
Blood Component Therapy
82
Moderator Dr. T.Pensi (Professor) Dr Sunit Pathak(SR) Presented by .Dr Vivek Gupta
-
Upload
vivek-gupta -
Category
Documents
-
view
397 -
download
4
Transcript of Blood Component Therapy

Moderator
Dr. T.Pensi (Professor)
Dr Sunit Pathak(SR)
Presented by .Dr Vivek Gupta
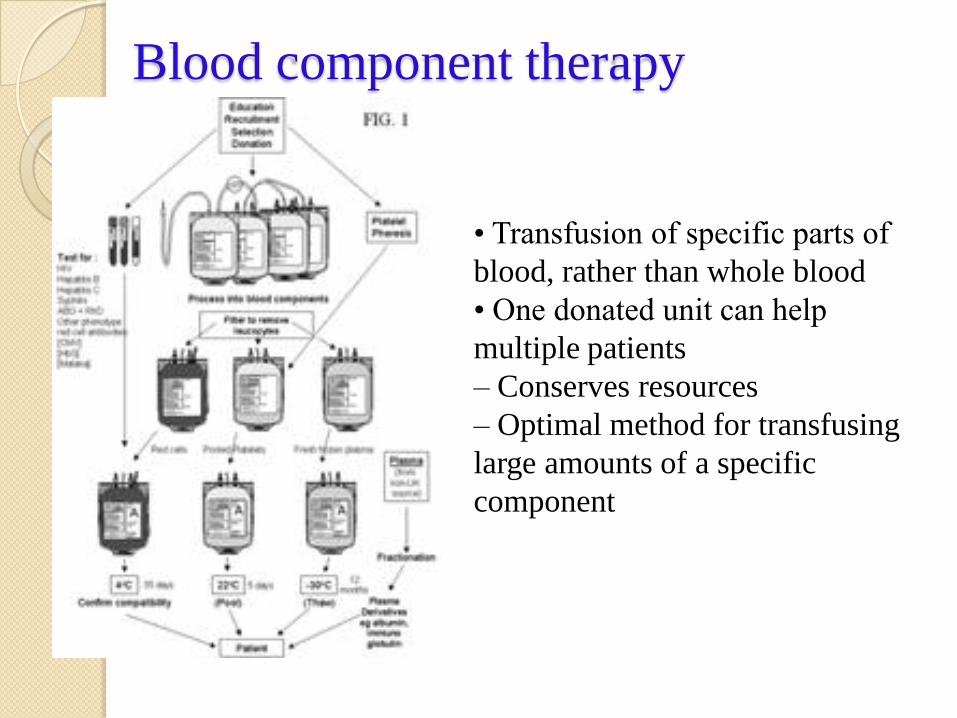
• Transfusion of specific parts of
blood, rather than whole blood
• One donated unit can help
multiple patients
– Conserves resources
– Optimal method for transfusing
large amounts of a specific
component
Blood component therapy

