BMJ Open2 of unstable angina and non-ST-elevation myocardial infarction 3 Josien Engel, MSc* 1,...
101
For peer review only A cross-sectional multicenter study of cardiac risk score use in the management of unstable angina and non-ST- elevation myocardial infarction Journal: BMJ Open Manuscript ID: bmjopen-2015-008523 Article Type: Research Date Submitted by the Author: 16-Apr-2015 Complete List of Authors: Engel, Josien; EMGO Institute for Health and Care Research / VU University Medical Center, Public and Occupational Health Van der Wulp, Ineke; EMGO Institute for Health and Care Research / Vu University Medical Center, Public and Occupational Health de Bruijne, Martine; EMGO Institute, VU University Medical Center, Amsterdam, the Netherlands, Dept. of Public and Occupational Health Wagner, Cordula; NIVEL, Netherlands Institute for Health Services Research, ; EMGO Institute, VU University Medical Center, Amsterdam, the Netherlands, Dept. of Public and Occupational Health <b>Primary Subject Heading</b>: Health services research Secondary Subject Heading: Cardiovascular medicine, Evidence based practice, Health services research Keywords: acute coronary syndromes, risk assessment, guideline adherence, predictors, chart review For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml BMJ Open on July 10, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-008523 on 24 November 2015. Downloaded from
Transcript of BMJ Open2 of unstable angina and non-ST-elevation myocardial infarction 3 Josien Engel, MSc* 1,...

For peer review only
A cross-sectional multicenter study of cardiac risk score use in the management of unstable angina and non-ST-
elevation myocardial infarction
Journal: BMJ Open
Manuscript ID: bmjopen-2015-008523
Article Type: Research
Date Submitted by the Author: 16-Apr-2015
Complete List of Authors: Engel, Josien; EMGO Institute for Health and Care Research / VU University Medical Center, Public and Occupational Health Van der Wulp, Ineke; EMGO Institute for Health and Care Research / Vu
University Medical Center, Public and Occupational Health de Bruijne, Martine; EMGO Institute, VU University Medical Center, Amsterdam, the Netherlands, Dept. of Public and Occupational Health Wagner, Cordula; NIVEL, Netherlands Institute for Health Services Research, ; EMGO Institute, VU University Medical Center, Amsterdam, the Netherlands, Dept. of Public and Occupational Health
<b>Primary Subject Heading</b>:
Health services research
Secondary Subject Heading: Cardiovascular medicine, Evidence based practice, Health services research
Keywords: acute coronary syndromes, risk assessment, guideline adherence, predictors, chart review
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on July 10, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-008523 on 24 N
ovember 2015. D
ownloaded from

For peer review only
1
A cross-sectional multicenter study of cardiac risk score use in the management 1
of unstable angina and non-ST-elevation myocardial infarction 2
3
Josien Engel, MSc*1
, Ineke van der Wulp, PhD1
, Martine de Bruijne, PhD1
, Cordula Wagner, 4
PhD 1,2
5
6
1
EMGO Institute for Health and Care Research, Department of Public and Occupational 7
Health, VU University Medical Center, Amsterdam, the Netherlands 8
2
NIVEL, Netherlands Institute for Health Services Research, Utrecht, the Netherlands 9
10
* Corresponding Author: 11
Josien Engel; EMGO Institute for Health and Care Research, Department of Public and 12
Occupational Health, VU University Medical Center; Van der Boechorststraat 7, 1081 BT 13
Amsterdam, The Netherlands; Tel: +31 20 4445452; E-Mail: [email protected] 14
15
Key words: acute coronary syndromes, risk assessment, guideline adherence, predictors, 16
chart review 17
18
Word count: main text: 2822 words, abstract: 285 words 19
Number of figures/tables: 6 20
21
Page 1 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
2
STRENGTHS AND LIMITATIONS 22
• This multicenter study is the first to provide thorough insight in the extent of cardiac 23
risk score use in clinical practice by reviewing patient charts in thirteen hospital 24
throughout the Netherlands. 25
• Generalized Linear Mixed Models were used to study hospital- and patient-related 26
factors associated with lower or higher cardiac risk score use. 27
• The results can serve as a basis for future improvement initiatives to enhance cardiac 28
risk score use in practice, by tailoring strategies to patient groups in which risk scores 29
are less often documented; 30
• It was not possible to study associations between the extent of cardiac risk score use 31
and the occurrence of adverse patient outcomes (e.g. death) due to practical 32
constraints; 33
• Using retrospective review of medical charts as the underlying method of data 34
collection made it impossible to determine the actual influence of cardiac risk score 35
use on clinical decision making of health care providers involved in the management 36
of patients with unstable angina or non-ST-elevation Myocardial Infarction. 37
38
Page 2 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
3
ABSTRACT 39
40
Background: Quantitative risk assessment in unstable angina (UA) and non-ST-elevation 41
myocardial infarction (NSTEMI), by using cardiac risk scores, is recommended in 42
international guidelines. However, a gap between recommended care and actual practice 43
exists, as these instruments seem underused in practice. Prior to creating future improvement 44
initiatives to increase cardiac risk score use, knowledge about the extent of this gap and 45
associated factors is necessary. 46
Methods: A retrospective chart review of UA and NSTEMI patients, discharged in 2012, in 47
thirteen hospitals throughout the Netherlands was conducted. Generalized Linear Mixed 48
Models were used to study the factors associated with cardiac risk score use. 49
Results: A total of 1788 charts were eligible for analysis. In 57% (n=1019) of the charts, 50
physicians documented the use of a cardiac risk score. Substantial variation between hospitals 51
was observed (16.7% to 87%), although this variation could not be explained by the presence 52
of on-site revascularization facilities or a hospitals’ teaching status. Obese patients (OR=1.49; 53
CI 95%= 1.03–2.15) and former smokers (OR=1.56; CI 95%= 1.15–2.11) were more likely to 54
have a cardiac risk score documented. Risk scores were less likely being used among patients 55
diagnosed with unstable angina (OR=0.60; CI 95%= 0.46–0.77), in-hospital resuscitation 56
(OR=0.23; CI 95%= 0.09–0.64), in-hospital heart failure (OR=0.46; CI 95%= 0.27–0.76) or 57
tachycardia (OR=0.45; CI 95%= 0.26–0.75). 58
Conclusions: Despite recommendations in cardiac guidelines, the use of cardiac risk scores 59
has not been fully implemented in Dutch practice. A substantial number of patients did not 60
have a cardiac risk score documented in their chart. Strategies to improve cardiac risk score 61
use should pay special attention to patient groups in which risk scores were less often 62
documented, as these patients may currently be undertreated. 63
Page 3 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
4
BACKGROUND 64
65
In the past decade mortality rates in acute coronary syndromes, including unstable angina 66
(UA) and non-ST-elevation myocardial infarction (NSTEMI), decreased significantly due to 67
substantial improvements in treatment possibilities.[1, 2] Despite these advancements, these 68
conditions still account for a large part of the annual deaths worldwide and are expected to 69
account for the largest disease burden worldwide by 2020.[3, 4] Part of these deaths may be 70
prevented, as it has previously been reported that a substantial number of patients were not 71
treated according to the current standards of care.[5-7] Patients with diabetes mellitus, renal 72
insufficiency, signs of heart failure and patients aged 75 years or older, were often neglected 73
guideline recommended care.[5] On the other hand, patients presenting to academic hospitals 74
and to hospitals with revascularisation facilities on-site (e.g. percutaneous coronary 75
intervention (PCI) or coronary artery bypass grafting (CABG)), were more often treated in 76
accordance to the guidelines.[6,8] Patients diagnosed with UA or NSTEMI can be treated 77
with medication or invasive procedures such as PCI or CABG. According to international 78
cardiac guidelines the decision to treat such patients with one or the other may be made on the 79
basis of a quantitative assessment of the patient’s risk of re-infarction or death.[9-11] To assist 80
clinicians in identifying patients at high risk of adverse cardiac events that would benefit most 81
from invasive therapies, several instruments have been developed.[9-11] The GRACE (Global 82
registry of Acute Coronary Events),[12, 13] TIMI (Thrombolysis in Myocardial 83
Infarction),[14] FRISC (fast revascularization in instability in coronary disease),[15] 84
PURSUIT (Platelet glycoprotein IIb/IIIa in Unstable angina: Receptor Suppression Using 85
Integrilin),[16] and HEART risk scores [17] are examples of validated cardiac risk scoring 86
instruments. In estimating risk, these instruments incorporate and combine several diagnostic 87
elements including a patients’ history, biomarkers and electrocardiogram findings, and can be 88
Page 4 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
5
used in the emergency department or coronary care unit. The predictive validity of these 89
instruments was reported to be good.[15, 18, 19] Previous research found that cardiac risk 90
scores were effective in identifying patients at high risk for cardiac events.[20, 21] However, 91
it has been suggested that cardiac risk scores are not routinely used in clinical practice, which 92
possibly contributed to the perpetuating treatment risk paradox.[20, 22, 23] In this paradox 93
patients with low risk of adverse cardiac events, opposite to cardiac guideline 94
recommendations, were more likely to receive invasive cardiac treatment compared to high 95
risk patients.[5, 24-29] To improve physicians’ risk estimation on the one hand and efficient 96
use of resources on the other, the present study aimed to determine the extent of cardiac risk 97
score use in Dutch clinical practice and to study factors associated with lower or higher 98
cardiac risk score use. 99
100
METHODS 101
102
This study concerns a cross-sectional multicenter study. A detailed description of the study 103
protocol has been published previously.[30] The study protocol was reviewed and approved 104
by the medical ethical committee of the VU University Medical Center Amsterdam. Where 105
required, approval from hospitals’ local ethics board were obtained. 106
107
Setting 108
Thirteen hospitals in the Netherlands participated in this study. By a multistage random 109
sampling procedure, initially 12 hospitals were selected from a pool of 40 hospitals that 110
participated in a nationwide quality improvement program. The program comprised several 111
themes, including the theme ‘Optimal care for Acute Coronary Syndromes’ which, among 112
other things, aimed to increase the application of cardiac risk scores in clinical practice.[31] 113
Page 5 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
6
Additionally, one hospital was selected to obtain optimal diversity in on-site revascularization 114
facilities and teaching status. The final sample consisted of two university hospitals, seven 115
tertiary teaching hospitals, and four general hospitals. Bed capacity in the hospitals varied 116
between 200 and 1200 beds. 117
118
Data collection 119
The primary study outcome was the extent to which cardiac risk scores were used in the 120
management of UA and NSTEMI patients. Data were collected monthly by means of 121
retrospective chart review. 122
Potentially eligible charts were selected from the hospitals’ billing system based on 123
diagnostic-related group codes for UA and NSTEMI. All patients discharged in 2012, 18 124
years or older, with a diagnosis of UA or NSTEMI (as confirmed in the discharge letter) were 125
considered for inclusion. Charts of patients who were transferred in from another hospital 126
were excluded, as these patients were initially treated elsewhere and therefore the necessary 127
data could not be obtained. In addition, charts of patients who provided insufficient 128
information regarding the discharge diagnosis, who were hospitalized for an elective 129
procedure, or who had an underlying illness or condition, other than a coronary stenosis, 130
causing UA or NSTEMI (e.g. anemia) were excluded. 131
Charts of patients were selected per month in chronological order of discharge until the 132
screening capacity of the chart abstractors was reached. Charts of potentially eligible patients 133
were manually reviewed to confirm a discharge diagnosis of UA or NSTEMI. In case a 134
patient’s final discharge diagnosis was unclear, a physician of the cardiology department was 135
consulted. The following patient-related and hospital-related information was registered on 136
standardized data extraction forms, including the following: demographic characteristics, 137
cardiac history, presence of cardiac risk factors, presenting symptoms, biochemical and 138
Page 6 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
7
electrocardiographic findings and treatment practices. In addition, information regarding 139
cardiac risk score use was registered, including the use of a validated risk score (yes/no), date 140
of application, type of risk score used and risk score outcome and classification. Besides 141
patient related information, the following hospital factors were registered: teaching status 142
(yes/no) and the presence of on-site revascularization facilities. 143
The data were entered into a database using fixed entry fields (BLAISE version 4.7, Statistics 144
Netherlands) and data reliability checks were conducted. To ensure reliable data extraction, 145
more than 5% (103/1933) of the charts were screened by two chart abstractors independently. 146
The total percentage of agreement between these abstractors was 95.1%, and ranged for the 147
variables of interest (Box 1) between 80.6% (electrocardiographic findings) and 100% 148
(gender), indicating good to excellent data reliability. 149
150
Box 1 Independent variables in Generalized Linear Mixed Model
Patient characteristics Patient characteristics Patient characteristics
Demographics
• Age
• Gender
Presenting factors
• Heart rate
• Systolic blood pressure
• Resuscitation at admission
• Cardiogenic shock
• In-hospital heart failure
• ST deviations on ECG
Discharge diagnosis
• UA
• NSTEMI
Cardiac history
• Coronary artery disease
• Peripheral vascular disease
• (Unstable) angina pectoris
• Acute myocardial infarction
• Previous CABG
• Previous PCI
• Revascularization/AMI < 6
months
Risk factors
• Diabetes mellitus
• Hypertension
• Renal failure
• Chronic heart failure
• Positive family history
• Smoking
• Former smoker
• Hypercholesterolemia*
• Obesity (BMI > 30)
• Coronary stenosis ≥50%
(in history)
Hospital characteristics
• Presence of revascularisation
options
• Teaching status
Abbreviations: ECG, electrocardiogram; UA, unstable angina; NSTEMI, non-ST-elevation myocardial
infarction; CABG, Coronary artery bypass graft surgery; PCI, Percutaneous coronary intervention; AMI, acute
myocardial infarction; BMI, body mass index. *Defined as statin use prior to admission, or described in
patients history (elevated cholesterol levels, hyperlipidaemia or hypercholesterolemia).
151
Page 7 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
8
Missing data 152
In total 1.5% of the values in the dataset were missing, ranging from 0.1% to 22% per 153
variable. Eleven variables had no missing values, including cardiac risk score use. Despite the 154
small amount of missing data and the spread of missing data in the dataset, a complete case 155
analysis would have led to a large loss of information and power. Therefore, missing values 156
were imputed using a multiple imputation procedure following the approach of van Buuren, 157
[32] resulting in five imputed datasets. In imputing missing values it was assumed that the 158
data were missing at random. The estimated values were corrected for the variables ‘hospital’ 159
and ‘cardiac risk score use’ as these variables were of primary interest in the analyses. By 160
means of the Kolmogorov-Smirnov test, and density and residual plots, it was determined, 161
whether the missing at random assumption was sustainable and the imputed values were 162
plausible. In addition, a sensitivity analysis was conducted by comparing the results from the 163
analyses of the imputed data with the results of a complete case analysis. Between these 164
models, only small differences were found. The missing value analyses and their imputations 165
were conducted in R (version 3.0.2 for Microsoft Windows) using the MICE package.[32, 33] 166
167
Data analysis 168
Sample characteristics were calculated using descriptive statistics, and included frequencies 169
and percentages for categorical variables, and means and standard deviations for continuous 170
variables. Associations of independent variables (box 1) with the use of cardiac risk scores 171
(yes/no) were studied with a generalized linear mixed model (GLMM), taking into account 172
the clustering of data within hospitals.[34] Odds ratios, that are based on median probabilities 173
over hospitals for cardiac risk score use, are presented. To facilitate interpretation, relevant 174
explanatory variables were transformed into categorical variables (i.e. age, heart rate and 175
systolic blood pressure). Furthermore, month of discharge was represented by a categorical 176
Page 8 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
9
variable with 12 levels in every model, to account for the fact that chart abstractors were 177
present to abstract data. In univariate analyses, associations between cardiac risk score use 178
and the independent variables were tested. All variables with a significance level of p≤0.15 179
were entered in a multivariable model. Variables significantly associated (p≤0.05) with 180
cardiac risk score use in the multivariable model were considered important in predicting risk 181
score adherence. In addition, based on previous literature two factor interactions with on-site 182
revascularization options, teaching status, age and gender were tested. All analyses were 183
conducted in R for windows (version 3.0.2) using the package lme4 on pooled data of five 184
imputed data sets.[33] The script of the pool function in MICE was rewritten for pooling 185
GLMM models. 186
187
RESULTS 188
189
Study population 190
A total of 1933 charts of patients with a confirmed diagnoses of UA or NSTEMI were 191
screened. Of these, 145 (7.5%) were excluded from the study as these concerned patients 192
transferred from one hospital to another, leaving 1788 patients for further analysis (Figure 1). 193
The majority (62.6%) of these patients had a discharge diagnosis of NSTEMI (Table 1). 194
Males accounted for 66.9% of the patients, and more than a third (35.9%) of the patients were 195
aged 75 years or older. Three quarters (75.3%) of the total population underwent coronary 196
catheterization. The average length of hospital stay was five days (SD 4.97). 197
198
199
200
201
Page 9 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
10
Table 1. Baseline characteristics (pooled data) (n= 1788) n (%)†
Age (<75 years) 1146 (64.1)
Gender (male) 1196 (66.9)
Discharge diagnoses (NSTEMI) 1119 (62.6)
Length of hospital stay (days) (mean ± SD) 5 ± 4.97
Systolic blood pressure (mmHg)
High (≥ 160) 552 (30.9)
Normal to slightly elevated (81-159) 1236 (69.1)
Low (≤ 80) 0 (0)
Heart rate (bpm)
Tachycardia (≥ 110) 103 (5.8)
Normal (51-109) 1634 (91.4)
Bradycardia (≤ 50) 51 (2.8)
Resuscitation at admission 33 (1.9)
Cardiogenic shock 7 (0.4)
In-hospital heart failure 103 (5.8)
ST deviations on electrocardiogram 810 (45.3)
History of coronary artery disease 252 (14.1)
History of peripheral vascular disease 131 (7.3)
Previous (U)A 432 (24.1)
Previous MI 499 (27.9)
Previous PCI 523 (29.3)
Previous CABG 289 (16.2)
MI or PCI/CABG 6 months prior to admission 125 (7)
Diabetes mellitus 451 (25.2)
Hypertension 936 (52.4)
Renal failure 88 (4.9)
Chronic heart failure 101 (5.7)
Hypercholesterolemia‡ 986 (55.1)
Obesity (BMI>30) 203 (11.3)
Smoking 427 (23.9)
Former smoker 350 (19.6)
Coronary stenosis (≥50%) 192 (10.8)
Positive family history 618 (34.6)
Coronary catheterization 1346 (75.3)
Management strategy
Pharmacological therapy 754 (42.2)
(scheduled) PCI 846 (47.3)
(scheduled) CABG 188 (10.5)
Page 10 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
11
†Data are presented in n(%), unless stated otherwise. ‡ Defined as statin use prior to
admission, or described in patients history (elevated cholesterol levels, hyperlipidaemia or
hypercholesterolemia).Abbreviations: n.a., not applicable; (U)A, (Unstable)Angina; MI,
myocardial infarction; PCI, percutaneous coronary intervention; CABG, coronary artery
bypass grafting; BMI, body mass index.
