
BMJ Open 2014 Iyngkaran
16
Northern Territory Heart Failure Initiative —Clinical Audit (NTHFI —CA) —a prospective database on the quality of care and outcomes for acute decompensated heart failure admission in the Northern Territory: study design and rationale Pupalan Iyngkaran, 1 Jeff Tinsley, 2 David Smith, 3 Mark Haste, 4 Kangaharan Nadarajan, 5 Marcus Ilton, 6 Malcolm Battersby, 7 Simon Stewart, 8 Alex Brown 9 To cite: Iyngkaran P, Tinsley J, Smith D, et al. Northern Territory Heart Failure Initiative—Clinical Audit (NTHFI—CA)—a prospective database on the quality of care and outcomes for acute decompensated heart failure admission in the Northern Territory: study design and rationale. BMJ Open 2014;4: e004137. doi:10.1136/ bmjopen-2013-004137 ▸ Prepublication history and additional material for this paper is available online. To view these files please visit the journal online (http://dx.doi.org/10.1136/ bmjopen-2013-004137). Received 1 October 2013 Revised 30 November 2013 Accepted 4 December 2013 For numbered affiliations see end of article. Correspondence to Dr Pupalan Iyngkaran; [email protected] ABSTRACT Introduction: Congestive heart failure is a significant cause of morbidity and mortality in Australia. Accurate data for the Northern Territory and Indigenous Australians are not presently available. The economic burden of this chronic cardiovascular disease is felt by all funding bodies and it still remains unclear what impact current measures have on preventing the ongoing disease burden and how much of this filters down to more remote areas. Clear differentials also exist in rural areas including a larger Indigenous community, greater disease burden, differing aetiologies for heart failure as well as service and infrastructure discrepancies. It is becoming increasingly clear that urban solutions will not affect regional outcomes. To understand regional issues relevant to heart failure management, an understanding of the key performance indicators in that setting is critical. Methods and analysis: The Northern Territory Heart Failure Initiative—Clinical Audit (NTHFI-CA) is a prospective registry of acute heart failure admissions over a 12-month period across the two main Northern Territory tertiary hospitals. The study collects information across six domains and five dimensions of healthcare. The study aims to set in place an evidenced and reproducible audit system for heart failure and inform the developing heart failure disease management programme. The findings, is believed, will assist the development of solutions to narrow the outcomes divide between remote and urban Australia and between Indigenous and Non-Indigenous Australians, in case they exist. A combination of descriptive statistics and mixed effects modelling will be used to analyse the data. Ethics and dissemination: This study has been approved by respective ethics committees of both the admitting institutions. All participants will be provided a written informed consent which will be completed prior to enrolment in the study. The study results will be disseminated through local and international health conferences and peer reviewed manuscripts. INTRODUCTION The congestive heart failure (CHF) syndrome is the leading cause for admissions and is in the top three causes for mortality in the Western World. It is associated with significant morbidity, impacts on individual’ s quality of life and through the necessity of frequent medical and allied health interventions, prescription of pharmacological agents and recurrent hospita- lisations, is a source of stress on health resources. Guidelines-based care improves out- comes but challenges exist in implementation. Neglecting this resource-intensive investment leads to poor outcomes and so the cycle perpetuates. CHF is speculated, as no accurate prospective data are available, to be higher in the Northern Territory (NT) and among Indigenous Australians. The recent Central Australian Secondary Prevention of Acute Coronary Syndromes (CASPA) study high- lighted a significant burden of CHF, greater among the Indigenous communities, 1 confirm- ing earlier studies of under-representation nationally. 2 These works have highlighted several key indicators relevant to the NT 1–26 : 1. There is a high burden of CHF that cannot be explained by traditional risk factors alone. Among the Indigenous population, given that social factors influence the risk of CHF, the excess in mortality is most likely to be multifactorial in origin, and have its foun- dations in the economic, social, physio- logical, psychological and educational disadvantages. 1–3 2. There appears a greater burden of CHF related to rheumatic and non-ischaemic aeti- ology , which is reversible and has a better Iyngkaran P, Tinsley J, Smith D, et al. BMJ Open 2014;4:e004137. doi:10.1136/bmjopen-2013-004137 1 Open Access Protocol group.bmj.com on August 3, 2014 - Published by bmjopen.bmj.com Downloaded from group.bmj.com on August 3, 2014 - Published by bmjopen.bmj.com Downloaded from group.bmj.com on August 3, 2014 - Published by bmjopen.bmj.com Downloaded from
Transcript of BMJ Open 2014 Iyngkaran
Northern Territory Heart Failure Initiative—Clinical Audit (NTHFI—CA)—aprospective database on the quality of careand outcomes for acute decompensatedheart failure admission in the NorthernTerritory: study design and rationale
Pupalan Iyngkaran,1 Jeff Tinsley,2 David Smith,3 Mark Haste,4
Kangaharan Nadarajan,5 Marcus Ilton,6 Malcolm Battersby,7 Simon Stewart,8
Alex Brown9
To cite: Iyngkaran P,Tinsley J, Smith D, et al.Northern Territory Heart FailureInitiative—Clinical Audit(NTHFI—CA)—a prospectivedatabase on the quality of careand outcomes for acutedecompensated heart failureadmission in the NorthernTerritory: study design andrationale. BMJ Open 2014;4:e004137. doi:10.1136/bmjopen-2013-004137
▸ Prepublication history andadditional material for thispaper is available online. Toview these files please visitthe journal online(http://dx.doi.org/10.1136/bmjopen-2013-004137).
Received 1 October 2013Revised 30 November 2013Accepted 4 December 2013
For numbered affiliations seeend of article.
Correspondence toDr Pupalan Iyngkaran;[email protected]
ABSTRACTIntroduction: Congestive heart failure is a significantcause of morbidity and mortality in Australia. Accuratedata for the Northern Territory and IndigenousAustralians are not presently available. The economicburden of this chronic cardiovascular disease is felt byall funding bodies and it still remains unclear whatimpact current measures have on preventing theongoing disease burden and how much of this filtersdown to more remote areas. Clear differentials also existin rural areas including a larger Indigenous community,greater disease burden, differing aetiologies for heartfailure as well as service and infrastructurediscrepancies. It is becoming increasingly clear thaturban solutions will not affect regional outcomes. Tounderstand regional issues relevant to heart failuremanagement, an understanding of the key performanceindicators in that setting is critical.Methods and analysis: The Northern Territory HeartFailure Initiative—Clinical Audit (NTHFI-CA) is aprospective registry of acute heart failure admissions overa 12-month period across the two main NorthernTerritory tertiary hospitals. The study collects informationacross six domains and five dimensions of healthcare.The study aims to set in place an evidenced andreproducible audit system for heart failure and inform thedeveloping heart failure disease managementprogramme. The findings, is believed, will assist thedevelopment of solutions to narrow the outcomes dividebetween remote and urban Australia and betweenIndigenous and Non-Indigenous Australians, in case theyexist. A combination of descriptive statistics and mixedeffects modelling will be used to analyse the data.Ethics and dissemination: This study has beenapproved by respective ethics committees of both theadmitting institutions. All participants will be provided awritten informed consent which will be completed priorto enrolment in the study. The study results will bedisseminated through local and international healthconferences and peer reviewed manuscripts.