OVERVIEW
What are blood components?
What to transfuse?
General issue in transfusion.
Indication of transfusion ?
How to transfuse ?
What to expect after transfusion ?
What can go wrong with transfusion ?
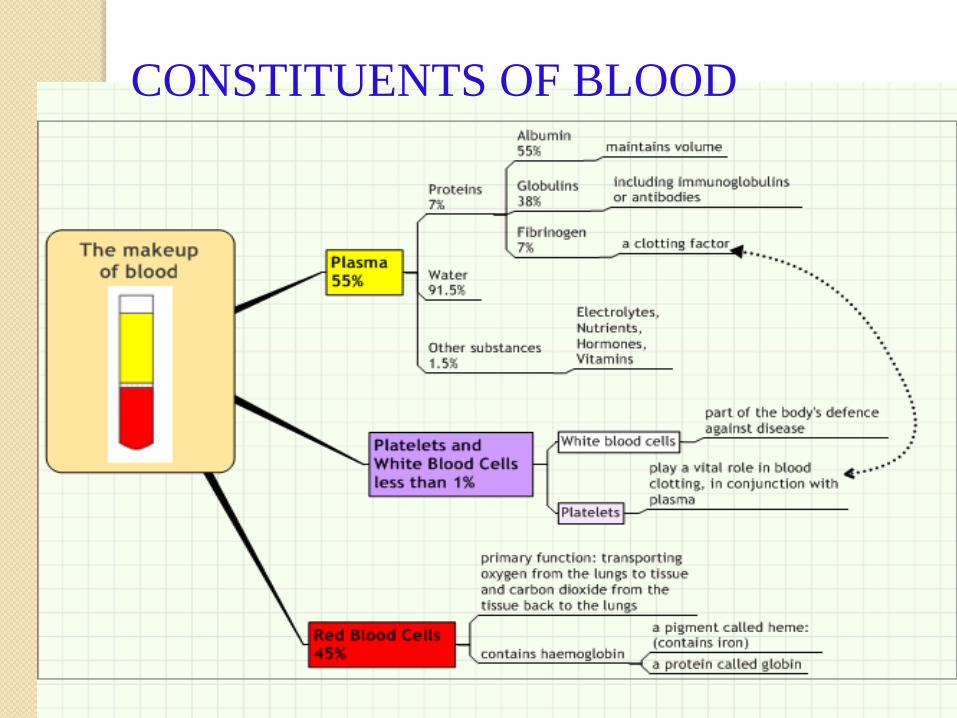
CONSTITUENTS OF BLOOD
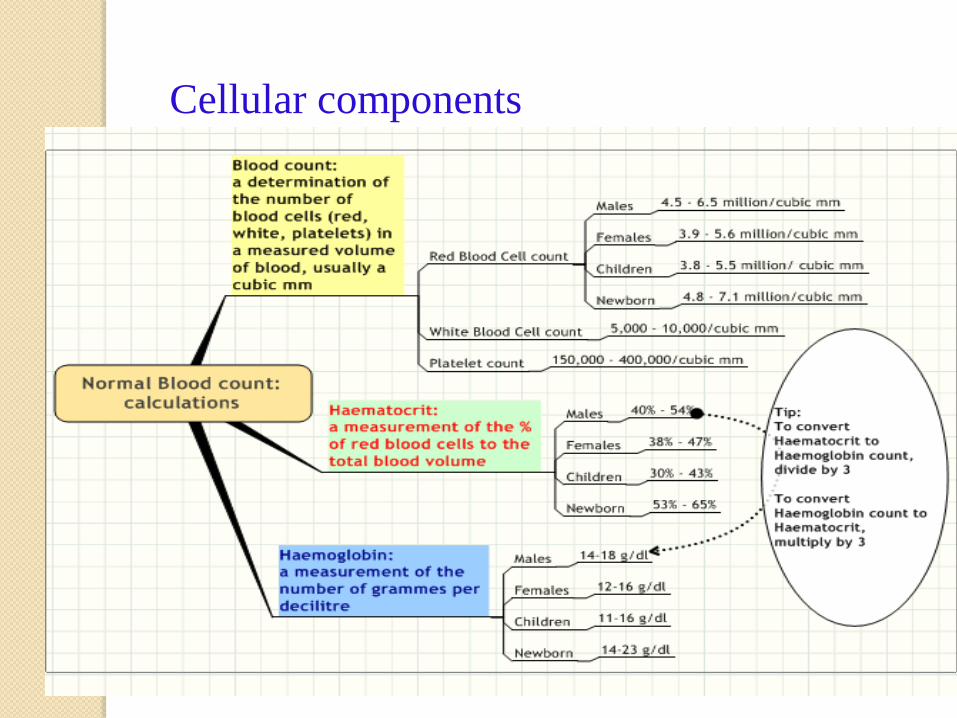
Cellular components