202
Cardiac risk score use 203
In 57% of the patient charts, a cardiac risk score was documented, though, substantial 204
variation between hospitals was observed i.e. 16.7% to 87% (Table 2). The variance 205
component for the random hospital effect in the GLMM ranged between 1.29 and 1.31 in the 206
five imputed datasets, confirming the great variety between hospitals in the use of cardiac risk 207
scores. When, for instance, the effects for two hospitals are equal to the 5 and 95 percentiles 208
of the normal distribution with variance 1.3 for hospital effects, the odds ratio of one hospital 209
relative to the other for cardiac risk score use is 42.6. 210
In univariate analyses, 15 patient related factors were significantly (p≤0.15) associated with 211
cardiac risk score use (Table 3). No significant associations with hospital related factors were 212
found (teaching status p=0.25, on-site revascularisation facilities p=0.67). In multivariable 213
analyses, patients with obesity (OR=1.49; 95%CI= 1.03-2.15; p=0.04) and former smokers 214
(OR=1.56; 95% CI=1.15-2.11; p≤0.01) were more likely to have a cardiac risk score 215
documented. Conversely patients with UA (OR=0.60; 95% CI=0.46-0.77; p≤0.01), in-hospital 216
heart failure (OR=0.46; 95% CI=0.27-0.76; p≤0.01), tachycardia (OR=0.45; 95% CI=0.26-217
0.75; p≤0.01) or who had been resuscitated at admission (OR=0.23; 95% CI=0.09-0.64; 218
p≤0.01) were less likely to have a cardiac risk score documented (Table 3). 219
220
221
222
223
Page 11 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
12
224
225
226
227
228
229
230
231
232
233
234
235
236
237
238
239
Table 2. Adherence to cardiac risk score use per hospital (pooled data)
Hospital
ID†
Teaching
status
Revascularization
options
Screened patient
charts n‡
Risk score use
n (%)
1 No No 84 14 (16.7)
2 Yes Yes 109 22 (20.2)
3 No No 110 26 (23.6)
4 No No 171 57 (33.3)
5 Yes Yes 132 46 (34.8)
6 Yes No 53 19 (35.8)
7 Yes Yes 145 79 (54.5)
8 Yes Yes 182 108 (59.3)
9 Yes Yes 96 68 (70.8)
10 Yes Yes 140 107 (76.4)
11 Yes Yes 108 87 (80.6)
12 No No 205 166 (81.0)
13 Yes No 253 220 (87.0)
Total -- -- 1788 1019 (57%)
† ranging from lowest to highest scoring hospital. ‡ Large variation in screened patient charts
per hospital is explained by differences in the amount of monthly admission for
UA/NSTEMI.
Page 12 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
13
Table 3. Univariate and multivariable associations between risk score documentation in patient charts and
hospital- and patient related factors (pooled data) (n=1788) †
Univariate associations Multivariable associations
OR (95% CI) P OR (95% CI) P
Hospital factors
Teaching status 2.15 (0.59 – 7.85) 0.25 n.a. n.a.
On-site revascularisation facilities 1.32 (0.38 – 4.60) 0.67 n.a. n.a.
Patient factors‡
Discharge diagnosis (reference NSTEMI) 0.65 (0.52 – 0.83) ≤0.01** 0.60 (0.46 – 0.77) ≤0.01**
Age (reference <75 years) 0.76 (0.61 – 0.96) 0.02* 0.86 (0.67 – 1.11) 0.24
Resuscitation at admission 0.25 (0.10 – 0.67) ≤0.01** 0.23 (0.09 – 0.64) ≤0.01**
In-hospital heart failure 0.38 (0.24 -0.62) ≤0.01** 0.46 (0.27 – 0.76) ≤0.01**
History of coronary artery disease 0.65 (0.47 – 0.89) ≤0.01** 0.87 (0.59 – 1.27) 0.46
History of peripheral artery disease 0.72 (0.47 – 1.09) 0.12 0.81 (0.53 – 1.26) 0.35
Previous (U)A 0.83 (0.64 – 1.07) 0.15 1.00 (0.75 – 1.34) 0.98
Previous MI 0.77 (0.61 – 0.98) 0.03* 0.89 (0.68 – 1.18) 0.43
Previous PCI 0.83 (0.65 – 1.05) 0.13 1.07 (0.80 – 1.43) 0.66
Renal failure 0.54 (0.33 – 0.90) 0.02* 0.72 (0.42 – 1.23) 0.23
Obesity (BMI>30) 1.49 (1.05 – 2.13) 0.03* 1.49 (1.03 – 2.15) 0.04*
Smoking 1.23 (0.95 – 1.60) 0.11 1.16 (0.86 – 1.55) 0.33
Former smoker 1.48 (1.12 – 1.97) ≤0.01** 1.56 (1.15 – 2.11) ≤0.01**
Coronary stenosis (≥50%) 0.65 (0.46 – 0.93) 0.02* 0.81 (0.54 – 1.22) 0.31
Heart rate (bpm) (reference Normal)
Tachycardia 0.46 (0.28 – 0.76) ≤0.01** 0.45 (0.26 – 0.75) ≤0.01**
Bradycardia 0.85 (0.44 – 1.63) 0.62 0.92 (0.46 – 1.86) 0.82
† pooled p-value based on normal approximation. ‡Only variables (patient characteristics) with p ≤ 0.15 in the
univariate analyses are presented in this table. Reference category is ‘no’, unless stated otherwise. *p-value ≤
0.05; **p-value ≤0.01. Abbreviations: OR, odds ratio; CI, 95% confidence interval; n.a., not applicable; PCI,
percutaneous coronary intervention; CABG: coronary artery bypass grafting; (U)A, (Unstable)Angina; MI,
myocardial infarction; BMI, body mass index.
240
Page 13 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
14
Interactions 241
Besides the interactions with on-site revascularization options, teaching status, age and 242
gender, it was decided to also test whether interactions with former smoker were present. This 243
was because an unexpected significant association between former smoker and risk score use 244
was found. Significant interactions were found between the variables former smoker and 245
discharge diagnosis (p=0.03), age and previous PCI (p=0.02), age and in-hospital heart failure 246
(p=0.04), age and history of peripheral artery disease (p=0.03), and age and heart rate 247
(p=0.04) (Table 4). 248
Looking at the interaction effects with age, it was found that patients aged 75 years or over 249
presenting with a previous PCI had a higher odds of cardiac risk score documentation 250
compared to patients without a previous PCI (OR=1.53; 95% CI=1.00 – 2.34; p=0.05). In 251
contrast, older patients were less likely to have a cardiac risk score documented in case they 252
presented with heart failure (OR=0.29; 95% CI=0.14 – 0.57; p<0.001), with a history of 253
peripheral artery disease (OR=0.47; 95% CI=0.24 – 0.91; p=0.02) or with tachycardia 254
(OR=0.20; 95% CI=0.08 – 0.52; p=<0.001). 255
256
257
Page 14 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
15
Table 4. Estimated odds ratio’s and 95% confidence intervals for significant (p≤0.05) interactions terms
added to multivariable model of GLMM (pooled data) †
OR CI 95% P-value‡
Former smoker*discharge diagnosis
Discharge diagnosis (UA vs. NSTEMI) within former smoker (no) 0.52 0.40 – 0.69 <0.001**
Discharge diagnosis (UA vs. NSTEMI) within former smoker (yes) 1.00 0.59 – 1.71 0.98
Former smoker (yes vs. no) within discharge diagnosis (UA) 2.28 1.43 – 3.61 <0.001**
Former smoker (yes vs. no) within discharge diagnosis (NSTEMI) 1.19 0.81 – 1.75 0.38
Age*previous PCI
Age (≥75 vs. <75 years) within previous PCI (no) 0.71 0.52 – 0.96 0.02*
Age (≥75 vs. <75 years) within previous PCI (yes) 1.30 0.84 – 1.99 0.23
Previous PCI (yes vs. no) within age (<75 years) 0.84 0.58 – 1.19 0.32
Previous PCI (yes vs. no) within age (≥75 years) 1.53 1.00 – 2.34 0.05*
Age*in-hospital heart failure
Age (≥75 vs. <75 years) within in-hospital heart failure (no) 0.92 0.71 – 1.20 0.54
Age (≥75 vs. <75 years) within in-hospital heart failure (yes) 0.32 0.12 – 0.85 0.02*
In-hospital heart failure (yes vs. no) within age (<75 years) 0.84 0.39 – 1.82 0.66
In-hospital heart failure (yes vs. no) within age (≥75 years) 0.29 0.14 – 0.57 <0.001**
Age*History of peripheral artery disease
Age (≥75 vs. <75 years) within history of peripheral artery disease (no) 0.93 0.72 – 1.21 0.60
Age (≥75 vs. <75 years) within history of peripheral artery disease (yes) 0.34 0.14 – 0.80 0.01**
History of peripheral artery disease (yes vs. no) within age (<75 years) 1.28 0.70 – 2.32 0.42
History of peripheral artery disease (yes vs. no) within age (≥75 years) 0.47 0.24 – 0.91 0.02*
Age*Heart rate
Age (≥75 vs. <75 years) within heart rate (normal) 0.91 0.70 – 1.18 0.47
Age (≥75 vs. <75 years) within heart rate (tachycardia) 0.28 0.09 – 0.85 0.03*
Age (≥75 vs. <75 years) within heart rate (bradycardia) 1.25 0.31 – 5.00 0.75
Heart rate (tachycardia vs. normal) within age (<75 years) 0.67 0.34 – 1.30 0.23
Heart rate (bradycardia vs. normal) within age (<75 years) 0.81 0.33 – 2.01 0.65
Heart rate (tachycardia vs. normal) within age (≥75 years) 0.20 0.08 – 0.52 <0.001**
Heart rate (bradycardia vs. normal) within age (≥75 years) 1.12 0.38 – 3.27 0.84
Page 15 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
16
†All four OR’s per interaction term are presented in the table to form an impression of the nature of the interaction.
For instance, two separate OR’s for former smoker no versus yes for UA and NSTEMI patients and two separate
OR’s for UA versus NSTEMI for former smoker no and yes. These four OR’s are all shown, because when
interaction between two factors is added to the model, the OR of one factor may depend upon the level of the other
factor. ‡P-value indicates if OR is significantly different from one. *p-value ≤ 0.05; **p-value ≤0.01.Abbreviations:
OR, odds ratio; CI 95%, 95% confidence interval; UA, unstable angina; NSTEMI, non-ST-elevation myocardial
infarction.
258
Page 16 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
17
DISCUSSION 259
260
This study aimed to provide insight in the extent of cardiac risk score use in Dutch hospitals 261
as recommended by international cardiac guidelines. In addition, associations with patient and 262
hospital related factors were studied. Substantial variation between hospitals’ cardiac risk 263
score use was observed, with in approximately 40% of patient charts a cardiac risk score was 264
not documented. Several patient related factors including a diagnosis of UA, the presence of 265
in-hospital heart failure, tachycardia, and resuscitation at admission were associated with a 266
lower likelihood of cardiac risk score use. Also the likelihood of cardiac risk score use was 267
often lower in older patients (≥ 75 years) with additional conditions, such as in-hospital heart 268
failure, a history of peripheral artery disease or tachycardia. 269
Previous studies also reported advanced age, heart failure and tachycardia as important 270
predictors of lower guideline adherence in patients with acute coronary syndromes.[5, 35-40] 271
Moreover, several of these studies also reported a decreased likelihood of survival. [36 ,37, 272
39] Implying that patients at high risk for adverse cardiac outcomes are less likely to receive 273
guideline recommended care. However, according to the European guidelines these high risk 274
subgroups of patients benefit most from early invasive treatments[9]. It may, however, be 275
discussed to what degree an invasive treatment may be desired in these high risk subgroups of 276
patients. Also, it could be questionable to what degree risk stratification using a cardiac risk 277
score adds value in deciding on the treatment for these patients, e.g. in the case of 278
resuscitation the decision for a certain procedure may be evident. The European Society of 279
Cardiology guidelines however, do not take these circumstances into account and recommend 280
estimating risk levels with a cardiac risk scoring instrument for every patient suspected of 281
UA/NSTEMI.[9] 282
Page 17 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
18
An interesting finding, that contrasted the findings of previous studies, was that a hospitals’ 283
teaching status or the presence of on-site revascularisation facilities were not significantly 284
associated with cardiac risk score use.[6, 35] These differences may be explained by the 285
relatively small number of hospitals participating in the present study compared to previous 286
studies. A large variation between hospitals in adherence scores regarding cardiac risk score 287
use were found. The large component of variance explained by the random hospital effect 288
suggests that cardiac risk score use in patients presenting with the same characteristics may 289
heavily depend on which hospital the patient is presented in and that other factors, beside a 290
hospital’s teaching status or on-site revascularisation facilities, are of influence. 291
Common barriers in the implementation of cardiac risk scores, including the absence of 292
necessary resources for implementation and cultural differences, may explain this substantial 293
variation.[41] It has also been suggested that physicians find the evidence underlying cardiac 294
risk scores unconvincing.[23] To increase the use of cardiac risk scores in clinical practice 295
several implementation strategies, which pay explicit attention to patients with suspected UA 296
may be employed. A recent improvement initiative in the USA for instance, in which 297
continuous education was the primary intervention, led to a significant increase in cardiac risk 298
score documentation in UA and NSTEMI patients.[42] The use of continuous education has 299
proven to be effective in achieving change in practice, however it is recommended to also 300
take into account facilitating factors and barriers on a patient, provider and organizational 301
level.[43] Therefore, further research is needed to carefully understand factors that explain the 302
variation between hospitals’ cardiac risk score use. 303
304
Study limitations 305
Several limitations potentially affect the interpretation of the results of this study. First, the 306
use of cardiac risk scores was measured by screening charts on the documentation of a cardiac 307
Page 18 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
19
risk score. As a result it is unknown to what degree a cardiac risk score influenced physicians’ 308
decision making regarding appropriate management strategies. However, it is plausible that 309
when a cardiac risk score was documented, it was also used in practice. 310
Second, four predictors reported in previous studies of risk score use i.e. aspirin use prior to 311
admission, creatinine level, troponin level and biomarkers, were not considered in the present 312
study. These data could not be abstracted reliably. As a result, the precision of the model 313
reported in this study might be smaller compared to other studies. 314
Third, in two hospitals the method of selection of patient charts differed, as it was not possible 315
to select patients based on the hospital’s billing system. This could have influenced the 316
selection of patients. However, their effects may be limited as it appeared that the random 317
effects of these two hospitals were well in range with those of the other hospitals. 318
Finally, it was not possible to extract all data from the charts at one time point per hospital. 319
Therefore, monthly data collection visits were deemed necessary. For this reason, the reported 320
associations were corrected for month of discharge, though, the frequent presence of the 321
researchers on-site may have led to more awareness of the health care providers using cardiac 322
risk scores, and as a result higher adherence scores than in hospital not participating in the 323
evaluation of the quality improvement program. 324
325
CONCLUSIONS 326
327
The results of the present study indicate that cardiac risk scores have not been fully 328
implemented in Dutch clinical practice, as a substantial number of patients had no risk score 329
documented in their chart. The large variation between hospitals could not be explained by the 330
presence of on-site revascularization facilities or a hospitals’ teaching status, as well as by 331
several patient related factors that were associated with higher or lower usage of cardiac risk 332
Page 19 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
20
scores in clinical practice. It is recommended that further research should focus first on 333
explanatory factors for differences between hospitals, which could provide a basis for future 334
improvement initiatives in which strategies are targeted towards patient groups in which risk 335
scores were less often documented, as these patients may currently be undertreated. 336
337
ACKNOWLEDGEMENTS 338
We would like to thank Marie-Julie Heeren, Felix van Urk, Suzanne Vonk and Rixt Zuidema 339
for their support in data collection. 340
341
COMPETING INTERESTS 342
The authors declare that they have no competing interests. 343
344
AUTHORS’ CONTRIBUTION 345
All authors made substantial contributions to conception and design of the study. JE carried 346
out data collection, performed statistical analysis, and drafted the manuscript, and prepared 347
the manuscript for publication. IvdW provided substantial support in imputation of data and 348
statistical analysis. IvdW, MdB and CW made substantial contributions to interpretation of 349
the data and revised the manuscript critically for important intellectual content. All authors 350
read and approved the final manuscript. 351
352
FUNDING 353
The study was funded by the Dutch Ministry of Public health, Welfare and Sports. The study 354
sponsor had no role in the study design, collection, analysis and interpretation of the data, or 355
in writing of the manuscript and decision to submit the manuscript for publication. 356
357
Page 20 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
21
358
Page 21 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
22
REFERENCES 359
360
1. Fox KAA, Steg PG, Eagle KA, et al. Decline in rates of death and heart failure in acute 361
coronary syndromes, 1999-2006. JAMA 2007,297:1892-1900. 362
2. Yeh RW, Sidney S, Chandra M, et al. Population trends in the incidence and outcomes 363
of acute myocardial infarction. N Engl J Med 2010,362:2155-2165. 364
3. Lopez AD, Murray CJ. The global burden of disease. A comprehensive assessment of 365
mortality and disability from diseases, injuries and risk factors in 1990 and projected to 366
2020. Cambridge MA: Harvard University Press 1996. 367
4. Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 368
1990-2020: Global Burden of Disease Study. Lancet 1997,349:1498-1504. 369
5. Roe MT, Peterson ED, Newby LK, et al. The influence of risk status on guideline 370
adherence for patients with non-ST-segment elevation acute coronary syndromes. Am 371
Heart J 2006,151:1205-1213. 372
6. Peterson ED, Roe MT, Mulgund J, et al. Association between hospital process 373
performance and outcomes among patients with acute coronary syndromes. JAMA 374
2006,295:1912-1920. 375
7. Gulati M, Patel S, Jaffe AS, et al. Impact of contemporary guideline compliance on risk 376
stratification models for acute coronary syndromes in The Registry of Acute Coronary 377
Syndromes. Am J Cardiol 2004,94:873-878. 378
8. Patel MR, Chen AY, Roe MT, et al. A comparison of acute coronary syndrome care at 379
academic and nonacademic hospitals. Am J Med 2007,120:40-46. 380
Page 22 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
23
9. Hamm CW, Bassand JP, Agewall S, et al. ESC Guidelines for the management of acute 381
coronary syndromes in patients presenting without persistent ST-segment elevation: The 382
Task Force for the management of acute coronary syndromes (ACS) in patients 383
presenting without persistent ST-segment elevation of the European Society of 384
Cardiology (ESC). Eur Heart J 2011,32:2999-3054. 385
10. Anderson JL, Adams CD, Antman EM, et al. ACC/AHA 2007 guidelines for the 386
management of patients with unstable angina/non ST-elevation myocardial infarction: a 387
report of the American College of Cardiology/American Heart Association Task Force 388
on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the 389
Management of Patients With Unstable Angina/Non ST-Elevation Myocardial 390
Infarction): developed in collaboration with the American College of Emergency 391
Physicians, the Society for Cardiovascular Angiography and Interventions, and the 392
Society of Thoracic Surgeons: endorsed by the American Association of Cardiovascular 393
and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. 394
Circulation 2007,116:e148-e304. 395
11. Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC Guideline for the 396
Management of Patients With Non-ST-Elevation Acute Coronary Syndromes: A Report 397
of the American College of Cardiology/American Heart Association Task Force on 398
Practice Guidelines. Circulation 2014,130:2354-2394. 399
12. Granger CB, Goldberg RJ, Dabbous O, et al. Predictors of hospital mortality in the 400
global registry of acute coronary events. Arch Intern Med 2003,163:2345-2353. 401
13. Fox KA, Dabbous OH, Goldberg RJ, et al. Prediction of risk of death and myocardial 402
infarction in the six months after presentation with acute coronary syndrome: 403
prospective multinational observational study (GRACE). BMJ 2006,333:1091. 404
Page 23 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
24
14. Antman EM, Cohen M, Bernink PJ, et al. The TIMI risk score for unstable angina/non-405
ST elevation MI: A method for prognostication and therapeutic decision making. JAMA 406
2000,284:835-842. 407
15. Lagerqvist B, Diderholm E, Lindahl B, et al. FRISC score for selection of patients for an 408
early invasive treatment strategy in unstable coronary artery disease. Heart 409
2005,91:1047-1052. 410
16. Boersma E, Pieper KS, Steyerberg EW, et al. Predictors of outcome in patients with 411
acute coronary syndromes without persistent ST-segment elevation. Results from an 412
international trial of 9461 patients. The PURSUIT Investigators. Circulation 413
2000,101:2557-2567. 414
17. Six AJ, Backus BE, Kelder JC. Chest pain in the emergency room: value of the HEART 415
score. Neth Heart J 2008,16:191-196. 416
18. de Araujo GP, Ferreira J, Aguiar C, et al. TIMI, PURSUIT, and GRACE risk scores: 417
sustained prognostic value and interaction with revascularization in NSTE-ACS. Eur 418
Heart J 2005,26:865-872. 419
19. Backus BE, Six AJ, Kelder JC, et al. Chest pain in the emergency room: a multicenter 420
validation of the HEART Score. Crit Pathw Cardiol 2010,9:164-169. 421
20. Yan AT, Yan RT, Tan M, et al. Risk scores for risk stratification in acute coronary 422
syndromes: useful but simpler is not necessarily better. Eur Heart J 2007,28:1072-1078. 423
21. Chew DP, Juergens C, French J, et al. An examination of clinical intuition in risk 424
assessment among acute coronary syndromes patients: observations from a prospective 425
multi-center international observational registry. Int J Cardiol 2014,171:209-216. 426
Page 24 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
25
22. Manfrini O, Bugiardini R. Barriers to clinical risk scores adoption. Eur Heart J 427
2007,28:1045-1046. 428
23. Van de Werf F, Ardissino D, Bueno H, et al. Acute coronary syndromes: considerations 429
for improved acceptance and implementation of management guidelines. Expert Rev 430
Cardiovasc Ther 2012,10:489-503. 431
24. Yan AT, Yan RT, Tan M, et al. In-hospital revascularization and one-year outcome of 432
acute coronary syndrome patients stratified by the GRACE risk score. Am J Cardiol 433
2005,96:913-916. 434
25. Yan AT, Yan RT, Tan M, et al. Management patterns in relation to risk stratification 435
among patients with non-ST elevation acute coronary syndromes. Arch Intern Med 436
2007,167:1009-1016. 437
26. Fox KA, Anderson FA, Jr., Dabbous OH et al. Intervention in acute coronary 438
syndromes: do patients undergo intervention on the basis of their risk characteristics? 439
The Global Registry of Acute Coronary Events (GRACE). DHeart 2007,93:177-182. 440
27. Heras M, Bueno H, Bardaji A et al. Magnitude and consequences of undertreatment of 441
high-risk patients with non-ST segment elevation acute coronary syndromes: insights 442
from the DESCARTES Registry. Heart 2006,92:1571-1576. 443
28. Lee CH, Tan M, Yan AT, et al. Use of cardiac catheterization for non-ST-segment 444
elevation acute coronary syndromes according to initial risk: reasons why physicians 445
choose not to refer their patients. Arch Intern Med 2008,168: 291-296. 446
Page 25 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
