Bone Marrow Biopsy: Interpretive Guidelines For the … Article Bone Marrow Biopsy: Interpretive...
19
Review Article Bone Marrow Biopsy: Interpretive Guidelines For the Surgical Pathologist James D. Cotelingam Department of Pathology, Louisiana State University Health Sciences Center, Shreveport, Louisiana, U.S.A. Summary: Ideally, the bone marrow core biopsy should be reviewed with knowledge of the clinical history, complete blood count, and findings in the peripheral blood and bone marrow aspirate smears. However, for a variety of reasons, the pathologist may receive the core biopsy and aspirate clot section without all of this information. Although this approach is not optimal, a great deal of valuable information can be generated from these specimens. Over the past 20 years, there has been considerable progress in the fields of flow cytometric analysis, immunohistochemistry, and mo- lecular diagnostic studies that can be performed on smears or extracted DNA from paraffin embedded tissue. These modalities have augmented and refined diagnostic criteria formerly ascertained by light microscopy, cytochemistry, and cytogenetics. This is particularly true of some myeloid and lymphoreticular neoplasms where a collaborative and multidisciplinary approach to the diagnosis has become necessary. Despite this growing complexity and dependence on newer methodologies, the tradi- tional role of histopathology in evaluating the bone marrow biopsy remains as impor- tant as it has been in the past. In this review, we focus on contemporary practices and expectations for interpreting bone marrow biopsies and clot sections. Key Words: Bone marrow core biopsy—Immunohistochemistry—Fluorescence in situ hybridiza- tion—Polymerase chain reaction. INTRODUCTION Assessment of changes in the bone marrow is an im- portant prerequisite for the care and stratification of pa- tients with disease of the hematopoietic system. Located within the labyrinth of the intertrabecular and medullary spaces of bone, this highly specialized organ with com- plex hematopoietic and immunologic functions provides an excellent substrate for pathologic investigation in- cluding the staging of nonhematopoietic neoplasms and the monitoring of response to therapy. Due to variations in logistical detail, organizational experience, billing practices, and attempts at cost con- tainment from one medical facility to another, Anatomic Pathology Services often receive only the core biopsy and clot section, while other components of the bone marrow specimen are submitted elsewhere for evalua- tion. Despite this fragmented and unsatisfactory ap- proach to total specimen interpretation, the surgical pa- thologist can ascertain considerable clinically relevant pathologic detail by supplementing traditional histopa- thology on paraffin embedded tissue (PET) with state of the art immunohistochemistry (IHC) and molecular di- agnostic studies. ROLE OF THE BONE MARROW BIOPSY IN PATIENT CARE Ever since the role of the bone marrow in hematopoi- esis was described in the German literature by Neumann Address correspondence and reprint requests to Dr. James D. Cotelingam, Department of Pathology, Louisiana State University Health Sciences Center, 1501 Kings Highway, Shreveport, LA 71330. The opinions published herein are the private views of the author and do not reflect the official position of the Louisiana State University Health Science Center. Advances in Anatomic Pathology Vol. 10, No. 1, pp. 8–26 © 2003 Lippincott Williams & Wilkins, Inc., Philadelphia 8
Transcript of Bone Marrow Biopsy: Interpretive Guidelines For the … Article Bone Marrow Biopsy: Interpretive...

Review Article
Bone Marrow Biopsy: Interpretive Guidelines For theSurgical Pathologist
James D. Cotelingam
Department of Pathology, Louisiana State University Health Sciences Center, Shreveport, Louisiana, U.S.A.
Summary: Ideally, the bone marrow core biopsy should be reviewed with knowledgeof the clinical history, complete blood count, and findings in the peripheral blood andbone marrow aspirate smears. However, for a variety of reasons, the pathologist mayreceive the core biopsy and aspirate clot section without all of this information.Although this approach is not optimal, a great deal of valuable information can begenerated from these specimens. Over the past 20 years, there has been considerableprogress in the fields of flow cytometric analysis, immunohistochemistry, and mo-lecular diagnostic studies that can be performed on smears or extracted DNA fromparaffin embedded tissue. These modalities have augmented and refined diagnosticcriteria formerly ascertained by light microscopy, cytochemistry, and cytogenetics.This is particularly true of some myeloid and lymphoreticular neoplasms where acollaborative and multidisciplinary approach to the diagnosis has become necessary.Despite this growing complexity and dependence on newer methodologies, the tradi-tional role of histopathology in evaluating the bone marrow biopsy remains as impor-tant as it has been in the past. In this review, we focus on contemporary practices andexpectations for interpreting bone marrow biopsies and clot sections. Key Words:Bone marrow core biopsy—Immunohistochemistry—Fluorescence in situ hybridiza-tion—Polymerase chain reaction.
INTRODUCTION
Assessment of changes in the bone marrow is an im-portant prerequisite for the care and stratification of pa-tients with disease of the hematopoietic system. Locatedwithin the labyrinth of the intertrabecular and medullaryspaces of bone, this highly specialized organ with com-plex hematopoietic and immunologic functions providesan excellent substrate for pathologic investigation in-cluding the staging of nonhematopoietic neoplasms andthe monitoring of response to therapy.
Due to variations in logistical detail, organizationalexperience, billing practices, and attempts at cost con-
tainment from one medical facility to another, AnatomicPathology Services often receive only the core biopsyand clot section, while other components of the bonemarrow specimen are submitted elsewhere for evalua-tion. Despite this fragmented and unsatisfactory ap-proach to total specimen interpretation, the surgical pa-thologist can ascertain considerable clinically relevantpathologic detail by supplementing traditional histopa-thology on paraffin embedded tissue (PET) with state ofthe art immunohistochemistry (IHC) and molecular di-agnostic studies.
ROLE OF THE BONE MARROW BIOPSY INPATIENT CARE
Ever since the role of the bone marrow in hematopoi-esis was described in the German literature by Neumann
Address correspondence and reprint requests to Dr. James D.Cotelingam, Department of Pathology, Louisiana State UniversityHealth Sciences Center, 1501 Kings Highway, Shreveport, LA 71330.
The opinions published herein are the private views of the author anddo not reflect the official position of the Louisiana State UniversityHealth Science Center.
Advances in Anatomic PathologyVol. 10, No. 1, pp. 8–26© 2003 Lippincott Williams & Wilkins, Inc., Philadelphia
8
(1) and Bizzozero (2) in 1868, and the first biopsy wasperformed by Mosler (3) in 1876, there have been re-markable improvements in the instrumentation and tech-niques of specimen acquisition, analysis, and interpreta-tion.
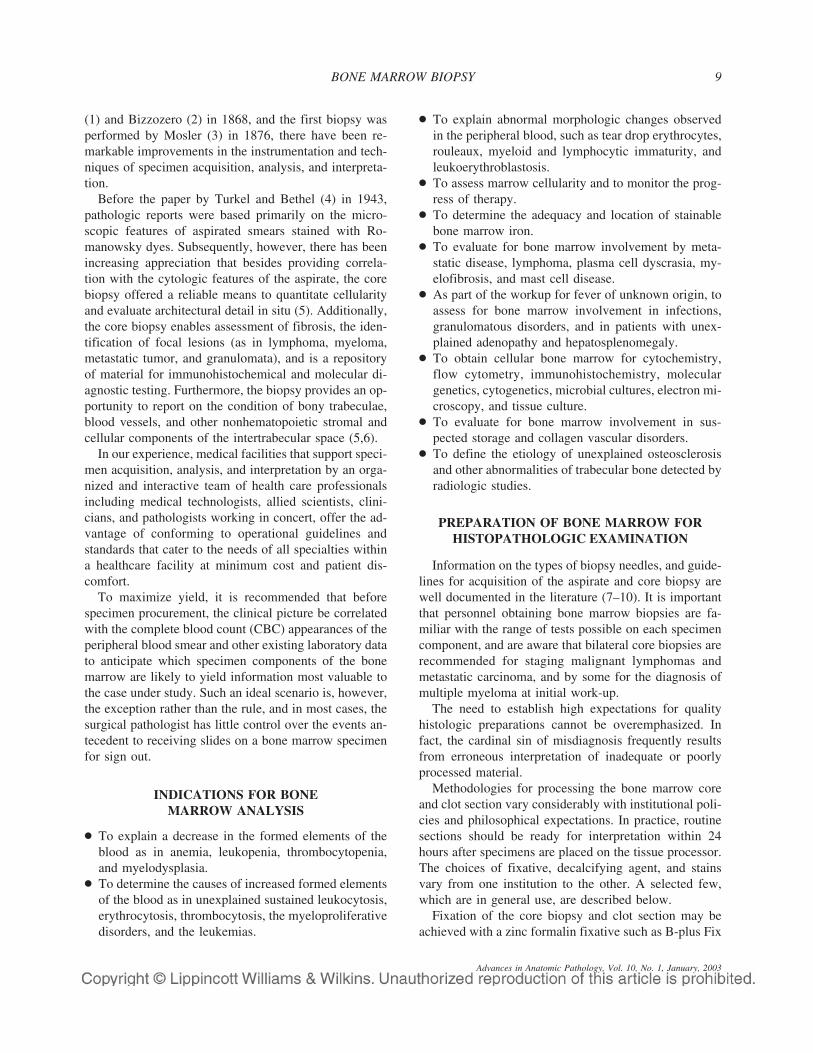
Before the paper by Turkel and Bethel (4) in 1943,pathologic reports were based primarily on the micro-scopic features of aspirated smears stained with Ro-manowsky dyes. Subsequently, however, there has beenincreasing appreciation that besides providing correla-tion with the cytologic features of the aspirate, the corebiopsy offered a reliable means to quantitate cellularityand evaluate architectural detail in situ (5). Additionally,the core biopsy enables assessment of fibrosis, the iden-tification of focal lesions (as in lymphoma, myeloma,metastatic tumor, and granulomata), and is a repositoryof material for immunohistochemical and molecular di-agnostic testing. Furthermore, the biopsy provides an op-portunity to report on the condition of bony trabeculae,blood vessels, and other nonhematopoietic stromal andcellular components of the intertrabecular space (5,6).
In our experience, medical facilities that support speci-men acquisition, analysis, and interpretation by an orga-nized and interactive team of health care professionalsincluding medical technologists, allied scientists, clini-cians, and pathologists working in concert, offer the ad-vantage of conforming to operational guidelines andstandards that cater to the needs of all specialties withina healthcare facility at minimum cost and patient dis-comfort.
To maximize yield, it is recommended that beforespecimen procurement, the clinical picture be correlatedwith the complete blood count (CBC) appearances of theperipheral blood smear and other existing laboratory datato anticipate which specimen components of the bonemarrow are likely to yield information most valuable tothe case under study. Such an ideal scenario is, however,the exception rather than the rule, and in most cases, thesurgical pathologist has little control over the events an-tecedent to receiving slides on a bone marrow specimenfor sign out.
INDICATIONS FOR BONEMARROW ANALYSIS
● To explain a decrease in the formed elements of theblood as in anemia, leukopenia, thrombocytopenia,and myelodysplasia.
● To determine the causes of increased formed elementsof the blood as in unexplained sustained leukocytosis,erythrocytosis, thrombocytosis, the myeloproliferativedisorders, and the leukemias.
● To explain abnormal morphologic changes observedin the peripheral blood, such as tear drop erythrocytes,rouleaux, myeloid and lymphocytic immaturity, andleukoerythroblastosis.
● To assess marrow cellularity and to monitor the prog-ress of therapy.
● To determine the adequacy and location of stainablebone marrow iron.
● To evaluate for bone marrow involvement by meta-static disease, lymphoma, plasma cell dyscrasia, my-elofibrosis, and mast cell disease.
● As part of the workup for fever of unknown origin, toassess for bone marrow involvement in infections,granulomatous disorders, and in patients with unex-plained adenopathy and hepatosplenomegaly.
● To obtain cellular bone marrow for cytochemistry,flow cytometry, immunohistochemistry, moleculargenetics, cytogenetics, microbial cultures, electron mi-croscopy, and tissue culture.
● To evaluate for bone marrow involvement in sus-pected storage and collagen vascular disorders.
● To define the etiology of unexplained osteosclerosisand other abnormalities of trabecular bone detected byradiologic studies.
PREPARATION OF BONE MARROW FORHISTOPATHOLOGIC EXAMINATION
Information on the types of biopsy needles, and guide-lines for acquisition of the aspirate and core biopsy arewell documented in the literature (7–10). It is importantthat personnel obtaining bone marrow biopsies are fa-miliar with the range of tests possible on each specimencomponent, and are aware that bilateral core biopsies arerecommended for staging malignant lymphomas andmetastatic carcinoma, and by some for the diagnosis ofmultiple myeloma at initial work-up.
The need to establish high expectations for qualityhistologic preparations cannot be overemphasized. Infact, the cardinal sin of misdiagnosis frequently resultsfrom erroneous interpretation of inadequate or poorlyprocessed material.
Methodologies for processing the bone marrow coreand clot section vary considerably with institutional poli-cies and philosophical expectations. In practice, routinesections should be ready for interpretation within 24hours after specimens are placed on the tissue processor.The choices of fixative, decalcifying agent, and stainsvary from one institution to the other. A selected few,which are in general use, are described below.
