Bone mineral disease
52
BONE MINERAL DISEASE
-
Upload
shamila-karuthu -
Category
Documents
-
view
223 -
download
2
description
BMD in dialysis
Transcript of Bone mineral disease

BONE MINERAL DISEASE

Definition

Types of bone disease• Predominant hyperparathyroid-mediated high-turnover
bone disease (osteitis fibrosa [OF])• Low-turnover osteomalacia (defective mineralization in
association with low osteoclast and osteoblast activities)• Mixed uremic osteodystrophy (MUO; hyperparathyroid
bone disease with a superimposed mineralization defect)• Osteomalacia (defined as a mineralization lag time >100
days).• Adynamic bone (diminished bone formation and
resorption)

Prevalance of types of bone disease as determined by bone biopsy in patients with CKD-MBD
AD, adynamic bone; OF, osteitis fibrosa; OM, osteomalacia.





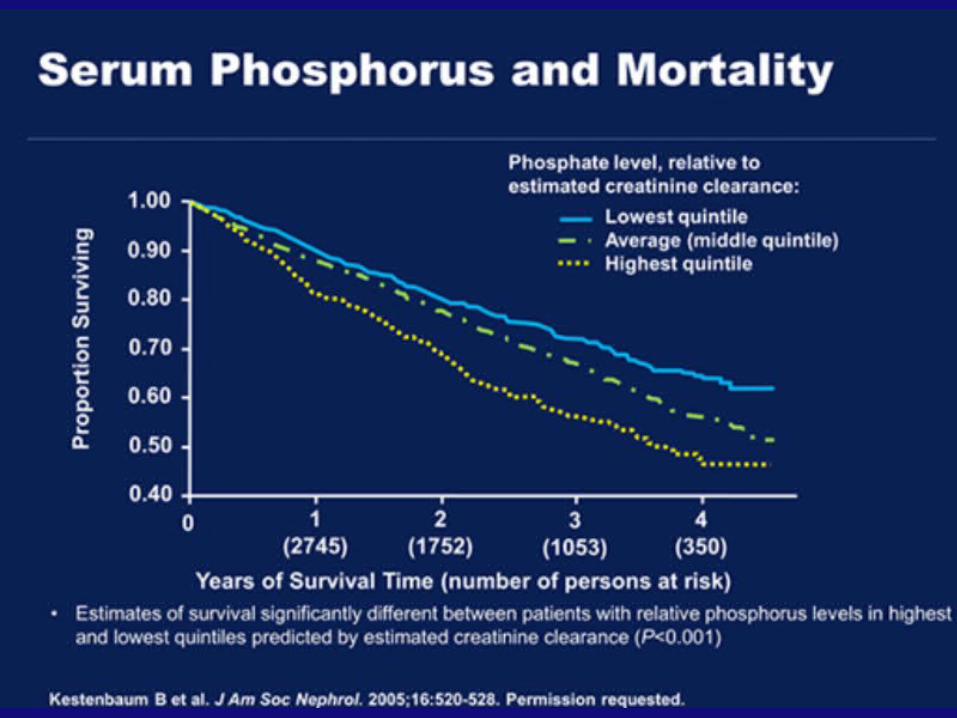
Risk of all-cause mortality associated with combinations of baseline serum phosphorus and calcium categories by PTH level
(from DOPPS)
Tentori F, et al. AJKD 52: 519, 2008

VASCULAR CALCIFICATION


VASCULAR CALCIFICATION








Calcium/Phosphate• KDIGO recommend dialysate calcium
concentration 1.25 -1.5 mmol/l ( 2.5-3.0 meq/l)• KDOQI : 2.5meq• KDOQI : Total calcium should be maintain 2.2-
2.37 mmol (8.8 -9.5). If calcium > 2.54 ( 10.2)…something needs to be done
• Phosphate; 0.87-1.49 (2.7-4.6)mg/dl GFR 15-59• Phosphate: 1.13-1.78 (3.5-5.5) GFR<15

PTH
• KDOQI :eGFR 30-59 : 35-70 eGFR 15-29: 70-110eGFR <15: 150-300 (16.5 -33.0)• KDIGO : 2-9 upper limit of normal values


Treatment
• Calcium • Phosphate Binders• Vitamin D• Cinnacalcet• Parathyroidectomy

Calcium based binders
Calcium acetate more efficient phosphate binder than calcium carbonateCalcium carbonate dissolve only at acid pH and many patients have low acid levels or on antiacidsTotal dose of elementary calcium ( include dietary) should not exceed 2000mg. For binders should exceed 1500mg