26
29. Motivala AA, Cannon CP, Srinivas VS, et al. Changes in myocardial infarction 447
guideline adherence as a function of patient risk: an end to paradoxical care? J Am Coll 448
Cardiol 2011,58: 1760-1765. 449
30. Tra J, Engel J, van der Wulp I et al. Monitoring guideline adherence in the management 450
of acute coronary syndrome in hospitals: design of a multicentre study. Neth Heart J 451
2014,22: 346-53. 452
31. VMSzorg. Optimal care in Acute Coronary Syndromes [Original title in Dutch: Optimale 453
zorg in Acute Coronaire Syndromen]. Dutch National Patient Safety Programme. 2010 454
Http://www.vmszorg.nl/Themas/ACS 455
32. van Buuren S, Groothuis-Oudshoorn K (Eds). mice: Multivariate Imputation by Chained 456
Equations in R. In Journal of Statistical Software 2011,45:1-67. 457
33. R Core Team. R: A language and environment for statistical computing. 2013. Vienna, 458
Austria, R Foundation for Statistical Computing. http://www.R-project.org. 459
34. McCulloch CE, Searle SR, Neuhaus JM: Generalized, Linear, and Mixed Models., 2 460
edn. New Jersey: John Wiley & Sons, 2008. 461
35. Kumbhani DJ, Fonarow GC, Cannon CP et al. Predictors of adherence to performance 462
measures in patients with acute myocardial infarction. Am J Med 2013,126:74-79. 463
36. Scott IA, Harper CM. Guideline-discordant care in acute myocardial infarction: 464
predictors and outcomes. Med J Aust 2002,177:26-31. 465
37. Allen LA, O'Donnell CJ, Camargo CAJ et al. Comparison of long-term mortality across 466
the spectrum of acute coronary syndromes. Am Heart J 2006,151:1065-1071. 467
Page 26 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
27
38. Tran CTT, Laupacis A, Mamdani MM, et al. Effect of age on the use of evidence-based 468
therapies for acute myocardial infarction. Am Heart J 2004,148:834-841. 469
39. Ohman EM, Roe MT, Smith SCJ et al. Care of non-ST-segment elevation patients: 470
insights from the CRUSADE national quality improvement initiative. Am Heart J 471
2004,148:S34-S39. 472
40. Haim M, Battler A, Behar S et al. Acute coronary syndromes complicated by 473
symptomatic and asymptomatic heart failure: does current treatment comply with 474
guidelines? Am Heart J 2004,147:859-864. 475
41. Glickman SW, Boulding W, Staelin R et al. A framework for quality improvement: an 476
analysis of factors responsible for improvement at hospitals participating in the Can 477
Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with 478
Early Implementation of the ACC/AHA Guidelines (CRUSADE) quality improvement 479
initiative. Am Heart J 2007,154:1206-1220. 480
42. Cannon CP, Hoekstra JW, Larson DM et al. A report of quality improvement in the care 481
of patients with acute coronary syndromes. Crit Pathw Cardiol 2011,10: 29-34. 482
43. Grol R, Grimshaw J. From best evidence to best practice: effective implementation of 483
change in patients' care. Lancet 2003,362: 1225-1230. 484
485
486
487
488
489
490
491
Page 27 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
28
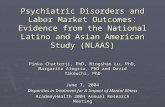
Figure 1. Inclusion and exclusion procedure of chart selection and screening 492
Page 28 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
Figure 1. Inclusion and exclusion procedure of chart selection and screening
Screened charts
n=1933
Sample study
n=1788
Exclusion chart, because:
- Age < 18
- Elective admission/procedure
- UA/NSTEMI due to non-ischemic cause
- Insufficient information in chart
Exclusion chart, because:
- patient is transferred in from another
hospital (n=145).
Identified
records from
hospital billing
system based on
discharge
diagnosis
Confirmation
discharge
diagnosis of UA
or NSTEMI Consultation of attending physician:
UA/NSTEMI?
Charts fulfill all
eligible criteria No
Yes
Exclusion of chart
Doubt
Yes
No No
Page 29 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
STROBE 2007 (v4) Statement—Checklist of items that should be included in reports of cross-sectional studies
Although we are aware of the SPIRIT checklist, the STROBE checklist seems most suited for this manuscript, as it describes the study design of a cross-sectional
study. The SPIRIT checklist is specifically developed for reporting randomized trials and therefore its applicability to the contents of the present manuscript is
limited. In addition, some parts of the STROBE checklist will not be applicable to our manuscript, these will be left empty.
Section/Topic Item
# Recommendation Reported on page #
Title and abstract 1 (a) Indicate the study’s design with a commonly used term in the title or the abstract 1
(b) Provide in the abstract an informative and balanced summary of what was done and what was found 3
Introduction
Background/rationale 2 Explain the scientific background and rationale for the investigation being reported 4-5
Objectives 3 State specific objectives, including any prespecified hypotheses 5
Methods
Study design 4 Present key elements of study design early in the paper 5
Setting 5 Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data
collection
5-7
Participants
6
(a) Give the eligibility criteria, and the sources and methods of selection of participants 6
Variables 7 Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic criteria, if
applicable
6
Data sources/
measurement
8* For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe
comparability of assessment methods if there is more than one group
6
Bias 9 Describe any efforts to address potential sources of bias 7
Study size 10 Explain how the study size was arrived at 6
Quantitative variables 11 Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and
why
8-9
Statistical methods 12 (a) Describe all statistical methods, including those used to control for confounding 8-9
(b) Describe any methods used to examine subgroups and interactions 8-9
(c) Explain how missing data were addressed 8
Page 30 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-008523 on 24 November 2015. Downloaded from

For peer review only
(d) If applicable, describe analytical methods taking account of sampling strategy n.a.
(e) Describe any sensitivity analyses 8
Results
Participants 13* (a) Report numbers of individuals at each stage of study—eg numbers potentially eligible, examined for eligibility,
confirmed eligible, included in the study, completing follow-up, and analysed
9
(b) Give reasons for non-participation at each stage n.a.
(c) Consider use of a flow diagram Figure 1
Descriptive data 14* (a) Give characteristics of study participants (eg demographic, clinical, social) and information on exposures and potential
confounders
9
(b) Indicate number of participants with missing data for each variable of interest 7-8
Outcome data 15* Report numbers of outcome events or summary measures 9
Main results 16 (a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (eg, 95% confidence
interval). Make clear which confounders were adjusted for and why they were included
9-11
(b) Report category boundaries when continuous variables were categorized
(c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period
Other analyses 17 Report other analyses done—eg analyses of subgroups and interactions, and sensitivity analyses 14
Discussion
Key results 18 Summarise key results with reference to study objectives 17-18
Limitations 19 Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and
magnitude of any potential bias
18-19
Interpretation 20 Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from
similar studies, and other relevant evidence
17-18
Generalisability 21 Discuss the generalisability (external validity) of the study results 17-18
Other information
Funding 22 Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on
which the present article is based
19
*Give information separately for cases and controls in case-control studies and, if applicable, for exposed and unexposed groups in cohort and cross-sectional studies.
Page 31 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-008523 on 24 November 2015. Downloaded from

For peer review only
Note: An Explanation and Elaboration article discusses each checklist item and gives methodological background and published examples of transparent reporting. The STROBE
checklist is best used in conjunction with this article (freely available on the Web sites of PLoS Medicine at http://www.plosmedicine.org/, Annals of Internal Medicine at
http://www.annals.org/, and Epidemiology at http://www.epidem.com/). Information on the STROBE Initiative is available at www.strobe-statement.org.
Page 32 of 32
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-008523 on 24 November 2015. Downloaded from

For peer review only
A cross-sectional multicenter study of cardiac risk score use in the management of unstable angina and non-ST-
elevation myocardial infarction
Journal: BMJ Open
Manuscript ID: bmjopen-2015-008523.R1
Article Type: Research
Date Submitted by the Author: 07-Jul-2015
Complete List of Authors: Engel, Josien; EMGO Institute for Health and Care Research / VU University Medical Center, Public and Occupational Health Van der Wulp, Ineke; EMGO Institute for Health and Care Research / Vu
University Medical Center, Public and Occupational Health de Bruijne, Martine; EMGO Institute, VU University Medical Center, Amsterdam, the Netherlands, Dept. of Public and Occupational Health Wagner, Cordula; NIVEL, Netherlands Institute for Health Services Research, ; EMGO Institute, VU University Medical Center, Amsterdam, the Netherlands, Dept. of Public and Occupational Health
<b>Primary Subject Heading</b>:
Health services research
Secondary Subject Heading: Cardiovascular medicine, Evidence based practice, Health services research
Keywords: acute coronary syndromes, risk assessment, guideline adherence, predictors, chart review
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on July 10, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-008523 on 24 N
ovember 2015. D
ownloaded from

For peer review only
1
A cross-sectional multicenter study of cardiac risk score use in the management 1
of unstable angina and non-ST-elevation myocardial infarction 2
3
Josien Engel, MSc*1
, Ineke van der Wulp, PhD1
, Martine de Bruijne, PhD1
, Cordula Wagner, 4
PhD 1,2
5
6
1
EMGO Institute for Health and Care Research, Department of Public and Occupational 7
Health, VU University Medical Center, Amsterdam, the Netherlands 8
2
NIVEL, Netherlands Institute for Health Services Research, Utrecht, the Netherlands 9
10
* Corresponding Author: 11
Josien Engel; EMGO Institute for Health and Care Research, Department of Public and 12
Occupational Health, VU University Medical Center; Van der Boechorststraat 7, 1081 BT 13
Amsterdam, The Netherlands; Tel: +31 20 4445452; E-Mail: [email protected] 14
15
Key words: acute coronary syndromes, risk assessment, guideline adherence, predictors, 16
chart review 17
18
Word count: main text: 2822 words, abstract: 285 words 19
Number of figures/tables: 6 20
21
Page 1 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
2
STRENGTHS AND LIMITATIONS 22
• This multicenter study is the first to provide thorough insight in the extent of cardiac 23
risk score use in clinical practice by reviewing patient charts in thirteen hospitals 24
throughout the Netherlands; 25
• Generalized Linear Mixed Models were used to study hospital- and patient-related 26
factors associated with lower or higher cardiac risk score use; 27
• The results can serve as a basis for future improvement initiatives aimed to enhance 28
cardiac risk score use in practice, by tailoring strategies to patient groups in which risk 29
scores are less often documented; 30
• It was not possible to study associations between the extent of cardiac risk score use 31
and the occurrence of adverse patient outcomes (e.g. death) due to practical 32
constraints; 33
• Using retrospective review of medical charts as the underlying method of data 34
collection made it impossible to determine the actual influence of cardiac risk score 35
use on clinical decision making of health care providers involved in the management 36
of patients with unstable angina or non-ST-elevation Myocardial Infarction. 37
38
Page 2 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
3
ABSTRACT 39
40
Objectives: Quantitative risk assessment in unstable angina (UA) and non-ST-elevation 41
myocardial infarction (NSTEMI), by using cardiac risk scores, is recommended in 42
international guidelines. However, a gap between recommended care and actual practice 43
exists, as these instruments seem underused in practice. The present study aimed to determine 44
the extent of cardiac risk score use and to study factors associated with lower or higher 45
cardiac risk score use. 46
Setting: Thirteen hospitals throughout the Netherlands 47
Participants: A retrospective chart review of 1788 charts of UA and NSTEMI patients, 48
discharged in 2012 49
Primary and secondary outcomes: The extent of cardiac risk score use reflected in a 50
documented risk score outcome in the patient’s chart. And factors associated with cardiac 51
risk score use determined by generalized linear mixed models. 52
Results: In 57% (n=1019) of the charts, physicians documented the use of a cardiac risk 53
score. Substantial variation between hospitals was observed (16.7% to 87%), although this 54
variation could not be explained by the presence of on-site revascularization facilities or a 55
hospitals’ teaching status. Obese patients (OR=1.49; CI 95%= 1.03–2.15) and former smokers 56
(OR=1.56; CI 95%= 1.15–2.11) were more likely to have a cardiac risk score documented. 57
Risk scores were less likely being used among patients diagnosed with unstable angina 58
(OR=0.60; CI 95%= 0.46–0.77), in-hospital resuscitation (OR=0.23; CI 95%= 0.09–0.64), in-59
hospital heart failure (OR=0.46; CI 95%= 0.27–0.76) or tachycardia (OR=0.45; CI 95%= 60
0.26–0.75). 61
Conclusions: Despite recommendations in cardiac guidelines, the use of cardiac risk scores 62
has not been fully implemented in Dutch practice. A substantial number of patients did not 63
Page 3 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
4
have a cardiac risk score documented in their chart. Strategies to improve cardiac risk score 64
use should pay special attention to patient groups in which risk scores were less often 65
documented, as these patients may currently be undertreated. 66
Page 4 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
5
BACKGROUND 67
68
In the past decade mortality rates in acute coronary syndromes, including unstable angina 69
(UA) and non-ST-elevation myocardial infarction (NSTEMI), decreased significantly due to 70
substantial improvements in treatment possibilities.[1, 2] Despite these advancements, these 71
conditions still account for a large part of the annual deaths worldwide and are expected to be 72
the leading cause of death and to account for the largest disease burden worldwide by 2020-73
2030.[3-5] Part of these deaths may be prevented, as it has previously been reported that a 74
substantial number of patients were not treated according to the current standards of care.[6-8] 75
Patients with diabetes mellitus, renal insufficiency, signs of heart failure and patients aged 75 76
years or older, were often neglected guideline recommended care.[6] On the other hand, 77
patients presenting to academic hospitals and to hospitals with revascularisation facilities on-78
site (e.g. percutaneous coronary intervention (PCI) or coronary artery bypass grafting 79
(CABG)), were more often treated in accordance to the guidelines.[7,9] Patients diagnosed 80
with UA or NSTEMI can be treated with medication or invasive procedures such as PCI or 81
CABG. According to international cardiac guidelines the decision to treat such patients with 82
one or the other may be made on the basis of a quantitative assessment of the patient’s risk of 83
re-infarction or death.[10-12] To assist clinicians in identifying patients at high risk of adverse 84
cardiac events that would benefit most from invasive therapies, several instruments have been 85
developed.[10-12] The GRACE (Global registry of Acute Coronary Events),[13, 14] TIMI 86
(Thrombolysis in Myocardial Infarction),[15] FRISC (fast revascularization in instability in 87
coronary disease),[16] PURSUIT (Platelet glycoprotein IIb/IIIa in Unstable angina: Receptor 88
Suppression Using Integrilin),[17] and HEART risk scores [18] are examples of validated 89
cardiac risk scoring instruments. In estimating risk, these instruments incorporate and 90
combine several diagnostic elements including a patients’ history, biomarkers and 91
Page 5 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
6
electrocardiogram findings, and can be used in the emergency department or coronary care 92
unit. The predictive validity of these instruments was reported to be good.[16, 19, 20] 93
Previous research found that cardiac risk scores were effective in identifying patients at high 94
risk for cardiac events.[21, 22] However, a gap between recommended care in the guidelines 95
and actual practice seems to exist, as it has been suggested before that cardiac risk scores are 96
not routinely used in clinical practice. [21, 23, 24] This possibly contributed to the 97
perpetuating “treatment risk paradox”, in which patients with low risk of adverse cardiac 98
events, opposite to cardiac guideline recommendations, were more likely to receive invasive 99
cardiac treatment compared to high risk patients.[6, 25-30] Prior to creating future 100
improvement initiatives to increase cardiac risk score use, knowledge about the extent of this 101
gap and associated factors is necessary. The present study, therefore, aimed to determine the 102
extent of cardiac risk score use in Dutch clinical practice and to study factors associated with 103
lower or higher cardiac risk score use. 104
105
METHODS 106
107
This study concerns a cross-sectional multicenter study. A detailed description of the study 108
protocol has been published previously.[31] The study protocol was reviewed and approved 109
by the medical ethical committee of the VU University Medical Center Amsterdam. Where 110
required, approval from hospitals’ local ethics board were obtained. 111
112
Setting 113
In 2008 all hospitals in the Netherlands committed themselves to the implementation of a 114
quality improvement program aimed to enhance patient safety in Dutch hospitals. The 115
program comprised several themes, including the theme ‘Optimal care for Acute Coronary 116
Page 6 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
7
Syndromes’ which, among other things, aimed to increase the application of cardiac risk 117
scores in clinical practice.[32] A random selection of 40 hospitals participated voluntarily in 118
the evaluation of the nationwide quality improvement program. By a multistage random 119
sampling procedure, initially 12 hospitals were selected from the pool of 40 hospitals to 120
participate in the current study (i.e. evaluation of cardiac risk score use). Three PCI-capable 121
hospitals declined participation, for which three additional PCI-capable hospitals were 122
selected. Additionally, one hospital was selected to obtain optimal diversity in on-site 123
revascularization facilities and teaching status. The final sample consisted of thirteen 124
hospitals, of which two university hospitals, seven tertiary teaching hospitals, and four 125
general hospitals. Bed capacity in the hospitals varied between 200 and 1200 beds. 126
127
Data collection 128
The primary study outcome was the extent to which cardiac risk scores were used in the 129
management of UA and NSTEMI patients, reflected in a documented risk score outcome in 130
the patient’s chart. Data were collected monthly by means of retrospective chart review. 131
Potentially eligible charts were selected from the hospitals’ billing system based on 132
diagnostic-related group codes for UA and NSTEMI. All patients discharged in 2012, 18 133
years or older, with a diagnosis of UA or NSTEMI (as confirmed in the discharge letter) were 134
considered for inclusion. Charts of patients who were transferred in from another hospital 135
were excluded, as these patients were initially treated elsewhere and therefore the necessary 136
data could not be obtained. In addition, charts of patients who provided insufficient 137
information regarding the discharge diagnosis, who were hospitalized for an elective 138
procedure, or who had an underlying illness or condition, other than a coronary stenosis, 139
causing UA or NSTEMI (e.g. anemia) were excluded. 140
Page 7 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
8
Charts of patients were selected per month in chronological order of discharge until the 141
screening capacity of the chart abstractors was reached. Charts of potentially eligible patients 142
were manually reviewed to confirm a discharge diagnosis of UA or NSTEMI. In case a 143
patient’s final discharge diagnosis was unclear, a physician of the cardiology department was 144
consulted. The following patient-related and hospital-related information was registered on 145
standardized data extraction forms, including the following: demographic characteristics, 146
cardiac history, presence of cardiac risk factors, presenting symptoms, biochemical and 147
electrocardiographic findings and treatment practices. In addition, information regarding 148
cardiac risk score use was registered, including the use of a validated risk score (yes/no), date 149
of application, type of risk score used and risk score outcome and classification. Besides 150
patient related information, the following hospital factors were registered: teaching status 151
(yes/no) and the presence of on-site revascularization facilities. 152
The data were entered into a database using fixed entry fields (BLAISE version 4.7, Statistics 153
Netherlands) and data reliability checks were conducted. To ensure reliable data extraction, 154
more than 5% (103/1933) of the charts were screened by two chart abstractors independently. 155
The total percentage of agreement between these abstractors was 95.1%, and ranged for the 156
variables of interest (Box 1) between 80.6% (electrocardiographic findings) and 100% 157
(gender), indicating good to excellent data reliability. 158
Box 1 Independent variables in Generalized Linear Mixed Model
Patient characteristics Patient characteristics Patient characteristics
Demographics
• Age
• Gender
Presenting factors
• Heart rate
• Systolic blood pressure
• Resuscitation at admission
• Cardiogenic shock
• In-hospital heart failure
Cardiac history
• Coronary artery disease
• Peripheral vascular disease
• (Unstable) angina pectoris
• Acute myocardial infarction
• Previous CABG
• Previous PCI
• Revascularization/AMI < 6
months
Risk factors
• Diabetes mellitus
• Hypertension
• Renal failure
• Chronic heart failure
• Positive family history
• Smoking
• Former smoker
Page 8 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
9
• ST deviations on ECG
Discharge diagnosis
• UA
• NSTEMI
Hospital characteristics
• Presence of revascularisation
options
• Teaching status
• Hypercholesterolemia*
• Obesity (BMI > 30)
• Coronary stenosis ≥50%
(in history)
Abbreviations: ECG, electrocardiogram; UA, unstable angina; NSTEMI, non-ST-elevation myocardial
infarction; CABG, Coronary artery bypass graft surgery; PCI, Percutaneous coronary intervention; AMI, acute
myocardial infarction; BMI, body mass index. *Defined as statin use prior to admission, or described in
patients history (elevated cholesterol levels, hyperlipidaemia or hypercholesterolemia).