Fixation of the core biopsy and clot section may beachieved with a zinc formalin fixative such as B-plus Fix
BONE MARROW BIOPSY 9
Advances in Anatomic Pathology, Vol. 10, No. 1, January, 2003

(BBC, Stanwood, WA), B-5, or neutral buffered forma-lin. Thereafter, the specimen should be decalcified in a10% aqueous solution of nitric acid, Redecal (a 12.5%aqueous solution of hydrochloric acid in EDTA, Stat LabMedical Products Inc., Lewisville, TX) or RDO (APBEngineering Products Corporation, Plainfield, IL), an-other proprietary solution of hydrochloric acid in a coaltar base ensuring good histologic sections, without dam-age to the microtome knife. Decalcification results in theleaching out of some storage iron from the core biopsy,and nitric acid and hydrochloric acid have been reportedto diminish the acid fastness of mycobacteria (11,12)resulting in false negative results. Acid fastness is how-ever retained when decalcification is in formic acid-sodium citrate or citric acid buffer (12). Therefore, theseare the decalcifying agents of choice when the need todemonstrate mycobacteria can be anticipated. Combina-tion fixative/decalcification preparations in use are Zen-ker’s solution (13), Surgipath Decalcifier (a formic-acidformalin mixture, Surgipath Medical Industries, Rich-mond, IL), and Decal Plus (an aqueous solution of for-malin, formic acid, and methanol, Stat Lab Medicalproducts, Inc. Lewisville, TX). An advantage of Zenk-er’s solution and B-5 is a mordanting effect that en-hances the tinctorial properties of the Giemsa and hema-toxylin and eosin (H & E) stains. Additionally, glacialacetic acid, the decalcifying component in Zenker’s so-lution counteracts the cell shrinkage resulting from fixa-tion. Metallic fixatives such as Zenker’s and B-5 degradeDNA and impair subsequent molecular diagnostic test-ing. This limitation is circumvented by fixation in a zinc-formalin fixative such as B-plus Fix. It is noteworthy thatthe manufacturer’s specified ratio of specimen volume tofixative/decalcifying agent and treatment times beclosely followed to achieve optimum results.
Clot sections do not need to be decalcified. Bone dustand small fragments of bony trabeculae that are occa-sionally aspirated when acquisition of the core biopsyprecedes that of the aspirate, can usually be cut throughwithout decalcification. Agar embedding techniques (14)for processing the clot section, plastic embedding (15,16)of the undecalcified core and electron microscopy (16–20) of aspirated material are described in the literature;however, these techniques are not widely used for rou-tine purposes.
Ideally, histologic sections of the core and clot sectionshould be cut at 4 micron. In addition to routine hema-toxylin-eosin stained sections, other stains of value in-clude iron (preferably performed on the nondecalcifiedaspirate clot section), reticulin, periodic acid-Schiff stain(PAS), and Giemsa. Although difficult to perform, awell-done Giemsa preparation can be very helpful. This
stain imports a purple hue to the cytoplasm of plasmacells, prominently highlights the metachromatic granulesof mast cells and basophils, and enhances the tinctorialproperties of neutrophilic and eosinophilic granules. Ad-ditional immunohistochemical stains may be necessary,and are further discussed below.
Samples for molecular studies require special han-dling. For instance, lesions for assessment by fluores-cence in-situ hybridization (FISH) may need to be local-ized for the benefit of personnel in the molecular diag-nostic laboratory. Paraffin sections for FISH aresubmitted on Superfrost Plus glass slides (Fisher Scien-tific, Pittsburgh, PA). For the polymerase chain reaction(PCR), scrolls of paraffin embedded tissue are deparaf-finized before DNA isolation in accordance with localpolicies and practices.
EXPECTED DIAGNOSTIC YIELD FROMCOMPONENTS OF THE BONE
MARROW SPECIMEN
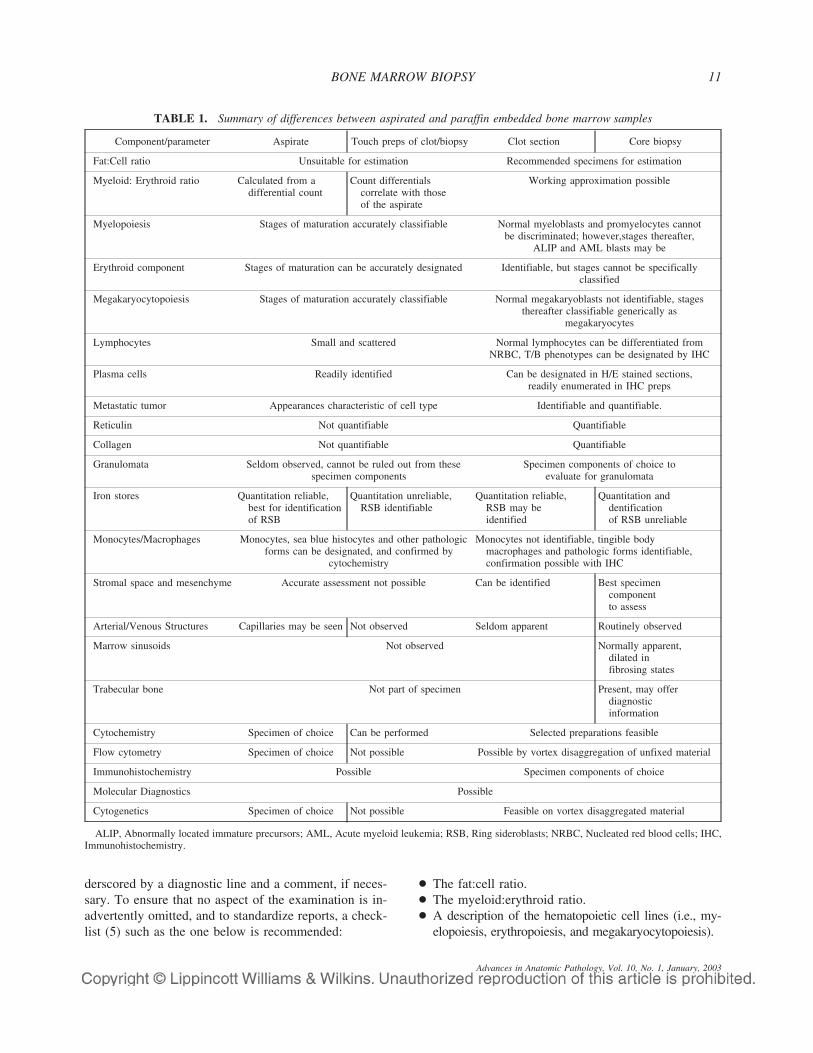
Not every item in the preceding list of indicationsprompting bone marrow analysis can be resolved by ex-amination of the core biopsy and clot section. Further-more, the optimum yield of diagnostic information fromindividual components of a bone marrow specimen in-nately vary, and often reflect the type of disorder beinginvestigated (21). In general, the aspirate and touchpreparations provide qualitative cytologic detail, whilethe core biopsy and clot section provide quantitative in-formation. Because the surgical pathologist frequentlyreceives only PET, it is important to identify the expec-tations and limitations of the diagnostic yield from suchmaterial. These are enumerated and compared to thosefrom the aspirate and touch preparations in Table 1(5,6,21–36), and are further discussed below.
INTERPRETATION OF PARAFFIN EMBEDDEDTISSUE AND DATA INTEGRATION
For most anatomic pathologists, a bone marrowsample is often one among a number of surgicals in a runrequiring interpretation and sign-out. Although the pa-tients name, age, and gender are part of the standardbiographic template, information concerning the clinicalpicture, CBC, peripheral blood film, and bone marrowaspirate are often absent or inadequate, and need to beprocured to ensure a meaningful interpretation. Theguidelines used in evaluating a bone marrow specimenare understandably parochial. However, most observersintegrate the microscopic features of the specimen withthe ancillary data listed in Table 1 into a synopsis, un-
J. D. COTELINGAM10
Advances in Anatomic Pathology, Vol. 10, No. 1, January, 2003
derscored by a diagnostic line and a comment, if neces-sary. To ensure that no aspect of the examination is in-advertently omitted, and to standardize reports, a check-list (5) such as the one below is recommended:
● The fat:cell ratio.● The myeloid:erythroid ratio.● A description of the hematopoietic cell lines (i.e., my-
elopoiesis, erythropoiesis, and megakaryocytopoiesis).
TABLE 1. Summary of differences between aspirated and paraffin embedded bone marrow samples
Component/parameter Aspirate Touch preps of clot/biopsy Clot section Core biopsy
Fat:Cell ratio Unsuitable for estimation Recommended specimens for estimation
Myeloid: Erythroid ratio Calculated from adifferential count
Count differentialscorrelate with thoseof the aspirate
Working approximation possible
Myelopoiesis Stages of maturation accurately classifiable Normal myeloblasts and promyelocytes cannotbe discriminated; however,stages thereafter,
ALIP and AML blasts may be
Erythroid component Stages of maturation can be accurately designated Identifiable, but stages cannot be specificallyclassified
Megakaryocytopoiesis Stages of maturation accurately classifiable Normal megakaryoblasts not identifiable, stagesthereafter classifiable generically as
megakaryocytes
Lymphocytes Small and scattered Normal lymphocytes can be differentiated fromNRBC, T/B phenotypes can be designated by IHC
Plasma cells Readily identified Can be designated in H/E stained sections,readily enumerated in IHC preps
Metastatic tumor Appearances characteristic of cell type Identifiable and quantifiable.
Reticulin Not quantifiable Quantifiable
Collagen Not quantifiable Quantifiable
Granulomata Seldom observed, cannot be ruled out from thesespecimen components
Specimen components of choice toevaluate for granulomata
Iron stores Quantitation reliable,best for identificationof RSB
Quantitation unreliable,RSB identifiable
Quantitation reliable,RSB may beidentified
Quantitation anddentificationof RSB unreliable
Monocytes/Macrophages Monocytes, sea blue histocytes and other pathologicforms can be designated, and confirmed by
cytochemistry
Monocytes not identifiable, tingible bodymacrophages and pathologic forms identifiable,confirmation possible with IHC
Stromal space and mesenchyme Accurate assessment not possible Can be identified Best specimencomponentto assess
Arterial/Venous Structures Capillaries may be seen Not observed Seldom apparent Routinely observed
Marrow sinusoids Not observed Normally apparent,dilated infibrosing states
Trabecular bone Not part of specimen Present, may offerdiagnosticinformation
Cytochemistry Specimen of choice Can be performed Selected preparations feasible
Flow cytometry Specimen of choice Not possible Possible by vortex disaggregation of unfixed material
Immunohistochemistry Possible Specimen components of choice
Molecular Diagnostics Possible
Cytogenetics Specimen of choice Not possible Feasible on vortex disaggregated material
ALIP, Abnormally located immature precursors; AML, Acute myeloid leukemia; RSB, Ring sideroblasts; NRBC, Nucleated red blood cells; IHC,Immunohistochemistry.
BONE MARROW BIOPSY 11
Advances in Anatomic Pathology, Vol. 10, No. 1, January, 2003

● A quantitation and description of lymphocytes andplasma cells.
● Evaluation of stainable iron.● Exclusion or description and quantitation of neoplastic
infiltrates such as blast forms, lymphoma, myeloma,and metastatic tumor.
● Exclusion or description of infections and granuloma-tous changes.
● Exclusion or description of fibrosis.● A statement, if necessary, to cover any miscellaneous
abnormality observed in the macrophage system, bonemarrow stroma, vascular structures, and trabecularbone.
● A concluding comment integrating the above with theresults of any corroborating cytochemical, flow cyto-metric, immunohistochemical, molecular diagnostic,cytogenetic, or other contributing studies.
THE FAT:CELL RATIO
It is the best to evaluate marrow cellularity and thefat:cell ratio from the core biopsy. Although less reliable,these may also be assessed from clot sections with mul-tiple marrow particles. Variations in the ratio of fat tocell in the bone marrow are an important index of bonemarrow activity. At birth and during early childhood, thebone marrow is 100% cellular and virtually devoid of fat.By the end of the first decade, the overall fat:cell ratio isapproximately 10:90, and in adults (Fig. 1), it variesbetween 30:70 and 70:30 with increasing age. Slightphysiologic variations of the ratio from one microscopicfield to another are not uncommon and review of theslide with a scanning objective can enable definition ofan overall ratio. Beyond the seventh decade, bone mar-row fat may be expected to increase by approximately10% with each passing decade (37–39). Despite this in-creasing hypocellularity, the CBC remains within physi-ologic limits. However, in the presence of otherwise un-explained cytopenia, a fat content of greater than 70%reflects hypoplasia. Quantitation of the latter is usuallyexpressed as mild, moderate, or severe.
The word “aplasia” is derived from Greek (40), andconnotes total fatty replacement of the bone marrow.Aplasia may be generalized or focal (spotty). The de-creased cellularity within the stromal space that resultsfrom chemotherapeutic induction of acute leukemia (Fig.2), serous fat atrophy (Fig. 3), hypoproliferative states,and fibrosis are not accompanied by increased bone mar-row fat. Therefore, these are examples of hypocellularityrather than true aplasia. Under these circumstances, it isconsidered more meaningful to report a ratio incorporat-ing the relationships of fat, cell, and stroma. Accurate
evaluation of the fat:cell ratio is possible only on paraffinembedded tissue, and areas with stromal hemorrhage,dropout, and aspiration artifact should be excluded. Incases with unexplained aplasia without peripheral bloodcytopenia, it is advisable to recommend a contralateralcore biopsy to rule out sampling error.
QUANTITATION OF CELLULARCOMPONENTS IN THE BONE MARROW
Differential counts of cellular elements in the bonemarrow are traditionally expressed in percentile figures(6,27,41–50). Included herein are blast forms, myelo-monocytic, erythroid, megakaryocytic, plasma cellular,and lymphoid cell lines. Macrophages, stromal cells, os-teoclasts, osteoblasts, fat cells, and metastatic tumor cellsare excluded. The “hematopoietic” compartment is com-prised of all myelomonocytic, erythroid, and megakaryo-cytic elements. All other forms are classified as “nonhe-matopoietic.” Quantitation of the extent of involvementby tumor does convey meaning, and should be expressedas a percentage of the involved marrow space or totalmarrow cellularity.
