
Bone Pathology. The cells Anatomy of bone Bone growth Types of fractures Fracture healing Fat emboli...
54
Bone Pathology
-
Upload
cornelius-harrell -
Category
Documents
-
view
217 -
download
0
Transcript of Bone Pathology. The cells Anatomy of bone Bone growth Types of fractures Fracture healing Fat emboli...

Bone Pathology

Bone Pathology
• The cells• Anatomy of bone• Bone growth• Types of fractures• Fracture healing• Fat emboli• Osteoporosis• Osteomalacia/Rickets• Compartment syndrome

The Cells
• Osteoblasts
• Osteoclasts
• Fibroblasts
• Chondroblasts


Anatomy of Bone
• Spongy bone
• Compact bone



Spongy Bone
• Trabeculae
• Spaces filled with red marrow
• Haematopoiesis

Compact Bone
• Osteon
• Central Haversian canal surrounded with lamellae of hard bone
• Perforating (Volkmann) canals
• Osteocytes
• Lacunae
• Canaliculi


Osteogenesis
• Intramembranous
• Endochondral





Bone Growth
• Length
• Appositional
• Remodelling
• Hormonal regulation




Types of Fractures









Fracture Healing
1 Haematoma
2 Fibrocartilaginous callous
3 Bony callous
4 Remodelling

Haematoma
• Local shock (minutes to 1/2 hour)
• Static blood at fracture site
• Bone cells lack oxygen and die


Fibrocartilaginous Callous
• 6 - 10 days• Capillaries grow into haematoma• Phagocytes clean up debris• Fibroblasts and osteoblasts migrate • Fibroblasts produce collagen• Osteoblasts form spongy bone• Chondroblasts secrete cartilage matrix• Bone is “splinted”


Bony Callous
• 3 - 10 weeks
• Osteoblasts migrate inwards and multiply to form callous of spongy bone

Remodeling
• Months
• Excess callous shrinks
• Compact bone laid down
• Final structure is a response to the mechanical stress experienced by the bone


Factors Affecting Healing
• nature of injury
• amount of bone loss
• type of bone injured
• degree of immobilization
• infection
• circulation
Fat Emboli
• may appear in lung or peripheral capillaries• Fat Embolism Syndrome
– dyspnoea– confusion– tachycardia– fever– rash– fat globules in sputum and urine

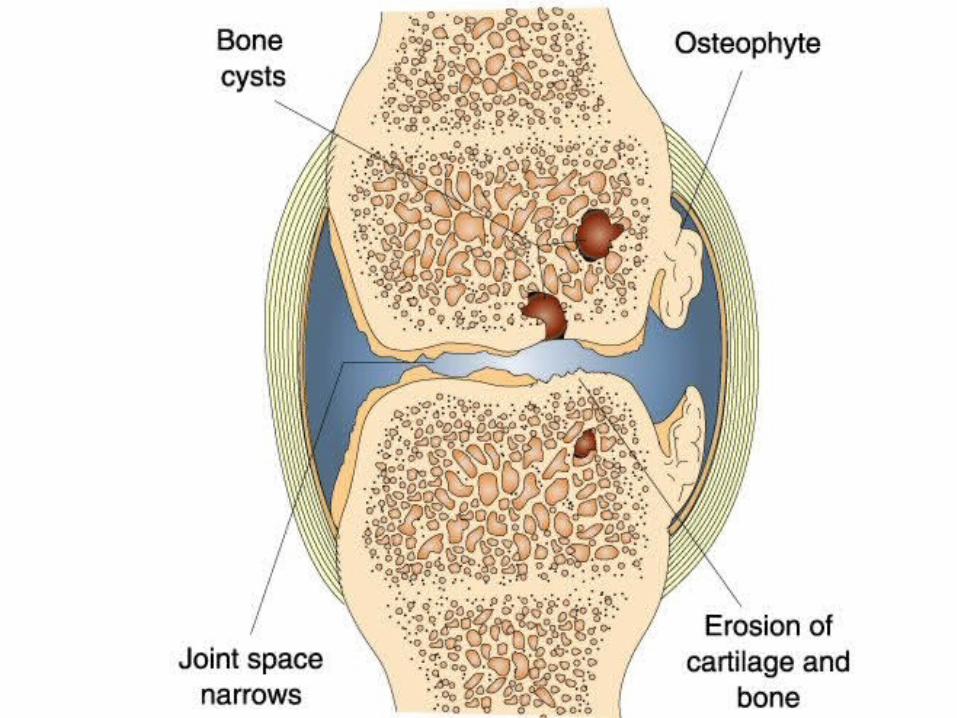
Osteoarthritis
• Wearing out of the joint
• Obesity, marathon runners, gymnasts
• Health of chondrocytes determines joint integrity
• Changes in both composition and mechanical properties of cartilage
• Cracks appear in cartilage
• Subchondral bone becomes exposed

Osteoarthritis
• Fragments of cartilage and bone become free floating “joint mice”
• Osteophytes or spurs form at joint margins
• Non specific inflammation of the synovium

Mechanical injury
Chondrocyte response
Release of Cytokines
(e.g. TNF, IL-1)
Production, releaseof protease enzymes
Destruction ofjoint structures
Development ofsurface cracks
Loss of smoothcartilage surface
Destruction of Subchondral bone
Osteophyteformation

Disc degeneration
• Disc narrowing producing low back pain and disc degeneration are related to increasing BMI.

Osteoporosis
• A gradual decrease in bone mass
• risk of fractures
• bone resorption is greater than bone formation
• bone loss involves matrix and minerals
• exercise and good nutrition may prevent or delay osteoporosis

Postmenopausal osteoporosis
• due to decrease in oestrogen levels
• oestrogen stimulates osteoblasts to form bone and inhibits osteoclasts
• fractures tend to be in vertebrae & distal radius due to loss of trabeculae

Prevention
• changes are reversed during oestrogen therapy (but what else?)
• Calcium: RDA = 1000mg/day; RDA(post-menopause) = 1200mg/day
• weight bearing exercise increases bone mass

Model for the Effects of Physical Activity on Bone
Mass
AGE
BMD(g/cm2)
“Fracture Threshold”
Increased BMD
growth
adulthoodmenopause

Osteomalacia/Rickets
• abnormal levels of minerals in bone
• due to low levels of Vit D
• caused by:– diet deficiency (Vit D or calcium) – low sun exposure– chronic renal failure– liver disease

Compartment Syndrome

Compartment Syndrome
• collagenous fascia doesn’t stretch
• haemorrhage is contained
• pressure may increase compromising blood flow and nervous function distally
• fasciotomy may be required













![The Difficult Diagnosis of Hypophosphatemic Rickets-A Review of …article.clinicalmed.org/pdf/10.11648.j.cmr.20200905.11.pdf · D-resistant rickets/osteomalacia [5]. 2. Material](https://static.fdocuments.net/doc/165x107/60407e73e4edd922d0572ba6/the-difficult-diagnosis-of-hypophosphatemic-rickets-a-review-of-d-resistant-ricketsosteomalacia.jpg)