Plasma
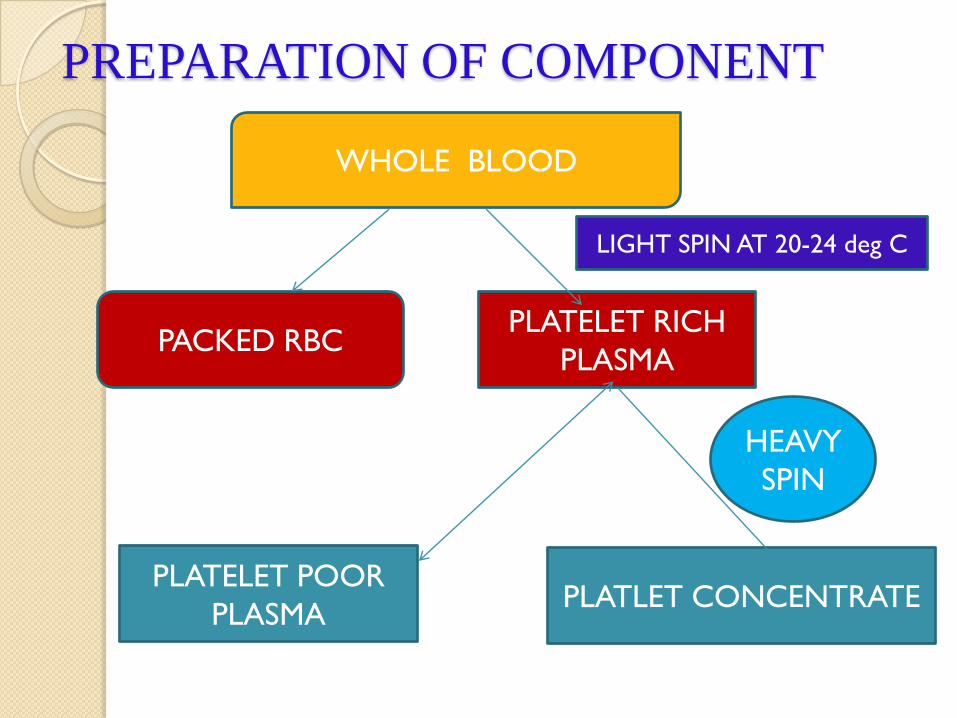
WHOLE BLOOD
PLATELET POOR
PLASMA
PLATELET RICH
PLASMAPACKED RBC
PLATLET CONCENTRATE
LIGHT SPIN AT 20-24 deg C
PREPARATION OF COMPONENT
HEAVY
SPIN

WHOLE BLOOD
P RBC Plasma
Light spin at 4
degree
PRBC
Heavy spin at 4
degree
Rapid freeze -70
deg C
Rapid thaw 0-6
deg
Cryo –poor
plasma
Plasma
Cryo
precipitateFFP Albumin
Buffy coat
granulocyteFreeze at -70
deg C within
6hr
PREPARATION OF COMPONENTS
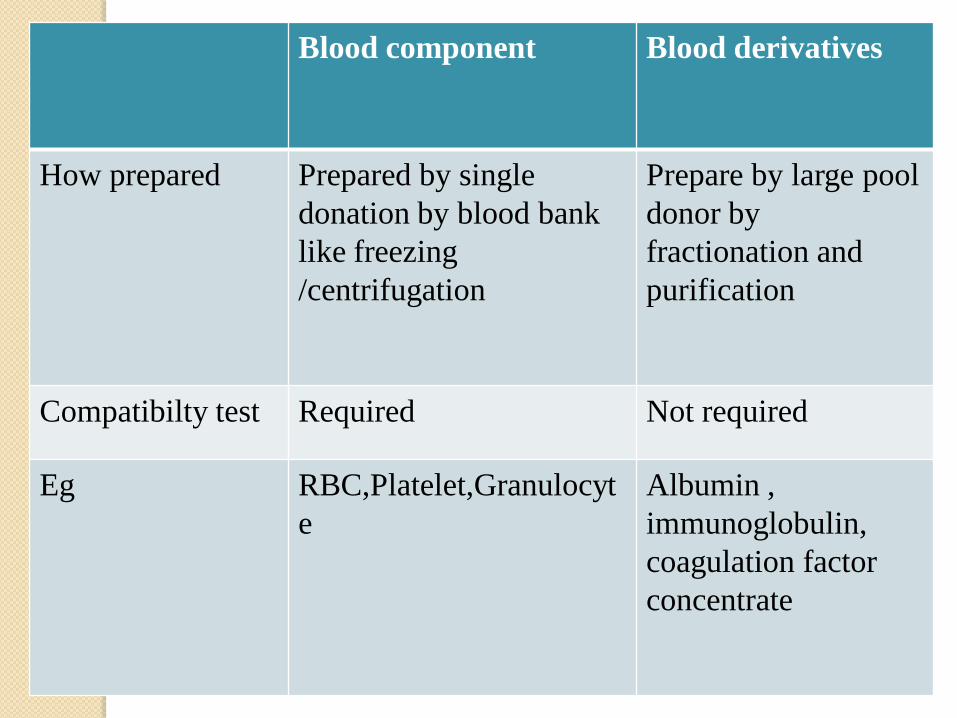
Blood component Blood derivatives
How prepared Prepared by single
donation by blood bank
like freezing
/centrifugation
Prepare by large pool
donor by
fractionation and
purification
Compatibilty test Required Not required
Eg RBC,Platelet,Granulocyt
e
Albumin ,
immunoglobulin,
coagulation factor
concentrate
What can be transfuseEither standard products (like whole blood, packed red cells) or
specialized ones like (saline washed red cells or frozen red cells).
The various options available for blood component therapy are : -
1. Cellular components
•Red cell concentrate and leucoreduced red cell concentrate
•Platelet concentrate
Granulocyte concentrate
2. Plasma components
•Fresh frozen plasma
•Cryoprecipitate
•Cryo poor Plasma

