
body cavity trauma - · PDF fileBasic Facts of Body Cavity Trauma zSecond most frequent cause...
65
BODY BODY CAVITY CAVITY TRAUMA TRAUMA
Transcript of body cavity trauma - · PDF fileBasic Facts of Body Cavity Trauma zSecond most frequent cause...

BODY BODY CAVITY CAVITY
TRAUMATRAUMA

Basic Facts of Body Cavity Basic Facts of Body Cavity TraumaTrauma
Second most frequent cause of motor-vehicle deathInjuries can be anticipated by assessing direction of forceEffects can be predicted by the organ system likely to be injuredAssessment, recognition of life-threatening conditions, and rapid transportation to a trauma center are the keys to proper care

Anatomy and PhysiologyAnatomy and Physiology
The thorax--both container and component of the respiratory process and site of major components of the circulatory systemThoracic cage– Bound and protected by musculoskeletal
structures– Expansion produces inspiration– Relaxation produces exhalation

Anatomy and PhysiologyAnatomy and Physiology
Mediastinum--central region of the chest that houses several structures vital to body function– Heart
PericardiumMajor vesselsAortic archLigamentum arteriosum

Anatomy and PhysiologyAnatomy and Physiology
– Trachea– Vena cava– Aorta– Esophagus

LungsLungsLungs--fill chest cavity on either side of the mediastinumRight lung, three lobes; left lung, two lobesPleura--double layer of tissueParietal and visceral pleuraLubricating fluid ensures lungs adhere to chest wall

AlveoliAlveoliMicroscopic chambers within lungs– Site of oxygen-carbon
dioxide exchange– 300 million– Give lungs spongy
compliance, volume, and light weight

Bellows systemBellows system
Skeletal muscles change volume of thoraxPleura causes chest walls and lungs to moveAlveoli respond to changes in thoracic volumeAirway permits air to move in and out of lungs

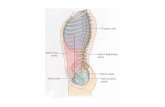
The abdomenThe abdomenAbdominal cavity– Diaphragm separates thorax from abdomen– Right upper quadrant contains
LiverRight kidneyGall bladderDuodenumPart of the pancreasPart of bowels

Left upper quadrant contains– Stomach, Left kidney, Spleen, Most of the
pancreas, Part of bowels

Left lower quadrant contains– Sigmoid colon, Part of bowels
Right lower quadrantcontains– Appendix– Part of bowels

Alimentary canalAlimentary canal
Continuous tube from esophagus to rectumHouses entire digestive systemMoves food via peristalsisNutrients taken, waste products removed

Accessory organsAccessory organsLiver– Metabolic regulation, hematological regulation,
bile productionPancreas– Secrete buffers, digestive enzymes, hormones
Spleen– Engulfs pathogens, immune response
Kidneys– Forms and concentrates urine

PeritoneumPeritoneum
Delicate covering for abdominal organsLubricating fluidMesentery--tissue that provides small bowel with support, circulation, innervationOmentum--tissue that insulates anterior abdomen from trauma and temperature extremes

Chest injuriesChest injuries
Bellows system compromise– Pain restricting chest excursion– Air entering pleural space– Chest wall failing to move in unison

Rib fracturesRib fractures
Most often caused by blunt trauma, bowing effect with midshaft fractureMost often elderly patientsRibs 4-9 are most often fractured (thin and poorly protected

Can produce respiratory restriction due to pain and splintingCan lead to atelectasis, ventilation/perfusion mismatchMay indicate underlying lung contusion

Flail chestFlail chest
History of frontal or lateral impactThree or more ribs fractured in 2 or more places, causing floating segmentParadoxical movement of flail segment, opposite to rest of chest

Flail chest careFlail chest care
Stabilize the floating segmentProvide positive pressure ventilation, if necessary

Pulmonary contusionPulmonary contusion
Damage to lung tissue causing bleeding and swellingReduces lung complianceIncreases respiratory effortInterferes with gas exchangeIncreases PaCO2, decreases pH

Closed pneumothoraxClosed pneumothoraxInternal wound allows air to enter the pleural spaceSmall tears self-seal, larger ones may progressPaper bag syndromeAir will accumulate in the apices, check there first for diminished breath soundsTrachea may tug toward the affected sideVentilation/perfusion mismatch

Open pneumothoraxOpen pneumothorax
Penetrating injury to the chest which does not seal itselfSucking chest woundOpen wound from chest wall to atmosphere