MYELOID:ERYTHROID RATIO
At birth, the myeloid:erythroid (M:E) ratio is approxi-mately 1.5:1. The myeloid (granulocytic) componentgradually increases and peaks at approximately 6:1 bythe end of the first week of life (51). Thereafter, valuesplateau at a physiologic range of 2.5:1 to 4:1, with littlevariation throughout life (6,20,51). Increase in eithercomponent is reported as myeloid/erythroid “predomi-nant” in the presence of a normal fat:cell ratio, and “hy-perplasia” when the cellularity of the bone marrow ex-ceeds 70%. While an M:E ratio can be calculated from a500 cell count down to a decimal point in the aspirate,paraffin embedded tissue provides only a coarse approxi-mation of the same. However, paraffin embedded tissuehas the advantage of providing an overview of this ratioin situ, and in different areas of the specimen. Also,eliminated herein is any bias that may be manifest inparticle-depleted smears of sinusoidal blood. It is best toread M:E ratios on core biopsies, away from paratrabecu-lar areas, which are normally myeloid predominant. Be-cause of their characteristic cytologic features, the my-eloid component beyond the promyelocyte stage can bereadily designated with a 40 x objective, right up to theneutrophil, eosinophil, and mast cell stage. Similarly,nucleated erythroid elements beyond the early normo-blast stage can be differentiated from lymphocytes bytheir round, dense, and pyknotic nuclei. In contrast to
J. D. COTELINGAM12
Advances in Anatomic Pathology, Vol. 10, No. 1, January, 2003
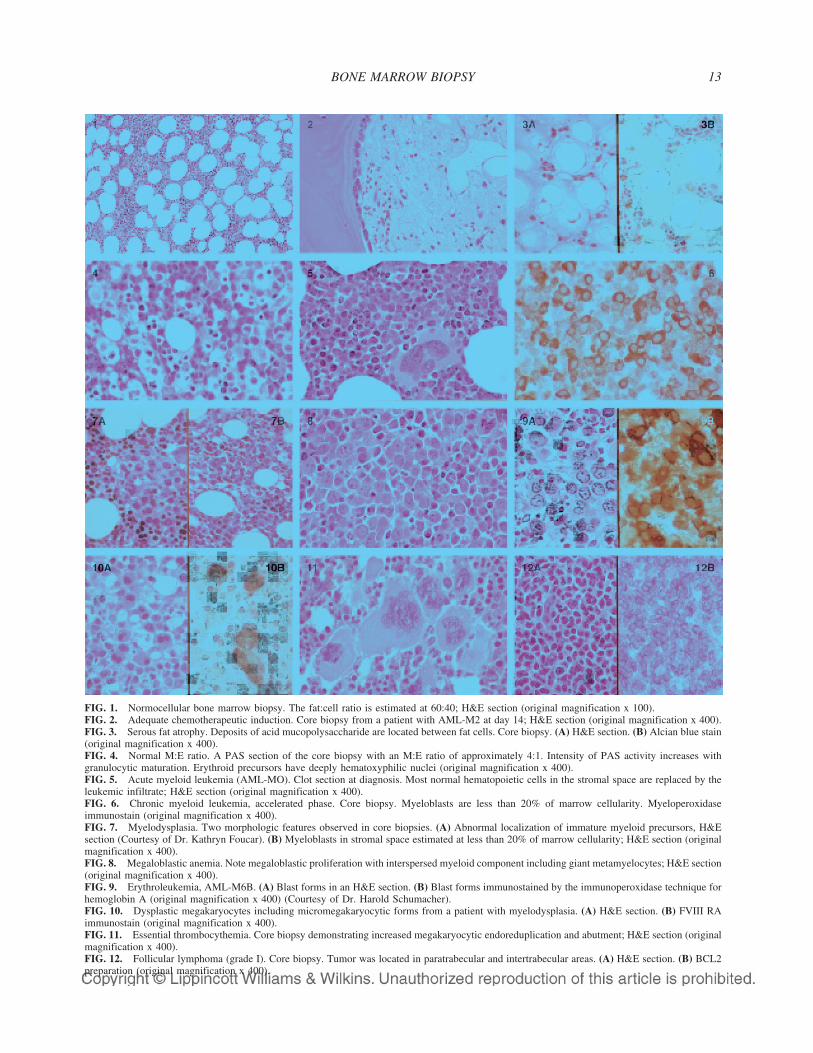
FIG. 1. Normocellular bone marrow biopsy. The fat:cell ratio is estimated at 60:40; H&E section (original magnification x 100).FIG. 2. Adequate chemotherapeutic induction. Core biopsy from a patient with AML-M2 at day 14; H&E section (original magnification x 400).FIG. 3. Serous fat atrophy. Deposits of acid mucopolysaccharide are located between fat cells. Core biopsy. (A) H&E section. (B) Alcian blue stain(original magnification x 400).FIG. 4. Normal M:E ratio. A PAS section of the core biopsy with an M:E ratio of approximately 4:1. Intensity of PAS activity increases withgranulocytic maturation. Erythroid precursors have deeply hematoxyphilic nuclei (original magnification x 400).FIG. 5. Acute myeloid leukemia (AML-MO). Clot section at diagnosis. Most normal hematopoietic cells in the stromal space are replaced by theleukemic infiltrate; H&E section (original magnification x 400).FIG. 6. Chronic myeloid leukemia, accelerated phase. Core biopsy. Myeloblasts are less than 20% of marrow cellularity. Myeloperoxidaseimmunostain (original magnification x 400).FIG. 7. Myelodysplasia. Two morphologic features observed in core biopsies. (A) Abnormal localization of immature myeloid precursors, H&Esection (Courtesy of Dr. Kathryn Foucar). (B) Myeloblasts in stromal space estimated at less than 20% of marrow cellularity; H&E section (originalmagnification x 400).FIG. 8. Megaloblastic anemia. Note megaloblastic proliferation with interspersed myeloid component including giant metamyelocytes; H&E section(original magnification x 400).FIG. 9. Erythroleukemia, AML-M6B. (A) Blast forms in an H&E section. (B) Blast forms immunostained by the immunoperoxidase technique forhemoglobin A (original magnification x 400) (Courtesy of Dr. Harold Schumacher).FIG. 10. Dysplastic megakaryocytes including micromegakaryocytic forms from a patient with myelodysplasia. (A) H&E section. (B) FVIII RAimmunostain (original magnification x 400).FIG. 11. Essential thrombocythemia. Core biopsy demonstrating increased megakaryocytic endoreduplication and abutment; H&E section (originalmagnification x 400).FIG. 12. Follicular lymphoma (grade I). Core biopsy. Tumor was located in paratrabecular and intertrabecular areas. (A) H&E section. (B) BCL2preparation (original magnification x 400).
BONE MARROW BIOPSY 13

appearances in H & E preparations, cells of myeloid anderythroid lineage are easier to recognize in Giemsa andPAS stains (Fig. 4), and can be designated with certaintyon myeloperoxidase (MPX) and hemoglobin peroxidase(HbPX) preparations of paraffin embedded tissue. It isnoteworthy that monocytes and lymphocytes (also re-ferred to as nongranulocytes), plasma cells, and mega-karyocytes are not included in the M:E ratio.
MYELOID SERIES
The myeloid component of the bone marrow arisesfrom self-replicating stem cells, which also gives rise tothe monocytic, erythroid, and megakaryocytic cell lines.Data on the physiologic range of myeloid precursors andmature forms in the bone marrow (Table 2)(41–43) havebeen derived from aspirate preparations where the cyto-logic features of each cell type are readily appreciatedunder an oil immersion lens. Even though quantitation ofsimilar information on PET is in contrast largely subjec-tive, and unlike aspirate counts lacks mathematical pre-cision, it does have clinical utility.
In our experience, normal myeloblasts and promyelo-cytes are not readily differentiated from pronormoblastsand early normoblasts in PET with a high dry objective.However, mature forms beyond the promyelocyte stageand pathologic shifts in compartment size as in myeloidhyperplasia, the myelodysplastic syndromes (MDS), theacute myeloid leukemias (AML) AML-MO (Fig. 5)through M6A, some of the myeloproliferative disorders,and chronic leukemias of myeloid origin are readily dif-ferentiated. Confirmation of myeloid lineage in PET maybe achieved by specific esterase (Leder), MPX (Fig. 6)and other immunostains (28–31,52–55); and a mono-cytic lineage may be supported by the identification ofCD68, lysozyme, alpha-1-antitrypsin, and alpha-1-antichymotrypsin activity in AML-M4, AML-M5 andchronic myelomonocytic leukemia (CMML)(56). Le-
sions of mast cell lineage can be specifically confirmedwith mast cell tryptase and CD117 (C-Kit) preparations(57–60), and TdT activity may be apparent in cases ofacute mixed lineage leukemia (61,62). Although the cy-tologic features of blast forms in AML on PET are notspecific for the subtypes of AML according to the FAB(French-American-British) scheme, cases of AML-M3,AML-M4, and AML-M5B do tend to have “monocyt-oid” nuclei. Also, minimal myeloid differentiation is ob-served in AML-M2, and an abnormal eosinophil com-ponent is apparent in AML-M4EO. Abnormal localiza-tion of immature myeloid precursors (ALIP) (Fig. 7) inthe intertrabecular space is a feature of myelodysplasia(63–65). Increased expression of PCNA antigen andCD34 activity by immunostaining on PET serve to dis-tinguish hypoplastic myelodysplastic syndromes fromacquired aplastic anemia, where these parameters are de-creased (66). While immunostaining with CD34 is ofvalue in identifying immature populations of leukemiccells, it does not distinguish between a myeloid and alymphoid lineage. Without incorporating data generatedfrom examination of the aspirate, cytochemistry, flowcytometry, cytogenetics, and molecular diagnostic stud-ies, it may be impossible to classify myeloid, and mixedlineage lesions, according to the recent recommendationsof the Society for Hematopathology and World HealthOrganization (WHO) expert committee (67–69).
In cases where no aspirate is available due to a dry tap,vortex disaggregation of leukemic cells from the unfixedcore biopsy and clot can serve as a resource of materialfor cytogenetics and flow cytometry. With the introduc-tion of newer generations of therapy such as Myelotarg(70) (formerly known as CMA-676), which is specifi-cally directed against the CD33 epitope in AML, andSTI571, (71,72) which targets and inhibits bcr-abl tyro-sine kinase in chronic myeloid leukemia (CML), there isa growing expectation that laboratory identification ofsuch loci will become available as part of the diagnosticarmamentarium. Furthermore, it has now become appar-ent that in patients with CML on STI571, despite micro-scopic restoration of marrow cellularity with normal M:Eratios, bcr-abl fusion persists (72) and may be demon-strated by FISH on the core biopsy and clot section(Table 3). This technology is therefore certain to influ-ence therapeutic protocols for STI571 in the future. Ac-cording to the WHO expert panel and the Society forHematopathology, the threshold for transition of blastcounts from myelodysplastic syndrome (MDS) (Fig. 7)to AML is set at 20% with the exception of lesions thatinclude a t(8;21) chromosomal abnormality (67,68,73).Despite lower blast counts, this entity, which would havebeen formerly classified as MDS, is now, because of a
TABLE 2. Types of myeloid elements and their normalrange in the bone marrow
Cell type Range
Myeloblasts 0% to 2%Promyelocytes 2% to 5%Myelocytes (neutrophilic) 9% to 16%Metamyelocytes 7% to 23%Band Forms 8% to 15%Neutrophils 4% to 10%Myelocytes (eosinophilic) 0% to 2%
Band 0% to 2%Mature 0% to 2%
Monocytes/macrophages 0% to 3%Basophils 0% to 1%Mast Cells 0% to 2%
J. D. COTELINGAM14
Advances in Anatomic Pathology, Vol. 10, No. 1, January, 2003

superior long-term outlook in adults, diagnosed andtreated earlier in its natural history as AML (69,73). Thesupportive role of molecular diagnostic studies, some ofwhich are now available on PET (Table 3), is therefore ofparamount importance. Additionally, it is noteworthythat the malignant progranulocytes of AML-M3 be in-cluded in the total blast count, as should the myeloblastsof erythroleukemia AML-M6A (74,75) (traditionalerythroleukemia of the FAB classification).
ERYTHROID SERIES
The erythroid component of the bone marrow nor-mally comprises between 15% and 37% of a differentialcell (6,42,43,52) count that includes granulocytes, mega-karyocytes, lymphocytes, and plasma cells. Maturingerythroid precursors include pronormoblasts, early nor-moblasts, intermediate normoblasts, and late normo-blasts. Of these, pronormoblasts and early normoblastscannot always be distinguished with certainty from my-eloblasts and promyelocytes in PET with a high dry ob-jective. However, later stages of erythroid maturationwith their characteristic round, dense and deeply baso-philic nuclei can be easily identified, and distinguishedfrom interspersed lymphocytes. In circumstances wherethis distinction poses a problem, IHC identification oferythroid precursors with an HbPX immunostain is de-finitive. This technology is also invaluable in confirmingthe absence of erythroid precursors in cases of total redcell aplasia. Under normal circumstances and in regen-erative states, clones of normoblasts tend to cluster in theintertrabecular space. However, in florid megaloblastichyperplasia (Fig. 8), marrow cellularity may be diffuse
and resemble the neoplastic proliferations of acute leu-kemia and large cell lymphoma (LCL). Unlike these con-ditions however, myeloid elements including giant meta-myelocytes are interspersed between megaloblasts. Un-der these circumstances, correlation of biopsy findingswith other laboratory data such as the appearances of theaspirate, CBC, serum LDH, folate, and B12 can be in-valuable. Arrested erythroid maturation, giant pronormo-blasts, and intranuclear inclusions are manifestations ofparvovirus B19 infection (76). Herein, viral material canbe positively identified by in situ hybridization (ISH) inPET. Multinucleated erythroid precursors may be ob-served in CDA (77), where additional confirmatory he-matological testing such as the Ham and Sugar Watertests become necessary. In cases of AML-M6B (74,75,78), bizarre multinuclearity of leukemic erythroid pre-cursors may be a prominent feature and lineage identitycan be established with HbPX immunostaining (Fig. 9)on PET (79). In such cases, neoplastic pronormoblastsshould be included with myeloblasts in the overall blastcount, and in keeping with the recommendations of theSociety of Hematopathology and WHO, cases with ablast count under 20% be classified as myelodysplasia,and those above as acute leukemia. Vortex disaggrega-tion of cellular material from the unfixed core biopsy forflow cytometric, cytogenetic, and molecular diagnosticstudies can be an invaluable adjunct in patients with adry tap (34).