INTRODUCTIONThe congestive heart failure (CHF) syndromeis the leading cause for admissions and is in thetop three causes for mortality in the WesternWorld. It is associated with significant morbidity,impacts on individual’s quality of life andthrough the necessity of frequent medical andallied health interventions, prescription ofpharmacological agents and recurrent hospita-lisations, is a source of stress on healthresources. Guidelines-based care improves out-comes but challenges exist in implementation.Neglecting this resource-intensive investmentleads to poor outcomes and so the cycleperpetuates. CHF is speculated, as no accurateprospective data are available, to be higher inthe Northern Territory (NT) and amongIndigenous Australians. The recent CentralAustralian Secondary Prevention of AcuteCoronary Syndromes (CASPA) study high-lighted a significant burden of CHF, greateramong the Indigenous communities,1 confirm-ing earlier studies of under-representationnationally.2 These works have highlightedseveral key indicators relevant to the NT1–26:1. There is a high burden of CHF that cannot
be explained by traditional risk factors alone.Among the Indigenous population, giventhat social factors influence the risk of CHF,the excess in mortality is most likely to bemultifactorial in origin, and have its foun-dations in the economic, social, physio-logical, psychological and educationaldisadvantages.1–3
2. There appears a greater burden of CHFrelated to rheumatic and non-ischaemic aeti-ology, which is reversible and has a better
Iyngkaran P, Tinsley J, Smith D, et al. BMJ Open 2014;4:e004137. doi:10.1136/bmjopen-2013-004137 1
Open Access Protocol
group.bmj.com on August 3, 2014 - Published by bmjopen.bmj.comDownloaded from group.bmj.com on August 3, 2014 - Published by bmjopen.bmj.comDownloaded from group.bmj.com on August 3, 2014 - Published by bmjopen.bmj.comDownloaded from

prognosis when treatment is delivered or preventivemeasures are enforced.2–5 14
3. There appears a greater burden of CHF with comorbid-ities among Indigenous clients, which requires greaterresources to deliver comprehensive care.2 15
4. There are significant barriers and differentials in access toappropriate, acceptable and evidence-based medicalcare and preventative measures for Indigenous andremote clients. New delivery methods are importantas CHF can largely be delivered as community-basedcare.13–25
5. There is significant delay in presentation and receipt ofacute care during periods of decompensation, andfor geographical and other reasons delay of definitivetherapies or procedures.
6. There is poor uptake of postdischarge services such ascardiac rehabilitation, and at present, unknowndemographics will assist implementation of remoteallied health or technological-based solutions.3 14
7. Unique geography—the NT consists of a vast area withtwo major public hospitals in Alice Springs andDarwin servicing 230 000 clients; approximately 70%of people live within the urban proximity. Specialistservices reside at the tertiary hospitals with satellitedistrict hospitals in several smaller townships support-ing a small number of visiting specialists. Serviceplanning must take this into account.3 14
8. External validity—adherence to guidelines early inhospital admission can improve outcomes; however,not all groups meet trial conditions in remote areasnor are trial conditions for dosing strategies reprodu-cible.15 27 28 A consensus on therapeutics strategies isneeded.Lack of accurate prospective data for the listed points
makes it difficult to accurately develop a tailored, yet com-prehensive heart failure (HF) programme. Developingtools to gather evidence require adhering to standards forvalidity and reproducibility, which are also lacking. Thisstudy is focused on understanding the current evidencebase for quantifying healthcare systems and informing thedesign of diagnostic and management clinical audits thatwould form the backbone for the direction of CHF diseasemanagement systems within an NT context. We thuspropose to study the quality and outcomes of care forpatients admitted with acute decompensated heart failure(ADHF). We aim to develop key clinical and process ofcare performance indicators (key performance indicators,KPI) and translate these findings for improved servicedelivery if and where deficiencies are highlighted. Thispaper describes the rationale for the Northern TerritoryHeart Failure Initiative—Clinical Audit (NTHFI-CA)design.
METHODSAims and scientific hypothesesThe NTHFI-CA survey was designed with four majorobjectives: first, to develop validated and reproducible
KPI for the comprehensive measurement of quality ofcare and outcomes for clients admitted with ADHF. Inthis, we aim to measure for the clients, the proportionmeeting standardised clinical outcomes, process out-comes and defined targets of secondary prevention andcompare by age, ethnicity, sex and place of usual resi-dence. For the health system, identify failures of thehealth care system in relation to timely acute care and tothe provision of secondary CHF care, particularly forIndigenous and remote clients; second, to develop asystem of data collection and reporting, that can be usedfor ongoing quality assessment and improvement acrossthe care continuum; third, the results of the first twoobjectives, are believed, will help tailor a pilot interven-tion study similar to the ongoing nurse-led interventiondeveloped around the CASPA-acute coronary syndrome(ACS) study findings; fourth, to accumulate sufficientepidemiology and implementation-focused informationto steer future action in the provision, monitoring anddevelopment of guidelines-based quality CHF care forrural, urban, Indigenous and Non-Indigenous clients.We hypothesise that patients presenting with ADHF areexpected to have: a disproportionate representation ofIndigenous clients with advanced systolic impairment;excess of alcohol, ischaemic or rheumatic aetiology;greater comorbidities in diabetes, hypertension, lipidabnormalities and/or renal insufficiency, and with othernon-cardiac comorbidities; delayed presentations forIndigenous and remote clients; we hypothesise thattreatment for Indigenous and remote clients: are likelysuboptimal for the stage of HF; have fewer clinical inter-ventions and support compared with their urban coun-terparts; are less likely to receive novel therapeuticoptions or enrolled in multicentre trials; and are morelikely to have their HF managed without regular cardi-ology specialist input.
Projected outcomesWe anticipate several outcomes from this work: first, iden-tification of the points of weaknesses in the hospital andcommunity health centre systems that impact on urban,rural, Indigenous and Non-Indigenous clients and hope-fully lead to the development of focused serviceimprovement models across this care continuum;second, to link with a number of collaborative researchprojects assessing barriers to care for Indigenous clientssuffering with heart diseases; third, lead to the develop-ment of ongoing and sustainable quality improvementpractices and monitoring within hospital and primaryhealthcare (PHC) services across the region; fourth,help develop, trial and implement standardised medicaldischarge summaries and care plans during hospital stayand following discharge; fifth, explore the potential con-tribution of poor systems of care to the high level ofillness faced by Indigenous people; and finally, assess-ment of the potential barriers that may exist for primaryand secondary prevention for CHF. These goals shouldinitially drive improved service delivery and subsequently
2 Iyngkaran P, Tinsley J, Smith D, et al. BMJ Open 2014;4:e004137. doi:10.1136/bmjopen-2013-004137
Open Access
group.bmj.com on August 3, 2014 - Published by bmjopen.bmj.comDownloaded from

provide a baseline for evaluating ongoing service out-comes on which to base future acute and preventive pro-gramme development and inform the development ofalternative models of secondary prevention for NTclients with CHF.
ProtocolThe project comprises two specific stages. Stage 1 is thecollaborative development of suitable KPI coveringprocess and outcome measures across the continuum ofcare; and stage 2, involves two phases, is the developmentof appropriate, feasible data collection tools and theirsubsequent measurement in hospital and PHC settings.
Development of appropriate clinical indicators (stage 1)We conducted an extensive literature review with keywords “heart failure or acute heart failure or chronicheart failure or CHF”; “database or study design or studyrationale or registry” and “Data Collection/or QualityIndicators, Health Care/ or Management Audit/ or per-formance indicators.mp or Healthcare Disparities/Quality Assurance, Health Care/or Quality of HealthCare/or Quality Indicators, Health Care/or quality ofcare indicators.mp or ‘Outcome and Process Assessment(Health Care)’/or process of care.mp”. Published andestablished existing KPI for measuring the quality andoutcomes of care for patients experiencing ADHF werecollated6–12 29–40 The CASPA study KPI was used as atemplate. Within six domains and five dimensions ofcare, KPI were added or rested on this template usingthe American College of Cardiology and the AmericanHeart Association (ACC/AHA) attributes of perform-ance measures.31 Addition or removal required consen-sus of the principal investigator and one co-investigator.Uniform agreement by all co-investigators was requiredfor accepting the final measures (figures 1 and 2). ACS(as an aetiology for ischaemic cardiomyopathies oraggravator of existing cardiomyopathies) and KPI thatwere deemed not to add any additional benefit on whatwas already known from CASPA were also rested.
Study design and registry (stage 2)The NTHFI-CA registry is a prospective observationalcohort study designed to examine the performance ofhealth systems in relation to the acute management andsecondary prevention of ADHF in patients admitted totwo teaching hospitals in the NT, Royal Darwin Hospital(RDH) and Alice Springs Hospital (ASH) startingSeptember 2013 and followed for 12 months endingSeptember 2015. Performance will be measured againstcurrently available evidence-based guidelines for thetreatment and secondary prevention of CHF4 6–11.29–38
Data collected will be entered in the NTHFI-CA studyregistry located at NT Cardiac Services/Menzies Schoolof Health Research, Darwin. All documentation relatingto study participants will be treated in accordance withNational Statement of Ethical Conduct in HumanResearch.41
Eligibility criteriaPatients admitted to either hospital with the diagnosis ofHF (International Classification of Diseases (ICD)-10CMI42.0–I42.8, 143.0, 150.0–150.9) will be eligible for theprospective case note audit. The participants will also bedrawn from inpatients who develop acute symptomswhile in hospital for other reasons. Further assessmentwill also involve the generation of lists ICD CM I00–I02,I05–I09, I10–I15, I20–I28, I30–I41, I44–I49, I70–I89 andI95–I99 (complicated with acute heart failure) for cross-checking of initial coding and recording of outcomevariables. Participants will be considered eligible if thereview of medical records demonstrates that they, in fact,have suffered an ADHF based on ACC/AHA andNational Health Data Dictionary standardiseddefinitions.