159
Missing data 160
In total 1.5% of the values in the dataset were missing, ranging from 0.1% to 22% per 161
variable. Eleven variables had no missing values, including cardiac risk score use. Despite the 162
small amount of missing data and the spread of missing data in the dataset, a complete case 163
analysis would have led to a large loss of information and power. Therefore, missing values 164
were imputed using a multiple imputation procedure following the approach of van Buuren, 165
[33] resulting in five imputed datasets. In imputing missing values it was assumed that the 166
data were missing at random. The estimated values were corrected for the variables ‘hospital’ 167
and ‘cardiac risk score use’ as these variables were of primary interest in the analyses. By 168
means of the Kolmogorov-Smirnov test, and density and residual plots, it was determined, 169
whether the missing at random assumption was sustainable and the imputed values were 170
plausible. In addition, a sensitivity analysis was conducted by comparing the results from the 171
analyses of the imputed data with the results of a complete case analysis. Between these 172
models, only small differences were found. The missing value analyses and their imputations 173
were conducted in R (version 3.0.2 for Microsoft Windows) using the MICE package.[33, 34] 174
175
Data analysis 176
Sample characteristics were calculated using descriptive statistics, and included frequencies 177
and percentages for categorical variables, and means and standard deviations for continuous 178
Page 9 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
10
variables. Associations of independent variables (box 1) with the use of cardiac risk scores 179
(yes/no) were studied with a generalized linear mixed model (GLMM), taking into account 180
the clustering of data within hospitals.[35] Odds ratios, that are based on median probabilities 181
over hospitals for cardiac risk score use, are presented. To facilitate interpretation, relevant 182
explanatory variables were transformed into categorical variables (i.e. age, heart rate and 183
systolic blood pressure). Furthermore, month of discharge was represented by a categorical 184
variable with 12 levels in every model, to account for the fact that chart abstractors were 185
present to abstract data. In univariate analyses, associations between cardiac risk score use 186
and the independent variables were tested. All variables with a significance level of p≤0.15 187
were entered in a multivariable model. Variables significantly associated (p≤0.05) with 188
cardiac risk score use in the multivariable model were considered important in predicting risk 189
score adherence. In addition, based on previous literature two factor interactions with on-site 190
revascularization options, teaching status, age and gender were tested. All analyses were 191
conducted in R for windows (version 3.0.2) using the package lme4 on pooled data of five 192
imputed data sets.[34] The script of the pool function in MICE was rewritten for pooling 193
GLMM models. 194
195
RESULTS 196
197
Study population 198
A total of 1933 charts of patients with a confirmed diagnoses of UA or NSTEMI were 199
screened. Of these, 145 (7.5%) were excluded from the study as these concerned patients 200
transferred from one hospital to another, leaving 1788 patients for further analysis (Figure 1). 201
The majority (62.6%) of these patients had a discharge diagnosis of NSTEMI (Table 1). 202
Males accounted for 66.9% of the patients, and more than a third (35.9%) of the patients were 203
Page 10 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
11
aged 75 years or older. Three quarters (75.3%) of the total population underwent coronary 204
catheterization. The average length of hospital stay was five days (SD 4.97). 205
206
Table 1. Baseline characteristics (pooled data) (n= 1788) n (%)†
Age (<75 years) 1146 (64.1)
Gender (male) 1196 (66.9)
Discharge diagnoses (NSTEMI) 1119 (62.6)
Length of hospital stay (days) (mean ± SD) 5 ± 4.97
Systolic blood pressure (mmHg)
High (≥ 160) 552 (30.9)
Normal to slightly elevated (81-159) 1236 (69.1)
Low (≤ 80) 0 (0)
Heart rate (bpm)
Tachycardia (≥ 110) 103 (5.8)
Normal (51-109) 1634 (91.4)
Bradycardia (≤ 50) 51 (2.8)
Resuscitation at admission 33 (1.9)
Cardiogenic shock 7 (0.4)
In-hospital heart failure 103 (5.8)
ST deviations on electrocardiogram 810 (45.3)
History of coronary artery disease 252 (14.1)
History of peripheral vascular disease 131 (7.3)
Previous (U)A 432 (24.1)
Previous MI 499 (27.9)
Previous PCI 523 (29.3)
Previous CABG 289 (16.2)
MI or PCI/CABG 6 months prior to admission 125 (7)
Diabetes mellitus 451 (25.2)
Hypertension 936 (52.4)
Renal failure 88 (4.9)
Chronic heart failure 101 (5.7)
Hypercholesterolemia‡ 986 (55.1)
Obesity (BMI>30) 203 (11.3)
Smoking 427 (23.9)
Former smoker 350 (19.6)
Coronary stenosis (≥50%) 192 (10.8)
Positive family history 618 (34.6)
Page 11 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
12
Coronary catheterization 1346 (75.3)
Management strategy
Pharmacological therapy 754 (42.2)
(scheduled) PCI 846 (47.3)
(scheduled) CABG 188 (10.5)
†Data are presented in n(%), unless stated otherwise. ‡ Defined as statin use prior to
admission, or described in patients history (elevated cholesterol levels, hyperlipidaemia or
hypercholesterolemia).Abbreviations: n.a., not applicable; (U)A, (Unstable)Angina; MI,
myocardial infarction; PCI, percutaneous coronary intervention; CABG, coronary artery
bypass grafting; BMI, body mass index.
207
Cardiac risk score use 208
In 57% of the patient charts, a cardiac risk score was documented, though, substantial 209
variation between hospitals was observed i.e. 16.7% to 87% (Table 2). Six out of the thirteen 210
hospitals used more than one risk scoring instrument to calculate a risk score, being the 211
following: GRACE (12/13 hospitals), TIMI (3/13 hospitals), FRISC (1/13 hospitals) and the 212
HEART risk score (6/13 hospitals) (Table 2). The variance component for the random 213
hospital effect in the GLMM ranged between 1.29 and 1.31 in the five imputed datasets, 214
confirming the great variety between hospitals in the use of cardiac risk scores. When, for 215
instance, the effects for two hospitals are equal to the 5 and 95 percentiles of the normal 216
distribution with variance 1.3 for hospital effects, the odds ratio of one hospital relative to the 217
other for cardiac risk score use is 42.6. 218
In univariate analyses, 15 patient related factors were significantly (p≤0.15) associated with 219
cardiac risk score use (Table 3). No significant associations with hospital related factors were 220
found (teaching status p=0.25, on-site revascularisation facilities p=0.67). In multivariable 221
analyses, patients with obesity (OR=1.49; 95%CI= 1.03-2.15; p=0.04) and former smokers 222
(OR=1.56; 95% CI=1.15-2.11; p≤0.01) were more likely to have a cardiac risk score 223
documented. Conversely patients with UA (OR=0.60; 95% CI=0.46-0.77; p≤0.01), in-hospital 224
heart failure (OR=0.46; 95% CI=0.27-0.76; p≤0.01), tachycardia (OR=0.45; 95% CI=0.26-225
Page 12 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
13
0.75; p≤0.01) or who had been resuscitated at admission (OR=0.23; 95% CI=0.09-0.64; 226
p≤0.01) were less likely to have a cardiac risk score documented (Table 3). 227
228
Table 2. Adherence to cardiac risk score use per hospital (pooled data)
Hospital
ID†
Teaching
status
PCI/
CABG
options
Screened
charts n‡
Risk score
use n (%)˥
Type of risk score used∞
GRACE TIMI FRISC HEART
1 No No 84 14 (16.7) X - - -
2 Yes Yes 109 22 (20.2) X X - -
3 No No 110 26 (23.6) X - - -
4 No No 171 57 (33.3) - - - X
5 Yes Yes 132 46 (34.8) X - - X
6 Yes No 53 19 (35.8) X - - -
7 Yes Yes 145 79 (54.5) X - X X
8 Yes Yes 182 108 (59.3) X - - X
9 Yes Yes 96 68 (70.8) X - - -
10 Yes Yes 140 107 (76.4) X - - X
11 Yes Yes 108 87 (80.6) X X - X
12 No No 205 166 (81.0) X X - -
13 Yes No 253 220 (87.0) X - - -
Total -- -- 1788 1019 (57%) -- -- -- --
† ranging from lowest to highest scoring hospital. ‡ Large variation in screened patient charts per hospital is explained
by differences in the amount of monthly admission for UA/NSTEMI. ˥ Risk score use is represented by (one or more)
documented risk score outcome(s) in the patient’s chart. ∞Several hospitals calculated more than one risk score per
patient, using different risk scoring instruments. Abbreviations: CABG, coronary artery bypass grafting; FRISC, fast
revascularization in instability in coronary disease; GRACE, global registry of acute coronary events; PCI,
percutaneous coronary intervention; TIMI, Thrombolysis in Myocardial Infarction
Page 13 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
14
Table 3. Univariate and multivariable associations between risk score documentation in patient charts and
hospital- and patient related factors (pooled data) (n=1788) †
Univariate associations Multivariable associations
OR (95% CI) P OR (95% CI) P
Hospital factors
Teaching status 2.15 (0.59 – 7.85) 0.25 n.a. n.a.
On-site revascularisation facilities 1.32 (0.38 – 4.60) 0.67 n.a. n.a.
Patient factors‡
Discharge diagnosis (reference NSTEMI) 0.65 (0.52 – 0.83) ≤0.01** 0.60 (0.46 – 0.77) ≤0.01**
Age (reference <75 years) 0.76 (0.61 – 0.96) 0.02* 0.86 (0.67 – 1.11) 0.24
Resuscitation at admission 0.25 (0.10 – 0.67) ≤0.01** 0.23 (0.09 – 0.64) ≤0.01**
In-hospital heart failure 0.38 (0.24 -0.62) ≤0.01** 0.46 (0.27 – 0.76) ≤0.01**
History of coronary artery disease 0.65 (0.47 – 0.89) ≤0.01** 0.87 (0.59 – 1.27) 0.46
History of peripheral artery disease 0.72 (0.47 – 1.09) 0.12 0.81 (0.53 – 1.26) 0.35
Previous (U)A 0.83 (0.64 – 1.07) 0.15 1.00 (0.75 – 1.34) 0.98
Previous MI 0.77 (0.61 – 0.98) 0.03* 0.89 (0.68 – 1.18) 0.43
Previous PCI 0.83 (0.65 – 1.05) 0.13 1.07 (0.80 – 1.43) 0.66
Renal failure 0.54 (0.33 – 0.90) 0.02* 0.72 (0.42 – 1.23) 0.23
Obesity (BMI>30) 1.49 (1.05 – 2.13) 0.03* 1.49 (1.03 – 2.15) 0.04*
Smoking 1.23 (0.95 – 1.60) 0.11 1.16 (0.86 – 1.55) 0.33
Former smoker 1.48 (1.12 – 1.97) ≤0.01** 1.56 (1.15 – 2.11) ≤0.01**
Coronary stenosis (≥50%) 0.65 (0.46 – 0.93) 0.02* 0.81 (0.54 – 1.22) 0.31
Heart rate (bpm) (reference Normal)
Tachycardia 0.46 (0.28 – 0.76) ≤0.01** 0.45 (0.26 – 0.75) ≤0.01**
Bradycardia 0.85 (0.44 – 1.63) 0.62 0.92 (0.46 – 1.86) 0.82
† pooled p-value based on normal approximation. ‡Only variables (patient characteristics) with p ≤ 0.15 in the
univariate analyses are presented in this table. Reference category is ‘no’, unless stated otherwise. *p-value ≤
0.05; **p-value ≤0.01. Abbreviations: OR, odds ratio; CI, 95% confidence interval; n.a., not applicable; PCI,
percutaneous coronary intervention; CABG: coronary artery bypass grafting; (U)A, (Unstable)Angina; MI,
myocardial infarction; BMI, body mass index.
229
Page 14 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
15
Interactions 230
Besides the interactions with on-site revascularization options, teaching status, age and 231
gender, it was decided to also test whether interactions with former smoker were present. This 232
was because an unexpected significant association between former smoker and risk score use 233
was found. Significant interactions were found between the variables former smoker and 234
discharge diagnosis (p=0.03), age and previous PCI (p=0.02), age and in-hospital heart failure 235
(p=0.04), age and history of peripheral artery disease (p=0.03), and age and heart rate 236
(p=0.04) (Table 4). 237
Looking at the interaction effects with age, it was found that patients aged 75 years or over 238
presenting with a previous PCI had a higher odds of cardiac risk score documentation 239
compared to patients without a previous PCI (OR=1.53; 95% CI=1.00 – 2.34; p=0.05). In 240
contrast, older patients were less likely to have a cardiac risk score documented in case they 241
presented with heart failure (OR=0.29; 95% CI=0.14 – 0.57; p<0.001), with a history of 242
peripheral artery disease (OR=0.47; 95% CI=0.24 – 0.91; p=0.02) or with tachycardia 243
(OR=0.20; 95% CI=0.08 – 0.52; p=<0.001). 244
245
246
Page 15 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
16
Table 4. Estimated odds ratio’s and 95% confidence intervals for significant (p≤0.05) interactions terms
added to multivariable model of GLMM (pooled data) †
OR CI 95% P-value‡
Former smoker*discharge diagnosis
Discharge diagnosis (UA vs. NSTEMI) within former smoker (no) 0.52 0.40 – 0.69 <0.001**
Discharge diagnosis (UA vs. NSTEMI) within former smoker (yes) 1.00 0.59 – 1.71 0.98
Former smoker (yes vs. no) within discharge diagnosis (UA) 2.28 1.43 – 3.61 <0.001**
Former smoker (yes vs. no) within discharge diagnosis (NSTEMI) 1.19 0.81 – 1.75 0.38
Age*previous PCI
Age (≥75 vs. <75 years) within previous PCI (no) 0.71 0.52 – 0.96 0.02*
Age (≥75 vs. <75 years) within previous PCI (yes) 1.30 0.84 – 1.99 0.23
Previous PCI (yes vs. no) within age (<75 years) 0.84 0.58 – 1.19 0.32
Previous PCI (yes vs. no) within age (≥75 years) 1.53 1.00 – 2.34 0.05*
Age*in-hospital heart failure
Age (≥75 vs. <75 years) within in-hospital heart failure (no) 0.92 0.71 – 1.20 0.54
Age (≥75 vs. <75 years) within in-hospital heart failure (yes) 0.32 0.12 – 0.85 0.02*
In-hospital heart failure (yes vs. no) within age (<75 years) 0.84 0.39 – 1.82 0.66
In-hospital heart failure (yes vs. no) within age (≥75 years) 0.29 0.14 – 0.57 <0.001**
Age*History of peripheral artery disease
Age (≥75 vs. <75 years) within history of peripheral artery disease (no) 0.93 0.72 – 1.21 0.60
Age (≥75 vs. <75 years) within history of peripheral artery disease (yes) 0.34 0.14 – 0.80 0.01**
History of peripheral artery disease (yes vs. no) within age (<75 years) 1.28 0.70 – 2.32 0.42
History of peripheral artery disease (yes vs. no) within age (≥75 years) 0.47 0.24 – 0.91 0.02*
Age*Heart rate
Age (≥75 vs. <75 years) within heart rate (normal) 0.91 0.70 – 1.18 0.47
Age (≥75 vs. <75 years) within heart rate (tachycardia) 0.28 0.09 – 0.85 0.03*
Age (≥75 vs. <75 years) within heart rate (bradycardia) 1.25 0.31 – 5.00 0.75
Heart rate (tachycardia vs. normal) within age (<75 years) 0.67 0.34 – 1.30 0.23
Heart rate (bradycardia vs. normal) within age (<75 years) 0.81 0.33 – 2.01 0.65
Heart rate (tachycardia vs. normal) within age (≥75 years) 0.20 0.08 – 0.52 <0.001**
Heart rate (bradycardia vs. normal) within age (≥75 years) 1.12 0.38 – 3.27 0.84
Page 16 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
17
†All four OR’s per interaction term are presented in the table to form an impression of the nature of the interaction.