MEGAKARYOCYTES
Megakaryocytes are the largest of the hematopoieticcells, and comprise between 0.5% and 2.0% of all nucle-ated marrow elements (6,52,80). The earliest cell of
TABLE 3. Lineage specific molecular cytogenetic probes* currently in use to identify myeloid lesions by fluorescence in situhybridization (FISH) on core biopsies of bone marrow
Disease Locus Chromosome abnormality
FISH Signal color
Green Orange Yellow
AML-M0/M1,MDS EGR1 5q Deletions-interstitial (5q31) 5p15.2 (control) 5q31-EGR1 N/AAML-M0/M1, MDS CSF1R 5q Deletions-telomeric(5q33-q34) 5p15.2 (control) 5q33-CSF1R N/AAML-MDS D20S108 (20q12) Deletions in 20q N/A 20q12 N/AAML/MDS D7S486 (7q31) Deletions in 7q, i(7q) Alpha-satellite 7
(7p11.1-q11.1)D7S486 (7q) N/A
AML/MDS 8p11.1-q11.1 Trisomy 8 N/A Alpha-satellite 8(8p11.1-q11.1)
N/A
AML-M2 AML1/ETO t(8;21)(q22;q22) 8q-ETO (CBFA2T1) 21q-AML1 (RUNX1) 8;21 Fusion signalAML-M3 (variant) RAR� t(11;17)(q23;q21) and related X/RARA Abnormal-1 green
(split signal)Abnormal-1 orange
(split signal)Dual color (normal)
AML-M3 PML/RAR� t(15;17)(q22;q21.1) 17q-RARA 15q-PML 15;17 Fusion signalAML-M4EO CBF� inv(16)(p13q22) and t(16;16)(p13;q22) Abnormal-1 green
(split signal)Abnormal-1 orange
(split signal)Dual color (normal)
AML-M5 and Mixed lineage MLL(ALL-1, HRX) 11q23 rearrangements-t(4;11)(q21;q23),t(9;11)(p22;q23),t(11;19)(q23;p13) and variants
Abnormal-1 green(split signal)
Abnormal-1 orange(split signal)
Dual color (normal)
CML BCR/ABL t(9;22)(q34;q11.2) 22q-BCR 9q-ABL 9;22 Fusion signal
* Vysis Inc. Downers Grove, IL.Tabulated by Mary L. Nordberg PhD.
BONE MARROW BIOPSY 15
Advances in Anatomic Pathology, Vol. 10, No. 1, January, 2003

megakaryocytic lineage discernable microscopically isthe megakaryoblast, a mononucleated cell with scantdeeply basophilic cytoplasm rich in RNA. Megakaryo-blasts are slightly larger than myeloblasts and pronormo-blasts, from which they are not readily distinguished inPET with a high dry objective. Subsequent stages ofmaturation are characterized by increased cell size, pro-gressive nuclear lobulation (endoreduplication), loss ofcytoplasmic basophilia, and increase in “cotton candy”like granules. Normal megakaryocytes are randomly dis-tributed among other hematopoietic cells, occasionallyreveal mature hematopoietic cells within their cytoplasm(emperipolesis), and only seldom make physical contactwith other megakaryocytes. Because megakaryocytesnormally comprise about 1:200 nucleated marrow cells,increase in the megakaryocytic compartment as in idio-pathic thrombocytopenic purpura and other reactivestates can be readily appreciated with a low power ob-jective. Megakaryocytes are PAS positive, and in PET,megakaryoblasts and megakaryocytes are FVIII related-antigen (von Willebrand factor), FXIII, CD41, and CD61positive by immunohistochemistry (81,82,83). This tech-nology is invaluable in establishing lineage identity inacute megakaryocytic leukemia (AML M-7), where blastforms may be indistinguishable from those of some otherforms of AML on H & E stains of PET (84,85). Immu-nohistochemistry also helps in the identification of dys-morphic, dysplastic, and micromegakaryocytic formsthat may be observed in the myeloproliferative and my-elodysplastic disorders (Fig. 10). It is noteworthy thatmegakaryocytes abut, cluster, sheet out, and reveal in-creased endoreduplication in essential thrombocythemia(Fig. 11). These features may be variably present in theother myeloproliferative disorders, but are less pro-nounced. Increased numbers of mature mononuclearmegakaryocytic forms may be observed in chronic my-eloid leukemia and the 5q− syndrome (86–89), and lossof nuclear lobulation with development of small discretenuclei (“pawn ball” forms) may be apparent in myelo-dysplasia on H&E sections in PET.
LYMPHOCYTES ANDLYMPHORETICULAR LESIONS
In the bone marrow of normal adults, lymphocytes aresmall, randomly interspersed between hematopoieticcells, and comprise between 8% and 24% of all nucleatedelements (44–47). The ratio of T-cells to B-cells is ap-proximately 3:1, and the CD4:CD8 ratio is approxi-mately 2:1. In pediatric samples, the total lymphocytecount is higher, and normal values up to 40% may beobserved (90). Labeled antibodies are now available
commercially, facilitating the evaluation of lymphocytesubsets in PET by IHC. Beyond the third decade, benignnonparatrabecular lymphoid aggregates may be observedand rarely may contain reactive germinal centers (91). Inaspirate smears, it is not uncommon to observe benignpolyclonal lymphoid aggregates as a monolayer of ma-ture lymphocytes.
In PET, monoclonal lymphoid infiltrates are usuallycharacteristic of involvement by a chronic lymphoid leu-kemia (5) or a low or intermediate grade nonHodgkinlymphoma. Rarely, follicle center cell lymphoma (FCL)first presents within the bone marrow in patients withcytopenia but without organomegaly or adenopathy. Theaspirate smears in these patients are commonly negative(92) but paratrabecular aggregates diagnostic of lym-phoma are found in the core (Fig. 12) and are CD20 andBCL2 positive (93). Such infiltrates may be accompa-nied by some reactive CD3-positive T-cells. In patientswith treated FCL, minimal residual (and occasionallyintertrabecular) deposits of tumor can be identified bysimilar IHC procedures. This may correlate with thepresence of a combined CD19, CD10, and BCL2 popu-lation of lymphocytes on flow cytometric analysis. Largecell lymphoma has appearances in the bone marrowcomparable to those seen in node-based biopsies (Fig.13). The presence of BCL6 activity in LCL serves todistinguish this lesion from blastic mantle cell lym-phoma.
Hodgkin lymphoma in the bone marrow (Fig. 14) isassociated with fibrosis, accounting for the rarity withwhich Reed-Sternberg cells are observed in aspiratepreparations (94–98). As with the nonHodgkin lympho-mas, bilateral core biopsies are recommended for stagingof Hodgkin lymphoma (21). The true identity of mono-nuclear Reed-Sternberg cells in the bone marrow can beestablished with antibodies specific for CD15 and CD30and other related immunostains (69).
In cases of bone marrow involvement by acute lym-phoblastic leukemia (Fig. 15) and the high-gradelymphomas (i.e., lymphoblastic lymphoma and Burkittlymphoma) (Fig. 15), the pattern of infiltration is invari-ably interstitial and diffuse (6). Correlation of the mor-phology with immunophenotypic, cytochemical, and cy-togenetic data is invaluable (99–101). The identificationof a minimal residual population of acute lymphoblasticleukemia (ALL) in PET can be achieved by immuno-staining for CD34 (Fig. 16), TdT, CD20, CD3, CD45RO,and additionally with molecular diagnostic studies forIgH, TCR gene rearrangement, and the identification ofabnormal genetic loci by PCR or FISH (Table 4). Also ofgreat importance is the distinction of acute lymphoblasticleukemia from hematogones (102). The latter are B-
J. D. COTELINGAM16
Advances in Anatomic Pathology, Vol. 10, No. 1, January, 2003
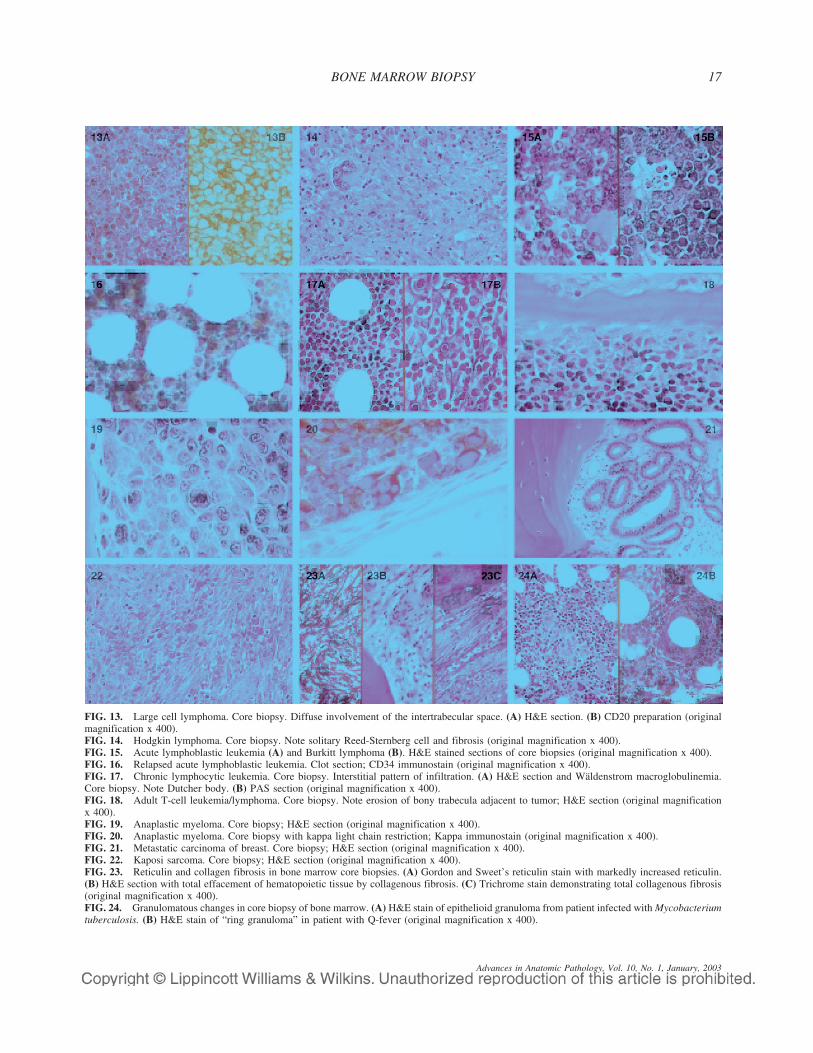
FIG. 13. Large cell lymphoma. Core biopsy. Diffuse involvement of the intertrabecular space. (A) H&E section. (B) CD20 preparation (originalmagnification x 400).FIG. 14. Hodgkin lymphoma. Core biopsy. Note solitary Reed-Sternberg cell and fibrosis (original magnification x 400).FIG. 15. Acute lymphoblastic leukemia (A) and Burkitt lymphoma (B). H&E stained sections of core biopsies (original magnification x 400).FIG. 16. Relapsed acute lymphoblastic leukemia. Clot section; CD34 immunostain (original magnification x 400).FIG. 17. Chronic lymphocytic leukemia. Core biopsy. Interstitial pattern of infiltration. (A) H&E section and Wäldenstrom macroglobulinemia.Core biopsy. Note Dutcher body. (B) PAS section (original magnification x 400).FIG. 18. Adult T-cell leukemia/lymphoma. Core biopsy. Note erosion of bony trabecula adjacent to tumor; H&E section (original magnificationx 400).FIG. 19. Anaplastic myeloma. Core biopsy; H&E section (original magnification x 400).FIG. 20. Anaplastic myeloma. Core biopsy with kappa light chain restriction; Kappa immunostain (original magnification x 400).FIG. 21. Metastatic carcinoma of breast. Core biopsy; H&E section (original magnification x 400).FIG. 22. Kaposi sarcoma. Core biopsy; H&E section (original magnification x 400).FIG. 23. Reticulin and collagen fibrosis in bone marrow core biopsies. (A) Gordon and Sweet’s reticulin stain with markedly increased reticulin.(B) H&E section with total effacement of hematopoietic tissue by collagenous fibrosis. (C) Trichrome stain demonstrating total collagenous fibrosis(original magnification x 400).FIG. 24. Granulomatous changes in core biopsy of bone marrow. (A) H&E stain of epithelioid granuloma from patient infected with Mycobacteriumtuberculosis. (B) H&E stain of “ring granuloma” in patient with Q-fever (original magnification x 400).