Exclusion criteriaPatients will be excluded if they die within 24 h of admis-sion or do not usually reside within either region orwhom no follow-up data can be obtained; however, theseclients will still provide baseline incidence data. Casesthat do not fulfil the case definition of ADHF on reviewof the notes will also be excluded, and recorded but willnot form baseline data.
Population/recruitment of subjectsA dedicated research assistant will recruit consecutivepatients who present acutely to either hospital or trans-ferred from remote Indigenous communities from theemergency clinical screen and medical admission lists for.Of these, clients who are Aboriginal, or non-Aboriginal,have a documented urban residence and reside in remotecommunities will be followed. The participants will also bedrawn from inpatients who develop acute symptoms whilein hospital for other reasons. Flyers will be posted in emer-gency, wards, intensive care and a brief presentation willbe made to the medical and nursing staff at relevant units.Referrals from hospital staff in this form will be a second-ary recruitment strategy. For retrospective audit, lists ofindividuals will be generated through hospital separationand CCU admissions data for the years 2011 and 2012.The approved research assistant in each site will performthis. An independent physician will review uncertain cases.
Data collection and storageData will be collected on a standardised case note extrac-tion form developed during phase I of the project.Information will be accessed through multiple sourcesincluding hospital records, PHC clinic records, specialistdatabases and record systems maintained by visiting dis-trict medical officers. The period of interest for data col-lection will be 0–12 months after discharge followingdocumented ADHF. Data definitions will be standardisedand widely accepted case and outcome definitions asoutlined in the ACC Clinical Data Standards.9–11 31–37
All cases that demonstrate ambiguity in data definitionsor outcome data will initially be discussed with site
Iyngkaran P, Tinsley J, Smith D, et al. BMJ Open 2014;4:e004137. doi:10.1136/bmjopen-2013-004137 3
Open Access
group.bmj.com on August 3, 2014 - Published by bmjopen.bmj.comDownloaded from

investigator; if ambiguity persists, the principal investiga-tor and a locally convened panel of the research teamwill review, and consensus sought.
Measurement of performancePhase I involves prospectively auditing admitted clientshospital records. Phase II involves further assessment ofperformance and will involve the auditing of clientrecords held at remote community health centres,urban PHC centres, specialists’ records, hospitalrecords and outpatient and cardiac rehabilitation files.Files are coded and stored by three health providers, NTDepartment of Health and Community Services (DHCS—ASH/RDH), PHC records and NT Cardiac Services
Pty Ltd. NT DHCS hospital separation data, hospitalrecords coding and storage of data follow a nationwideformat. PHC records will also be accessed to completethe secondary prevention and follow-up components ofthe audit and is subject to variability. NT Cardiac, mainprovider of cardiac diagnostics and outpatient care, data-bases and coronary intervention information systemsholds a range of clinical and cardiac investigation/inter-vention (angiography, coronary stenting, echocardiog-raphy, stress testing) information. This information willbe used to complete the data collection sheet for eachpatient file. Denominator and numerator values for KPIwill be based on standardised values from ACC/AHAguidelines, local laboratory specification for biochemical
Figure 1 International
Classification of Diseases
(ICD)-10 of the circulatory system.
Primary screening includes codes
I42, I43 and I50. Secondary
screening involved acute
decompensated heart failure
during index admission with
highlighted codes.
4 Iyngkaran P, Tinsley J, Smith D, et al. BMJ Open 2014;4:e004137. doi:10.1136/bmjopen-2013-004137
Open Access
group.bmj.com on August 3, 2014 - Published by bmjopen.bmj.comDownloaded from
tests and Australian accrediting bodies for invasive andnon-invasive investigations. Overall performance will becompared with the National benchmark for CHF out-comes. As this is subject to change, the broad principalswill include CSANZ, Heart Foundation and locally pub-lished studies that involve a public tertiary HF referralcentre from any of the six states in Australia. We will also
seek the opinion of several local leading HF cliniciansshould there be issues standardising these benchmarks.
Participant follow-upClients will be followed up to determine subsequent hos-pitalisation, major medical events and interventions.Similar ICD codes for acute CHF will be used for
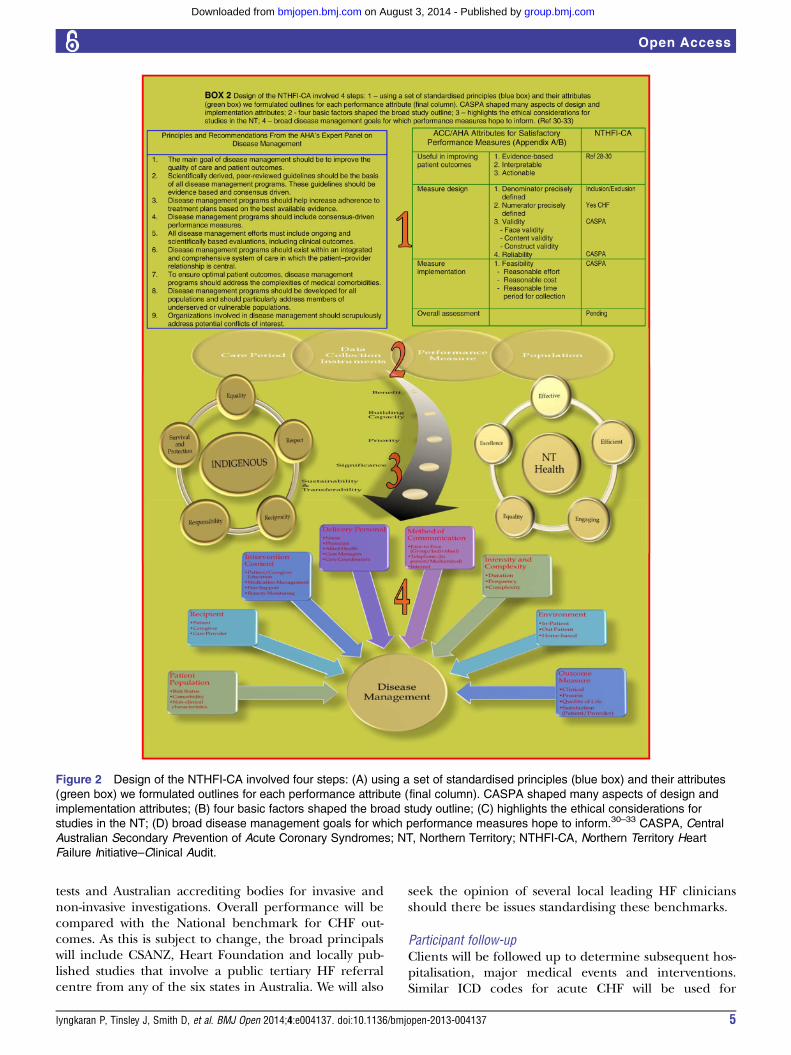
Figure 2 Design of the NTHFI-CA involved four steps: (A) using a set of standardised principles (blue box) and their attributes
(green box) we formulated outlines for each performance attribute (final column). CASPA shaped many aspects of design and
implementation attributes; (B) four basic factors shaped the broad study outline; (C) highlights the ethical considerations for
studies in the NT; (D) broad disease management goals for which performance measures hope to inform.30–33 CASPA, Central
Australian Secondary Prevention of Acute Coronary Syndromes; NT, Northern Territory; NTHFI-CA, Northern Territory Heart
Failure Initiative–Clinical Audit.