For instance, two separate OR’s for former smoker no versus yes for UA and NSTEMI patients and two separate
OR’s for UA versus NSTEMI for former smoker no and yes. These four OR’s are all shown, because when
interaction between two factors is added to the model, the OR of one factor may depend upon the level of the other
factor. ‡P-value indicates if OR is significantly different from one. *p-value ≤ 0.05; **p-value ≤0.01.Abbreviations:
OR, odds ratio; CI 95%, 95% confidence interval; UA, unstable angina; NSTEMI, non-ST-elevation myocardial
infarction.
247
Page 17 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
18
DISCUSSION 248
249
This study aimed to provide insight in the extent of cardiac risk score use in Dutch hospitals 250
as recommended by international cardiac guidelines. In addition, associations with patient and 251
hospital related factors were studied. Substantial variation between hospitals’ cardiac risk 252
score use was observed, with in approximately 40% of patient charts a cardiac risk score was 253
not documented. Several patient related factors including a diagnosis of UA, the presence of 254
in-hospital heart failure, tachycardia, and resuscitation at admission were associated with a 255
lower likelihood of cardiac risk score use. Although evidence is not conclusive, the 256
probability of cardiac risk score use was often lower in older patients (≥ 75 years) with 257
additional conditions, such as in-hospital heart failure, a history of peripheral artery disease or 258
tachycardia. 259
Previous studies also reported advanced age, heart failure and tachycardia as important 260
predictors of lower guideline adherence in patients with acute coronary syndromes.[6, 36-41] 261
Moreover, several of these studies also reported a decreased likelihood of survival. [37,38, 262
40] Implying that patients at high risk for adverse cardiac outcomes are less likely to receive 263
guideline recommended care. However, according to the European guidelines these high risk 264
subgroups of patients benefit most from early invasive treatments[10]. It may, however, be 265
discussed to what degree an invasive treatment may be desired in these high risk subgroups of 266
patients. Also, it could be questionable to what degree risk stratification using a cardiac risk 267
score adds value in deciding on the treatment for these patients, e.g. in the case of 268
resuscitation the decision for a certain procedure may be evident. The European Society of 269
Cardiology guidelines however, do not take these circumstances into account and recommend 270
estimating risk levels with a cardiac risk scoring instrument for every patient suspected of 271
UA/NSTEMI.[10] 272
Page 18 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
19
Obese patients and former smokers were more likely to have a cardiac risk score documented. 273
The association of former smoking and the use of a cardiac risk score, however, was 274
unexpected and difficult to explain. There are no indications for partial confounding with 275
other factors in the model as odds ratio’s for former smoker in univariate and multivariable 276
models are sizeable and similar. Possibly, former smoking is an alias for some other 277
underlying and unknown variable. For instance, former smoking is seen as an indication of a 278
former more high-risk lifestyle and that way affects judgement. Further research may provide 279
more insight on this. 280
Another interesting finding, that contrasted the findings of previous studies, was that a 281
hospitals’ teaching status or the presence of on-site revascularisation facilities were not 282
significantly associated with cardiac risk score use.[7, 36] These differences may be explained 283
by the relatively small number of hospitals participating in the present study compared to 284
previous studies. A large variation between hospitals in adherence scores regarding cardiac 285
risk score use were found. The large component of variance, explained by the random hospital 286
effect, suggests that cardiac risk score use in patients presenting with the same characteristics 287
may heavily depend on which hospital the patient is presented in and that other factors, beside 288
a hospital’s teaching status or on-site revascularisation facilities, are of influence. 289
Common barriers in the implementation of cardiac risk scores, including the absence of 290
necessary resources for implementation and cultural differences, may explain this substantial 291
variation.[42] It has been suggested that physicians find the evidence underlying cardiac risk 292
scores unconvincing.[24] To increase the use of cardiac risk scores in clinical practice several 293
implementation strategies, which pay explicit attention to patients with suspected UA may be 294
employed. A recent improvement initiative in the USA for instance, in which continuous 295
education was the primary intervention, led to a significant increase in cardiac risk score 296
documentation in UA and NSTEMI patients.[43] The use of continuous education has proven 297
Page 19 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
20
to be effective in achieving change in practice, however it is recommended to also take into 298
account facilitating factors and barriers on a patient, provider and organizational level.[44] 299
Therefore, further research is needed to carefully understand factors that explain the variation 300
between hospitals’ cardiac risk score use. 301
302
Study limitations 303
Several limitations potentially affect the interpretation of the results of this study. 304
First, the use of cardiac risk scores was measured by screening charts on the documentation of 305
a cardiac risk score. As a result it is unknown to what degree a cardiac risk score influenced 306
physicians’ decision making regarding appropriate management strategies. However, it is 307
plausible that when a cardiac risk score was documented, it was also used in practice. 308
Second, four predictors reported in previous studies of risk score use i.e. aspirin use prior to 309
admission, creatinine level, troponin level and biomarkers, were not considered in the present 310
study. These data could not be abstracted reliably. As a result, the precision of the model 311
reported in this study might be smaller compared to other studies. In addition, it was not 312
possible to reliable extract at what time point a risk score was recorded. The time registered in 313
the patient’s file was often imprecise (i.e. time was entered retrospectively and did not 314
represent the actual time point at which the risk score was used) or lacking. Making it 315
impossible to provide any additional contextual information regarding the use of cardiac risk 316
scores in clinical practice. 317
Third, in two hospitals the method of selection of patient charts differed, as it was not possible 318
to select patients based on the hospital’s billing system. This could have influenced the 319
selection of patients. However, their effects may be limited as it appeared that the random 320
effects of these two hospitals were well in range with those of the other hospitals. 321
Page 20 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
21
Fourth, it was not possible to extract all data from the charts at one time point per hospital. 322
Therefore, monthly data collection visits were deemed necessary. For this reason, the reported 323
associations were corrected for month of discharge, though, the frequent presence of the 324
researchers on-site may have led to more awareness of the health care providers using cardiac 325
risk scores, and as a result higher adherence scores than in hospitals not participating in the 326
evaluation of the quality improvement program. This overestimation of adherence rates can 327
also be a result of the fact that the evaluation of the improvement program took place in a 328
cohort of highly motivated hospitals, as they all voluntarily agreed to participate. 329
Finally, three of the randomly selected hospitals declined participation in this study, which 330
may have introduced selection-bias. Hospitals that declined participation were possibly 331
lagging behind in implementation. The actual use of cardiac risk scores in practice might 332
therefore be even lower than estimated in this paper. 333
334
CONCLUSIONS 335
336
The results of the present study indicate that cardiac risk scores have not been fully 337
implemented in Dutch clinical practice, as a substantial number of patients had no risk score 338
documented in their chart. The large variation between hospitals could not be explained by 339
the presence of on-site revascularization facilities or a hospitals’ teaching status, as well as by 340
several patient related factors that were associated with higher or lower usage of cardiac risk 341
scores in clinical practice. It is recommended that further research should focus first on 342
explanatory factors for differences between hospitals, which could provide a basis for future 343
improvement initiatives in which strategies are targeted towards patient groups in which risk 344
scores were less often documented, as these patients may currently be undertreated. 345
346
Page 21 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
22
ACKNOWLEDGEMENTS 347
We would like to thank Marie-Julie Heeren, Felix van Urk, Suzanne Vonk and Rixt Zuidema 348
for their support in data collection. 349
350
COMPETING INTERESTS 351
The authors declare that they have no competing interests. 352
353
AUTHORS’ CONTRIBUTION 354
All authors made substantial contributions to conception and design of the study. JE carried 355
out data collection, performed statistical analysis, and drafted the manuscript, and prepared 356
the manuscript for publication. IvdW provided substantial support in imputation of data and 357
statistical analysis. IvdW, MdB and CW made substantial contributions to interpretation of 358
the data and revised the manuscript critically for important intellectual content. All authors 359
read and approved the final manuscript. 360
361
FUNDING 362
The study was funded by the Dutch Ministry of Public health, Welfare and Sports. The study 363
sponsor had no role in the study design, collection, analysis and interpretation of the data, or 364
in writing of the manuscript and decision to submit the manuscript for publication. 365
366
DATA SHARING STATEMENT 367
No additional data are available. 368
369
Page 22 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
23
REFERENCES 370
371
1. Fox KAA, Steg PG, Eagle KA, et al. Decline in rates of death and heart failure in acute 372
coronary syndromes, 1999-2006. JAMA 2007,297:1892-1900. 373
2. Yeh RW, Sidney S, Chandra M, et al. Population trends in the incidence and outcomes 374
of acute myocardial infarction. N Engl J Med 2010,362:2155-2165. 375
3. Lopez AD, Murray CJ. The global burden of disease. A comprehensive assessment of 376
mortality and disability from diseases, injuries and risk factors in 1990 and projected to 377
2020. Cambridge MA: Harvard University Press 1996. 378
4. Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 379
1990-2020: Global Burden of Disease Study. Lancet 1997,349:1498-1504. 380
5. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 381
to 2030. PLoS Med 2006,3:e442. 382
6. Roe MT, Peterson ED, Newby LK, et al. The influence of risk status on guideline 383
adherence for patients with non-ST-segment elevation acute coronary syndromes. Am 384
Heart J 2006,151:1205-1213. 385
7. Peterson ED, Roe MT, Mulgund J, et al. Association between hospital process 386
performance and outcomes among patients with acute coronary syndromes. JAMA 387
2006,295:1912-1920. 388
8. Gulati M, Patel S, Jaffe AS, et al. Impact of contemporary guideline compliance on risk 389
stratification models for acute coronary syndromes in The Registry of Acute Coronary 390
Syndromes. Am J Cardiol 2004,94:873-878. 391
Page 23 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
24
9. Patel MR, Chen AY, Roe MT, et al. A comparison of acute coronary syndrome care at 392
academic and nonacademic hospitals. Am J Med 2007,120:40-46. 393
10. Hamm CW, Bassand JP, Agewall S, et al. ESC Guidelines for the management of acute 394
coronary syndromes in patients presenting without persistent ST-segment elevation: The 395
Task Force for the management of acute coronary syndromes (ACS) in patients 396
presenting without persistent ST-segment elevation of the European Society of 397
Cardiology (ESC). Eur Heart J 2011,32:2999-3054. 398
11. Anderson JL, Adams CD, Antman EM, et al. ACC/AHA 2007 guidelines for the 399
management of patients with unstable angina/non ST-elevation myocardial infarction: a 400
report of the American College of Cardiology/American Heart Association Task Force 401
on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the 402
Management of Patients With Unstable Angina/Non ST-Elevation Myocardial 403
Infarction): developed in collaboration with the American College of Emergency 404
Physicians, the Society for Cardiovascular Angiography and Interventions, and the 405
Society of Thoracic Surgeons: endorsed by the American Association of Cardiovascular 406
and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. 407
Circulation 2007,116:e148-e304. 408
12. Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC Guideline for the 409
Management of Patients With Non-ST-Elevation Acute Coronary Syndromes: A Report 410
of the American College of Cardiology/American Heart Association Task Force on 411
Practice Guidelines. Circulation 2014,130:2354-2394. 412
13. Granger CB, Goldberg RJ, Dabbous O, et al. Predictors of hospital mortality in the 413
global registry of acute coronary events. Arch Intern Med 2003,163:2345-2353. 414
Page 24 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
25
14. Fox KA, Dabbous OH, Goldberg RJ, et al. Prediction of risk of death and myocardial 415
infarction in the six months after presentation with acute coronary syndrome: 416
prospective multinational observational study (GRACE). BMJ 2006,333:1091. 417
15. Antman EM, Cohen M, Bernink PJ, et al. The TIMI risk score for unstable angina/non-418
ST elevation MI: A method for prognostication and therapeutic decision making. JAMA 419
2000,284:835-842. 420
16. Lagerqvist B, Diderholm E, Lindahl B, et al. FRISC score for selection of patients for an 421
early invasive treatment strategy in unstable coronary artery disease. Heart 422
2005,91:1047-1052. 423
17. Boersma E, Pieper KS, Steyerberg EW, et al. Predictors of outcome in patients with 424
acute coronary syndromes without persistent ST-segment elevation. Results from an 425
international trial of 9461 patients. The PURSUIT Investigators. Circulation 426
2000,101:2557-2567. 427
18. Six AJ, Backus BE, Kelder JC. Chest pain in the emergency room: value of the HEART 428
score. Neth Heart J 2008,16:191-196. 429
19. de Araujo GP, Ferreira J, Aguiar C, et al. TIMI, PURSUIT, and GRACE risk scores: 430
sustained prognostic value and interaction with revascularization in NSTE-ACS. Eur 431
Heart J 2005,26:865-872. 432
20. Backus BE, Six AJ, Kelder JC, et al. Chest pain in the emergency room: a multicenter 433
validation of the HEART Score. Crit Pathw Cardiol 2010,9:164-169. 434
21. Yan AT, Yan RT, Tan M, et al. Risk scores for risk stratification in acute coronary 435
syndromes: useful but simpler is not necessarily better. Eur Heart J 2007,28:1072-1078. 436
Page 25 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
26
22. Chew DP, Juergens C, French J, et al. An examination of clinical intuition in risk 437
assessment among acute coronary syndromes patients: observations from a prospective 438
multi-center international observational registry. Int J Cardiol 2014,171:209-216. 439
23. Manfrini O, Bugiardini R. Barriers to clinical risk scores adoption. Eur Heart J 440
2007,28:1045-1046. 441
24. Van de Werf F, Ardissino D, Bueno H, et al. Acute coronary syndromes: considerations 442
for improved acceptance and implementation of management guidelines. Expert Rev 443
Cardiovasc Ther 2012,10:489-503. 444
25. Yan AT, Yan RT, Tan M, et al. In-hospital revascularization and one-year outcome of 445
acute coronary syndrome patients stratified by the GRACE risk score. Am J Cardiol 446
2005,96:913-916. 447
26. Yan AT, Yan RT, Tan M, et al. Management patterns in relation to risk stratification 448
among patients with non-ST elevation acute coronary syndromes. Arch Intern Med 449
2007,167:1009-1016. 450
27. Fox KA, Anderson FA, Jr., Dabbous OH et al. Intervention in acute coronary 451
syndromes: do patients undergo intervention on the basis of their risk characteristics? 452
The Global Registry of Acute Coronary Events (GRACE). DHeart 2007,93:177-182. 453
28. Heras M, Bueno H, Bardaji A et al. Magnitude and consequences of undertreatment of 454
high-risk patients with non-ST segment elevation acute coronary syndromes: insights 455
from the DESCARTES Registry. Heart 2006,92:1571-1576. 456
Page 26 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
27
29. Lee CH, Tan M, Yan AT, et al. Use of cardiac catheterization for non-ST-segment 457
elevation acute coronary syndromes according to initial risk: reasons why physicians 458
choose not to refer their patients. Arch Intern Med 2008,168: 291-296. 459
30. Motivala AA, Cannon CP, Srinivas VS, et al. Changes in myocardial infarction 460
guideline adherence as a function of patient risk: an end to paradoxical care? J Am Coll 461
Cardiol 2011,58: 1760-1765. 462
31. Tra J, Engel J, van der Wulp I et al. Monitoring guideline adherence in the management 463
of acute coronary syndrome in hospitals: design of a multicentre study. Neth Heart J 464
2014,22: 346-53. 465
32. VMSzorg. Optimal care in Acute Coronary Syndromes [Original title in Dutch: Optimale 466
zorg in Acute Coronaire Syndromen]. Dutch National Patient Safety Programme. 2010 467
Http://www.vmszorg.nl/Themas/ACS 468
33. van Buuren S, Groothuis-Oudshoorn K (Eds). mice: Multivariate Imputation by Chained 469
Equations in R. In Journal of Statistical Software 2011,45:1-67. 470
34. R Core Team. R: A language and environment for statistical computing. 2013. Vienna, 471
Austria, R Foundation for Statistical Computing. http://www.R-project.org. 472
35. McCulloch CE, Searle SR, Neuhaus JM: Generalized, Linear, and Mixed Models., 2 473
edn. New Jersey: John Wiley & Sons, 2008. 474
36. Kumbhani DJ, Fonarow GC, Cannon CP et al. Predictors of adherence to performance 475
measures in patients with acute myocardial infarction. Am J Med 2013,126:74-79. 476
37. Scott IA, Harper CM. Guideline-discordant care in acute myocardial infarction: 477
predictors and outcomes. Med J Aust 2002,177:26-31. 478
Page 27 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
28
38. Allen LA, O'Donnell CJ, Camargo CAJ et al. Comparison of long-term mortality across 479
the spectrum of acute coronary syndromes. Am Heart J 2006,151:1065-1071. 480
39. Tran CTT, Laupacis A, Mamdani MM, et al. Effect of age on the use of evidence-based 481
therapies for acute myocardial infarction. Am Heart J 2004,148:834-841. 482
40. Ohman EM, Roe MT, Smith SCJ et al. Care of non-ST-segment elevation patients: 483
insights from the CRUSADE national quality improvement initiative. Am Heart J 484
2004,148:S34-S39. 485
41. Haim M, Battler A, Behar S et al. Acute coronary syndromes complicated by 486
symptomatic and asymptomatic heart failure: does current treatment comply with 487
guidelines? Am Heart J 2004,147:859-864. 488
42. Glickman SW, Boulding W, Staelin R et al. A framework for quality improvement: an 489
analysis of factors responsible for improvement at hospitals participating in the Can 490
Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with 491
Early Implementation of the ACC/AHA Guidelines (CRUSADE) quality improvement 492
initiative. Am Heart J 2007,154:1206-1220. 493
43. Cannon CP, Hoekstra JW, Larson DM et al. A report of quality improvement in the care 494
of patients with acute coronary syndromes. Crit Pathw Cardiol 2011,10: 29-34. 495
44. Grol R, Grimshaw J. From best evidence to best practice: effective implementation of 496
change in patients' care. Lancet 2003,362: 1225-1230. 497
498
499
500
Page 28 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
29
Figure 1. Inclusion and exclusion procedure of chart selection and screening 501
Page 29 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
147x216mm (300 x 300 DPI)
Page 30 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
STROBE 2007 (v4) Statement—Checklist of items that should be included in reports of cross-sectional studies
Although we are aware of the SPIRIT checklist, the STROBE checklist seems most suited for this manuscript, as it describes the study design of a cross-sectional
study. The SPIRIT checklist is specifically developed for reporting randomized trials and therefore its applicability to the contents of the present manuscript is
limited. In addition, some parts of the STROBE checklist will not be applicable to our manuscript, these will be left empty.