3. Plasma derivatives (commercial preparations)
•Albumin (5% & 20%)
•Factor VIII concentrate
•Fibrinogen
•Immunoglobulins
•Other coagulation factors
.
Terminology
• One whole blood unit : 350ml
blood/450mlwith14mlCPDA/100ml of
blood) of whole blood in the original
collection bag is referred to as one whole
blood unit
.
• One component unit : Each component
made from that unit is defined as one unit of
that component.
• Each whole blood unit constitutes approx
10% of a donors blood volume.
General measure for blood transfusion
Things to do before administering blood products
1. Donor blood and recipient identification
2. check the compatibility label.
attached to every blood pack with following information
patient name
hospital reference number
patient ward
patient ABO and Rh group
expiry date
date of compatibility test
blood group of blood pack
What to check in the blood pack
1. Sign of haemolysis in the plasma .plasma become
pink(indicate that either blood is contaminated /allowed to
freeze/too warm)
2. Sign of hemolysis on the line between the red cell and
plasma
3.change in color in the red cell (darker/purple or black
color ) indicative of contamination
4 .any clot
5. The patient ‘s identity and blood pack before
transfusion
don’t administer the transfusion if blood pack appear
abnormal or damaged or it has out of refrigerator for longer
than 30 min .

Infusion set• Transfused through BT set with inbuilt filters of standard size 170-
260 mm (helps removes microscopic clots, cellular debris,
undesirable particles).
• IV sets should not be used (no filter)
Blood warming• Routine warming is not needed
.
• As blood flows drop by drop, it attains body temperature quickly.
Warming is indicated in• Children being infused @>15 ml/kg/hr
• Infants receiving exchange transfusion
• Patients with cold agglutinins
Methods of heating• Water bath with warming coil
• Dry heat warmer
• High volume heat exchanger
• Blood should never be wormed in bowl of hot water(haemolysis)
In what duration tranfusion should be completed.• There is risk of bacterial proliferation and loss of function in
blood product once they have removed from correct storage
condition.

Time limit for infusion
Start infusion Complete infusion
Whole blood/ within 30 within 2 hour
Red cells minutes (4hr in unstable eg. CHF)
Platelet conc. Immediately within 30 minutes
Fresh Frozen As soon as within 30 minutes
Plasma possible

• Patient monitoring
DON’T left unattended while transfusion is on
Sever reaction (MC during initial 15 min of transfusion)
Monitor the patient at starting of transfusion ,15 min of
transfusion , at least every hour of transfusion ,at end of transfusion ,
at 4hr of end of transfusion.
Encourage the patient to notify any reaction as shivering, flushing
, pain ,shortness of breath, begining to feel anxious.
What to write on the blood transfusion notes
Record . Identity of patient /blood pack /compatibilty label/Time of
transfusion started/completed/volume and type of product/donor
number/any adverse reaction
Vital .appearance/temperature/pulse/respiratory rate / fluid
balance(input /urine out put)/BP
Addition of drug and medications to blood bag / Blood set
• Is prohibited except normal saline; however this should be
done in blood bank.
• The same IV line should not be used for any other IV
solution except NS
• 5% dextrose results in haemolysis .
• Ringer lactate causes clotting of blood in the tubing.
• Addition of drugs may cause a change in the blood or a
change in drug can occur because of pH and ionic molecular
constituent.