Iyngkaran P, Tinsley J, Smith D, et al. BMJ Open 2014;4:e004137. doi:10.1136/bmjopen-2013-004137 5
Open Access
group.bmj.com on August 3, 2014 - Published by bmjopen.bmj.comDownloaded from

screening information at 1, 6 and 12 months. Dataextraction will include a combination of case notesreview, medical databases and contact with PHC andclients directly. Consent for this will be obtained duringthe initial recruitment.
End pointsThe main indicators we are measuring cover a range ofdomains across the spectrum of care for people withADHF. In brief variables include▸ Baseline– Demographics: age, sex, usual place of residence,
ethnicity;– Background: medical history of CHF and treat-
ments, known risk factors and comorbidities;– Symptom onset: time, nature, location, first point of
contact with PHC, delay times to care.▸ Prehospital management: appropriate medical/para-
medical assessment, provision of prehospital nitrates,diuretics, ventilation and analgesia
▸ Emergency department: presentation, delas, biochem-istry, investigations (chest X-ray, ECG, echocardiog-raphy), therapeutics (assisted ventilation, intravenousnitrates or diuretics); risk stratification.
▸ Admission details: clinical examination, investigations,management, complications during admission, per-formance of phase I rehabilitation.
▸ Discharge: discharge diagnosis, discharge status, medi-cation regime, referral to phase II cardiac rehabilita-tion, discharge planning and referral to PHC provider.
▸ Outpatients– Cardiac rehabilitation: attendance and completion
of cardiac rehabilitation.– Secondary prevention: risk factor modification, care
plan, cardiac education received, measurement ofand achievements of specified target goals for HF andprevention of risk factors related to aetiology (eg, car-diovascular disease, ie, smoking cessation, lipidcontrol, blood pressure control), complications.
– Self-management.– Depression—PHQ9.– Outcomes: readmission, major cardiovascular and
non-cardiovascular events, mortality.– IT and telecommunications: availability, access and
type of mobile phone and Internet platforms.Special Ethical Consideration and Adverse Events: cul-
tural and religious issues surrounding confidentialityand storage of human tissue are of significant import-ance for Indigenous clients. The NT is also host to adiverse multiethnic population. We have thus chosennot to store samples for future use. We have sought spe-cific support from key Indigenous Community groups,NT-DHCS, Cardiac Services, Remote and PrimaryHealth Services, Independent Health Services andIndigenous Health Services, in advance. As primarily ahospital and clinic file audit, this proposal does not dir-ectly broach the issues of reciprocity, respect, equality,responsibility, survival and protection, which are critical
in Indigenous research, confirmation of which wasobtained through the ethics submission. We do notanticipate any other adverse events. We have received fullethics approval to conduct the study by Central Australia andTop End Human Research Committees.
Training and standardisationThis project requires access to data housed and main-tained by NT DHCS and NT Cardiac Services. HospitalSeparation Data, Hospital Records and PHC Recordswill be sought from NT DHCS and will be arrangedthrough PI’s in Darwin. In the event that PHC recordsare housed within independent services (non-DHCSclinics), appropriate consultation will be undertaken asrequested by the independent services themselves.Formalised consent processes as directed by independ-ent services will be followed. If they wish to perform theaudit themselves, as a training and quality assuranceprocess, appropriate training and support will be pro-vided by the research team. All staff recording informa-tion will be briefed by training staff from the CASPAstudy and undergo education in variability or datarecording, ambiguous data and differing case records,ICD-10 classification, ACC/AHA guidelines for KPI31
and NHMRC good clinical practice as the minimumrequirement. Addressing ambiguity has been discussedunder data collection and storage.
Expected sample sizeOn the basis of generated hospital separation and CCUstatistics, 2009, for ASH of 113 and RDH of 450 patients,the sample population will be approximately 150patients with ADHF at ASH and 500 matched at RDH inthe time period 2009. Of the ASH separations, 99 (88%)are identified as being indigenous. The matched (ethni-city and gender) RDH sample extrapolates to 180(40%), Aboriginal clients in phase II. As data will be col-lected on three separate occasions for each patient, arobust dataset is expected to identify any significant asso-ciations between predictors and patient outcomes.Findings from this investigation will also inform thedevelopment of more testable hypotheses in futurestudies and appropriate sample sizes.
Statistical considerationsAll generated data will be entered into and analysedwith SPSS V.11.5. Initial data analysis will be conductedto assess for data quality including allowable ranges, datastructure and errors. Descriptive statistics for baselineparticipant characteristics, diagnostics and therapeuticswithin highlighted domains will be calculated and pre-sented as means (SD), IQR for continuous data andcount (per cent) for categorical data. Univariatebetween group analyses will be performed using t testsfor continuous variables, and χ2 tests of association forcategorical variables. For study outcome measures, atype 1 error rate of α=0.05 will be used to test for statis-tical significance. A generalised mixed-effects model
6 Iyngkaran P, Tinsley J, Smith D, et al. BMJ Open 2014;4:e004137. doi:10.1136/bmjopen-2013-004137
Open Access
group.bmj.com on August 3, 2014 - Published by bmjopen.bmj.comDownloaded from
approach will be used in the analysis of repeated mea-sures for continuous and categorical outcomes.Mixed-effects models take into account the interindivi-dual differences in intraindividual change with repeatedresponses and use all the available data on each partici-pant. Mixed models are also unaffected by randomlymissing data and therefore do not require imputationmethods.42 The model-building strategy will includefitting nested models by sequentially adding blocks ofpredictor variables: sociodemographics, comorbid disor-ders and factors related to health service interventions.Interaction terms that are considered to be potentiallyimportant from a clinical perspective will be tested andremain in final models if significant. Predicted estimatesof outcomes at each time point will be calculated usingfitted models of the data in order to examine patternsof individual change. To interpret effect sizes and preci-sion for categorical outcomes, ORs and CIs will becalculated.
DISCUSSIONThe NTHFI-CA represents one of a few opportunitiesoffered for longitudinal studies designed to extract datathat inform service development. Information gatheredhas to be relevant for current and future needs. It is dif-ficult to determine service factors beyond five yearlyintervals. To compensate for this, there have been mea-sures taken to set infrastructure and standardise proto-cols to facilitate episodic updates in information as wellas ensuring reproducibility of study design and imple-mentation. With the actual study design, a series of stepswere taken. The first step was establishing basic princi-ples for defining the disease (figure 1, see online sup-plementary appendix A). The second step involvedstandardising principles for attributes in KPI, that is,care dimensions (figure 2A, see online supplementaryappendices B and C) and the study care domains to betested, in this case six (figure 2B). The third stepinvolved addressing the broad NT health goals andresearch conducted in Indigenous population to steerimplementation within five key priorities (figure 2C).The fourth step is design of disease managementsystems in the NT context from the available evidence(figure 2D, see online supplementary appendix D).The resultant study pathway is highlighted in Figure 3.The specific study in greater detail are explored.The ACC/AHA has released several position statements
to standardise the process of developing, assessing, imple-menting performance measures and disease manage-ment systems.30–33 From this consensus-driven platform,we identified the target disease, population and exploredstandardised measures that inform the observation forthe required time period. The NTHFI-CA is defined forall stages and causes of CHF, for NT resident populationwho receive care within six domains of treatment. Thisbroad definition partly relates to uncertainties on actualCHF demographics, and as the yearly admission is
unlikely to exceed 500, will not lead to significant difficul-ties in enrolment. To determine the performance mea-sures, we again explored the position statement. Theauthors rated 27 potential measures on 13 dimensionsusing a five-point Likert scales.31 If a KPI received fullcommittee support with a score of at least 3, it wasadvanced. The process concluded with 7 inpatients’ and12 outpatients’ measures. These KPI informed fivedimensions of care encompassing: diagnostics, patienteducation (including prognosis and aetiology), treat-ment, and self-management (for inpatient and out-patient) and monitoring of disease status (for outpatientsonly).31 This statement did not, however, focus on out-comes as the design was shaped to assist physiciansimprove care. We have included outcomes, as this is thestrongest indicator of funding for vulnerable groupsbeyond the conventional block funding models. To deter-mine the final KPI, several additional points wereconsidered.1. Existing studies: Several recent databases stand as land-
mark achievements in HF epidemiology and have con-firmed clinical understanding of evidence base andpositive outcomes.9–11 35 37 43 Interestingly Krumholzet al30 pointed out a disparity between what is conven-tionally accepted evidence and its generalisabilty. Thisis particularly so for the NTwhere there are significantnon-traditional factors that impact on the delivery ofevidence-based care and affect outcomes. While itwould be unreasonable to propose reconducting largeCHF studies to incorporate an increasingly diversegroup of patients, we have come to realise that theheart of these matters is to develop an intrinsic under-standing of the underlying regional demographic dif-ferences and service delivery dynamics to be able toformulate informed decisions in implementing thenecessary measures, be they simple or more complex.Developing the necessary KPI in these settings is achallenge as there is a divide between perceivedoptimal care and realistic and deliverable care that, infact, is optimal for the region. From this, it was evidentthat some measures needed to be rested (eg, treat-ment optimisation) and others added (eg, the dimen-sion of technology).
