Blood supply of spinal cord
55
THE SPINAL CORD Dr. Serge Eddy Mba Surgical Block – Basic Sciences
-
Upload
serge-eddy-mba -
Category
Health & Medicine
-
view
1.032 -
download
0
Transcript of Blood supply of spinal cord
PowerPoint Presentation
THE SPINAL CORDDr. Serge Eddy MbaSurgical Block Basic Sciences
TOPICDESCRIBE THE ANATOMY OF THE SPINAL CORDDESCRIBE THE BLOOD SUPPLY OF THE SPINAL CORDWHAT ARE THE EFFECTS OF DISRUPTION OF EACH OF THE MAJOR BLOOD SUPPLYDESCRIBE THE PATHOPHYSIOLOGY OF HEMITRANSECTION OF THE SPINAL CORD
PRESENTATION OUTLINEHISTORIC BACKGROUNDEMBRYOLOGICAL DEVELOPMENT OF THE SPINAL CORDGROSS ANATOMY OF THE SPINAL CORDBLOOD SUPPLY OD THE SPINAL CORDRECAP OF MAJOR BLOOD SUPPLY OF THE SPINAL CORDEFFECT OF DISRUPTION OF EACH BLOOD SUPPLYHEMITRANSECTION OF THE CORDDEFINITIONEPIDEMIOLOGYPATHOPHYSIOLOGYMANAGEMENTCURRENT RESEARCH
HISTORICAL BACKGROUND3000-2500BCEEgyptEdwin Smith Papyrus460-370BCEGreeceHippocrates129-210 CERomeGalen, spinal cord research1881USAJames Garfield (US President)1895GermanyWilhelm Rontgen (X-Ray)1913USAHenry Ford (Automobile)1995USAChristopher Reeve2008AustraliaMackay-Sim et All phase I/IIa trials of autologous transplant olfactory ensheathing cellsToday: we need to invest more in spinal cord research as Africans
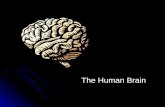
DEVELOPMENT OF THE SPINAL CORD start at 3rd weed of fetal developmentNeural Plate (ectoderm)Neural FoldsNeural TubeCranial and caudal NeuroporesCranial closes at Day 25 (20 somites stage), Caudal 2 days later
Embryology NEUROEPITHELIAL CELLSNEUROEPITHELIAL LAYERNEUROBLASTSMANTLE LAYERMARGINAL LAYERVENTRAL BASAL PLATEDORSALALAR PLATESULCUS LIMITANSROOF PLATE AND FLOOR PLATE
Molecular regulationSonic HedgeHog in Notochord represses expression of PAX3, PAX7, MSX1 and MSX2Bone Morphogenic Proteins expressed in non neuronal ectoderm upregulate PAX3 and PAX7
Types of spina bifida
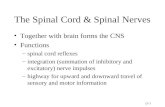
Gross anatomy. externalCylindrical structure located in spinal canal of vertebral columCovered by meninges, PIA, ARACHNOID and DURASuspended by denticulate ligaments (sheaths of dura)Ends as the conus medullaris (all the segmental nerve roots below L1)
Gross anatomy. External Filum terminal (streak of pia matter)/ Cauda equine (lumbosacral roots)31 pairs of spinal nerves which each divide into ventral and dorsal Primary rami surface is marked by furrowsDeep VENTRAL MEDIAN FISSUREDORSAL MEDIAN SULCUS
GROSS ANATOMY
GROSS ANATOMY INTERNALH shape in transverse sectionCentral canal lined by ependymal cells Gray matter consists ofDorsal hornVentral hornIntermadiate ZONELateral horn (preganglionic neurons, thoracic and upper lumbar)Gray matter has three main categories of neuronsMotor cells ( and motor neurons )Cell bodies of tract cells interneurons
15
White matter consists of three FUNICULIDorsal funiculus ( Gracile and cuneate Fasciculi)Lateral funicullusVentral funicullusDorsolateral tract of LISSAUER at apex of dorsal horn axons decussate in the ventral white commissureGROSS ANATOMY INTERNAL..