Air enters and exits the wound, no gas exchangeVena cava kinked from swaying of mediastinumPreload decreased from kinking of inferior vena cava

HemothoraxHemothorax
Blood enters pleural spaceShockIncreased dysneaDull to percussion

Thoracic trauma careThoracic trauma care
Soft-tissue injury careCover open wounds with occlusive dressingSecure on three sidesPlace patient on injured side if spinal cord injury not suspectedMonitor closely for signs of respiratory distress

Tension pneumothoraxTension pneumothorax
Caused by opening in chest wall or lungOne-way opening allows air to enter, but not exit, the pleural space, collapsing affected lungPressure progressively increases, pushing the mediastinum toward the unaffected sideInfringes on function of unaffected lung

Severe hypoxia and hypotension probableKinking of vena cava possible, venous return retardedExtreme dyspnea, circulatory collapsePleural space may fill with blood (hemothorax) Pneumohemothorax common

Tension pneumothorax careTension pneumothorax careEmergency needle decompression– 12 Gauge angiocath– Mid clavicular or mid axillary line– Over top of rib
Monitor for redevelopment of the conditionOxygen

Pericardial tamponadePericardial tamponade
Blood enters the pericardial space from penetrating or blunt traumaPassive filling of the heart is restricted, reducing preload significantlyCan also be caused by increasing pressure of tension pneumothorax

Pericardial tamponadePericardial tamponade
Decreasing pulse pressureShockMuffled heart sounds

Pericardial tamponade carePericardial tamponade care
A dire emergencyPerform pericardiocentesis, if trained

Traumatic aortic ruptureTraumatic aortic rupture

Traumatic aortic ruptureTraumatic aortic rupture
Sudden deceleration causes the aortic layers to break apartTears most often occur at the ligamentum arteriosumIf force is severe, aorta can tear, causing immediate exsanguinationVery high mortality for any aortic tears or aneurysm

Traumatic aortic aneurysm Traumatic aortic aneurysm carecare
Rapid and gentle transportTreat for shockIf ruptured, expect rapid exsanguination

Cardiac contusionCardiac contusion
Damage to myocardium causing bleeding and swellingReduces cardiac output

Cardiac contusion careCardiac contusion care
Treat as aggressively as an MI patientImplement cardiac protocolsAnticipate arrythymias or arrest

Injuries to other structures in Injuries to other structures in the mediastinumthe mediastinum
Aortic aneurysmEsophageal ruptureVena cava lacerationsTracheal tear– Air enters the neck, mediastinum– Can cause mediastinal shifting and tension
mediastinum

Diaphragmatic rupture– Tear in the diaphragm causes abdominal
contents to enter the thorax– Bowel sounds heard in thorax, respiratory
distress, hypoxia

Traumatic asphyxiaTraumatic asphyxia
Sudden compressional force squeezes the chest (e.g., auto seat and steering wheel)HypoventilationBlood backs up into the head and neckJugular veins engorge, capillaries rupturePatient presents with cyanotic upper body, bulging eyes, blue tongue

Traumatic asphyxia careTraumatic asphyxia care
Expect hypotension as tension is releasedTreat aggressively for shockExpect patient to deteriorate to cardiac arrestConsider sodium bicarbonate for potential acidosis

Abdominal InjuriesAbdominal Injuries

Penetrating traumaPenetrating trauma
Injury dependent upon penetrating object and organs involvedLiver, kidneys, spleen especially susceptible to injury from cavitational wave caused by high-speed projectilesCannot determine depth, pathway, or organs affected from entrance wound alone

EviscerationEvisceration
Rupture of abdominal wall that allows abdominal contents to escapeCan cause three harmful conditions– Interference with blood supply to
protruding bowel– Drying of bowel– Infection

Blunt traumaBlunt trauma
Solid organ injury– Contusions, lacerations, fractures of solid
organs– Rapid hemorrhage, exsanguination possible

Hollow organ injury– Rupture of hollow organs with spilling of
contents– Severe infection (peritonitis) possibleOther blunt trauma-related injuries– Tearing of blood vessels– Tearing of liver at ligamentum teres– Bladder, colon, or rectum rupture

Genitalia injuryGenitalia injuryFemale– Common cause--child molestation/rape– May present with severe internal/external bleeding
due to tearing from object forced into vagina
Male– Injuries more frequent than in females– Laceration may cause large blood loss– Blunt trauma may cause hematoma