BONE MARROW BIOPSY 17
Advances in Anatomic Pathology, Vol. 10, No. 1, January, 2003
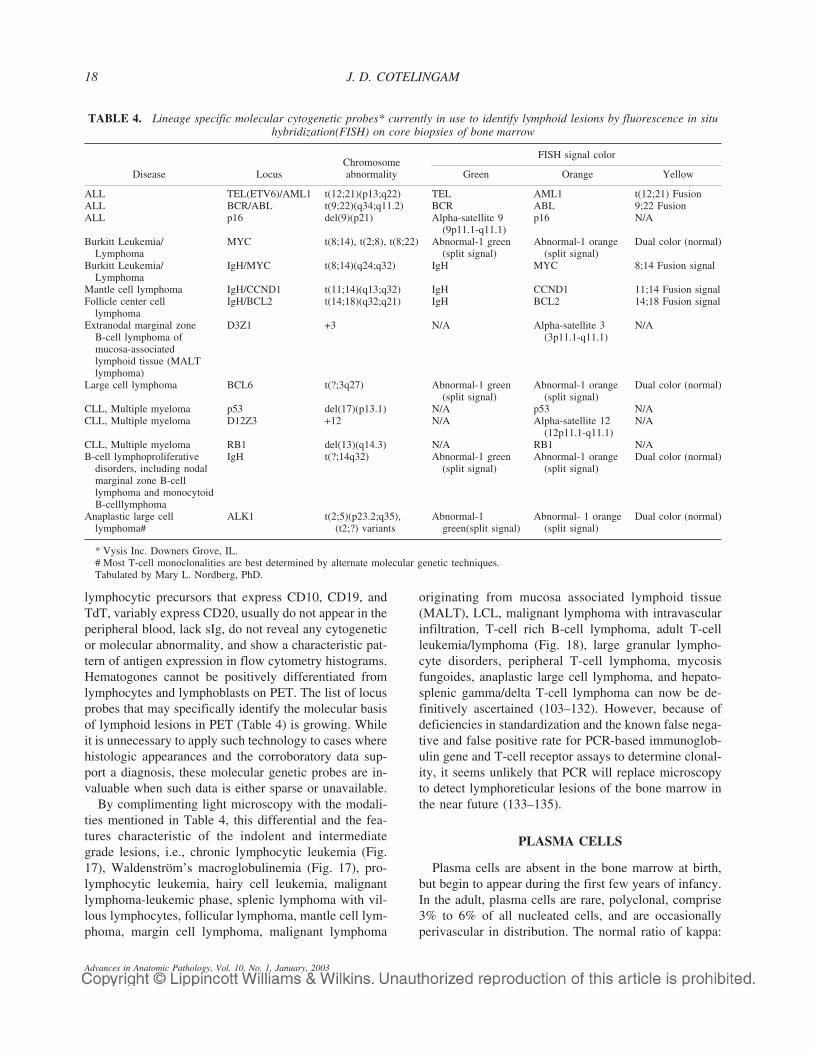
lymphocytic precursors that express CD10, CD19, andTdT, variably express CD20, usually do not appear in theperipheral blood, lack sIg, do not reveal any cytogeneticor molecular abnormality, and show a characteristic pat-tern of antigen expression in flow cytometry histograms.Hematogones cannot be positively differentiated fromlymphocytes and lymphoblasts on PET. The list of locusprobes that may specifically identify the molecular basisof lymphoid lesions in PET (Table 4) is growing. Whileit is unnecessary to apply such technology to cases wherehistologic appearances and the corroboratory data sup-port a diagnosis, these molecular genetic probes are in-valuable when such data is either sparse or unavailable.
By complimenting light microscopy with the modali-ties mentioned in Table 4, this differential and the fea-tures characteristic of the indolent and intermediategrade lesions, i.e., chronic lymphocytic leukemia (Fig.17), Waldenström’s macroglobulinemia (Fig. 17), pro-lymphocytic leukemia, hairy cell leukemia, malignantlymphoma-leukemic phase, splenic lymphoma with vil-lous lymphocytes, follicular lymphoma, mantle cell lym-phoma, margin cell lymphoma, malignant lymphoma
originating from mucosa associated lymphoid tissue(MALT), LCL, malignant lymphoma with intravascularinfiltration, T-cell rich B-cell lymphoma, adult T-cellleukemia/lymphoma (Fig. 18), large granular lympho-cyte disorders, peripheral T-cell lymphoma, mycosisfungoides, anaplastic large cell lymphoma, and hepato-splenic gamma/delta T-cell lymphoma can now be de-finitively ascertained (103–132). However, because ofdeficiencies in standardization and the known false nega-tive and false positive rate for PCR-based immunoglob-ulin gene and T-cell receptor assays to determine clonal-ity, it seems unlikely that PCR will replace microscopyto detect lymphoreticular lesions of the bone marrow inthe near future (133–135).
PLASMA CELLS
Plasma cells are absent in the bone marrow at birth,but begin to appear during the first few years of infancy.In the adult, plasma cells are rare, polyclonal, comprise3% to 6% of all nucleated cells, and are occasionallyperivascular in distribution. The normal ratio of kappa:
TABLE 4. Lineage specific molecular cytogenetic probes* currently in use to identify lymphoid lesions by fluorescence in situhybridization(FISH) on core biopsies of bone marrow
Disease LocusChromosomeabnormality
FISH signal color
Green Orange Yellow
ALL TEL(ETV6)/AML1 t(12;21)(p13;q22) TEL AML1 t(12;21) FusionALL BCR/ABL t(9;22)(q34;q11.2) BCR ABL 9;22 FusionALL p16 del(9)(p21) Alpha-satellite 9
(9p11.1-q11.1)p16 N/A
Burkitt Leukemia/Lymphoma
MYC t(8;14), t(2;8), t(8;22) Abnormal-1 green(split signal)
Abnormal-1 orange(split signal)
Dual color (normal)
Burkitt Leukemia/Lymphoma
IgH/MYC t(8;14)(q24;q32) IgH MYC 8;14 Fusion signal
Mantle cell lymphoma IgH/CCND1 t(11;14)(q13;q32) IgH CCND1 11;14 Fusion signalFollicle center cell
lymphomaIgH/BCL2 t(14;18)(q32;q21) IgH BCL2 14;18 Fusion signal
Extranodal marginal zoneB-cell lymphoma ofmucosa-associatedlymphoid tissue (MALTlymphoma)
D3Z1 +3 N/A Alpha-satellite 3(3p11.1-q11.1)
N/A
Large cell lymphoma BCL6 t(?;3q27) Abnormal-1 green(split signal)
Abnormal-1 orange(split signal)
Dual color (normal)
CLL, Multiple myeloma p53 del(17)(p13.1) N/A p53 N/ACLL, Multiple myeloma D12Z3 +12 N/A Alpha-satellite 12
(12p11.1-q11.1)N/A
CLL, Multiple myeloma RB1 del(13)(q14.3) N/A RB1 N/AB-cell lymphoproliferative
disorders, including nodalmarginal zone B-celllymphoma and monocytoidB-celllymphoma
IgH t(?;14q32) Abnormal-1 green(split signal)
Abnormal-1 orange(split signal)
Dual color (normal)
Anaplastic large celllymphoma#
ALK1 t(2;5)(p23.2;q35),(t2;?) variants
Abnormal-1green(split signal)
Abnormal- 1 orange(split signal)
Dual color (normal)
* Vysis Inc. Downers Grove, IL.# Most T-cell monoclonalities are best determined by alternate molecular genetic techniques.Tabulated by Mary L. Nordberg, PhD.
J. D. COTELINGAM18
Advances in Anatomic Pathology, Vol. 10, No. 1, January, 2003

lambda light chain producing cells is approximately 4:1as evaluated by flow cytometry and IHC (136). Plasmacells characteristically reveal intracytoplasmic immuno-globulin and are CD38 and CD138 positive and CD20negative. Increased numbers of polyclonal plasma cellsare observed in reactive states. However, when immu-noglobulin light chain restriction is observed, a plasmacell dyscrasia such as monoclonal gammopathy of unde-termined significance (MGUS) or multiple myeloma(Fig. 19) should be considered (136). In such cases,plasma cells often cluster and demonstrate cytologicatypia and light chain restriction on kappa and lambdaimmunostains in PET (Fig. 20). Several locus probes forthe prognostication of multiple myeloma in PET are nowavailable (Table 4). However, these may be of practicalvalue only in controversial or research settings.
Correlation of plasma cell counts with clinical, radio-logic, and biochemical parameters is of considerablevalue. In patients with abnormal lymphoplasmacytic in-filtrates, Waldenströms macroglobulinemia, heavy chaindisease, and amyloidosis additionally enter the differen-tial diagnosis (107,108,137). Plasma cells may occasion-ally reveal flame-like cytoplasmic transformation, bi-nuclearity, and crystalline inclusions (Snapper-Schneidbodies), features that are better appreciated on aspiratesmears (138–140). These changes may be observed inboth benign and malignant plasma cells. Because thelesions of multiple myeloma are focal in the bone mar-row, some authorities recommend bilateral core biopsiesat the time of initial investigation.
METASTATIC DISEASE
A large number of epithelial (Fig. 21) and mesenchy-mal (Fig. 22) tumors metastasize to the bone marrow(141,142). There is, however, considerable institutional,biologic, and specimen related variation in the incidenceof these lesions. Tumors that commonly metastasize tothe bone marrow include carcinomas of the breast, pros-tate, lung, and gastrointestinal tract in adults, and neuro-blastoma in children. Metastatic tumor deposits in thebone marrow may be detected in one or all of the speci-men components submitted for review (21). Occasion-ally, tumor deposits in the core biopsy are necrotic. Nev-ertheless, tumor cells variably retain their protein epit-opes and their true nature may be confirmed by their IHCprofile. Based on the architectural and cytologic patternof the tumor in question, a recommended battery of IHCstains should include but not be limited to cytokeratin,epithelial membrane antigen, carcinoembryonic antigen,alpha-fetoprotein, prostate specific antigen, prostaticacid phosphatase, HMB-45, S-100, leukocyte commonantigen (CD45), chromogranin, synaptophysin, CD99,
neuron-specific enolase, Leu-7, smooth muscle actin,desmin, vimentin, and FVIII related-antigen (143–146).Semiquantitation of tumor burden as a percentage ofbone marrow cellularity or medullary space involvedconveys additional meaning in the pathologic report.
RETICULIN AND COLLAGENPROLIFERATION
Normally, a delicate filigree of reticulin (type III col-lagen) is found to pervade the stroma of the bone mar-row, encircle fat cells and vascular structures, and sepa-rate cellular bone marrow from adjoining bony trabecu-lae. In core biopsy and aspirate clot sections, reticulincan be demonstrated with a good Wilder or Jones stain,and is reported as normal or increased. The latter may begraded as mild, moderate, or marked (Fig. 23). Reticulinproliferation is usually antecedent to collagen (type Icollagen) deposition. The latter may be suspected by itscoarse fiber pattern in H&E sections (Fig. 23), but shouldbe confirmed with a trichrome (Fig. 23) or other collagenstain. Because of its inaspirable nature, collagen fibrosisis not accurately quantifiable in aspirate clot sections andshould be evaluated only in the core biopsy.
Myelofibrosis may be acute or chronic, and idiopathicor secondary to myeloproliferative, lymphoproliferative,metastatic, or granulomatous disease (147–150). Slowlyprogressive fibrosis, as evident in the early stages ofagnogenic myeloid metaplasia and established polycy-themia vera, causes sinusoids in the bone marrow topermanently dilate and develop intravascular hematopoi-esis. These changes may also be observed in the othermyeloproliferative disorders. In contrast, rapidly pro-gressive fibrosis replaces hematopoietic tissue, vascularelements, stroma, and fat, resulting in obliteration of themarrow space.
Grading of bone marrow reticulin and collagen may bequantitated according to the Bauermeister Scale (151)(Table 5). The limits of normality lie between grades 0and 2.
TABLE 5. The Bauermeister scale for grading bonemarrow reticulin and collagen
Grade Morphologic features
0 No reticulin fibers demonstrable.1 Occasional fine individual fibers and foci of a fine fiber
network.2 Fine fiber network throughout most of the section. No coarse
fibers present.3 Diffuse fiber network with scattered thick coarse fibers. No
mature collagen present.4 Diffuse and often coarse fiber network with areas of
collagenization.
BONE MARROW BIOPSY 19
Advances in Anatomic Pathology, Vol. 10, No. 1, January, 2003

INFECTIONS ANDGRANULOMATOUS CHANGES
A wide range of infections localize to the bone mar-row (152), and may result in an inflammatory, necrotiz-ing, or granulomatous response. Intact granulomas areseldom observed in aspirate preparations, and their pres-ence cannot be excluded if the aspirate is the only speci-men available for evaluation. Granulomatous changes(Fig. 24) may be specific or nonspecific (150,153), andare best defined in the core biopsy and clot section. It isnecessary to work up all epithelioid granulomas withacid fast and fungus stains, and correlate changes withthe results of microbial cultures (154). In immunocom-promised patients, well-defined granulomas may fail todevelop. Under these circumstances, proliferation of mi-crobial-laden macrophages (as in Mycobacteriumavium–intracellulare infection) may be evident (155)(Fig. 25). The most frequently encountered granuloma inclinical practice is the nonspecific lipid granuloma (156).The latter are not associated with hematologic disease,and do not require work up with microbial stains. It isnoteworthy that the amastigote forms of leishmaniasisand the intranuclear viral inclusions of cytomegalovirus(Fig. 26), herpes simplex and parvovirus B19 infection(Fig. 27) are readily detected with a high dry lens andmay be confirmed by in situ hybridization if necessary(157).
STAINABLE IRON STORES
Quantitation of stainable iron in the bone marrow ismost accurately interpreted in Prussian blue preparationsof the aspirate smear and clot section. The choice be-tween manual and automated stains (BioGenex Labora-tories, San Ramon, CA) is largely parochial and work-load related. Decalcification, a prerequisite for prepara-tion of the core biopsy, results in leaching out of somestorage iron. Despite this drawback, evaluation of iron inthe core biopsy is informative in cases where the aspirateand clot sections were not procured or are dilute anddevoid of particles. Assessment on a scale of 0 to 4 plusis both simple and reproducible (158,159). In this scale,stainable iron is designated as follows: 0 � absent, 1 �trace/decreased, 2 to 3 � adequate, and 4 � increased(Fig. 28). In the bone marrow, elemental iron can bevisualized in several compartments, including the cyto-plasm of macrophages, in developing normoblasts (sid-eroblasts), and as free hemosiderin deposits within thebone marrow stroma. Reports should include descrip-tions of both the quantity and the location of iron, and
also the results of a search for pathologic sideroblastsincluding ring forms.