Neuronal architecture of spinal cord10 layers of neurons (I to X): LAMINAE of REXEDLamina II, the substantia gelatinosa (interneurons that can modify pain)Lamina VII (nucleus dorsalis ( gives rise to dorsal spinocerebellar tract)Intermediolateral cell colum(preganglionic sympathetic neurons)Lamina IX, motor neurone, supply skeletal musclesDictinctive colums of motor neuronsACCESSORY NUCLEUS (C1-C5)PHRENIC NUCLEUS (C3-C5)NUCLEUS OF ONUF (S2 and S3)
Dorsal root branches into two divisionsLateral: group C (unmyelinated) and group A (myelinated) axons enter the tract of Lissauer and divide into asc and desc branches synapse with tract cells of SPINOTHALAMIC FIBRES Medial: large caliber myelinated fibers, enter the spinal cord medial to dorsal horn and ascend in posterior funicullus concerned with other sensory modalities except pain and temperature
Neuronal architecture of spinal cordDORSAL HORN
Lamina IXTwo types of motor neuronsALPHA. Numerous, supply extrafusal fibers of striated muscles each alpha neuron receives at least 20.000 synaptic contactsGAMMA. Smaller, less numerous, supply intrafusal fibers of neuromuscular spindles interneurons: RENSHAW CELLS receives excitatory input but form inhibitory synaptic junctions on motor neurones Neuronal architecture of spinal cordventral horn
ascending descending tracts
DORSAL FUNICULUSIPSILATERALDiscriminative touch, vibration, joint position senseGracilis fasciculus medially (lower limb)Cuneatus fasciculus laterally(upper limb)Both end in medulla (gracilis and cuneatus nuclei)
LATERAL FUNICULUSlateral corticospinal tract
From cortex of frontal lobe, medullary pyramid, DECUSSATE and enter lateral funiculus From frontal cortex: terminate in intermediate gray matter and ventral hornFrom parietal cortex: terminate in dorsal horn
Lf- dorsal spinocerebellar tract
Present only above level L3Axons arise from Clarkes columTerminate ipsilaterally in the cerebellar cortex
Lf- spinothalamic tractCells of origins are in laminae IV and V-VIConsist of axons of neurons located in gray matter of opposite of cordTactile, thermal and painful stimuli
Lf- ventral spinocerebellar tractConsists largely of crossed fibersCrosses twiceThus ipsilateral proprioception
Ventral funiculusContains only descending tractsVentral corticospinal (decussate at segmental levels) skilled volitional movementsVestibulospinal tract: uncrossed arises from vestibular nucleus of Deiters in the medullaReticulospinal tracts: control ordinary activities that do not require conscious effortDescending bundle of the lateral horn are ipsilateral excitatory axons to the preganlionic sympathetic neurons
Blood supply of the spinal cordEXTRASPINALSEGMENTAL ARTERIESINTRASPINALANTERIOR SPINAL ARTERYPOSTERIOR SPINAL ARTERIESRADICULAR ARTEIESINTRAMEDULLARY ARTERIES
SEGMENTAL ARTERIESANT RADICULAR POST RADICULAR
12 ant radicularcontribute to pia plexus14 post radicular
join the join theANT SPINAL APOST SPINAL A
sulcal branchesLargest radicular aIn upper lumbar region(ADAMKIEWICZ)
Supply small plexuses present in piasupplyVentral gray horns VASORORONAremainder of dorsal gray hornsPart of dorsal gray horns supply white matter beneath pia dorsal funiculi of white matterVentral and lat white funiculi
Live operative picture of radicular arteryNote the small size in relation to the spinal nerve
Intraop photograph noting the artery of Adamkiewicz
SEGMENTAL SPINAL ARTERIES compromise
HypotensionAortic aneurysmAortic dissectionDevascularisation surgery (idiopathic)
COMPROMISE OF ANT AND POST SPINAL ARTERIES
ANTERIOR SPINAL ARTERY ANTERIOR CORD SYNDROMEBilateral disruption of the corticospinal tract, causing motor deficits, Bilateral disruption of the spinothalamic tract, causing sensory deficits in the form of pain/temperature sense loss.