• transfusion circuit should be closed. Once the bag has been
punctured by BT set( blood is brought to the tip of the tubing,
which must be connected directly to venous access device. This
would constitute closed circuit)
Don’ts for blood transfusion• Don’t delay initiation of blood transfusion.
• Don’t use routine pre transfusion medications.
• Don’t add any medication to blood bag.
• Don’t use unmonitored refrigerator for storage.
• Don’t use transfusion set for more than one blood bag.

Red blood cell
• Whole Blood
• Packed Red Cells
• Leukoreduced
• Irradiated
•Frozen thawed

Whole blood transfusion
.Viable for 35 days for transfusion (with preservative used being
CPD-A).
FRESH BLOOD :- when whole blood /its component is used within
1 day of collection
Disadvantage – Use of freshly drawn whole blood is a
vestige of the old transfusion practice .
Processing donor blood, which includes typing for ABO &
Rh antigens, antibody screening tests of HBsAg, antibody to
HIV virus and syphilis is rarely completed in 24 hrs.
Thus, tests are no valid indications for transfusing fresh
whole blood before completing all necessary tests.

SPECIAL RECOMMENDATION FOR INFANT:-
• Whole blood stored upto 72 hrs is the ideal component for
exchange transfusion in neonates.
• Infants tolerate whole blood less than 7 days old which has
plasma electrolyte concentration within acceptable normal limits
and adequate 2,3-DPG.
Indication of whole blood transfusion:-
• Exchange transfusion(DVET) in neonate
• Acute Massive blood loss(>25% in children and >10% in neonate)
• Hyperleucocytosis in acute leukemia (with WBC count > 100×109/L)
• Non availability of blood component
( IAP speciality series on hemato-oncology 2006)
WHEN TO TRANSFUSE:-
• when a patient requires both replacement of circulatory volume and
increase in O2 carrying capacity.
• Where specific component is not available
WHEN NOT TO TRANSFUSE:-• Though transfusion of whole blood is the simplest way to infuse
plasma and red cells simultaneously, it is not always advisable to use
whole blood in MILD- MODERATE BLOOD LOSS.
(This is so because the concept that stored whole blood is closest in
composition to the fluid that has been lost is not true and the choice
of transfusion of whole blood may be harmful as well as
uneconomical).
So alternatively blood volume can be restored early with the infusions
on non O2 carrying solutions (either colloid or crystalloid) and the
restoration of circulating hemoglobin can be accomplished with
packed red cell transfusion (But this does not provide much
replacement of plasma proteins, so in extensive hemorrhage
clinicians prefer to give whole blood
How much to transfuse
• Amount of whole blood transfused is10- 20ml/Kg.
• For exchange transfusion, we use 2 x vol of neonate
blood (i.e. double the blood volume).

FACTS OF WHOLE BLOOD :-
• Almost 90% of platelets and 40% factors and activity are lost
within 24 hrs at temp of 1-60°C
• .
• Granulocytes begin to loose their phagocytic and bactericidal
properties within 4-6 hrs.
• RBC have about 80% post transfusion viability on storage in
CPD-A solution for 35 days.
• Following transfusion, half of 2,3 DPG levels regenerate in3-8
hrs while complete restoration of 2,3-DPG takes about 24hrs.
• Plasma of stored blood is equivalent to 5% albumin as a volume
expands.
What can GO wrong after whole blood transfusion
• Apart from usual complications, there may be deficiency of labile
clotting factor and platelets after massive transfusion.
• To prevent this, following can be transfused –
• FFP (1unit for 3-5 units of whole blood)
• Platelets (6 units of platelet concentrate for 10 units of whole blood)
• During double volume exchange transfusion hypocalcemia (due to
citrate ) ,which can be prevented by IV administration of Ca
gluconate (@2ml/Kg).
Special points to be remembered for whole blood transfusion
• Start the transfusion within 30 minutes of receiving the blood
(otherwise return it to blood bank)
• Once the temperature has crossed 10°C it cannot be restored .
• Transfusion must be completed in 4 hrs. (risk of bacterial
contamination)