DISORDERS OF THE MACROPHAGE SYSTEM
Normally, monocytes and macrophages comprise upto 3% of cellular elements in the marrow (Table 2). InH&E stained sections of PET, monocytes cannot be posi-tively identified. Nevertheless, by immunostaining forCD68, lysozyme, alpha-1-antitrypsin, and alpha-1-antichymotripsin, infiltrates of this lineage, as in AML-M4, AML-M5, and CMML, can be designated (56). Oc-casional tingible body macrophages can be encounteredin cellular marrow, and do not connote a pathologic pro-cess. However, an abnormal macrophage componentmay be observed in Gaucher disease (160) (Fig. 29),CML (161,162) (pseudo-Gaucher cells), the hemophago-cytic syndromes (163), oxalosis (164–166) (Fig. 30),with thorotrast deposits (167) (Figure 31), sea-blue his-tocytosis, and in the acquired and inherited lipidosis(168). In each of these conditions, correlation with theclinical picture and related laboratory data is invaluable.
STROMAL AND VASCULAR ABNORMALITIES
Stromal cells and the mesenchyme of the extracellularmatrix are located between fat cells, and surround bothnonhematopoietic and hematopoietic tissue (169). Thelatter are decreased in hypoproliferative states, and arevirtually effaced by chemotherapy, an index of adequatetherapeutic induction in acute leukemia. Replacement ofhematopoietic tissue by mucopolysaccharide with com-mensurate atrophy of fat cells is observed in serous fatatrophy (170). Herein, the mucopolysaccharide can bedelineated with an Alcian Blue stain (Fig.3). It is impor-tant that the patterns of aplasia, serous fat atrophy, andadequate therapeutic induction of the acute leukemias beso designated.
Nutrient arteries, veins, and intervening sinusoids arealso located in the stromal compartment. Lesions thataffect larger vessels, which may be incidentally ob-served, are those of amyloid infiltration (171) (Fig. 32),vasculitis, (172) and thrombotic thrombocytopenic pur-pura (TTP) (6). It is noteworthy that sinusoidal dilatationis associated with increased stromal reticulin and colla-gen as in the cellular phase of agnogenic myeloid meta-plasia, and is occasionally accompanied by intrasinusoi-dal hematopoiesis (6,173,174) (Fig. 33).
DISORDERS OF TRABECULAR BONE
Although a core biopsy may have been procured toevaluate hematologic disease, the bony component of
J. D. COTELINGAM20
Advances in Anatomic Pathology, Vol. 10, No. 1, January, 2003

FIG. 25. Mycobacterium avium-intracellulare in the core biopsy of a terminal patient with the acquired immunodeficiency syndrome. (A) H&Esection with marked histiocytic proliferation. (B) Fite stain with numerous acid-fast bacteria within histiocytes (original magnification x 400).FIG. 26. Cytomegalovirus inclusion. Core biopsy in patient with acquired immunodeficiency syndrome. Nature of inclusion serologically andimmunohistochemically confirmed; H&E section (original magnification x 400) (Courtesy of Dr. Diana Veillon).FIG. 27. Parvovirus B19 inclusions in early erythroid precursors. Core biopsy. Patient with acquired immunodeficiency syndrome. Nature ofinclusions confirmed by serology and in-situ hybridization; H&E section (original magnification x 400).FIG. 28. Increased (4+) iron stores. Core biopsy. Patient with anemia of chronic disease; Prussian blue stain (original magnification x 400).FIG. 29. Gaucher disease. Core biopsy; H&E section (original magnification x 400).FIG. 30. Oxalosis. Core biopsy; H&E section (original magnification x 400) (Courtesy of Dr. Richard Brunning).FIG. 31. Thorotrast deposits. Core biopsy; H&E section (original magnification x 400).FIG. 32. Amyloid deposits. Core biopsy. (A) Congo-red preparation. (B) Birefringent appearances of amyloid with polarized light (originalmagnification x 400).FIG. 33. Intrasinusoidal hematopoiesis. Core biopsy. Patient with agnogenic myeloid metaplasia; H&E stain (original magnification x 400).FIG. 34. Increased osteoblastic activity in the vicinity of metastatic carcinoma of the prostate. Core biopsy; H&E section (original magnificationx 400).FIG. 35. Renal osteodystrophy. Core biopsy; H&E section (original magnification x 400).FIG. 36. Paget disease. Core biopsy; H&E section (original magnification x 400) (Courtesy of Dr. Tuyethoa Vinh).
BONE MARROW BIOPSY 21
Advances in Anatomic Pathology, Vol. 10, No. 1, January, 2003

this specimen should be routinely assessed. It has beenestimated that the volume of cortical and trabecular bonein an iliac crest bone biopsy comprises greater than 20%of the specimen (175); and despite physiologic variancesrelated to gender, race, and age, the mean trabecularwidth is approximately 200 microns (175,176). Cancel-lous bone of the iliac crest is in dynamic equilibriumwith the rest of the skeleton, and offers protection to thetissues within the labyrinthine marrow space. Trabecularbone is lamellar, and is variably bordered by a slenderosteoid seam. Osteoblasts (Fig. 34) and osteoclasts arelocated along the margins of trabeculae. These cells ef-fectively maintain the structural and physiologic integ-rity of bone when dispersed in a ratio of approximately100:1. Variations in this ratio along with changes in thestructure of trabecular bone may be observed in previousbiopsy sites, renal osteodystrophy (177,178) (Fig. 35),osteopenia, osteomalacia, (179) osteoporosis, (180)Paget disease, (181) (Fig. 36) and osteopetrosis (182).These lesions should be appropriately described and des-ignated in the pathology report.
SUMMARY
Reporting takes many forms, and is understandablyparochial. Whatever the choice, accuracy, clarity, brev-ity, and timeliness are paramount. A summary commentfollowing the microscopic description and diagnosticline which ties together other ancillary aspirate related,cytochemical, flow cytometric, molecular diagnostic,and other clinicopathologic data gleaned during the workup conveys depth to the report. This is invaluable forpurposes of prognostication, teaching, coding, retrieval,and research in keeping with local needs and philoso-phies. It is our practice to promptly appraise clinicalpersonnel by telephone of lesions and changes that areunexpected or have immediate therapeutic impact. Thisbrings excellence in communication and service and alsokeeps the pathologist abreast of clinical events.
ACKNOWLEDGMENT
The author thanks Ms. Bettie Crisler for secretarialsupport.
REFERENCES
1. Neumann E. Uber die Bedetung des Knochenmarks fur die Blut-building. Centralblatt Med Wiss 1868;6:689.
2. Bizzozero G. Sulla fungione ematopoietica del midollo delleossa. Zentralbl Med Wissensch 1868;6:885.
3. Mosler F. Klinische Symptome und Therapie der MedullalärenLeukemi. Berl Klin Wochenschr 1876;13:233.
4. Turkel H, Bethell FH. Biopsy of bone marrow performed by anew and simple instrument. J Lab Clin Med 1943;28:1246–1251.
5. Cotelingam JD. Bone marrow interpretation: the science and theart. Pathol Case Rev 2000;5:239–251.
6. Foucar K. Bone Marrow Pathology. 2nd ed. Chicago: AmericanSociety of Clinical Pathologists Press; 2001.
7. McFarland W, Damashek W. Biopsy of the bone marrow with theVim-Silverman needle. JAMA 1958;166:1464–1466.
8. Jamshidi K, Swaim WR. Bone marrow biopsy with unalteredarchitecture. A new biopsy device. J Lab Clin Med 1971;77:2335–2342.
9. Islam A. Bone marrow biopsy needle with core securing device.J Clin Pathol 1982;35:359–364.
10. MananTM bone marrow/aspiration needle MD TechR [packageinsert]. Gainsville, FL: Medical Device Technologies, Inc.; 1998.
11. Anderson G, Coup AJ. Effects of decalcifying agents on thestaining of Mycobacterium tuberculosis. J Clin Pathol 1975;28:744–745.
12. Wong FTS, Wu PC. The influence of decalcifying fluids on thedemonstration of Mycobacterium tuberculosis in paraffin sec-tions. Med Lab Sciences 1979;36:153–157.
13. Krause JR. Zenker-glacial acidic acid treatment of bone marrowbiopsies. In: Bone Marrow Biopsy. New York: Churchhill Liv-ingston; 1981;209.
14. Arber DA, Johnson RM, Rainer PA, et al. The bone marrow agarsection: a morphologic and immunohistochemical evaluation.Mod Pathol 1993;6:592–598.
15. Islam A. Proposal for a classification of acute myeloid leukemiabased on plastic embedded bone marrow biopsy sections. LeukRes 1993;17:421–427.
16. Burns WA, Yook CR. Plastic sections and ultrastructural tech-niques in the evaluation of bone marrow pathology. HematolOncol Clin North Am 1988;2:525–536.
17. Breton-Gorius J, Reyes F. Ultrastructure of human bone marrowcell maturation. Int Rev Cytol 1976;46:251–321.
18. Ghadially FN. Ultrastruct Pathol of the Cell and Matrix. 3rd ed.Boston: Butterworths; 1988.
19. Zucker-Franklin D, Greaves MF, Grossi CE, Marmont AM. Atlasof Blood Cells. 2nd ed. Philadelphia: Lea & Febiger; 1988.
20. Wickramasinghe SN. Bone marrow. In: Histology for Patholo-gists. 2nd ed. Philadelphia: Lippincott-Raven; 1997:707–742.
21. Barekman CL, Fair KP, Cotelingam JD. Comparative utility ofdiagnostic bone marrow components: a 10-year study. Am JHematol 1997;56:37–41.
22. Aboul-Nasr R, Estey EH, Kantarjian HM, et al. Comparison oftouch imprints with aspirate smears for evaluating bone marrowspecimens. Am J Clin Pathol 1999;111:753–758.
23. Custer RP. An Atlas of the Blood and Bone Marrow. 2nd ed.Philadelphia: WB Saunders; 1974.
24. Beckstead JH. The bone marrow biopsy: a diagnostic strategy.Arch Pathol Lab Med 1986;110:175–179.
25. Brynes RK, McKenna RW, Sundberg RD. Bone marrow aspira-tion and trephine biopsy: an approach to a thorough study. Am JClin Pathol 1987;70:753–759.
26. Hyun BH, Gulati GL, Ashton JK. Bone marrow examination:techniques and interpretation. Hematol Oncol Clin N Am 1988;2:513–523.
27. Naeim F. Atlas of Bone Marrow and Blood Pathology. Philadel-phia: WB Saunders; 2001.
28. Li C-Y, Yam LT. Cytochemistry and immunohistochemistry inhematologic diagnosis. Hematol Oncol Clin North Am 1994;8:665–681.
29. Pileri SA, Roncador G, Ceccarelli C, et al. Immunohistochemistryof bone-marrow biopsy. Leuk Lymphoma 1997;26 (Suppl1):69–75.
30. Erber WN, Willis JI, Hoffman GJ. An enhanced immunohisto-chemical method for staining bone marrow trephine sections. JClin Pathol 1997;50:389–393.
31. van der Valk P, Mullink H, Huijens PC, et al. Immunohistochem-
J. D. COTELINGAM22
Advances in Anatomic Pathology, Vol. 10, No. 1, January, 2003
istry in bone marrow diagnosis. Value of a panel of monoclonalantibodies on routinely processed bone marrow biopsies. Am JSurg Pathol 1989;13:97–106.
32. D’Onofrio G, Zini G, Tommasi M, et al. Automated analysis ofbone marrow: routine implementation and differences from pe-ripheral blood. Lab Hematol 1998;4:71–79.
33. Fan G, Alvares C, Ismail S, et al. Quantitative and qualitativebone marrow analysis by the Cell-Dyn 4000 Hematologic Ana-lyzer. Mod Pathol 1999;12:190A.
34. Vos JA, Simurdak JH, Davis BJ, et al. Vortex disaggregation forflow cytometry: a tissue preserving method. Mod Pathol 1999;12:147A.
35. McCoy J, Keren DF. Current practices in clinical flow cytometry:a practice survey by the American Society of Clinical Patholo-gists. Am J Clin Pathol 1999;111:156–160.
36. Willman CL. Acute leukemias: a paradigm for the integration ofnew technologies in diagnosis and classification. Mod Pathol1999;12:218–228.
37. Hartsock R, Smith EB, Petty CS. Normal variations with aging inthe amount of hematopoietic tissue in bone marrow from theanterior iliac crest. Am J Clin Pathol 1965;43:326–331.
38. Gruppo RA, Lampkin BC, Granger S. Bone marrow cellularitydetermination: comparison of the biopsy, aspirate, and buffy coat.Blood 1977;49:29–31.
39. Fong TP, Okafor LA, Schmitz TH, et al. An evaluation of cellu-larity in various types of bone marrow specimens. Am J ClinPathol 1979;72:812–816.
40. Vaquez MH, Aubertin C. L’anémie pernicieuse d’après concep-tions actuelles. Bull Mem Soc Med Hop Paris 1904;21:288.
41. Osgood EE, Seaman AJ. The cellular composition of bone mar-row as obtained by sternal puncture. Physiol Rev 1939;24:105–114.
42. Wickramasinghe SN. Normal hematopoiesis. Cellular composi-tion of normal bone marrow. In: Blood and Bone Marrow. Sys-temic Pathology. 3rd ed. Edinburgh: Churchill Livingstone;1991;70.
43. Perkins SL. Examination of blood and bone marrow. In: Lee GR,Foerster J, Lukens J, Paraskevas F, Greer JP, Rodgers GM, eds.Wintrobe’s Clinical Hematology. 10th ed. Baltimore: Williams &Wilkins; 1999:1;9.
