/2019 Bone Scan Pp
49/49