Genitalia injury treatmentGenitalia injury treatment
Control bleedingTreat shockImmobilized impaled objects

Impaled object careImpaled object care
Immobilize as foundCover entry wound with sterile gauzeRemove object only if it interferes with CPR

Abdominal trauma careAbdominal trauma care
Transport immediately if internal bleeding is suggestedStart IV fluidsApply PASG and be ready to inflateReevaluate vital signs often

Penetrating abdominal injury Penetrating abdominal injury carecare
Cover open woundsCover eviscerations with wet, occlusive dressingsImmobilize objects in placeExamine for exit woundsTreat for shock aggressively

Blunt abdominal injury careBlunt abdominal injury care
Care is basically supportivePlace patient in comfortable positionTransport carefully to trauma center

AssessmentAssessment
Mechanism of injury– Analyze the extent of auto damage– Look for steering wheel deformity– Check for use of seatbelts/air bags

Primary assessmentPrimary assessment
Airway and breathing– "Look" for signs of chest trauma
Inspect the chest wall for asymmetry during ventilationInspiration should be slightly shorter than expiration
– "Listen" for abnormal sounds– "Feel" for air movement

Circulation– Check for signs of hypovolemia by assessing
Heart rate and qualitySkin conditionCapillary refill time
Disability– Look for altered level of consciousness from
hypoxia or circulatory compromise

Expose and examine theExpose and examine theNeck for– Jugular venous distention (tension
pneumothorax, pericardial tamponade, traumatic asphyxia, heart failure from myocardial contusion)
– Tracheal displacement (deviated away from injury in tension pneumothorax, tugging toward injury in simple pneumothorax or hemothorax

Chest for– Subcutaneous emphysema from airway rupture– Thoracic cage stability– Sucking chest wounds– Ecchymosis, soft tissue injuries which indicate
underlying tissue damage– Auscultation of lung fields for presence, equality,
adequacy of ventilations (diminished or absent lung sounds in pneumothorax or hemothorax, pulmonary edema from lung contusion)

Abdomen for– External signs of injury and exaggerated
abdominal wall movement (through inspection and palpation)
– Tenderness, guarding, rigidity, pulsating masses (through palpation)

Evaluate primary assessmentEvaluate primary assessment
Identify and treat life threatsProtect airway and ensure adequate ventilationsAdminister oxygenSeal any open woundsLimit movement of flail segmentsTreat aggressively for shockAssess need for immediate transport

Secondary assessmentSecondary assessment
Chest assessment– Inspection
Observe for symmetry of movementDetermine minute volume and adequacy of respiratory effortUse pulse oximetryAssess for signs of respiratory failure
– Palpation for crepitation, subcutaneous emphysema, deformities

– AuscultationFor equality and adequacy of air movementHeart sounds
– PercussionFor quality of soundFor equality of resonance

Abdominal assessmentAbdominal assessmentInspection for external signs of injuryPalpation for pain, tenderness, guarding, rigidityVital signs– Pulse rate, quality– Blood pressure
Pulse pressurePulsus paradoxus
– Respirations

Patient historyPatient history
Chief complaintThoracic symptoms (specifically ask about respiratory effort)Abdominal symptoms (carefully record location and quality of pain)

ManagementManagement
Stabilize the spineSecure an open airwayProvide ventilatory support with supplemental oxygenPASG if hypovolemic shock suspectedRapid transport if patient is criticalIV fluid replacement en routeReassess and monitor for signs of deterioration

Pain medicationPain medicationNitronox– 50/50 mixture of oxygen and nitrous oxide– Self-administered by mask– Short-acting agent (subsides in 2-5
minutes)– May cause side effects (nausea, vomiting)– May cause increased ICP– Rule out pneumothorax prior to use

Morphine sulfate– Narcotic analgesic– May be used to treat pain of isolated rib
fracture– May cause respiratory depression– Not used in head or abdominal injuries









![Diagnostic process and management of diaphragmatic ...septum, which separates the thorax from the abdomi-nal cavity.[1,2] ... penetrating trauma to the body account for approxi-mately](https://static.fdocuments.net/doc/165x107/609ace603235857e1d3e209b/diagnostic-process-and-management-of-diaphragmatic-septum-which-separates-the.jpg)