2. NT experience: The CASPA study was groundbreakingin the sense that it allowed for the first-time explor-ation of ACS/cardiovascular KPI in Central Australia.The list was formulated from an extensive search ofavailable national and international clinical guide-lines, national health priority area indicators andreports and with reference to National HealthPerformance Committee guidelines and further aug-mented by performance measures used in publishedquality improvement projects. Three priorities—process of care, target achievement and outcomeindicators for the treatment and prevention weregenerated. This list underwent scrutiny by 60 key sta-keholders, key external content experts and theresearch team through mailed questionnaires and a
Iyngkaran P, Tinsley J, Smith D, et al. BMJ Open 2014;4:e004137. doi:10.1136/bmjopen-2013-004137 7
Open Access
group.bmj.com on August 3, 2014 - Published by bmjopen.bmj.comDownloaded from
workshop convened in Alice Springs. Each stake-holder was asked to grade each potential indicatoraccording to a number of criteria: strength of evi-dence; feasibility of measurement; plausibility ofeffects from quality improvement; impact on out-comes and an assessment of the overall utility of themeasure. Results were collated and analysed for eachindicator (overall grading) and for each of the fivecriteria across each indicator. Indicators that weregraded as high priority, frequently recorded, veryplausible and will have a large impact or better wereincluded in the final list (average score on gradingscale ≥4). Indicators that demonstrate an across cri-teria grade of less than 4, but was assessed by key sta-keholders as a high or essential priority within theoverall (utility) rating, were scrutinised by the projectteam and included as decided by consensus. Dataspecifications were then developed according tointernationally standardised definitions. Subsequentdata collection tools were developed and piloted in anumber of hospital and PHC records (n=20) andimplemented. The spill-over knowledge assistedgreatly in the NTHFI-CA design.
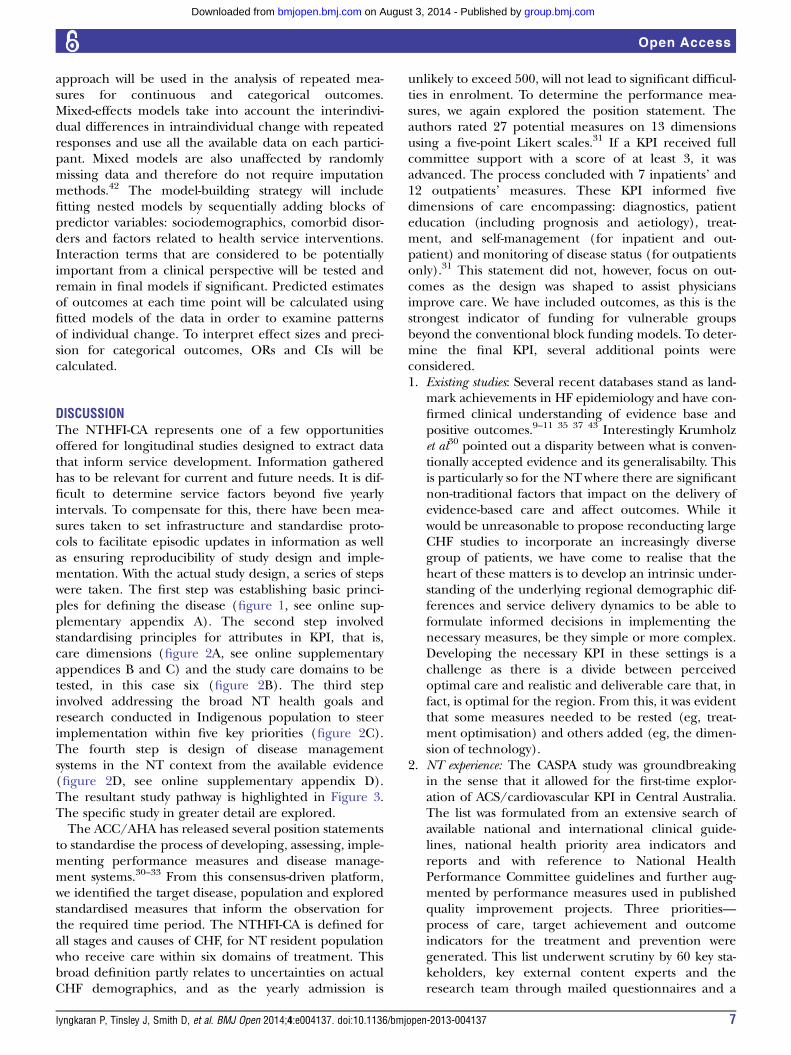
Combining this local and international experience,with the standardised ACC position,31 a conceptualframework KPI reflecting six critical domains for treat-ment delivery and five principal dimensions of careevolved (figure 3). All these well-established performancemeasures were individually scrutinised and included orrested. Level of evidence was the predominant scrutinis-ing theme in the second phase. The less validated ‘localknowledge’ and NT health priorities were additional con-siderations. Study investigators made the decisions onthese. Several less well-established indicators wereincluded through recent understanding and develop-ment of self-management and IT-based solutions.14 Indirect contrast to intervention-themed databases,34 35
focus on specifics in the treatment dimension was given alower priority (see online supplementary appendices Eand F). Figure 4 describes this in greater detail.Further rationale for specific KPI inclusion or exclu-
sion are as follows: Domain 1: demographics are at theheart of this study. Validated KPI derived from CASPAwere used to extract race, culture, language and supportnetworks; further expansion was made in the dimensionof HF aetiology with emphasis on ischaemic, hypertensive
Figure 3 Trial protocol and
study pathways.
8 Iyngkaran P, Tinsley J, Smith D, et al. BMJ Open 2014;4:e004137. doi:10.1136/bmjopen-2013-004137
Open Access
group.bmj.com on August 3, 2014 - Published by bmjopen.bmj.comDownloaded from

as well as rheumatic and alcohol-induced causes. Data ontertiary referral centres were collected, as there were twomain cardiac surgical referral hospitals. Decision referralpatterns vary with the treating physician practices as wellas waiting list and urgency. It is established that decisionson percutaneous or surgical revascularisation and valvu-lar restoration or replacement differ at these sites onphysician, group consensus and expertise at the respect-ive sites. Details on primary care physician, pharmacy,residence and principal next of kin were deemed import-ant as local and ethnicity were deemed factors in serviceuptake and delivery. Furthermore, access to primary carecould determine: admission, re-admission burden andearly measures to prevent deterioration; Domain 2–5:a comprehensive medical history of all systems wereincluded to establish the overall need for chronicmedical service needs and factors preventing use oruptake of HF pharmacology, cardiac rehabilitation orreferral for invasive management. Biochemistry detailswere included to establish pattern of establishing HF aeti-ology and outpatient risk for adverse events. Methods forestimating epidermal growth factor receptor wasobtained as much recent work raises validity of estimated
measures with illness and demographics, which subse-quently alter prescribing practices and outcomes.11 12 44
KPI for depression were expanded, as a high burden wasnoted in CASPA, this also being a significant factor inmany dimensions of self-care and compliance. In hos-pital, discharge and outpatient indicators were designedto reflect the potential blocks to maximising provenpharmacological prescription and access to cardiacrehabilitation; at the core of these were reasons for non-prescription or subtherapeutic prescription. The actualspecifics on medication titration across all domains wererested. It is noted that care and resources are needed totitrate many variables in CHF care, for example, ββ andACE-I (see online supplementary appendix E, F). Thisinformation can be extrapolated from frequency ofcontact with medical practitioner and central pharmacyprescription slips. Appropriate early therapeutics—toprevent further heart muscle damage, good symptomrelief and minimising iatrogenic adverse effects such asrenal dysfunction and electrolyte derangements arewithin the control of the health systems and builds clientconfidence, and are considered vital. Domain 6: overall,we felt, in the community, that the greatest value in the
Figure 4 Performance measures within each treatment dimensions divided into mild and moderate or greater acute
decompensated heart failure.