Section/Topic Item
# Recommendation Reported on page #
Title and abstract 1 (a) Indicate the study’s design with a commonly used term in the title or the abstract 1
(b) Provide in the abstract an informative and balanced summary of what was done and what was found 3
Introduction
Background/rationale 2 Explain the scientific background and rationale for the investigation being reported 4-5
Objectives 3 State specific objectives, including any prespecified hypotheses 5
Methods
Study design 4 Present key elements of study design early in the paper 5
Setting 5 Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data
collection
5-7
Participants
6
(a) Give the eligibility criteria, and the sources and methods of selection of participants 6
Variables 7 Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic criteria, if
applicable
6
Data sources/
measurement
8* For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe
comparability of assessment methods if there is more than one group
6
Bias 9 Describe any efforts to address potential sources of bias 7
Study size 10 Explain how the study size was arrived at 6
Quantitative variables 11 Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and
why
8-9
Statistical methods 12 (a) Describe all statistical methods, including those used to control for confounding 8-9
(b) Describe any methods used to examine subgroups and interactions 8-9
(c) Explain how missing data were addressed 8
Page 31 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-008523 on 24 November 2015. Downloaded from

For peer review only
(d) If applicable, describe analytical methods taking account of sampling strategy n.a.
(e) Describe any sensitivity analyses 8
Results
Participants 13* (a) Report numbers of individuals at each stage of study—eg numbers potentially eligible, examined for eligibility,
confirmed eligible, included in the study, completing follow-up, and analysed
9
(b) Give reasons for non-participation at each stage n.a.
(c) Consider use of a flow diagram Figure 1
Descriptive data 14* (a) Give characteristics of study participants (eg demographic, clinical, social) and information on exposures and potential
confounders
9
(b) Indicate number of participants with missing data for each variable of interest 7-8
Outcome data 15* Report numbers of outcome events or summary measures 9
Main results 16 (a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (eg, 95% confidence
interval). Make clear which confounders were adjusted for and why they were included
9-11
(b) Report category boundaries when continuous variables were categorized
(c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period
Other analyses 17 Report other analyses done—eg analyses of subgroups and interactions, and sensitivity analyses 14
Discussion
Key results 18 Summarise key results with reference to study objectives 17-18
Limitations 19 Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and
magnitude of any potential bias
18-19
Interpretation 20 Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from
similar studies, and other relevant evidence
17-18
Generalisability 21 Discuss the generalisability (external validity) of the study results 17-18
Other information
Funding 22 Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on
which the present article is based
19
*Give information separately for cases and controls in case-control studies and, if applicable, for exposed and unexposed groups in cohort and cross-sectional studies.
Page 32 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-008523 on 24 November 2015. Downloaded from

For peer review only
Note: An Explanation and Elaboration article discusses each checklist item and gives methodological background and published examples of transparent reporting. The STROBE
checklist is best used in conjunction with this article (freely available on the Web sites of PLoS Medicine at http://www.plosmedicine.org/, Annals of Internal Medicine at
http://www.annals.org/, and Epidemiology at http://www.epidem.com/). Information on the STROBE Initiative is available at www.strobe-statement.org.
Page 33 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-008523 on 24 November 2015. Downloaded from

For peer review only
A cross-sectional multicenter study of cardiac risk score use in the management of unstable angina and non-ST-
elevation myocardial infarction
Journal: BMJ Open
Manuscript ID: bmjopen-2015-008523.R2
Article Type: Research
Date Submitted by the Author: 16-Jul-2015
Complete List of Authors: Engel, Josien; EMGO Institute for Health and Care Research / VU University Medical Center, Public and Occupational Health Van der Wulp, Ineke; EMGO Institute for Health and Care Research / Vu
University Medical Center, Public and Occupational Health de Bruijne, Martine; EMGO Institute, VU University Medical Center, Amsterdam, the Netherlands, Dept. of Public and Occupational Health Wagner, Cordula; NIVEL, Netherlands Institute for Health Services Research, ; EMGO Institute, VU University Medical Center, Amsterdam, the Netherlands, Dept. of Public and Occupational Health
<b>Primary Subject Heading</b>:
Health services research
Secondary Subject Heading: Cardiovascular medicine, Evidence based practice, Health services research
Keywords: acute coronary syndromes, risk assessment, guideline adherence, predictors, chart review
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open on July 10, 2020 by guest. P
rotected by copyright.http://bm
jopen.bmj.com
/B
MJ O
pen: first published as 10.1136/bmjopen-2015-008523 on 24 N
ovember 2015. D
ownloaded from

For peer review only
1
A cross-sectional multicenter study of cardiac risk score use in the management 1
of unstable angina and non-ST-elevation myocardial infarction 2
3
Josien Engel, MSc*1
, Ineke van der Wulp, PhD1
, Martine de Bruijne, PhD1
, Cordula Wagner, 4
PhD 1,2
5
6
1
EMGO Institute for Health and Care Research, Department of Public and Occupational 7
Health, VU University Medical Center, Amsterdam, the Netherlands 8
2
NIVEL, Netherlands Institute for Health Services Research, Utrecht, the Netherlands 9
10
* Corresponding Author: 11
Josien Engel; EMGO Institute for Health and Care Research, Department of Public and 12
Occupational Health, VU University Medical Center; Van der Boechorststraat 7, 1081 BT 13
Amsterdam, The Netherlands; Tel: +31 20 4445452; E-Mail: [email protected] 14
15
Key words: acute coronary syndromes, risk assessment, guideline adherence, predictors, 16
chart review 17
18
Word count: main text: 2822 words, abstract: 285 words 19
Number of figures/tables: 6 20
21
Page 1 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
2
STRENGTHS AND LIMITATIONS 22
• This multicenter study is the first to provide thorough insight into the extent of cardiac 23
risk score use in clinical practice by reviewing patient charts in thirteen hospitals 24
throughout the Netherlands; 25
• Generalized Linear Mixed Models were used to study hospital- and patient-related 26
factors associated with lower or higher cardiac risk score use; 27
• The results can serve as a basis for future improvement initiatives aimed to enhance 28
cardiac risk score use in practice, by tailoring strategies to patient groups in which risk 29
scores are less often documented; 30
• It was not possible to study associations between the extent of cardiac risk score use 31
and the occurrence of adverse patient outcomes (e.g. death) due to practical 32
constraints; 33
• Using retrospective review of medical charts as the underlying method of data 34
collection, made it impossible to determine the actual influence of cardiac risk score 35
use on clinical decision making of health care providers involved in the management 36
of patients with unstable angina or non-ST-elevation Myocardial Infarction. 37
38
Page 2 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
3
ABSTRACT 39
40
Objectives: Quantitative risk assessment in unstable angina (UA) and non-ST-elevation 41
myocardial infarction (NSTEMI), by using cardiac risk scores, is recommended in 42
international guidelines. However, a gap between recommended care and actual practice 43
exists, as these instruments seem underused in practice. The present study aimed to determine 44
the extent of cardiac risk score use and to study factors associated with lower or higher 45
cardiac risk score use. 46
Setting: Thirteen hospitals throughout the Netherlands 47
Participants: A retrospective chart review of 1788 charts of UA and NSTEMI patients, 48
discharged in 2012 49
Primary and secondary outcomes: The extent of cardiac risk score use reflected in a 50
documented risk score outcome in the patient’s chart. Factors associated with cardiac risk 51
score use determined by generalized linear mixed models. 52
Results: In 57% (n=1019) of the charts, physicians documented the use of a cardiac risk 53
score. Substantial variation between hospitals was observed (16.7% to 87%), although this 54
variation could not be explained by the presence of on-site revascularization facilities or a 55
hospitals’ teaching status. Obese patients (OR=1.49; CI 95%= 1.03–2.15) and former smokers 56
(OR=1.56; CI 95%= 1.15–2.11) were more likely to have a cardiac risk score documented. 57
Risk scores were less likely to be used among patients diagnosed with unstable angina 58
(OR=0.60; CI 95%= 0.46–0.77), in-hospital resuscitation (OR=0.23; CI 95%= 0.09–0.64), in-59
hospital heart failure (OR=0.46; CI 95%= 0.27–0.76) or tachycardia (OR=0.45; CI 95%= 60
0.26–0.75). 61
Conclusions: Despite recommendations in cardiac guidelines, the use of cardiac risk scores 62
has not been fully implemented in Dutch practice. A substantial number of patients did not 63
Page 3 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
4
have a cardiac risk score documented in their chart. Strategies to improve cardiac risk score 64
use should pay special attention to patient groups in which risk scores were less often 65
documented, as these patients may currently be undertreated. 66
Page 4 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
5
BACKGROUND 67
68
In the past decade mortality rates in acute coronary syndromes, including unstable angina 69
(UA) and non-ST-elevation myocardial infarction (NSTEMI), decreased significantly due to 70
substantial improvements in treatment possibilities.[1, 2] Despite these advancements, these 71
conditions still account for a large part of the annual deaths worldwide and are expected to be 72
the leading cause of death and to account for the largest disease burden worldwide by 2020-73
2030.[3-5] Part of these deaths may be prevented, as it has previously been reported that a 74
substantial number of patients were not treated according to the current standards of care.[6-8] 75
Patients with diabetes mellitus, renal insufficiency, signs of heart failure and patients aged 75 76
years or older, were often neglected guideline recommended care.[6] On the other hand, 77
patients presenting to academic hospitals and to hospitals with revascularisation facilities on-78
site (e.g. percutaneous coronary intervention (PCI) or coronary artery bypass grafting 79
(CABG)), were more often treated in accordance to the guidelines.[7,9] Patients diagnosed 80
with UA or NSTEMI can be treated with medication or invasive procedures such as PCI or 81
CABG. According to international cardiac guidelines the decision to treat such patients with 82
one or the other may be made on the basis of a quantitative assessment of the patient’s risk of 83
re-infarction or death.[10-12] To assist clinicians in identifying patients at high risk of adverse 84
cardiac events that would benefit most from invasive therapies, several instruments have been 85
developed.[10-12] The GRACE (Global registry of Acute Coronary Events),[13, 14] TIMI 86
(Thrombolysis in Myocardial Infarction),[15] FRISC (fast revascularization in instability in 87
coronary disease),[16] PURSUIT (Platelet glycoprotein IIb/IIIa in Unstable angina: Receptor 88
Suppression Using Integrilin),[17] and HEART risk scores [18] are examples of validated 89
cardiac risk scoring instruments. In estimating risk, these instruments incorporate and 90
combine several diagnostic elements including a patients’ history, biomarkers and 91
Page 5 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
6
electrocardiogram findings, and can be used in the emergency department or coronary care 92
unit. The predictive validity of these instruments was reported to be good.[16, 19, 20] 93
Previous research found that cardiac risk scores were effective in identifying patients at high 94
risk for cardiac events.[21, 22] However, a gap between recommended care in the guidelines 95
and actual practice seems to exist, as it has been suggested before that cardiac risk scores are 96
not routinely used in clinical practice. [21, 23, 24] This possibly contributes to perpetuating 97
the “treatment risk paradox”, in which patients with low risk of adverse cardiac events, 98
opposite to cardiac guideline recommendations, were more likely to receive invasive cardiac 99
treatment compared to high risk patients.[6, 25-30] Prior to creating future improvement 100
initiatives aimed to increase cardiac risk score use, knowledge about the extent of this gap and 101
associated factors is necessary. The present study, therefore, aimed to determine the extent of 102
cardiac risk score use in Dutch clinical practice and to study factors associated with lower or 103
higher cardiac risk score use. 104
105
METHODS 106
107
This study concerns a cross-sectional multicenter study. A detailed description of the study 108
protocol has been published previously.[31] The study protocol was reviewed and approved 109
by the medical ethical committee of the VU University Medical Center Amsterdam. Where 110
required, approval from hospitals’ local ethics board were obtained. 111
112
Setting 113
In 2008 all hospitals in the Netherlands committed themselves to the implementation of a 114
quality improvement program aimed to enhance patient safety in Dutch hospitals. The 115
program comprised several themes, including the theme ‘Optimal care for Acute Coronary 116
Page 6 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
7
Syndromes’ which, among other things, aimed to increase the application of cardiac risk 117
scores in clinical practice.[32] A random selection of 40 hospitals participated voluntarily in 118
the evaluation of the nationwide quality improvement program. By a multistage random 119
sampling procedure, initially 12 hospitals were selected from the pool of 40 hospitals to 120
participate in the current study (i.e. evaluation of cardiac risk score use). Three PCI-capable 121
hospitals declined participation, for which three additional PCI-capable hospitals were 122
selected. Additionally, one hospital was selected to obtain optimal diversity in on-site 123
revascularization facilities and teaching status. The final sample consisted of thirteen 124
hospitals, of which two university hospitals, seven tertiary teaching hospitals, and four 125
general hospitals. Bed capacity in the hospitals varied between 200 and 1200 beds. 126
127
Data collection 128
The primary study outcome was the extent to which cardiac risk scores were used in the 129
management of UA and NSTEMI patients, reflected in a documented risk score outcome in 130
the patient’s chart. Data were collected monthly by means of retrospective chart review. 131
Potentially eligible charts were selected from the hospitals’ billing system based on 132
diagnostic-related group codes for UA and NSTEMI. All patients discharged in 2012, 18 133
years or older, with a diagnosis of UA or NSTEMI (as confirmed in the discharge letter) were 134
considered for inclusion. Charts of patients who were transferred in from another hospital 135
were excluded, as these patients were initially treated elsewhere and therefore the necessary 136
data could not be obtained. In addition, charts of patients who provided insufficient 137
information regarding the discharge diagnosis, who were hospitalized for an elective 138
procedure, or who had an underlying illness or condition, other than a coronary stenosis, 139
causing UA or NSTEMI (e.g. anemia) were excluded. 140
Page 7 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
8
Charts of patients were selected per month in chronological order of discharge, until the 141
screening capacity of the chart abstractors was reached. Charts of potentially eligible patients 142
were manually reviewed to confirm a discharge diagnosis of UA or NSTEMI. In case a 143
patient’s final discharge diagnosis was unclear, a physician of the cardiology department was 144
consulted. The following patient-related and hospital-related information was registered on 145
standardized data extraction forms: demographic characteristics, cardiac history, presence of 146
cardiac risk factors, presenting symptoms, biochemical and electrocardiographic findings and 147
treatment practices. In addition, information regarding cardiac risk score use was registered, 148
including the use of a validated risk score (yes/no), date of application, type of risk score used 149
and risk score outcome and classification. Besides patient related information, the following 150
hospital factors were registered: teaching status (yes/no) and the presence of on-site 151
revascularization facilities. 152
The data were entered into a database using fixed entry fields (BLAISE version 4.7, Statistics 153
Netherlands) and data reliability checks were conducted. To ensure reliable data extraction, 154
more than 5% (103/1933) of the charts were screened by two chart abstractors independently. 155
The total percentage of agreement between these abstractors was 95.1%, and ranged for the 156
variables of interest (Box 1) between 80.6% (electrocardiographic findings) and 100% 157
(gender), indicating good to excellent data reliability. 158
Box 1 Independent variables in Generalized Linear Mixed Model
Patient characteristics Patient characteristics Patient characteristics
Demographics
• Age
• Gender
Presenting factors
• Heart rate
• Systolic blood pressure
• Resuscitation at admission
• Cardiogenic shock
• In-hospital heart failure
Cardiac history
• Coronary artery disease
• Peripheral vascular disease
• (Unstable) angina pectoris
• Acute myocardial infarction
• Previous CABG
• Previous PCI
• Revascularization/AMI < 6
months
Risk factors
• Diabetes mellitus
• Hypertension
• Renal failure
• Chronic heart failure
• Positive family history
• Smoking
• Former smoker
Page 8 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
9
• ST deviations on ECG
Discharge diagnosis
• UA
• NSTEMI
Hospital characteristics
• Presence of revascularisation
options
• Teaching status
• Hypercholesterolemia*
• Obesity (BMI > 30)
• Coronary stenosis ≥50%
(in history)
Abbreviations: ECG, electrocardiogram; UA, unstable angina; NSTEMI, non-ST-elevation myocardial
infarction; CABG, Coronary artery bypass graft surgery; PCI, Percutaneous coronary intervention; AMI, acute
myocardial infarction; BMI, body mass index. *Defined as statin use prior to admission, or described in
patients history (elevated cholesterol levels, hyperlipidaemia or hypercholesterolemia).