PACKED CELL TRANSFUSION

Red blood cell/ packed cell transfusion
• Concentration of RBC depend on method of preparation .
•Sedimented cells : have PCV of 60-70%
•Centrifuged cells : have PCV of 80%
•Centrifuged cells with buffy coat expressed out : have PCV of >90%.
• Shelf-life:
– 21 days (CPD)
– 35 days (CPDA-1)
– 42 days AS-1
Component of choice to restore /maintain O2 . carrying capacity with
minimal expansion of blood volume
Advantages over whole blood :-
• Due to removal of plasma :
• Decrease in amount of electrolyte and ammonia and in
beneficial in patient with incipient CHF (Na+), renal failure
(due to K+ & acid) or hepatic failure (due to ammonia and
citrate).
• Chances of allergic /anaphylactic reactions are minimized.
• Decrease in amount of anti-A and anti-B normally present
in blood of individuals lacking corresponding antigen. This is
of value when it is necessary to use O group blood for recipient
of other blood groups.

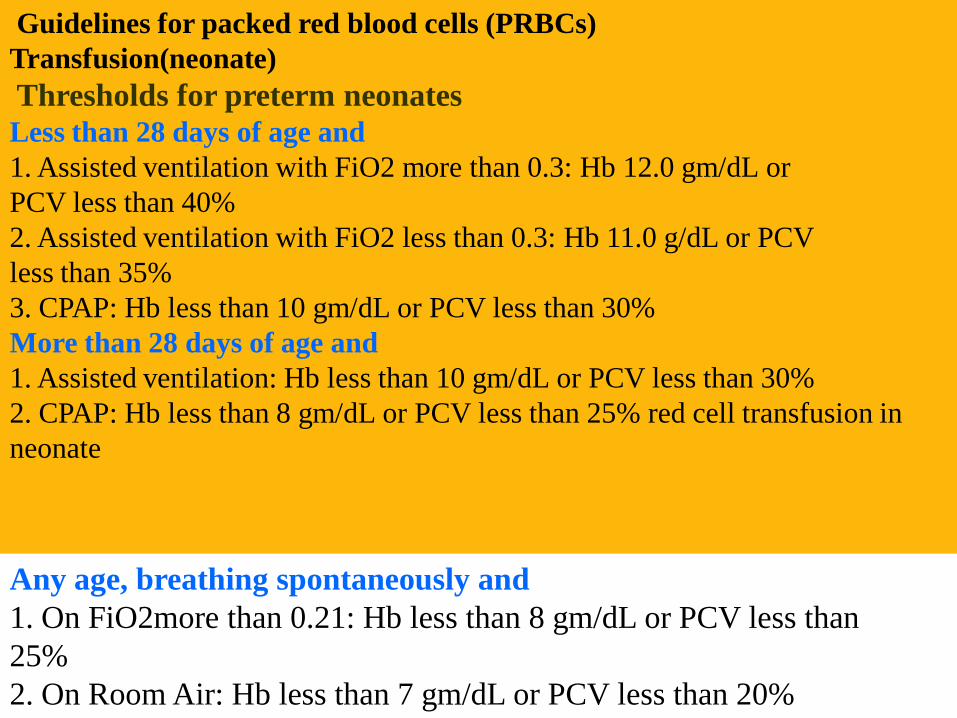
Guidelines for packed red blood cells (PRBCs)
Transfusion(neonate)
Thresholds for preterm neonates
Less than 28 days of age and
1. Assisted ventilation with FiO2 more than 0.3: Hb 12.0 gm/dL or
PCV less than 40%
2. Assisted ventilation with FiO2 less than 0.3: Hb 11.0 g/dL or PCV
less than 35%
3. CPAP: Hb less than 10 gm/dL or PCV less than 30%
More than 28 days of age and
1. Assisted ventilation: Hb less than 10 gm/dL or PCV less than 30%
2. CPAP: Hb less than 8 gm/dL or PCV less than 25% red cell transfusion in
neonate
Any age, breathing spontaneously and
1. On FiO2more than 0.21: Hb less than 8 gm/dL or PCV less than
25%
2. On Room Air: Hb less than 7 gm/dL or PCV less than 20%
(AIIMS NICU PROTOCOL 2008)