Iyngkaran P, Tinsley J, Smith D, et al. BMJ Open 2014;4:e004137. doi:10.1136/bmjopen-2013-004137 9
Open Access
group.bmj.com on August 3, 2014 - Published by bmjopen.bmj.comDownloaded from

performance measures related to two critical aspects—impacts on the overall health system (strain and morale)and contributors to poor outcomes (client and non-client). Post hospital access to services and blocks to refer-rals (non-client) and self-management (client) arefactors related to efficiency, planning and client educa-tion. Investment in these dimensions would not increasestrain on resources, with potential benefit.Data collection instrument was via Case Report Forms
(CRF) designed for a combination of retrospective andprospective audit from combination of several studiessuch as CASPA and WHICH. The Baker IDI, FlindersUniversity and SAHMRI have extensive track record inelectronic CRF. This was greatly beneficial and reducedchallenges faced at stage 2. At present, a considerableresearch work is conducted through the Menzies Schoolof Health Research. As part of this initiative, we havebegun the process of developing dedicated office toconduct studies across the cardiac and renal axis. Part ofthis also involved staff training in good clinical practiceand transfer of knowledge from partners to stand as anindependent entity.i
Indigenous health in the NT requires a special focus.Australia has seen the first Indigenous premier in 2013and a measured but controversial statement of removingthe Indigenous ministerial portfolio was “there arenumerous ministers for many areas and one for allIndigenous affairs”. Current sentiments that move awayfrom race-based programmes are encouraged but withcaution. We clarify that out approach does not targetany specific communities but is based on needs. It isunfortunate that disadvantaged communities are alsomarginalised in large studies partly for language, cul-tural and perceived compliance issues. In this case, theIndigenous community represents a significant group inAustralian society who have despairingly worse out-comes. The desire to preserve one’s traditional culturein an ever-modernising world poses huge challenges forthese communities and health systems. Poor understand-ing could lead to stereotyping that could brand somebehaviour as recalcitrant, adding to the vicious circle.Respecting these beliefs and tailoring care in lieu ofthese factors, we were able to advance the CASPA study.This was carried out through acknowledgement ofseveral sensitive areas in the ethics application; Equality—the overarching aims of the research project is basedwithin a framework driven by questions of equality inthe provision of healthcare across the continuum for allpatients regardless of ethnicity, gender or age, and onebased on need as demonstrated by clinical determinants;Survival and Protection—we also recognise that chronicdisease research and epidemiology has tended to con-tribute to deficit approaches to individual pathology,that is, disease is due to bad behaviour. Less focus has
been afforded the potential successes and failures inhealth systems, as contributors to differential outcomesfor populations based on ethnicity; Respect—we feel thatinformation generated within this project and the pro-cesses developed have the potential to contribute tocommunity-directed health service redevelopment andquality improvement activities; Reciprocity—we feel thatthis work may identify failures in health systems andtherefore identify obligations that are being unmet bysystems themselves; Responsibility—reframing the gaze ofhealth inequality, from individual-focused deficits tosystem failures stands as the key principle on which thisextensive work is based, and is a direct effort at ensuringthat exploring health inequalities does not undermineand harm Indigenous individuals and communities.These principles may play great importance to futureresearch practices in these areas.Interim analysis will be conducted at the 6-month
mark. It is anticipated at this point lessons learnt andspill-over knowledge from the ongoing CASPA-ACS inter-vention study may direct minor modifications to theexisting CRF. One such area is increasing the KPI indomains 1, 2 and 6 to better understand the barriers toaccessing primary care. CHF, an ambulatory case-sensitive condition, can largely be managed in the com-munity with the application of appropriate and timelypreventive care and early disease management. Theissues that remain unclear at this point are the adequacyand the barriers for accessing such care in each of theremote communities. Of interest, Ansari et al noted thata lack of timely and effective care had an impact onadmission rates in rural Victoria particularly amonglower socio-economic groups.45 46 A similar understand-ing in the NT could impact on how we allocate resourcesin the future.Measuring performance is not an end in its own right
and clinical indicators and their measurement alone arenot sufficient to change behaviour in service provisionand quality improvement. They must be supplementedwith key educational activities (eg, provision of continu-ous and sustained feedback of results to all levels ofservice provision), processes to sustain continuous moni-toring and assessment and to inform policy developmenton a local and regional level. Clearly defined dissemin-ation processes and involvement of Aboriginal HealthWorkers, hospital-based and community-based nurses,allied health professionals and clinicians are essential ifpractice is to change. Engaging non-governmental(NGO) service providers, data coders, quality improve-ment staff, NGOs (NHF NT Division, Healthy LivingNT), Division of General Practice/PHC and consumerrepresentatives in the development phase of the projectso as to ensure alignment between proposed indicatorsand local needs. The dissemination of key findingsthrough key advisory/research institutions will alsoincrease the awareness nationally/globally and buildfoundations for future competitive research funding.Finally, we have also been in negotiations for the
iInformation on our partners and expertise can be found on the webor via corresponding author.
10 Iyngkaran P, Tinsley J, Smith D, et al. BMJ Open 2014;4:e004137. doi:10.1136/bmjopen-2013-004137
Open Access
group.bmj.com on August 3, 2014 - Published by bmjopen.bmj.comDownloaded from

broader applicability of the findings of and tools utilisedwithin this project with the Australian CollaborativeProject (which seeks to measure PHC performance).This stands as a critical method of project outcomedissemination.
LimitationsConducting clinical studies in the NT is in itself a limita-tion: first, the realisation of non-traditional risk factors,which impact on management; second, as there are fewbenchmarks as comparators and; finally, shortfalls inresearch funding and infrastructure. While no systemhas the perfect mix of resource input to match serviceneeds to answer this question, for this region, there willbe components within many aspects of the study, that is,hypothesis generating, compared with the mainstream.Nonetheless, following the accepted consensus and pro-viding enough information to allow reproducibility areaccepted as a positive means for overcoming this limita-tion. Examples of this were resting KPI that collatein-depth information on medication dosing as per RCTsand large HF databases.30–38 This study will not addresswhether clinical trial prescribing practices are achieved;instead, we are keen to determine whether there is asystem in place to facilitate this, which will be answered.The infrastructure is also in place for the next step todetermine whether this can occur. We note that RCTlevel outcomes relate to achieving prescribing practicesin the trials. As examples, online supplementary appen-dix E/F highlight differences in two medications. Asnoted, ββ titration is ideally carried out at two weeklyintervals and may not need biochemistry, while ACE-Ican be carried out at 3–7-day intervals and usuallyrequires assessment of basic biochemistry.ii Addition ofaldosterone blockers and other agents are further com-plexities.ii We are hopeful that relevant information onthis will help steer the next phase, an intervention clin-ical study. This study relied on lessons from ACS studyconducted greater than 5 years ago. Unanticipatedchanges that cannot be standardised could act as con-founders, which will only be revealed in time; forexample, is potential drop off rate during follow-up. Inthe standardisation of design—we did not use five-pointLikert scale, as the number of NT consultants was only4. In addition the CHF task force position was compre-hensive.31 Finally, clinical practice guidelines are wellestablished, as Krumholtz stated “guidelines are writtenin a spirit of suggesting diagnostic or therapeutic inter-ventions for patients in most circumstances. Accordingly,significant judgment by clinicians is required to adaptthese guidelines to the care of individual patients toensure accountability in these judgments an evidencedbased process is important”. The standardising of
clinical judgement and interpretation of guidelinesremains contentious and may be more noticeable withfewer cardiologists. As such we intentionally left the cri-teria for KPI reference broad. This will be narrowed, aslessons are learnt and early data are analysed. Thisshould aid more focused and detailed assessments inthe future.