159
Missing data 160
In total 1.5% of the values in the dataset were missing, ranging from 0.1% to 22% per 161
variable. Eleven variables had no missing values, including cardiac risk score use. Despite the 162
small amount of missing data and the spread of missing data in the dataset, a complete case 163
analysis would have led to a large loss of information and power. Therefore, missing values 164
were imputed using a multiple imputation procedure following the approach of van Buuren, 165
resulting in five imputed datasets. [33] In imputing missing values it was assumed that the 166
data were missing at random. The estimated values were corrected for the variables ‘hospital’ 167
and ‘cardiac risk score use’ as these variables were of primary interest in the analyses. By 168
means of the Kolmogorov-Smirnov test, and density and residual plots, it was determined, 169
whether the missing at random assumption was sustainable and the imputed values were 170
plausible. In addition, a sensitivity analysis was conducted by comparing the results from the 171
analyses of the imputed data with the results of a complete case analysis. Between these 172
models, only small differences were found. The missing value analyses and their imputations 173
were conducted in R (version 3.0.2 for Microsoft Windows) using the MICE package.[33, 34] 174
175
Data analysis 176
Sample characteristics were calculated using descriptive statistics, and included frequencies 177
and percentages for categorical variables, and means and standard deviations for continuous 178
Page 9 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
10
variables. Associations of independent variables (box 1) with the use of cardiac risk scores 179
(yes/no) were studied with a generalized linear mixed model (GLMM), taking into account 180
the clustering of data within hospitals.[35] Odds ratios, that are based on median probabilities 181
over hospitals for cardiac risk score use, are presented. To facilitate interpretation, relevant 182
explanatory variables were transformed into categorical variables (i.e. age, heart rate and 183
systolic blood pressure). Furthermore, month of discharge was represented by a categorical 184
variable with 12 levels in every model, to account for the fact that chart abstractors were 185
present on hospital departments to abstract data. In univariate analyses, associations between 186
cardiac risk score use and the independent variables were tested. All variables with a 187
significance level of p≤0.15 were entered in a multivariable model. Variables significantly 188
associated (p≤0.05) with cardiac risk score use in the multivariable model were considered 189
important in predicting risk score adherence. In addition, based on previous literature two 190
factor interactions with on-site revascularization options, teaching status, age and gender were 191
tested. All analyses were conducted in R for windows (version 3.0.2) using the package lme4 192
on pooled data of five imputed data sets.[34] The script of the pool function in MICE was 193
rewritten for pooling GLMM models. 194
195
RESULTS 196
197
Study population 198
A total of 1933 charts of patients with a confirmed diagnoses of UA or NSTEMI were 199
screened. Of these, 145 (7.5%) were excluded from the study as these concerned patients 200
transferred from one hospital to another, leaving 1788 patients for further analysis (Figure 1). 201
The majority (62.6%) of these patients had a discharge diagnosis of NSTEMI (Table 1). 202
Males accounted for 66.9% of the patients, and more than a third (35.9%) of the patients were 203
Page 10 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
11
aged 75 years or older. Three quarters (75.3%) of the total population underwent coronary 204
catheterization. The average length of hospital stay was five days (SD 4.97). 205
206
Table 1. Baseline characteristics (pooled data) (n= 1788) n (%)†
Age (<75 years) 1146 (64.1)
Gender (male) 1196 (66.9)
Discharge diagnoses (NSTEMI) 1119 (62.6)
Length of hospital stay (days) (mean ± SD) 5 ± 4.97
Systolic blood pressure (mmHg)
High (≥ 160) 552 (30.9)
Normal to slightly elevated (81-159) 1236 (69.1)
Low (≤ 80) 0 (0)
Heart rate (bpm)
Tachycardia (≥ 110) 103 (5.8)
Normal (51-109) 1634 (91.4)
Bradycardia (≤ 50) 51 (2.8)
Resuscitation at admission 33 (1.9)
Cardiogenic shock 7 (0.4)
In-hospital heart failure 103 (5.8)
ST deviations on electrocardiogram 810 (45.3)
History of coronary artery disease 252 (14.1)
History of peripheral vascular disease 131 (7.3)
Previous (U)A 432 (24.1)
Previous MI 499 (27.9)
Previous PCI 523 (29.3)
Previous CABG 289 (16.2)
MI or PCI/CABG 6 months prior to admission 125 (7)
Diabetes mellitus 451 (25.2)
Hypertension 936 (52.4)
Renal failure 88 (4.9)
Chronic heart failure 101 (5.7)
Hypercholesterolemia‡ 986 (55.1)
Obesity (BMI>30) 203 (11.3)
Smoking 427 (23.9)
Former smoker 350 (19.6)
Coronary stenosis (≥50%) 192 (10.8)
Positive family history 618 (34.6)
Page 11 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
12
Coronary catheterization 1346 (75.3)
Management strategy
Pharmacological therapy 754 (42.2)
(scheduled) PCI 846 (47.3)
(scheduled) CABG 188 (10.5)
†Data are presented in n(%), unless stated otherwise. ‡ Defined as statin use prior to
admission, or described in patients history (elevated cholesterol levels, hyperlipidaemia or
hypercholesterolemia).Abbreviations: n.a., not applicable; (U)A, (Unstable)Angina; MI,
myocardial infarction; PCI, percutaneous coronary intervention; CABG, coronary artery
bypass grafting; BMI, body mass index.
207
Cardiac risk score use 208
In 57% of the patient charts, a cardiac risk score was documented, though, substantial 209
variation between hospitals was observed i.e. 16.7% to 87% (Table 2). Six out of the thirteen 210
hospitals used more than one risk scoring instrument to calculate a risk score, being the 211
following: GRACE (12/13 hospitals), TIMI (3/13 hospitals), FRISC (1/13 hospitals) and the 212
HEART risk score (6/13 hospitals) (Table 2). The variance component for the random 213
hospital effect in the GLMM ranged between 1.29 and 1.31 in the five imputed datasets, 214
confirming the great variety between hospitals in the use of cardiac risk scores. When, for 215
instance, the effects for two hospitals are equal to the 5 and 95 percentiles of the normal 216
distribution with variance 1.3 for hospital effects, the odds ratio of one hospital relative to the 217
other for cardiac risk score use is 42.6. 218
In univariate analyses, 15 patient-related factors were significantly (p≤0.15) associated with 219
cardiac risk score use (Table 3). No significant associations with hospital-related factors were 220
found (teaching status p=0.25, on-site revascularisation facilities p=0.67). In multivariable 221
analyses, patients with obesity (OR=1.49; 95%CI= 1.03-2.15; p=0.04) and former smokers 222
(OR=1.56; 95% CI=1.15-2.11; p≤0.01) were more likely to have a cardiac risk score 223
documented. Conversely patients with UA (OR=0.60; 95% CI=0.46-0.77; p≤0.01), in-hospital 224
heart failure (OR=0.46; 95% CI=0.27-0.76; p≤0.01), tachycardia (OR=0.45; 95% CI=0.26-225
Page 12 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
13
0.75; p≤0.01) or who had been resuscitated at admission (OR=0.23; 95% CI=0.09-0.64; 226
p≤0.01) were less likely to have a cardiac risk score documented (Table 3). 227
228
229
230
231
232
233
234
235
236
237
238
239
240
241
242
243
244
245
246
247
248
Table 2. Adherence to cardiac risk score use per hospital (pooled data)
Hospital
ID†
Teaching
status
PCI/
CABG
options
Screened
charts n‡
Risk score
use n (%)˥
Type of risk score used∞
GRACE TIMI FRISC HEART
1 No No 84 14 (16.7) X - - -
2 Yes Yes 109 22 (20.2) X X - -
3 No No 110 26 (23.6) X - - -
4 No No 171 57 (33.3) - - - X
5 Yes Yes 132 46 (34.8) X - - X
6 Yes No 53 19 (35.8) X - - -
7 Yes Yes 145 79 (54.5) X - X X
8 Yes Yes 182 108 (59.3) X - - X
9 Yes Yes 96 68 (70.8) X - - -
10 Yes Yes 140 107 (76.4) X - - X
11 Yes Yes 108 87 (80.6) X X - X
12 No No 205 166 (81.0) X X - -
13 Yes No 253 220 (87.0) X - - -
Total -- -- 1788 1019 (57%) -- -- -- --
† ranging from lowest to highest scoring hospital. ‡ Large variation in screened patient charts per hospital is explained
by differences in the amount of monthly admission for UA/NSTEMI. ˥ Risk score use is represented by (one or more)
documented risk score outcome(s) in the patient’s chart. ∞Several hospitals calculated more than one risk score per
patient, using different risk scoring instruments. Abbreviations: CABG, coronary artery bypass grafting; FRISC, fast
revascularization in instability in coronary disease; GRACE, global registry of acute coronary events; PCI,
percutaneous coronary intervention; TIMI, Thrombolysis in Myocardial Infarction
Page 13 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
14
Table 3. Univariate and multivariable associations between risk score documentation in patient charts and
hospital- and patient related factors (pooled data) (n=1788) †
Univariate associations Multivariable associations
OR (95% CI) P OR (95% CI) P
Hospital factors
Teaching status 2.15 (0.59 – 7.85) 0.25 n.a. n.a.
On-site revascularisation facilities 1.32 (0.38 – 4.60) 0.67 n.a. n.a.
Patient factors‡
Discharge diagnosis (reference NSTEMI) 0.65 (0.52 – 0.83) ≤0.01** 0.60 (0.46 – 0.77) ≤0.01**
Age (reference <75 years) 0.76 (0.61 – 0.96) 0.02* 0.86 (0.67 – 1.11) 0.24
Resuscitation at admission 0.25 (0.10 – 0.67) ≤0.01** 0.23 (0.09 – 0.64) ≤0.01**
In-hospital heart failure 0.38 (0.24 -0.62) ≤0.01** 0.46 (0.27 – 0.76) ≤0.01**
History of coronary artery disease 0.65 (0.47 – 0.89) ≤0.01** 0.87 (0.59 – 1.27) 0.46
History of peripheral artery disease 0.72 (0.47 – 1.09) 0.12 0.81 (0.53 – 1.26) 0.35
Previous (U)A 0.83 (0.64 – 1.07) 0.15 1.00 (0.75 – 1.34) 0.98
Previous MI 0.77 (0.61 – 0.98) 0.03* 0.89 (0.68 – 1.18) 0.43
Previous PCI 0.83 (0.65 – 1.05) 0.13 1.07 (0.80 – 1.43) 0.66
Renal failure 0.54 (0.33 – 0.90) 0.02* 0.72 (0.42 – 1.23) 0.23
Obesity (BMI>30) 1.49 (1.05 – 2.13) 0.03* 1.49 (1.03 – 2.15) 0.04*
Smoking 1.23 (0.95 – 1.60) 0.11 1.16 (0.86 – 1.55) 0.33
Former smoker 1.48 (1.12 – 1.97) ≤0.01** 1.56 (1.15 – 2.11) ≤0.01**
Coronary stenosis (≥50%) 0.65 (0.46 – 0.93) 0.02* 0.81 (0.54 – 1.22) 0.31
Heart rate (bpm) (reference Normal)
Tachycardia 0.46 (0.28 – 0.76) ≤0.01** 0.45 (0.26 – 0.75) ≤0.01**
Bradycardia 0.85 (0.44 – 1.63) 0.62 0.92 (0.46 – 1.86) 0.82
† pooled p-value based on normal approximation. ‡Only variables (patient characteristics) with p ≤ 0.15 in the
univariate analyses are presented in this table. Reference category is ‘no’, unless stated otherwise. *p-value ≤
0.05; **p-value ≤0.01. Abbreviations: OR, odds ratio; CI, 95% confidence interval; n.a., not applicable; PCI,
percutaneous coronary intervention; CABG: coronary artery bypass grafting; (U)A, (Unstable)Angina; MI,
myocardial infarction; BMI, body mass index.
249
Page 14 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
15
Interactions 250
Besides the interactions with on-site revascularization options, teaching status, age and 251
gender, it was decided to also test whether interactions with former smoker were present. 252
This, because an unexpected significant association between former smoker and risk score use 253
was found. Significant interactions were found between the variables former smoker and 254
discharge diagnosis (p=0.03), age and previous PCI (p=0.02), age and in-hospital heart failure 255
(p=0.04), age and history of peripheral artery disease (p=0.03), and age and heart rate 256
(p=0.04) (Table 4). 257
Looking at the interaction effects with age, it was found that patients aged 75 years or over 258
presenting with a previous PCI had a higher odds of cardiac risk score documentation 259
compared to patients without a previous PCI (OR=1.53; 95% CI=1.00 – 2.34; p=0.05). In 260
contrast, older patients were less likely to have a cardiac risk score documented in case they 261
presented with heart failure (OR=0.29; 95% CI=0.14 – 0.57; p<0.001), with a history of 262
peripheral artery disease (OR=0.47; 95% CI=0.24 – 0.91; p=0.02) or with tachycardia 263
(OR=0.20; 95% CI=0.08 – 0.52; p=<0.001). 264
265
266
Page 15 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
16
Table 4. Estimated odds ratio’s and 95% confidence intervals for significant (p≤0.05) interactions terms
added to multivariable model of GLMM (pooled data) †
OR CI 95% P-value‡
Former smoker*discharge diagnosis
Discharge diagnosis (UA vs. NSTEMI) within former smoker (no) 0.52 0.40 – 0.69 <0.001**
Discharge diagnosis (UA vs. NSTEMI) within former smoker (yes) 1.00 0.59 – 1.71 0.98
Former smoker (yes vs. no) within discharge diagnosis (UA) 2.28 1.43 – 3.61 <0.001**
Former smoker (yes vs. no) within discharge diagnosis (NSTEMI) 1.19 0.81 – 1.75 0.38
Age*previous PCI
Age (≥75 vs. <75 years) within previous PCI (no) 0.71 0.52 – 0.96 0.02*
Age (≥75 vs. <75 years) within previous PCI (yes) 1.30 0.84 – 1.99 0.23
Previous PCI (yes vs. no) within age (<75 years) 0.84 0.58 – 1.19 0.32
Previous PCI (yes vs. no) within age (≥75 years) 1.53 1.00 – 2.34 0.05*
Age*in-hospital heart failure
Age (≥75 vs. <75 years) within in-hospital heart failure (no) 0.92 0.71 – 1.20 0.54
Age (≥75 vs. <75 years) within in-hospital heart failure (yes) 0.32 0.12 – 0.85 0.02*
In-hospital heart failure (yes vs. no) within age (<75 years) 0.84 0.39 – 1.82 0.66
In-hospital heart failure (yes vs. no) within age (≥75 years) 0.29 0.14 – 0.57 <0.001**
Age*History of peripheral artery disease
Age (≥75 vs. <75 years) within history of peripheral artery disease (no) 0.93 0.72 – 1.21 0.60
Age (≥75 vs. <75 years) within history of peripheral artery disease (yes) 0.34 0.14 – 0.80 0.01**
History of peripheral artery disease (yes vs. no) within age (<75 years) 1.28 0.70 – 2.32 0.42
History of peripheral artery disease (yes vs. no) within age (≥75 years) 0.47 0.24 – 0.91 0.02*
Age*Heart rate
Age (≥75 vs. <75 years) within heart rate (normal) 0.91 0.70 – 1.18 0.47
Age (≥75 vs. <75 years) within heart rate (tachycardia) 0.28 0.09 – 0.85 0.03*
Age (≥75 vs. <75 years) within heart rate (bradycardia) 1.25 0.31 – 5.00 0.75
Heart rate (tachycardia vs. normal) within age (<75 years) 0.67 0.34 – 1.30 0.23
Heart rate (bradycardia vs. normal) within age (<75 years) 0.81 0.33 – 2.01 0.65
Heart rate (tachycardia vs. normal) within age (≥75 years) 0.20 0.08 – 0.52 <0.001**
Heart rate (bradycardia vs. normal) within age (≥75 years) 1.12 0.38 – 3.27 0.84
Page 16 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
17
†All four OR’s per interaction term are presented in the table to form an impression of the nature of the interaction.
For instance, two separate OR’s for former smoker no versus yes for UA and NSTEMI patients and two separate
OR’s for UA versus NSTEMI for former smoker no and yes. These four OR’s are all shown, because when
interaction between two factors is added to the model, the OR of one factor may depend upon the level of the other
factor. ‡P-value indicates if OR is significantly different from one. *p-value ≤ 0.05; **p-value ≤0.01.Abbreviations:
OR, odds ratio; CI 95%, 95% confidence interval; UA, unstable angina; NSTEMI, non-ST-elevation myocardial
infarction.