A. Asymptomatic with Hb < 7 gm with low retics/ Symptomatic anaemia with with Hb < 10 gm:
1. On <35% hood Oxgn/ nasal cannula
2. CPAP / IMV with MAP < 6cm water
3. Apnoea/bradycardia,tachypnoea/tachycardia.
4. Poor wt gain
B. Hb < 12 gm:
1. On >35% oxgn hood
2. CPAP / IMV with MAP > 6-8
C. Hb < 15 gm:
1. Cynotic CHD
2. ECMO ( IAP guidelines 2006)
RBC transfusion < 4 month of age
> 4 mnths of ageA. Blood loss:
> 15% total body volume/ with hypovolemia
B. Hb < 8gm
1. Symptomatic perioperative anaemia
2. Chemotherapy/radiotherapy
3. Chronic congenital/acquired anaemia
4. Emergency surgery with anticipated bld loss
5. Uncorrectable preoperative anaemia
6. Severe infection
C. Chronic transfusion dependent states:
1. Thalassemia and other hemoglobinopathies
2. Bone marrow failure states
D. Patient in overt or impending CCF due to anemia (IAP guidelines 2006)
Transfusion dependent anemias/Thalassemias
Every 3-4 wks ,maintain pre transfusion Hb 9.5-10.5gm% &
post transfusion Hb 13-13.5%.
Pediatrics Oncology( May be done acc.to protocol):
1.Hb < 8 gm% and/or symptomatic anemia
2.Maintain Hb%>10 gm if intensive chemotherapy is due.
3. Febrile neutropenia
4.Thrombocytopenic bleeding
5.Hyperleukocytosis ( Partial exchange preferable)
Special situations
How much to transfuse
• Standard transfusion volume : 10ml/kg(maximum 15ml/kg in
hemodynamicaly stable).
• In severe anemia (Hb<5gm%), child should receive multiple
small transfusions of 3-5ml/kg over 3 hrs.
• A partial exchange transfusion is recommended when there is
overt CHF.
Advantage : Anemia is corrected rapidly and isovolumically.
Factor determining RBC transfusion
•Cardorespiratory status of patient.
•Cause and anticipated course of underlying anemia.
•Alternative therapy such as iron and recombinant EPO.

What to expect after transfusion
• Each 8ml/kg of RBCs in children and 3ml/kg in infant is
expected to raise Hb by1gm% and Hct by 3%.
• In actively bleeding, the response cannot be assessed by blood
count or Hb; accurate assessment is made by monitoring CVP.
Modifications of packed cells
A) Leucocyte poor RBCs
• LR contain <70% of original WBC and retains 70 % of
the original red cells
• Reduces febrile reactions
• Reduces HLA immunization (e.g. transplant)
• Effective in reducing CMV transmission (CMVsafe)
• Cellular immune function preservation
• Does NOT prevent GVHD!!!
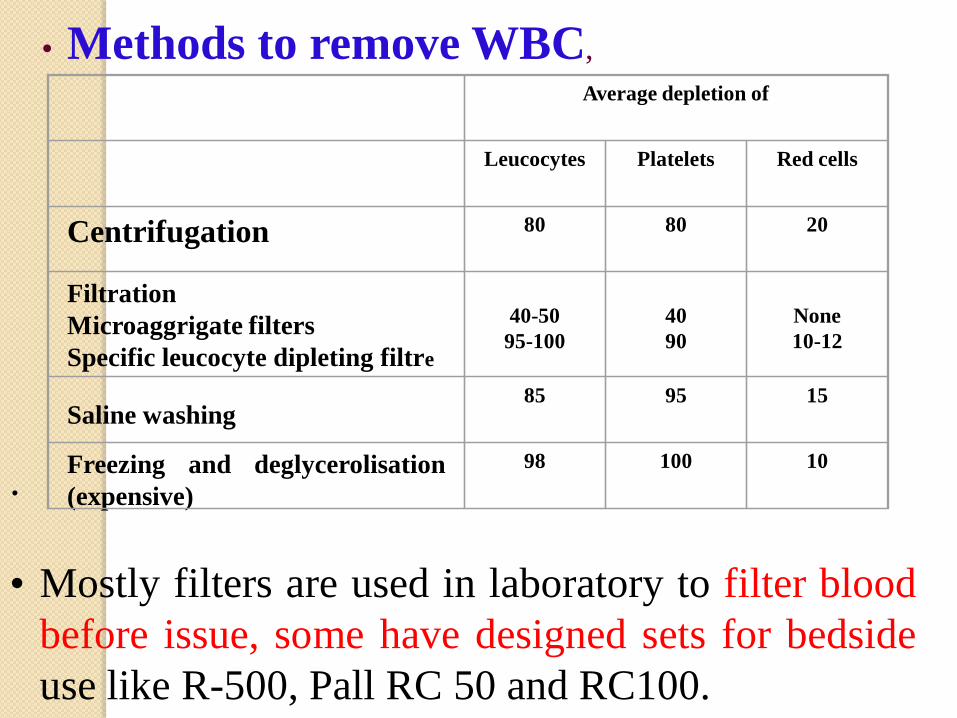
• Methods to remove WBC,
Average depletion of
Leucocytes Platelets Red cells
Centrifugation 80 80 20
Filtration
Microaggrigate filters
Specific leucocyte dipleting filtre
40-50
95-100
40
90
None
10-12
Saline washing85 95 15
Freezing and deglycerolisation
(expensive)
98 100 10
.
• Mostly filters are used in laboratory to filter blood
before issue, some have designed sets for bedside
use like R-500, Pall RC 50 and RC100.