CONCLUSIONAchieving optimal care in the remote setting is no differ-ent from urban settings. The ability to provide a con-tinuum of care from presentation to post dischargerequires activation of proven KPI at each level of care. Thesignificant differences in remote care revolve around theinteraction of service infrastructure, personnel, diseaseburden and cultural sensitivities. As such the outcomeslimiting factors are variable and require exploration. Thepotential gains of these findings in implementing earlyand later secondary prevention of CHF and its sequelaeare undisputed. In addition, little information exists onthe provision and outcomes for CHF initiatives forIndigenous populations, which are a significant client basein the remote setting. Even less is known about the post-discharge care. The extent to which care is suboptimaland the acute and long-term HF management amongAboriginal clients could be contributing to the large andgrowing cardiovascular mortality differentials seenbetween Aboriginal and non-Aboriginal clients. Thus, thedevelopment of meaningful, sustainable public health,clinical and continuous quality improvement policy in theprovision of CHF care in the NTrequires urgent attention,and must be used to drive the development of betterservice delivery at the individual and health system levels.It is anticipated that this work will highlight key areas ofdisparity and inform the implementation of an interven-tion study.
Author affiliations1Department of Cardiology, Royal Darwin Hospital, Tiwi, Northern Territory,Australia2Chronic Disease Coordination Unit, Department of Health, Royal DarwinHospital, Tiwi, Northern Territory, Australia3Flinders Human Behavior and Health Research Unit, Flinders University,Adelaide, South Australia, Australia4Heart Failure CNC—Top End, Chronic Disease Coordination Unit, Departmentof Health, Royal Darwin Hospital, Tiwi, Northern Territory, Australia5Division of Medicine, Royal Darwin Hospital, Tiwi, Northern Territory,Australia6Department of Cardiology, Darwin Private Hospital, Rocklands Drive, Tiwi,Northern Territory, Australia7Flinders Human Behaviour and Health Research Unit (FHBHRU), MargaretTobin Centre, Flinders University, South Australia, Australia8Department of Preventative Cardiology, Baker IDI Heart and DiabetesInstitute, Melbourne, Victoria, Australia9Department of Indigenous Health, SAHMRI, Adelaide, South Australia,Australia
Contributors All the authors are involved in (1) substantial contributions toconception and design, acquisition of the data, or analysis and interpretationof the data; (2) drafting the article or revising it critically for importantintellectual content and (3) final approval of the version to be published.
iiWe have not provided treatment pathways for AICD/CRT/ otherpharmacotherapies. These are available from several optimisingdatabases (34, 35, 37).
Iyngkaran P, Tinsley J, Smith D, et al. BMJ Open 2014;4:e004137. doi:10.1136/bmjopen-2013-004137 11
Open Access
group.bmj.com on August 3, 2014 - Published by bmjopen.bmj.comDownloaded from
Competing interests None.
Funding All authors have won independent and governmental researchfunding. PI is supported by the Royal Australasian College of PhysiciansFellows Contribution Award.
Ethics approval TEHREC and CAHREC.
Provenance and peer review Not commissioned; externally peer reviewed.
Data sharing statement The current data will belong to the NT CardiologyDepartment. The data will be shared with our partners in FHBHRU, Baker IDIand SAHMRI.
Open Access This is an Open Access article distributed in accordance withthe Creative Commons Attribution Non Commercial (CC BY-NC 3.0) license,which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, providedthe original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/
REFERENCES1. Brown A. Acute coronary syndromes in Indigenous Australians:
opportunities for improving outcomes across the continuum of care.Heart Lung Circ 2010;19:325–36.
2. Woods JA, Katzenellenbogen JM, Davidson PM, et al. Heart failureamong Indigenous Australians: a systematic review. BMCCardiovasc Dis 2012;12:99.
3. Health and Human Services, Department of Health NT. KPMG.Development of the Northern Territory Specialist Cardiac ServicesPlan 2011–2020: final report. KPMG April 2011.
4. Expenditures on Health Services for Aboriginal and Torres StraitIslander People. Australian Institute of Health and Welfare. 1998–2013 Cat No. HWE 6–57. http://www.aihw.gov.au/publication-detail/?id=60129542787
5. Ansari MZ, Henderson T, Ackland M, et al. Congestive cardiacfailure: urban and rural perspectives in Victoria. Aust J Rural Health2003;11:266–70.
6. Krum H, Jelinek MV, Stewart S, et al. Guidelines for the prevention,detection and management of people with chronic heart failure inAustralia. Med J Aust 2011;194:405–9.
7. Schoken DD, Benjamin EJ, Fonarrow GC, et al. Prevention of heartfailure: a scientific statement from the American Heart AssociationCouncils on Epidemiology and Prevention, Clinical Cardiology,Cardiovascular Nursing, and High Blood Pressure Research; Qualityof Care and Outcomes Research Interdisciplinary Working Group;and Functional Genomics and Translational Biology InterdisciplinaryWorking Group. Circulation 2008;117:2544–65.
8. Dickstein K, Cohen-Solal A, Filippatos G, et al. ESC guidelines forthe diagnosis and treatment of acute and chronic heart failure 2008:the Task Force for the Diagnosis and Treatment of Acute andChronic Heart Failure 2008 of the European Society of Cardiology.Developed in collaboration with the Heart Failure Association of theESC (HFA) and endorsed by the European Society of Intensive CareMedicine (ESICM). Eur Heart J 2008;29:2388–442.
9. Cleland JG, Swedberg K, Follath F, et al.; Study Group on Diagnosisof the Working Group on Heart Failure of the European Society ofCardiology. The European Heart Failure survey program—a surveyon the quality of care among patients with heart failure in Europe.Eur Heart J 2003;24:442–63.
10. Fonarow GC, Abraham WT, Albert NM, et al.; OPTIMIZE-HFInvestigators and Hospitals. Influence of a performance-improvement initiative on quality of care for hospitalized patients withheart failure: results of the organized program to initiate lifesavingtreatment in hospitalized patients heart failure (OPTIMIZE-HF). ArchIntern Med 2007;167:1493–502.
11. Heywood JT, Fonarow GC, Costanzo MR, et al. High prevalence ofrenal dysfunction and its impact on outcome in 118,465 patientshospitalized with acute decompensated heart failure: a report fromthe ADHERE database. J Cardiac Fail 2007;13:422–30.
12. Ezekowitz J, McAlister FA, Humphries KH, et al. for the APPRAOCHInvestigators. The association among renal insufficiency,pharmacotherapy, and outcomes in 6247 patients with heart failureand coronary artery disease. J Am Coll Cardiol 2004;44:1587–92.
13. Iyngkaran P, Majoni V, Haste M, et al. Australian Indigenous ChronicDisease Optimization Study (AUSI-CDS) Prospective observationalcohort study to determine if an established chronic disease healthcare model can be used to deliver better heart failure care among
Remote Indigenous Australians: Proof of concept. Study Rationaleand Protocol. Heart Lung Circ 2013;22:930–9.
14. Iyngkaran P, Harris M, Nadarajan K, et al. Implementing guidelinebased heart failure care in the Northern territory: challenges andsolutions. Heart Lung Circ 2014; in press.
15. Iyngkaran P, Thomas M, Sanders P, et al. Do we need a widertherapeutic paradigm for heart failure with comorbidities?—a remoteAustralian perspective. Health Care Curr Rev 2013;1:106.
16. White H, Walsh W, Brown A, et al. Rheumatic heart disease inIndigenous populations. Heart Lung Circ 2010;192:273–81.
17. Clark RA, Eckert KA, Stewart S, et al. Rural and urban differentialsin primary care management of chronic heart failure: new data fromthe CASE study. MJA 2007;186:441–5.
18. Thomas DP, Heller RF, Hunter JM. Clinical consultations in anaboriginal community controlled health service: a comparison withgeneral practice. Aust NZ J Public Health 1998;22:86–91.
19. Clark RA, Driscoll A, Nottage J, et al. Inequitable provision ofoptimal services for patients with chronic heart failure: a nationalgeo-maping study. MJA 2007;186:169–73.
20. Phillips SM, Marton RL, Tofler GH. Barriers to diagnosing andmanaging heart failure in primary care. MJA 2004;191:78–81.
21. Clark RA, McLennan S, Eckert K, et al. Chronic heart failure beyondcity limits. Rural Remote Health 2005;5:443(online).