267
Page 17 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
18
DISCUSSION 268
269
This study aimed to provide insight in the extent of cardiac risk score use in Dutch hospitals 270
as recommended by international cardiac guidelines. In addition, associations with patient- 271
and hospital-related factors were studied. Substantial variation between hospitals’ cardiac risk 272
score use was observed, with in approximately 40% of patient charts a cardiac risk score was 273
not documented. Several patient-related factors including a diagnosis of UA, the presence of 274
in-hospital heart failure, tachycardia, and resuscitation at admission were associated with a 275
lower likelihood of cardiac risk score use. Although evidence is not conclusive, the 276
probability of cardiac risk score use was often lower in older patients (≥ 75 years) with 277
additional conditions, such as in-hospital heart failure, a history of peripheral artery disease or 278
tachycardia. 279
Previous studies also reported advanced age, heart failure and tachycardia as important 280
predictors of lower guideline adherence in patients with acute coronary syndromes.[6, 36-41] 281
Moreover, several of these studies also reported a decreased likelihood of survival. [37,38, 282
40] Implying that patients at high risk for adverse cardiac outcomes are less likely to receive 283
guideline recommended care. However, according to the European guidelines these high risk 284
subgroups of patients benefit most from early invasive treatments[10]. It may, however, be 285
discussed to what degree an invasive treatment may be desired in these high risk subgroups of 286
patients. Also, it could be questionable to what degree risk stratification using a cardiac risk 287
score adds value in deciding on the treatment for these patients, e.g. in the case of 288
resuscitation the decision for a certain procedure may be evident. The European Society of 289
Cardiology guidelines however, do not take these circumstances into account and recommend 290
to estimate risk levels with a cardiac risk scoring instrument for every patient suspected of 291
UA/NSTEMI.[10] 292
Page 18 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
19
Obese patients and former smokers were more likely to have a cardiac risk score documented. 293
The association of former smoking and the use of a cardiac risk score, however, was 294
unexpected and difficult to explain. There are no indications for partial confounding with 295
other factors in the model as odds ratio’s for former smoker in univariate and multivariable 296
models are sizeable and similar. Possibly, former smoking is an alias for some other 297
underlying and unknown variable. For instance, former smoking is seen as an indication of a 298
former more high-risk lifestyle and that way affects judgement. Further research may provide 299
more insight on this. 300
Another interesting finding, that contrasted the findings of previous studies, was that a 301
hospitals’ teaching status or the presence of on-site revascularisation facilities were not 302
significantly associated with cardiac risk score use.[7, 36] These differences may be explained 303
by the relatively small number of hospitals participating in the present study compared to 304
previous studies. A large variation between hospitals in adherence scores regarding cardiac 305
risk score use was found. The large component of variance, explained by the random hospital 306
effect, suggests that cardiac risk score use in patients presenting with the same characteristics 307
may heavily depend on which hospital the patient is presented in, and that other factors, 308
beside a hospital’s teaching status or on-site revascularisation facilities, are of influence. 309
Common barriers in the implementation of cardiac risk scores, including the absence of 310
necessary resources for implementation and cultural differences, may explain this substantial 311
variation.[42] Also, it has been suggested that physicians find the evidence underlying cardiac 312
risk scores unconvincing.[24] To increase the use of cardiac risk scores in clinical practice 313
several implementation strategies, which pay explicit attention to patients with suspected UA, 314
may be employed. A recent improvement initiative in the USA for instance, in which 315
continuous education was the primary intervention, led to a significant increase in cardiac risk 316
score documentation in UA and NSTEMI patients.[43] The use of continuous education has 317
Page 19 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
20
proven to be effective in achieving change in practice, however it is recommended to also 318
take into account facilitating factors and barriers on a patient, provider and organizational 319
level.[44] Therefore, further research is needed to carefully understand factors that explain the 320
variation between hospitals’ cardiac risk score use. 321
322
Study limitations 323
Several limitations potentially affect the interpretation of the results of this study. 324
First, the use of cardiac risk scores was measured by screening charts on the documentation of 325
a cardiac risk score. As a result it is unknown to what degree a cardiac risk score influenced 326
physicians’ decision making regarding appropriate management strategies. However, it is 327
plausible that when a cardiac risk score was documented, it was also used in practice. 328
Second, four predictors reported in previous studies of risk score use i.e. aspirin use prior to 329
admission, creatinine level, troponin level and biomarkers, were not considered in the present 330
study. These data could not be abstracted reliably. As a result, the precision of the model 331
reported in this study might be smaller compared to other studies. In addition, it was not 332
possible to reliable extract at what time point a risk score was recorded. The time registered in 333
the patient’s file was often imprecise (i.e. time was entered retrospectively and did not 334
represent the actual time point at which the risk score was used) or lacking. Making it 335
impossible to provide any additional contextual information regarding the use of cardiac risk 336
scores in clinical practice. 337
Third, in two hospitals the method of selection of patient charts differed, as in these hospitals 338
it was not possible to select patients based on the hospital’s billing system. This could have 339
influenced the selection of patients. However, their effects may be limited as it appeared that 340
the random effects of these two hospitals were well in range with those of the other hospitals. 341
Page 20 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
21
Fourth, it was not possible to extract all data from the charts at one time point per hospital. 342
Therefore, monthly data collection visits were deemed necessary. For this reason, the reported 343
associations were corrected for month of discharge. However, the frequent presence of the 344
researchers on-site may have led to more awareness of the health care providers using cardiac 345
risk scores, and as a result have higher adherence scores than hospitals not participating in the 346
evaluation of the quality improvement program. This overestimation of adherence rates can 347
also be a result of the fact that the evaluation of the improvement program took place in a 348
cohort of highly motivated hospitals, as they all voluntarily agreed to participate. 349
Finally, three of the randomly selected hospitals declined participation in this study, which 350
may have introduced selection-bias. Hospitals that declined participation were possibly 351
lagging behind in implementation. The actual use of cardiac risk scores in practice might 352
therefore be even lower than estimated in this paper. 353
354
CONCLUSIONS 355
356
The results of the present study indicate that cardiac risk scores have not been fully 357
implemented in Dutch clinical practice, as a substantial number of patients had no risk score 358
documented in their chart. The large variation between hospitals could not be explained by 359
the presence of on-site revascularization facilities or a hospitals’ teaching status, as well as by 360
several patient related factors that were associated with higher or lower usage of cardiac risk 361
scores in clinical practice. It is recommended that further research should focus first on 362
explanatory factors for differences between hospitals, which could provide a basis for future 363
improvement initiatives in which strategies are targeted towards patient groups in which risk 364
scores were less often documented, as these patients may currently be undertreated. 365
366
Page 21 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
22
ACKNOWLEDGEMENTS 367
We would like to thank Marie-Julie Heeren, Felix van Urk, Suzanne Vonk and Rixt Zuidema 368
for their support in data collection. 369
370
COMPETING INTERESTS 371
The authors declare that they have no competing interests. 372
373
AUTHORS’ CONTRIBUTION 374
All authors made substantial contributions to conception and design of the study. JE carried 375
out data collection, performed statistical analysis, and drafted the manuscript, and prepared 376
the manuscript for publication. IvdW provided substantial support in imputation of data and 377
statistical analysis. IvdW, MdB and CW made substantial contributions to interpretation of 378
the data and revised the manuscript critically for important intellectual content. All authors 379
read and approved the final manuscript. 380
381
FUNDING 382
The study was funded by the Dutch Ministry of Public health, Welfare and Sports. The study 383
sponsor had no role in the study design, collection, analysis and interpretation of the data, or 384
in writing of the manuscript and decision to submit the manuscript for publication. 385
386
DATA SHARING STATEMENT 387
No additional data are available. 388
389
Page 22 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
23
REFERENCES 390
391
1. Fox KAA, Steg PG, Eagle KA, et al. Decline in rates of death and heart failure in acute 392
coronary syndromes, 1999-2006. JAMA 2007,297:1892-1900. 393
2. Yeh RW, Sidney S, Chandra M, et al. Population trends in the incidence and outcomes 394
of acute myocardial infarction. N Engl J Med 2010,362:2155-2165. 395
3. Lopez AD, Murray CJ. The global burden of disease. A comprehensive assessment of 396
mortality and disability from diseases, injuries and risk factors in 1990 and projected to 397
2020. Cambridge MA: Harvard University Press 1996. 398
4. Murray CJ, Lopez AD. Alternative projections of mortality and disability by cause 399
1990-2020: Global Burden of Disease Study. Lancet 1997,349:1498-1504. 400
5. Mathers CD, Loncar D. Projections of global mortality and burden of disease from 2002 401
to 2030. PLoS Med 2006,3:e442. 402
6. Roe MT, Peterson ED, Newby LK, et al. The influence of risk status on guideline 403
adherence for patients with non-ST-segment elevation acute coronary syndromes. Am 404
Heart J 2006,151:1205-1213. 405
7. Peterson ED, Roe MT, Mulgund J, et al. Association between hospital process 406
performance and outcomes among patients with acute coronary syndromes. JAMA 407
2006,295:1912-1920. 408
8. Gulati M, Patel S, Jaffe AS, et al. Impact of contemporary guideline compliance on risk 409
stratification models for acute coronary syndromes in The Registry of Acute Coronary 410
Syndromes. Am J Cardiol 2004,94:873-878. 411
Page 23 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
24
9. Patel MR, Chen AY, Roe MT, et al. A comparison of acute coronary syndrome care at 412
academic and nonacademic hospitals. Am J Med 2007,120:40-46. 413
10. Hamm CW, Bassand JP, Agewall S, et al. ESC Guidelines for the management of acute 414
coronary syndromes in patients presenting without persistent ST-segment elevation: The 415
Task Force for the management of acute coronary syndromes (ACS) in patients 416
presenting without persistent ST-segment elevation of the European Society of 417
Cardiology (ESC). Eur Heart J 2011,32:2999-3054. 418
11. Anderson JL, Adams CD, Antman EM, et al. ACC/AHA 2007 guidelines for the 419
management of patients with unstable angina/non ST-elevation myocardial infarction: a 420
report of the American College of Cardiology/American Heart Association Task Force 421
on Practice Guidelines (Writing Committee to Revise the 2002 Guidelines for the 422
Management of Patients With Unstable Angina/Non ST-Elevation Myocardial 423
Infarction): developed in collaboration with the American College of Emergency 424
Physicians, the Society for Cardiovascular Angiography and Interventions, and the 425
Society of Thoracic Surgeons: endorsed by the American Association of Cardiovascular 426
and Pulmonary Rehabilitation and the Society for Academic Emergency Medicine. 427
Circulation 2007,116:e148-e304. 428
12. Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC Guideline for the 429
Management of Patients With Non-ST-Elevation Acute Coronary Syndromes: A Report 430
of the American College of Cardiology/American Heart Association Task Force on 431
Practice Guidelines. Circulation 2014,130:2354-2394. 432
13. Granger CB, Goldberg RJ, Dabbous O, et al. Predictors of hospital mortality in the 433
global registry of acute coronary events. Arch Intern Med 2003,163:2345-2353. 434
Page 24 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
25
14. Fox KA, Dabbous OH, Goldberg RJ, et al. Prediction of risk of death and myocardial 435
infarction in the six months after presentation with acute coronary syndrome: 436
prospective multinational observational study (GRACE). BMJ 2006,333:1091. 437
15. Antman EM, Cohen M, Bernink PJ, et al. The TIMI risk score for unstable angina/non-438
ST elevation MI: A method for prognostication and therapeutic decision making. JAMA 439
2000,284:835-842. 440
16. Lagerqvist B, Diderholm E, Lindahl B, et al. FRISC score for selection of patients for an 441
early invasive treatment strategy in unstable coronary artery disease. Heart 442
2005,91:1047-1052. 443
17. Boersma E, Pieper KS, Steyerberg EW, et al. Predictors of outcome in patients with 444
acute coronary syndromes without persistent ST-segment elevation. Results from an 445
international trial of 9461 patients. The PURSUIT Investigators. Circulation 446
2000,101:2557-2567. 447
18. Six AJ, Backus BE, Kelder JC. Chest pain in the emergency room: value of the HEART 448
score. Neth Heart J 2008,16:191-196. 449
19. de Araujo GP, Ferreira J, Aguiar C, et al. TIMI, PURSUIT, and GRACE risk scores: 450
sustained prognostic value and interaction with revascularization in NSTE-ACS. Eur 451
Heart J 2005,26:865-872. 452
20. Backus BE, Six AJ, Kelder JC, et al. Chest pain in the emergency room: a multicenter 453
validation of the HEART Score. Crit Pathw Cardiol 2010,9:164-169. 454
21. Yan AT, Yan RT, Tan M, et al. Risk scores for risk stratification in acute coronary 455
syndromes: useful but simpler is not necessarily better. Eur Heart J 2007,28:1072-1078. 456
Page 25 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
26
22. Chew DP, Juergens C, French J, et al. An examination of clinical intuition in risk 457
assessment among acute coronary syndromes patients: observations from a prospective 458
multi-center international observational registry. Int J Cardiol 2014,171:209-216. 459
23. Manfrini O, Bugiardini R. Barriers to clinical risk scores adoption. Eur Heart J 460
2007,28:1045-1046. 461
24. Van de Werf F, Ardissino D, Bueno H, et al. Acute coronary syndromes: considerations 462
for improved acceptance and implementation of management guidelines. Expert Rev 463
Cardiovasc Ther 2012,10:489-503. 464
25. Yan AT, Yan RT, Tan M, et al. In-hospital revascularization and one-year outcome of 465
acute coronary syndrome patients stratified by the GRACE risk score. Am J Cardiol 466
2005,96:913-916. 467
26. Yan AT, Yan RT, Tan M, et al. Management patterns in relation to risk stratification 468
among patients with non-ST elevation acute coronary syndromes. Arch Intern Med 469
2007,167:1009-1016. 470
27. Fox KA, Anderson FA, Jr., Dabbous OH et al. Intervention in acute coronary 471
syndromes: do patients undergo intervention on the basis of their risk characteristics? 472
The Global Registry of Acute Coronary Events (GRACE). DHeart 2007,93:177-182. 473
28. Heras M, Bueno H, Bardaji A et al. Magnitude and consequences of undertreatment of 474
high-risk patients with non-ST segment elevation acute coronary syndromes: insights 475
from the DESCARTES Registry. Heart 2006,92:1571-1576. 476
Page 26 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
27
29. Lee CH, Tan M, Yan AT, et al. Use of cardiac catheterization for non-ST-segment 477
elevation acute coronary syndromes according to initial risk: reasons why physicians 478
choose not to refer their patients. Arch Intern Med 2008,168: 291-296. 479
30. Motivala AA, Cannon CP, Srinivas VS, et al. Changes in myocardial infarction 480
guideline adherence as a function of patient risk: an end to paradoxical care? J Am Coll 481
Cardiol 2011,58: 1760-1765. 482
31. Tra J, Engel J, van der Wulp I et al. Monitoring guideline adherence in the management 483
of acute coronary syndrome in hospitals: design of a multicentre study. Neth Heart J 484
2014,22: 346-53. 485
32. VMSzorg. Optimal care in Acute Coronary Syndromes [Original title in Dutch: Optimale 486
zorg in Acute Coronaire Syndromen]. Dutch National Patient Safety Programme. 2010 487
Http://www.vmszorg.nl/Themas/ACS 488
33. van Buuren S, Groothuis-Oudshoorn K (Eds). mice: Multivariate Imputation by Chained 489
Equations in R. In Journal of Statistical Software 2011,45:1-67. 490
34. R Core Team. R: A language and environment for statistical computing. 2013. Vienna, 491
Austria, R Foundation for Statistical Computing. http://www.R-project.org. 492
35. McCulloch CE, Searle SR, Neuhaus JM: Generalized, Linear, and Mixed Models., 2 493
edn. New Jersey: John Wiley & Sons, 2008. 494
36. Kumbhani DJ, Fonarow GC, Cannon CP et al. Predictors of adherence to performance 495
measures in patients with acute myocardial infarction. Am J Med 2013,126:74-79. 496
37. Scott IA, Harper CM. Guideline-discordant care in acute myocardial infarction: 497
predictors and outcomes. Med J Aust 2002,177:26-31. 498
Page 27 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
28
38. Allen LA, O'Donnell CJ, Camargo CAJ et al. Comparison of long-term mortality across 499
the spectrum of acute coronary syndromes. Am Heart J 2006,151:1065-1071. 500
39. Tran CTT, Laupacis A, Mamdani MM, et al. Effect of age on the use of evidence-based 501
therapies for acute myocardial infarction. Am Heart J 2004,148:834-841. 502
40. Ohman EM, Roe MT, Smith SCJ et al. Care of non-ST-segment elevation patients: 503
insights from the CRUSADE national quality improvement initiative. Am Heart J 504
2004,148:S34-S39. 505
41. Haim M, Battler A, Behar S et al. Acute coronary syndromes complicated by 506
symptomatic and asymptomatic heart failure: does current treatment comply with 507
guidelines? Am Heart J 2004,147:859-864. 508
42. Glickman SW, Boulding W, Staelin R et al. A framework for quality improvement: an 509
analysis of factors responsible for improvement at hospitals participating in the Can 510
Rapid Risk Stratification of Unstable Angina Patients Suppress Adverse Outcomes with 511
Early Implementation of the ACC/AHA Guidelines (CRUSADE) quality improvement 512
initiative. Am Heart J 2007,154:1206-1220. 513
43. Cannon CP, Hoekstra JW, Larson DM et al. A report of quality improvement in the care 514
of patients with acute coronary syndromes. Crit Pathw Cardiol 2011,10: 29-34. 515
44. Grol R, Grimshaw J. From best evidence to best practice: effective implementation of 516
change in patients' care. Lancet 2003,362: 1225-1230. 517
518
519
520
Page 28 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
29
Figure 1. Inclusion and exclusion procedure of chart selection and screening 521
Page 29 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
147x216mm (300 x 300 DPI)
Page 30 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright.
http://bmjopen.bm
j.com/
BM
J Open: first published as 10.1136/bm
jopen-2015-008523 on 24 Novem
ber 2015. Dow
nloaded from

For peer review only
STROBE 2007 (v4) Statement—Checklist of items that should be included in reports of cross-sectional studies
Although we are aware of the SPIRIT checklist, the STROBE checklist seems most suited for this manuscript, as it describes the study design of a cross-sectional
study. The SPIRIT checklist is specifically developed for reporting randomized trials and therefore its applicability to the contents of the present manuscript is
limited. In addition, some parts of the STROBE checklist will not be applicable to our manuscript, these will be left empty.
Section/Topic Item
# Recommendation Reported on page #
Title and abstract 1 (a) Indicate the study’s design with a commonly used term in the title or the abstract 1
(b) Provide in the abstract an informative and balanced summary of what was done and what was found 3
Introduction
Background/rationale 2 Explain the scientific background and rationale for the investigation being reported 4-5
Objectives 3 State specific objectives, including any prespecified hypotheses 5
Methods
Study design 4 Present key elements of study design early in the paper 5
Setting 5 Describe the setting, locations, and relevant dates, including periods of recruitment, exposure, follow-up, and data
collection
5-7
Participants
6
(a) Give the eligibility criteria, and the sources and methods of selection of participants 6
Variables 7 Clearly define all outcomes, exposures, predictors, potential confounders, and effect modifiers. Give diagnostic criteria, if
applicable
6
Data sources/
measurement
8* For each variable of interest, give sources of data and details of methods of assessment (measurement). Describe
comparability of assessment methods if there is more than one group
6
Bias 9 Describe any efforts to address potential sources of bias 7
Study size 10 Explain how the study size was arrived at 6
Quantitative variables 11 Explain how quantitative variables were handled in the analyses. If applicable, describe which groupings were chosen and
why
8-9
Statistical methods 12 (a) Describe all statistical methods, including those used to control for confounding 8-9
(b) Describe any methods used to examine subgroups and interactions 8-9
(c) Explain how missing data were addressed 8
Page 31 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-008523 on 24 November 2015. Downloaded from

For peer review only
(d) If applicable, describe analytical methods taking account of sampling strategy n.a.
(e) Describe any sensitivity analyses 8
Results
Participants 13* (a) Report numbers of individuals at each stage of study—eg numbers potentially eligible, examined for eligibility,
confirmed eligible, included in the study, completing follow-up, and analysed
9
(b) Give reasons for non-participation at each stage n.a.
(c) Consider use of a flow diagram Figure 1
Descriptive data 14* (a) Give characteristics of study participants (eg demographic, clinical, social) and information on exposures and potential
confounders
9
(b) Indicate number of participants with missing data for each variable of interest 7-8
Outcome data 15* Report numbers of outcome events or summary measures 9
Main results 16 (a) Give unadjusted estimates and, if applicable, confounder-adjusted estimates and their precision (eg, 95% confidence
interval). Make clear which confounders were adjusted for and why they were included
9-11
(b) Report category boundaries when continuous variables were categorized
(c) If relevant, consider translating estimates of relative risk into absolute risk for a meaningful time period
Other analyses 17 Report other analyses done—eg analyses of subgroups and interactions, and sensitivity analyses 14
Discussion
Key results 18 Summarise key results with reference to study objectives 17-18
Limitations 19 Discuss limitations of the study, taking into account sources of potential bias or imprecision. Discuss both direction and
magnitude of any potential bias
18-19
Interpretation 20 Give a cautious overall interpretation of results considering objectives, limitations, multiplicity of analyses, results from
similar studies, and other relevant evidence
17-18
Generalisability 21 Discuss the generalisability (external validity) of the study results 17-18
Other information
Funding 22 Give the source of funding and the role of the funders for the present study and, if applicable, for the original study on
which the present article is based
19
*Give information separately for cases and controls in case-control studies and, if applicable, for exposed and unexposed groups in cohort and cross-sectional studies.
Page 32 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-008523 on 24 November 2015. Downloaded from

For peer review only
Note: An Explanation and Elaboration article discusses each checklist item and gives methodological background and published examples of transparent reporting. The STROBE
checklist is best used in conjunction with this article (freely available on the Web sites of PLoS Medicine at http://www.plosmedicine.org/, Annals of Internal Medicine at
http://www.annals.org/, and Epidemiology at http://www.epidem.com/). Information on the STROBE Initiative is available at www.strobe-statement.org.
Page 33 of 33
For peer review only - http://bmjopen.bmj.com/site/about/guidelines.xhtml
BMJ Open
123456789101112131415161718192021222324252627282930313233343536373839404142434445464748495051525354555657585960
on July 10, 2020 by guest. Protected by copyright. http://bmjopen.bmj.com/ BMJ Open: first published as 10.1136/bmjopen-2015-008523 on 24 November 2015. Downloaded from




![arXiv:1804.06353v2 [cs.CV] 14 Sep 2018 · 2018. 9. 17. · Veronika Cheplyginab,, Marleen de Bruijnea,d, Josien P. W. Pluimb,c aBiomedical Imaging Group Rotterdam, Depts. Radiology](https://static.fdocuments.net/doc/165x107/603c8e01f08a63018a1def0e/arxiv180406353v2-cscv-14-sep-2018-2018-9-17-veronika-cheplyginab-marleen.jpg)