POSTERIOR SPINAL ARTERYVERY RAREDISRUPTION OF POSTERIOR COLUM ONLY
OHER VASCULAR DISORDERSARTERIO VENOUS MALFORMATIONATHEROSCLEROSISVASCULAR TUMORS
HEMITRANSECTION OF THE SPINAL CORDBrown-Squard syndrome is an incomplete spinal cord lesion characterized by a clinical picture reflecting hemisection injury of the spinal cord, often in the cervical cord regionPatints suffer from ipsilateral upper motor neuron paralysis and loss of proprioception, as well as contralateral loss of pain and temperature sensation. A zone of partial preservation or segmental ipsilateral lower motor neuron weakness and analgesia may be noted. Loss of ipsilateral autonomic function can result in Horner syndrome
PATHOPHYSIOLOGYBrown-Squard syndrome results from damage to or loss of ascending and descending spinal cord tracts on 1 side of the spinal cord. Scattered petechial hemorrhages develop in the gray matter and enlarge and coalesce by 1 hour postinjury. Subsequent development of hemorrhagic necrosis occurs within 24-36 hours. White matter shows petechial hemorrhage at 3-4 hours. Myelinated fibers and long tracts show extensive structural damage
EPIDEMIOLOGYRare conditionTrue incidence is unknownMale > female16 30 years of age
PROGNOSISgood
presentationClinical history often reflects the etiology of Brown-Squard syndrome. Onset of symptoms may be acute or gradually progressive. Complaints are related to hemiparesis or hemiparalysis and sensory changes, paresthesias, or dysesthesias in the contralateral limb(s). Isolated weakness or sensory changes may be reported
Physical examinationPure Brown-Squard syndrome (rarely seen in clinical practice) is associated with the following: Interruption of the lateral corticospinal tracts - Ipsilateral spastic paralysis below the level of the lesion and Babinski sign ipsilateral to the lesion (abnormal reflexes and Babinski sign may not be present in acute injury) Interruption of posterior white column - Ipsilateral loss of tactile discrimination, as well as vibratory and position sensation, below the level of the lesion Interruption of lateral spinothalamic tracts - Contralateral loss of pain and temperature sensation; this usually occurs 2-3 segments below the level of the lesion Use ASIA impairment scale to assess degree of motor and sensory deficit
Differential diagnosisSpinal infectionVascular malformationSpinal cord tumor, primary or metastaticSpinal cord herniationPostradiation spinal cord dysfunctionEccentric disk herniation with cord compressionCervical disc diseaseDecompression sicknes
Work upThe diagnosis is made on the basis of history and physical examination. Laboratory work is not necessary to evaluate for the condition but may be helpful in following the patient's clinical course. Laboratory studies may also be useful in nontraumatic etiologies, such as infectious or neoplastic causes. Purified protein derivative and sputum for acid-fast bacilli should be ordered if tuberculosis is suggested as an etiology. If the cause of the SCI was traumatic, do a full traunma workup. Recognize that hypotension may be the result of something other than neurogenic shock. If, for example, the spinal injury was caused by trauma, hypotension may result from hemorrhagic causes.
WORKUPIMAGINGXraysCTMagnetic resonance imaging (MRI) is very useful in determining the exact structures that have been damaged in Brown-Squard syndrome, as well as in identifying nontraumatic etiologies of the disorder. No contrast is necessary for acute injury, but if an intradural etiology is suspected, a gadolinium or phase-contrast cine MRI scan may be helpfu
TREATMENTPhysical therapy intervention starts in the acute care phase of treatment. Therapy goals include the following: Maintaining strength in neurologically intact muscles Maintaining range of motion in joints Preventing skin breakdown by proper positioning and weight shifting Improving respiratory function by positioning and breathing exercises Achieving early mobilization to increase tolerance of the upright position Providing emotional and educational support for the patient and his/her family
Treatment Occupational therapySPINAL REDUCTION, STABILIZATION AND DECOMPRESSIONConsultation with MDT (multidisciplinary team)
Medical managementdependent on the etiology and acuity of onset. Acute treatment of traumatic SCI involves immediate dosing of methyl prednisolone. Acute immobility that is unrelated to a bleed requires anticoagulation therapy, if not contraindicated.Gastrointestinal protection is strongly recommended. Other medications are used to manage symptoms and complications as needed, including antibiotics, antispasmodics, pain medications, and laxatives.
Medical management CorticosteroidsMultiple studies have demonstrated improved outcomes for patients with traumatic SCIs who were given high-dose steroids early in the clinical course. (Although study by Pollard and Apple did not find these results in incomplete cervical SCIs. ) These drugs have anti-inflammatory properties and cause profound and varied metabolic effects. Corticosteroids modify the body's immune response to diverse stimuli
referencesCliinical anatomy (2014) venous drainage of the spina and spinal cordClinical anatomy (2015) blood supply of the human spinal corsBarrs , the human nervous system, 10th EdMcCarron MO, Flynn PA, Pang KA, et al. Traumatic Brown-Squard-plus syndrome. Arch Neurol. Sep 2001;58(9):1470-2Pollard ME, Apple DF. Factors associated with improved neurologic outcomes in patients with incomplete tetraplegia. Spine. Jan 1 2003;28(1):33-9Spinal Cord Injury Information Network. Facts and Figures at a Glance. 2013Parmar H, Park P, Brahma B, et al. Imaging of idiopathic spinal cord herniation. Radiographics. Mar-Apr 2008;28(2):511-8
THANK YOU MERCI BEAUCOUP