22. Ong MA, Weeramanthri TS. Delay times and management of acutemyocardial infarction in Indigenous and non Indigenous people inthe Northern Territory. MJA 2000;173:201–4.
23. Cunningham J. Diagnostic and therapeutic procedures amongAustralian hospital patients identified as Indigenous. MJA2002;176:58–62.
24. Rowley KG, Daniel M, Skinner K, et al. Effectiveness of acommunity-directed ‘healthy lifestyle’ program in a remote Australianaboriginal community. Aust N Z J Public Health 2000;24:136–44.
25. Driscoll A, Davidson P, Clark R, et al. Tailoring consumer resourcesto enhance self care in chronic heart failure. Aust Crit Care2009;22:133–40.
26. Sheperd F, Battye K, Chalmers E. Improving access to cardiacrehabilitation for remote Indigenous clients. Aust N Z J Public Health2003;27:632–6.
27. Teng THK, Hung J, Finn J. The effect of evidence-based medicationuse on long-term survival in patients hospitalized for heart failure inWestern Australia. MJA 2010;192:306–10.
28. Wang OJ, Krumholz HM. Clinical trial participation: are westudying the patients we are trying to treat? Eur J Heart Fail2009;11:1021–2.
29. Najafi F, Dobson AJ, Jamrozik K. Recent changes in heart failurehospitalizations in Australia. Eur J Heart Fail 2007;9:228–33.
30. Krumholz HM, Currie PM, Riegel B, et al.; American HeartAssociation Disease Management Taxonomy Writing Group. Ataxonomy for disease management: a scientific statement from theAmerican Heart Association Disease Management TaxonomyWriting Group. Circulation 2006;114:1432–45.
31. Bonow RO, Bennett S, Casey DE, et al. Clinical performancemeasures for adults with chronic heart failure: a report of the AmericanCollege of Cardiology Foundation/American Heart Association TaskForce on Performance Measures. Circulation 2005;112:1853–87.
32. Spertus JA, Bo3now RO, Chan P, et al. ACCF/AHA New insightsinto the methodology of performance measurement: a report of theAmerican College of Cardiology Foundation/American HeartAssociation Task Force on Performance Measures. Circulation2010;122:2091–106.
33. Riegel B, Lee CS, Sochalski J. Developing an instrument tomeasure heart failure disease management program intensity andcomplexity. Circ Cardiovasc Qual Outcomes 2010;3:324–30.
34. Fonarow GC, AbrahamWT, Albert NM, et al. Organized Program toInitiate Lifesaving Treatment in Hospitalized Patients with Heart Failure(OPTIMIZE-HF): rationale and design. Am Heart J 2004;148:43–51.
35. Fonorrow GC, Yancy CW, Albert NM, et al. Improving the use ofevidence based heart failure therapies in the outpatient settings: theIMPROVE HF performance improvement registry. Am Heart J2007;154:12–38.
36. Cleland JCF, Sewdberg K, Cohen-Solal A, et al.; The Euro HeartFailure Survey of The EUROHEART Survey Programme: a surveyon the quality of care among patients with heart failure in Europe.Euro J Heart Fail 2000;2:123–32.
37. Ambedkar AV, Fonarrow GC, Hernandez AF, et al. Characteristicsand in-hospital outcomes for non-adherant patients with heart failure:get with the Guidelines-Heart Failure (GWTG-HF). Am Heart J2009;158:644–52.
38. Patterson ME, Hernandez AF, Hammill BG, et al. Process of careperformance measures and long-term outcomes in patientshospitalized with heart failure. Med Care 2010;48:210–16.
12 Iyngkaran P, Tinsley J, Smith D, et al. BMJ Open 2014;4:e004137. doi:10.1136/bmjopen-2013-004137
Open Access
group.bmj.com on August 3, 2014 - Published by bmjopen.bmj.comDownloaded from

39. Silver MA, Peacock WF, Diercks DB. Optimizing treatment andoutcomes in acute heart failure beyond initial triage. CHF2006;12:137–45.
40. Gheorghiade M, Zannad F, Sopko G, et al. Acute heart failuresyndromes: current state and framework for future research.Circulation 2005;112:3958–68.
41. National Statement of Ethical in Human Research. National Healthand Medical Research Council Australian Research CouncilAustralian Vice-Chancellors’ Committee 2007.
42. Gueorguieva R, Krystal JH. Move over ANOVA: progress in analyzingrepeated-measures data and its reflection in papers published inthe archives of general psychiatry. Arch Gen Psychiatry2004;61:310–17.
43. Fonarow GC, Albert NM, Curtis AB, et al. Improving evidence-basedcare for heart failure in outpatient cardiology practices primaryresults of the registry to Improve the Use of Evidence-Based HeartFailure Therapies in the Outpatient Setting (IMPROVE HF).Circulation 2010;122:585–96.
44. Iyngkaran P, Thomas M, Majoni W, et al. Comorbid heart failure andrenal impairment—epidemiology and management. Cardiorenal Med2012;2:281–97.
45. Ansari Z. A review of literature on access to primary health care.Aust J Prim Health 2007;13:80–95.
46. Ansari Z, Barbetti T, Carson NJ, et al. The Victorian ambulatory caresensitive conditions study: rural and urban perspectives. SozPräventivmed 2003;48:33–43.
Iyngkaran P, Tinsley J, Smith D, et al. BMJ Open 2014;4:e004137. doi:10.1136/bmjopen-2013-004137 13
Open Access
group.bmj.com on August 3, 2014 - Published by bmjopen.bmj.comDownloaded from

Correction
Iyngkaran P, Tinsley J, Smith D, et al. Northern Territory Heart Failure Initiative—ClinicalAudit (NTHFI—CA)—a prospective database on the quality of care and outcomes for acutedecompensated heart failure admission in the Northern Territory: study design and rationale.BMJ Open 2014;4:e004137. On page 9 of this paper (Discussion section) the copy editor mis-takenly defined eGFR as ‘epidermal growth factor receptor’. This is not correct; the correctterm is, ‘estimated glomerular filtration rate (eGFR)’. In addition, in figure 2 of this paperparts A,B,C,D should have been labelled 1,2,3,4 so as to correspond correctly with theillustration.
BMJ Open 2014;4:e004137. doi:10.1136/bmjopen-2013-004137corr1
BMJ Open 2014;4:e004137. doi:10.1136/bmjopen-2013-004137corr1 1
Miscellaneous
CollectionsTopic
(188 articles)Research methods � (218 articles)Qualitative research �
(740 articles)Public health � (451 articles)Health services research �
(781 articles)Epidemiology � (303 articles)Cardiovascular medicine �
Articles on similar topics can be found in the following collections
Notes
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on August 3, 2014 - Published by bmjopen.bmj.comDownloaded from

doi: 10.1136/bmjopen-2013-004137 2014 4: BMJ Open
Pupalan Iyngkaran, Jeff Tinsley, David Smith, et al. study design and rationalefailure admission in the Northern Territory: outcomes for acute decompensated heartdatabase on the quality of care and
a prospective−CA)−Clinical Audit (NTHFI−Northern Territory Heart Failure Initiative
http://bmjopen.bmj.com/content/4/1/e004137.full.htmlUpdated information and services can be found at:
These include:
Data Supplement http://bmjopen.bmj.com/content/suppl/2014/01/28/bmjopen-2013-004137.DC1.html
"Supplementary Data"
References http://bmjopen.bmj.com/content/4/1/e004137.full.html#ref-list-1
This article cites 41 articles, 9 of which can be accessed free at:
Open Access
non-commercial. See: http://creativecommons.org/licenses/by-nc/3.0/terms, provided the original work is properly cited and the use iswork non-commercially, and license their derivative works on different license, which permits others to distribute, remix, adapt, build upon thisCreative Commons Attribution Non Commercial (CC BY-NC 3.0) This is an Open Access article distributed in accordance with the
serviceEmail alerting
the box at the top right corner of the online article.Receive free email alerts when new articles cite this article. Sign up in
http://group.bmj.com/group/rights-licensing/permissionsTo request permissions go to:
http://journals.bmj.com/cgi/reprintformTo order reprints go to:
http://group.bmj.com/subscribe/To subscribe to BMJ go to:
group.bmj.com on August 3, 2014 - Published by bmjopen.bmj.comDownloaded from


