44. Clark P, Normansell DE, Innes DJ, et al. Lymphocyte subsets innormal bone marrow. Blood 1986;67:1600–1606.
45. Horny HP, Wehrmann M, Griesser H, et al. Investigation of bonemarrow lymphocyte subsets in normal, reactive, and neoplasticstates using paraffin-embedded biopsy specimens. Am J ClinPathol 1993;99:142–149.
46. O’Donnell LR, Alder SL, Balis UJ, et al. Immunohistochemicalreference ranges for B lymphocytes in bone marrow biopsy par-affin sections. Am J Clin Pathol 1995;104:517–523.
47. Algino KM, Thomason RW, King DE, et al. CD20 (Pan-B cellantigen) expression on bone marrow derived T-cells. Am J ClinPathol 1996;106:78–81.
48. Sternberg PA, Hill RJ. Platelets and megakaryocytes. In: Lee GR,Foerster J, Lukens J, Paraskevas F, Greer JP, Rodgers GM, eds.Wintrobe’s Clinical Hematology. 10th ed. Baltimore: Williams &Wilkins; 1999:1;615–660.
49. Wolf BC, Brady K, O’Murchadha MT, et al. An evaluation ofimmunohistologic stains for immunoglobulin light chains in bonemarrow biopsies in benign and malignant plasma cell prolifera-tions. Am J Clin Pathol 1990;94:742–746.
50. Harada H, Asaoku H, Kuramoto A, et al. Phenotypic difference ofnormal plasma cells from mature myeloma cells. Blood 1993;81:2658–2663.
51. Oski FA, Naiman JL. The bone marrow. In: Oski FA, Naiman JL,eds. Hematologic Problems in the Newborn. 3rd ed. Philadelphia:WB Saunders Co; 1982;20.
52. Naeim F. Pathology of Bone Marrow. 2nd ed. Baltimore: Wil-liams & Wilkins; 1997.
53. Pinkus GS, Pinkus JL. Myeloperoxidase: a specific marker formyeloid cells in paraffin sections. Mod Pathol 1991;4:733–741.
54. Horny HP, Campbell M, Steinke B, et al. Acute myeloid leuke-mia: immunohistochemical findings in paraffin-embedded bonemarrow specimens. Hum Pathol 1990;21:648–655.
55. Dunphy CH, Polski JM, Evans HL, et al. Evaluation of bonemarrow specimens with acute myelogenous leukemia for CD34,CD15, CD117, and myeloperoxidase. Arch Pathol Lab Med2001;125:1063–1069.
56. Warnke RA, Pulford KA, Pallesen G, et al. Diagnosis of myelo-monocytic and macrophage neoplasms in routinely processed tis-sue biopsies with monoclonal antibody KP1. Am J Pathol 1989;135:1089–1095.
57. Horny HP, Parwaresch MR, Lennert K. Bone marrow findings insystemic mastocytosis. Hum Pathol 1985;16:808–814.
58. Li WV, Kapadia SB, Sonmez-Alpan E, et al. Immunohistochem-ical characterization of mast cell disease in paraffin sections usingtryptase, CD68, myeloperoxidase, lysozyme, and CD20 antibod-ies. Mod Pathol 1996;9:982–988.
59. Horny HP, Sillaber C, Menke D, et al. Diagnostic utility of stain-ing for tryptase in patients with mastocytosis. Am J Surg Pathol1998;22:1132–1140.
60. Natkunam Y, Rouse RV. Utility of paraffin section immunohis-tochemistry for C-KIT (CD117) in the differential diagnosis ofsystemic mast cell disease involving the bone marrow. Am J SurgPathol 2000;24:81–91.
61. Hanson CA, Abaza M, Sheldon S, et al. Acute biphenotypicleukemia: immunophenotype and cytogenetic analysis. Br J Hae-matol 1993;84:49–60.
62. Gaffney RL, Lowrey MC, Sciotto CG. Acute lymphoblastic leu-kemia relapsing as acute myelogenous leukemia: the role of themixed lineage leukemia (MLL) gene. ASCP Check Sample HP-99, 1999.
63. Mangi MH, Salisbury JR, Mufti GJ. Abnormal localization ofimmature precursors in the bone marrow of myelodysplastic syn-dromes: current state of knowledge and future directions. LeukRes 1991;15:627–639.
64. Heaney ML, Golde DW. Myelodysplasia. N Engl J Med 1999;340:1649–1660.
65. Reddey VB. Topics in bone marrow biopsy pathology: role ofmarrow topography in myelodysplastic syndromes and evaluationof posttreatment and postbone marrow transplant biopsies. AnnDiagn Pathol 2001;5:110–120.
66. Orazi A, Albitar M, Heerema NA, et al. Hypoplastic myelodys-plastic syndromes can be distinguished from acquired aplasticanemia by CD34 and PCNA immunostaining of bone marrowbiopsy specimens. Am J Clin Pathol 1997;107:268–274.
67. Brunning R. The proposed WHO classification of MDS andMDS-related acute leukemias. Mod Pathol 1999;12:102.
68. Vardiman JW. Myelodysplastic/myeloproliferative disorders.Mod Pathol 1999;12:104–105.
69. Jaffe ES, Harris NL, Stein H, et al. Tumors of Hematopoietic andLymphoid Tissue (WHO Classification of Tumors: Pathology andGenetics). Lyon: IARC Press; 2001.
70. van Der Valden VH, te Marvelde JG, Hoogeveen PG, et al. Tar-geting of the CD33-calicheamicin immunoconjugate Myelotarg(CMA-676) in acute myeloid leukemia: in vivo and in vitro satu-ration internalization by leukemic and normal myeloid cells.Blood 2001;97:3197–3204.
71. Druker BJ, Talpaz M, Resta D, et al. Efficacy and safety of aspecific inhibitor of the BCR-ABL tyrosine kinase in chronicmyeloid leukemia. N Eng J Med 2001;334:1031–1037.
72. Hasserjian RP, Boecklin F, Parker S, et al. ST1571 (ImatinibMesylate) reduces bone marrow cellularity and normalizes mor-phologic features irrespective of cytogenetic response. Am J ClinPathol 2002;117:360–367.
73. Applebaum FR, Downing J, Willman C. The biology and therapyof acute myelogenous leukemia. Molecular detection and moni-toring of AML 1/ETO transcripts in AML with t(8;21). In: Kaus-
BONE MARROW BIOPSY 23
Advances in Anatomic Pathology, Vol. 10, No. 1, January, 2003

hansky K, McArthur JR, eds. Hematology Education Program,American Society of Hematology. Seattle: Smith, Bucklin & As-sociates; 1995;23–35.
74. Kowal-Vern A, Cotelingam JD, Schumacher HR. The prognosticsignificance of pronormoblasts in acute leukemia. Am J ClinPathol 1992;98:34–40.
75. Mazzella FM, Cotelingam JD, Kowal-Vern A, et al. ProposedWHO classification of acute myeloid leukemia and myelodys-plastic syndromes. Mod Pathol 2000;13:101–102.
76. Strauchen JA. B19 Parvovirus infection. In: Diagnostic Histopa-thology of the Bone Marrow. New York: Oxford UniversityPress; 1996;282–285.
77. Lee GR. Congenital dyserythropoietic anemias. In: Lee GR,Foerster J, Lukens J, Paraskevas F, Greer JP, Rodgers GM, eds.Wintrobe’s Clinical Hematology. 10th ed. Baltimore: Williams &Wilkins; 1999:2;1489–1496.
78. Mazzela FM, Kowal-Vern A, Shrit A, et al. Erythroleukemia.Evaluation of 48 cases with reference to classification, cell pro-liferation, cytogenetics and prognosis. Am J Clin Pathol 1998;110:590–598.
79. Crocker J, Gyde O, Jenkins R. Demonstration of normoblasts intissue sections by means of an immunohistochemical techniquefor haemoglobin. J Clin Pathol 1984;37:1312–1313.
80. Sternberg PA. Hill RJ. Platelets and megakaryocytes. In: Lee GR,Foerster J, Lukens J, Paraskevas F, Greer JP, Rodgers GM, eds.Wintrobe’s Clinical Hematology. 10th ed. Baltimore: Williams &Wilkins; 1999:1;615–660.
81. Innes DJ, Mills SE, Walker GK. Megakaryocytic leukemia: iden-tification using antifactor VIII immunoperoxidase. Am J ClinPathol 1982;77:107–110.
82. Calapso P, Vitarelli E, Crisafulli C, et al. Immunocytochemicaldetection of megakaryocytes by endothelial markers: a compara-tive study. Pathologica 1992;84:215–223.
83. Chuang SS, Yung YC, Li CY. Von Willebrand factor is the mostreliable immunohistochemical marker for megakaryocytes of my-elodysplastic syndrome and chronic myeloproliferative disorders.Am J Clin Pathol 2000;113:506–511.
84. Huang MJ, Li CY, Nichols WL, et al. Acute leukemia with mega-karyocytic differentiation: a study of 12 cases identified immu-nocytochemically. Blood 1984;64:427–439.
85. San Miguel JF, Gonzalez M, Canizo MC, et al. Leukemias withmegakaryoblastic involvement: clinical, hematologic, and immu-nologic characteristics. Blood 1988;72:402–407.
86. Ivanyi JL, Kiss A, Telek B, et al. Megakaryocyte markers inmyeloproliferative disorders. Acta Histochem 1993;95:79–88.
87. Jacobson S, Wadenvik H, Kutti J, et al. Low megakaryocyteploidy in Ph+ chronic myeloid leukemia measured by flow cy-tometry. Am J Clin Pathol 1999;111:185–190.
88. Boultwood J, Lewis S, Waincoat JS. The 5q− syndrome. Blood1994;84:3253–3260.
89. van den Berghe H, Michaux L. 5q−, twenty five years later:asynopsis. Cancer Genet Cytogenet 1997;94:1–7.
90. Rosse C, Kraemer MJ, Dillon TL, et al. Bone marrow cell popu-lations of normal infants: the predominance of lymphocytes. JLab Clin Med 1977;89:1225–1240.
91. Farhi DC. Germinal centers in bone marrow. Hematol Pathol1989;3:133–136.
92. Lambertenghi-Deliliers G, Annaloro C, Soligo D, et al. Incidenceand histologic features of bone marrow involvement in malignantlymphomas. Ann Hematol 1992;65:61–65.
93. Ben-Ezra JM, King BE, Harris AC, et al. Staining for Bcl-2protein helps to distinguish benign from malignant lymphoid ag-gregates in bone marrow biopsies. Mod Pathol 1994;7:560–564.
94. O’Carroll DI, McKenna RW, Brunning RD. Bone marrow mani-festations of Hodgkin’s disease. Cancer 1976;38:1717–1728.
95. Bartl R, Frisch B, Burnhardt R, et al. Assessment of bone marrowhistology in Hodgkin’s disease: correlation with clinical factors.Br J Haematol 1982;51:345–360.
96. Karcher DS. Clinically unsuspected Hodgkin disease presenting
initially in the bone marrow of patients infected with the humanimmunodeficiency virus. Cancer 1993;71:1235–1238.
97. Naughton MJ, Hess JL, Zutter MM, et al. Bone marrow stagingin patients with nonHodgkin’s lymphoma. Is flow cytometry auseful test? Cancer 1998;82:1154–1159.
98. Munker R, Hasencleaver D, Brosteanu O, et al. Bone marrowinvolvement in Hodgkin’s disease: an analysis of 135 consecutivecases. J Clin Oncol 1995;13:403–409.
99. Schumacher HR. Acute Leukemia: Difficult, Controversial andAutomated Analysis. Baltimore: Williams & Wilkins; 1997.
100. Orazi A, Cotton J, Cattoretti G, et al. Terminal deoxynucleotidyltransferase staining in acute leukemia and normal bone marrow inroutinely processed paraffin sections. Am J Clin Pathol 1994;102:640–645.
101. Kheiri SA, MacKerrell T, Bonagura VR, et al. Flow cytometrywith or without cytochemistry for the diagnosis of acute leuke-mias. Cytometry 1998;34:82–86.
102. Davis RE, Longacre TA, Cornbleet PJ. Hematogones in the bonemarrow of adults. Immunophenotypic features, clinical settingsand differential diagnosis. Am J Clin Pathol 1994;102:202–211.
103. Foucar K. Chronic lymphoid leukemias and lymphoproliferativedisorders. Mod Pathol 1999;12:141–150.
104. Gala J-L, Guiot Y, Delannoy A, et al. Use of image analysis andimmunostaining of bone marrow trephine biopsy specimens toquantify residual disease in patients with B-cell chronic lympho-cytic leukemia. Mod Pathol 1999;12:391–399.
105. Shapiro JL, Miller ML, Pohlman B, et al. CD5− B-cell lympho-proliferative disorders presenting in blood and bone marrow. Aclinicopathologic study of 40 patients. Am J Clin Pathol 1999;111:477–487.
106. Tworek JA, Singleton TP, Schnitzer B, et al. Flow cytometric andimmunohistochemical analysis of small lymphocytic lymphoma,mantle cell lymphoma, and plasmacytoid small lymphocytic lym-phoma. Am J Clin Pathol 1998;110:582–589.
107. Andriko JA, Aguilera NS, Chu WS, et al. Waldenström’s mac-roglobulinemia: a clinicopathologic study of 22 cases. Cancer1997;80:1926–1935.
108. Owen RG, Barrans SL, Richards SJ, et al. Waldenströms macro-globulinemia: development of diagnostic criteria and identifica-tion of prognostic factors. Am J Clin Pathol 2001;116:420–428.
109. Schlette EJ, Buesco-Ramos CE, Medeiros LJ. B-cell prolympho-cytic leukemia. Pathol Case Rev 2000;5:274–280.
110. Schumacher HR, Cotelingam JD. T-Prolymphocytic leukemia.In: Chronic Leukemia: Approach to Diagnosis. New York: Igaku-Shoin; 1993;269–280.