Vitamin D
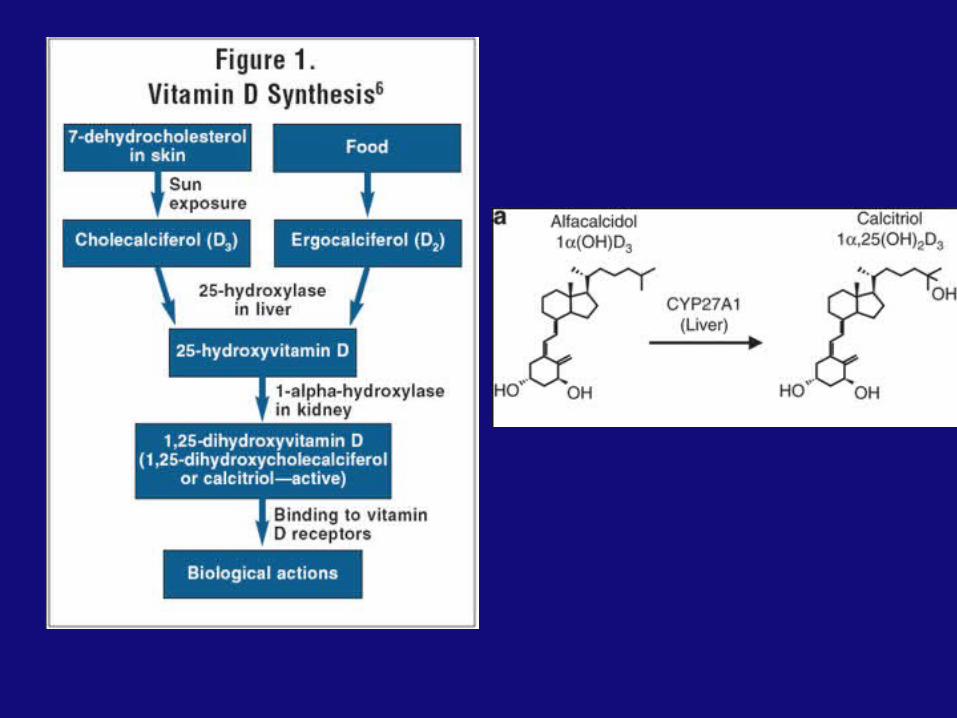

Zheng et al. BMC Nephrology 2013, 14 :199





THE LANCET: Effect of calcium based versus non-calcium based phosphate binders on martality in patients with chronic kidney disease : systemic review and meta-analysis






Cinnacalcet
• Lowers PTH levels by increasing the sensitivity of the calcium-sensing receptor to extracellular calcium
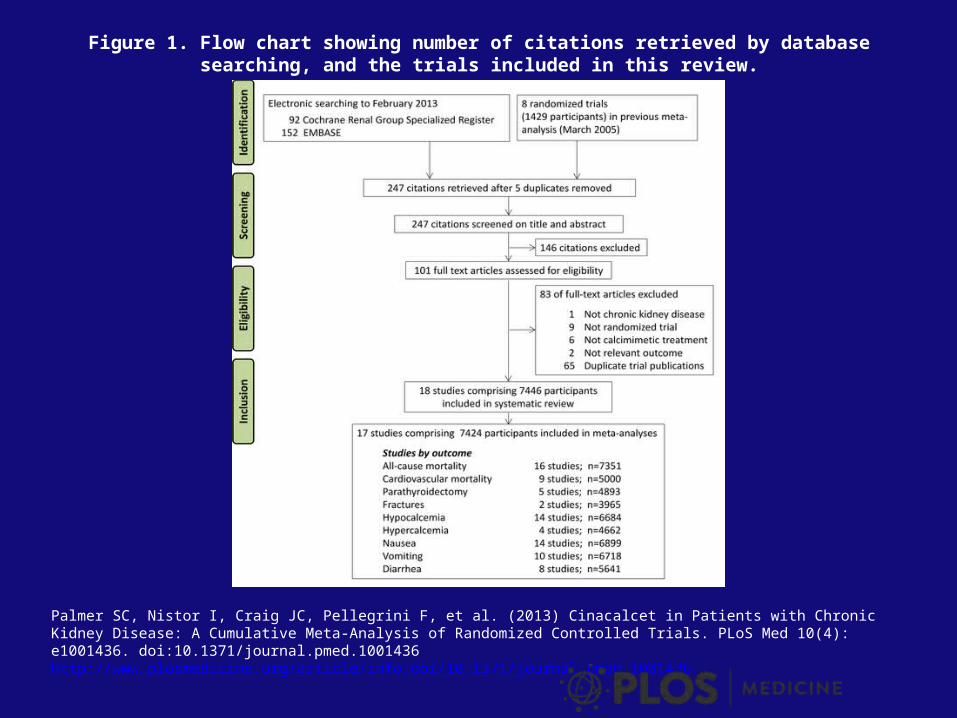
Figure 1. Flow chart showing number of citations retrieved by database searching, and the trials included in this review.
Palmer SC, Nistor I, Craig JC, Pellegrini F, et al. (2013) Cinacalcet in Patients with Chronic Kidney Disease: A Cumulative Meta-Analysis of Randomized Controlled Trials. PLoS Med 10(4): e1001436. doi:10.1371/journal.pmed.1001436http://www.plosmedicine.org/article/info:doi/10.1371/journal.pmed.1001436


Advance study



Evolve Study

Parathyroidectomy• Severe hypercalcemia.• Progressive and debilitating hyperparathyroid bone disease as
defined by radiographic or histologic evaluation. • Pruritus that does not respond to medical or dialytic therapy. • Progressive extraskeletal calcification or calciphylaxis that is
usually associated with hyperphosphatemia that is refractory to oral phosphate binders. In this setting, PTH-induced release of phosphate from bone contributes to the persistent elevation in the serum phosphate concentration. Parathyroidectomy will tend to minimize further calcification by lowering the serum calcium and phosphate concentrations
• Otherwise unexplained symptomatic myopathy.• PTH should > 800





Issues I did not touch on is:• Osteoporosis in CKD and Dialysis and
Management
• Thank you