111. Hounieu H, Chittal SM, AL Saati T, et al. Hairy cell leukemia.Diagnosis of bone marrow involvement in paraffin-embeddedsections with monoclonal antibody DBA 44. Am J Clin Pathol1992;98:26–33.
112. Pittaluga S, Tierens A, Dodoo YL, et al. How reliable is histo-logic examination of bone marrow trephine biopsy specimens forthe staging of nonHodgkin’s lymphoma? A study of hairy cellleukemia and mantle cell lymphoma involvement of the bonemarrow trephine specimen by histologic immunohistochemical,and polymerase chain reaction techniques. Am J Clin Pathol1999;111:179–184.
113. Troussard X, Valensi F, Duchayne E, et al. Splenic lymphomawith villous lymphocytes: clinical presentation, biology and prog-nostic factors in a series of 100 patients. Br J Haematol 1996;93:731–736.
114. McCluggage WG, Bharucha H, el-Agnaf M, et al. B-cell signetring cell lymphoma of bone marrow. J Clin Pathol 1995;48:275–278.
115. Vasef MA, Medeiros LJ, Koo C, et al. Cyclin D1 immunohisto-chemical staining is useful in distinguishing mantle cell lym-phoma from other low grade B-cell neoplasms in bone marrow.Am J Clin Pathol 1997;108:302–307.
116. Kent SA, Variakojis D, Peterson LC. Comparative study of mar-
J. D. COTELINGAM24
Advances in Anatomic Pathology, Vol. 10, No. 1, January, 2003

gin zone lymphoma involving bone marrow. Am J Clin Pathol2002;117:698–708.
117. Traweek ST, Sheibani K. Monocytoid B-cell lymphoma withbone marrow and peripheral blood involvement at presentation.Am J Clin Pathol 1990;94:117–118.
118. Hodges GF, Lenhardt TM, Cotelingam JD. Bone marrow in-volvement in large cell lymphoma. Prognostic implications ofdiscordant disease. Am J Clin Pathol 1994;101:305–311.
119. Jones D. Large B-cell lymphoma in the bone marrow. PatholCase Rev 2000;5:281–286.
120. Franco V. Florena AM, Campesi G. Intrasinusoidal bone marrowinfiltration: a possible hallmark of splenic lymphoma. Histopa-thology 1996;29:571–575.
121. Tucker TJ, Bardales RH, Miranda RN. Intravascular lymphoma-tosis with bone marrow involvement. Arch Pathol Lab Med 1999;123:952–956.
122. Khalidi HS, Brynes RK, Browne P, et al. Intravascular largeB-cell lymphoma: the CD5 antigen is expressed by a subset ofcases. Mod Pathol 1998;11:983–988.
123. Estalilla OC, Koo CH, Brynes RK, et al. Intravascular large B-cell lymphoma: a report of five cases initially diagnosed by bonemarrow biopsy. Am J Clin Pathol 1999;112:255.
124. Skinnider BF, Connors JM, Gascoyne RD. Bone marrow involve-ment in T-cell rich B-cell lymphoma. Am J Clin Pathol 1997;108:570–578.
125. Ogata M, Ogata Y, Kohno K, et al. Eosinophilia associated withadult T-cell leukemia: role of interleukin-5 and granulocyte-macrophage colony-stimulating factor. Am J Hematol 1995;59:242–245.
126. Evans HL, Burks E, Viswantatha D, et al. Utility of immunohis-tochemistry in bone marrow evaluation of T-lineage large granu-lar lymphocyte leukemia. Hum Pathol 2000;31:1266–1273.
127. Hanson CA, Brunning RD, Gajl-Peczalska KJ, et al. Bone mar-row manifestations of peripheral T-cell lymphoma. A study of 30cases. Am J Clin Pathol 1986;86:449–460.
128. Gaulard P, Kanavaros P, Farcet JP, et al. Bone marrow histologicand immunohistochemical findings in peripheral T-cell lym-phoma: a study of 38 cases. Hum Pathol 1991;22:331–338.
129. Graham SJ, Sharpe RW, Steinberg SM, et al. The prognosticimplications of a bone marrow histopathologic classification sys-tem in mycosis fungoides and the Sézary syndrome. Cancer1993;72:726–734.
130. Salhany KE, Greer JP, Cousar JB, et al. Marrow involvement incutaneous T-cell lymphoma. Am J Clin Pathol 1989:92;747–754.
131. Fraga M, Brosset P, Schaifer D, et al. Bone marrow involvementin anaplastic large cell lymphoma. Immunohistochemical detec-tion of minimal disease and it’s prognostic significance. Am JClin Pathol 1995;103:82–89.
132. Vega F, Medeiros LJ, Bueso-Ramos C, et al. Hepatosplenicgamma/delta T-cell lymphoma in bone marrow. A sinusoidal neo-plasm with blastic cytologic features. Am J Clin Pathol 2001;116:410–419.
133. Coad JE, Olson DJ, Christensen DR, et al. Correlation of PCR-detected clonal gene rearrangements with bone marrow morphol-ogy in patients with B-lineage lymphoma. Am J Surg Pathol1997;21:1047–1056.
134. Medeiros LJ, Carr J. Overview of the role of molecular methodsin the diagnosis of malignant lymphoma. Arch Path Lab Med1999;123:1189–1207.
135. Fader S, Kurzrock R, Estrov Z. Minimal residual disease in he-matologic disorders. Arch Pathol Lab Med 1999;123:1030–1034.
136. Wolf BC, Brady K, O’Murchadha MT, et al. An evaluation ofimmunohistologic stains for immunoglobulin light chains in bonemarrow biopsies in benign and malignant plasma cell prolifera-tions. Am J Clin Pathol 1990;94:742–746.
137. Harada H, Asaoku H, Kuramoto A, et al. Phenotypic difference ofnormal plasma cells from mature myeloma cells. Blood 1993;81:2658–2663.
138. Thiry A, Delvenne P, Fontaine MA, et al. Comparison of bone
marrow sections, smears, and immunohistologic staining for im-munoglobulin light chains in the diagnosis of benign and malig-nant plasma cell proliferation. Histopathology 1993;22:423–428.
139. Snapper J, Schneid B. On the influence of stilbamidine uponmyeloma cells. Blood 1946;1:534–536.
140. Roberts GT, Khalil SH. Multiple myeloma with bone marrowcrystal deposition and marrow fibrosis. Ann Saudi Med 1998;18:432–436.
141. Singh G, Krause JR, Breitfeld V. Bone marrow examination formetastatic tumor: aspirate and biopsy. Cancer 1977;40:2317–2321.
142. Jatoi A, Dallal GE, Nguyen PL. False negative rates of tumormetastases in the histologic examination of bone marrow. ModPathol 1999;12:29–32.
143. Mansi JL, Berger U, Wilson P, et al. Detection of tumor cells inbone marrow of patients with prostatic carcinoma by immunocy-tochemical techniques. J Urol 1988;139:545–548.
144. Lazda EJ, Berry PJ. Bone marrow metastasis in Ewing’s sarcomaand peripheral primitive neuroectodermal tumor: an immunohis-tochemical study. Pediatric & Developmental Pathol 1998;1:125–130.
145. Mathieu MC, Friedman S, Bosq J, et al. Immunohistochemicalstaining of bone marrow biopsies for detection of occult metas-tasis in breast cancer. Breast Cancer Res Treat 1990;15:21–26.
146. Dabbs DJ. Diagnostic Immunohistochemistry. New York: Chur-chill Livingstone; 2002.
147. Hruban RH, Kuhajda FP, Mann RB. Acute myelofibrosis. Immu-nohistochemical study of four cases and comparison with acutemegakaryoblastic leukemia. Am J Clin Pathol 1987;88:578–588.
148. Rywlin AM. Myelofibrosis and osteosclerosis. In: Histopathol-ogy of the Bone Marrow. Boston; Little Brown & Co.; 1976;153.
149. Burthem J, Cawley JC. Bone marrow fibrosis of hairy cell leu-kemia is caused by synthesis and assembly of fibronectin matrixby hairy cells. Blood 1994;15:479–504.
150. Bhargava V, Farhi DC. Bone marrow granulomas. Clinicopath-ologic findings in 72 cases and review of the literature. HematolPathol 1988;2:43–50.
151. Bauermeister DE. Quantitation of bone marrow reticulin: a nor-mal range. Am J Clin Pathol 1971;56:24–31.
152. Diebold J, Molina T, Camilleri-Broët S, et al. Bone marrow mani-festations of infectious and systemic diseases observed in bonemarrow trephine biopsy. Histopathology 2000;37:199–211.
153. Tefferi A, Li CY. Bone marrow granulomas associated withchronic natural killer cell lymphocytosis. Am J Hematol 1997;54:258–262.
154. Volk EE, Miller ML, Kirkley BA, et al. The diagnostic usefulnessof bone marrow cultures in patients with fever of unknown origin.Am J Clin Pathol 1998;110:150–153.
155. Farhi DC, Mason III UG, Horsburgh Jr CR. The bone marrow indisseminated MAI infection. Am J Clin Pathol 1985;83:463–468.
156. Rywlin AM, Ortega R. Lipid granulomas of the bone marrow. AmJ Clin Pathol 1972;57:457–462.
157. Conner DH, Chandler FW, Schwartz DA, et al. Pathology ofInfectious Disease. Stamford: Appleton and Lange; 1997:1;255.
158. Strauchen JA. Interpretation of iron stores in the bone marrow. In:Diagnostic Histopathology of the Bone Marrow. Oxford: OxfordUniversity Press; 1996;16.
159. Rywlin AM. Bone marrow hemosiderin. In: Histopathology ofthe Bone Marrow. Boston: Little Brown & Co.; 1976;53–58.
160. Rector JT, Cotelingam JD. Gaucher’s disease. ASCP Check Path(Hematopathology) 1996; QAH 96–4.
161. Lee RE, Ellis LD. The storage cells of chronic myeloid leukemia.Lab Invest 1971;24:261–264.
162. Ulirsch RC. Sea Blue histiocytes in chronic myeloid leukemia.ASCP Check Sample 1985; H-4.
163. Brunning RD, McKenna RW. Infection associated hemophago-cytic syndrome. In: Rosai J, Sobin LH, eds. Atlas of Tumor Pa-thology, Bone Marrow. AFIP Fasicle. Washington DC; ArmedForces Institute of Pathology; 1994;9:447–452.
BONE MARROW BIOPSY 25
Advances in Anatomic Pathology, Vol. 10, No. 1, January, 2003

164. McKenna RW, Dehner LP. Oxalosis: an unusual cause of my-elophthisis in childhood. Am J Clin Pathol 1976;66:991–997.
165. Boquist L, Lindquist B, Ostberg Y, et al. Primary oxalosis. Am JMed 1973;54:673–681.
166. Gherardi G, Poggi A, Sisca S, et al. Bone oxalosis and renalosteodystrophy. Arch Pathol Lab Med 1980;104:105–111.
167. Graham SJ, Heaton RB, Garvin DF, Cotelingam JD. Whole bodypathologic analysis of a patient with thorotrast induced myelo-dysplasia. Health Phys 1992;63:20–26.
168. Kolodny EH, Tenembaum AL. Bone marrow involvement in stor-age diseases. In: Nathan DG, Orkin SH, eds. Nathan and Oski’sHematology of Infancy and Childhood. 4th ed. Philadelphia: WBSaunders Co; 1992;1452–1492.
169. Wilkins BS, Jones DB. Immunophenotypic characterization ofstromal cells in aspirated human bone marrow samples. Exp He-matol 1998;26:1061–1067.
170. Mehta K, Gascon P, Robboy S. The gelatinous bone marrow(serous atrophy) in patients with AIDS, evidence of excess sul-phated glycosaminoglycan. Arch Pathol Lab Med 1992;116:504–508.
171. Wolf BC, Kumar A, Vera JC, et al. Bone marrow morphologyand immunology in systemic amyloidosis. Am J Clin Pathol1986;86:84–88.
172. Rosenthal NS, Farhi DC. Bone marrow findings in connectivetissue disease. Am J Clin Pathol 1989;92:650–654.
173. Burkhardt R, Bartl R, Beil E, et al. Myelofibrosis-osteosclerosis
syndrome: a review of literature and histomorphology. Adv Biosci1975;16:9–56.
174. Wolf BC, Neiman RS. Myelofibrosis with myeloid metaplasia:pathophysiologic implications of the correlation between bonemarrow changes and progression of splenomegaly. Blood 1985;65:803–809.
175. Vigorita VJ. The bone biopsy protocol for evaluating osteoporo-sis and osteomalacia. Am J Surg Pathol 1984;8:925–930.
176. Frisch B, Bartl R. Biopsy Interpretation of Bone and Bone Mar-row. London: Arnold-Oxford University Press; 1999;27.
177. Teitelbaum SL. Renal osteodystrophy. Human Pathol 1984;15:306–323.
178. Wittels B. Renal osteodystrophy. In: Bennington JL, ed. SurgicalPathology of Bone Marrow: Core Biopsy Diagnosis. Philadel-phia: WB Saunders Co; 1985;133–136.
179. Bain BJ, Clark DM, Lampert IA. Osteomalacia. In: Bone MarrowPathology. London: Blackwell Scientific Publications; 1993;258–259.
180. Becks JS, Nordin BEC. Histological assessment of osteoporosisby the iliac crest biopsy. J Pathol Bacteriol 1960;80:391–397.
181. Frisch B, Lewis SM, Burkhardt R, et al. Paget’s disease of bone.In: Biopsy Pathology of Bone and Bone Marrow. New York:Raven Press; 1985;97–100.
182. Milgram JW, Jasty M. Osteopetrosis. A morphologic study oftwenty-one cases. J Bone Joint Surg Am 1982;64:912–929.
J. D. COTELINGAM26
Advances in Anatomic Pathology, Vol. 10, No. 1, January, 2003