Clinical conditions which benefit from
leucoreduction
Thalassaemia major
Aplastic anaemia
Sickle cell anaemia
Leukaemia
Patients for organ transplantation
Patients on Dialysis
Patients with multiple/chronic infections

B) Frozen RBCs
• Red cells can be frozen in glycerol and stored at subzero
temperature for as long as 10 years.
Advantages :
• long term storage for use in patients with rare blood groups
especially in the form of autologous transfusion.
.
• Use of frozen thawed and deglycerolised blood prevents non
hemolytic febrile reactions in patients sensitized to WBC,
platelets or plasma proteins.
• It also prevents sensitisation against HLA antigens .

Irradiated Blood Components
Gamma irradiation of component
Inactivates donor lymphocytes to prevent Graft Vs. Host disease
(GHVD). Only accepted method.
Expiration date: 28 days (RBCs) from irradiation or original
outdate - which ever comes first.

Irradiated Blood Products- Indications
Congenital Immunodeficiency's: SCID, DiGeorge Syndrome
Bone Marrow Transplan
Intrauterine Transfusion of Fetus

PLATELET

Platelet transfusion
Platelet rich plasma
• Platelet concentrate
Types of platelet concentrates : –
• Random donor platelets (RDP) : Prepared from donated blood
within 4-6 hrs of collection by centrifugation and it contains
approx 5.5×1010 platelets.
• Single donor platelets (SDP) : are prepared by plasma apheresis
.
One unit of SDP : 5-10 units of RDP
One unit PC prepared from 450 ml of
whole blood contains at least 5.5×1010
platelets in 50ml plasma. One unit of PRP
has the same amount of platelet in 250ml
plasma.
Platelet transfusions
The indications for transfusion in children with quantitative and
qualitative platelet disorders are similar to those for adults but
neonates and infants <4mth from a special group and may need
platelet support at even higher platelet counts.
Decision making in platelet transfusions
Decision to transfuse platelets depends upon :
• Platelet count and function
• Clinical condition of the patient
• Cause of thrombocytopenia(marrow failure/ITP)
• Comfort level of treating physician

THERAPEUTIC PT PROPHYLACTIC PT
Thrombocytopenia + life
threatening bleed( intracranial,
malena, gum bleed , sever
menorrhagia )
Not very much
recommended dictim is if
no bleed don’t transfuse .
Platelet transfusion not
indicated for bleed like petechial
/ purpura/ echymosis
Thrombocytopenia <50,000
life threatening bleed is <1%
Transfuse at platelet count
<10,000 associated with
sepsis, fever, amphotericin B
therapy
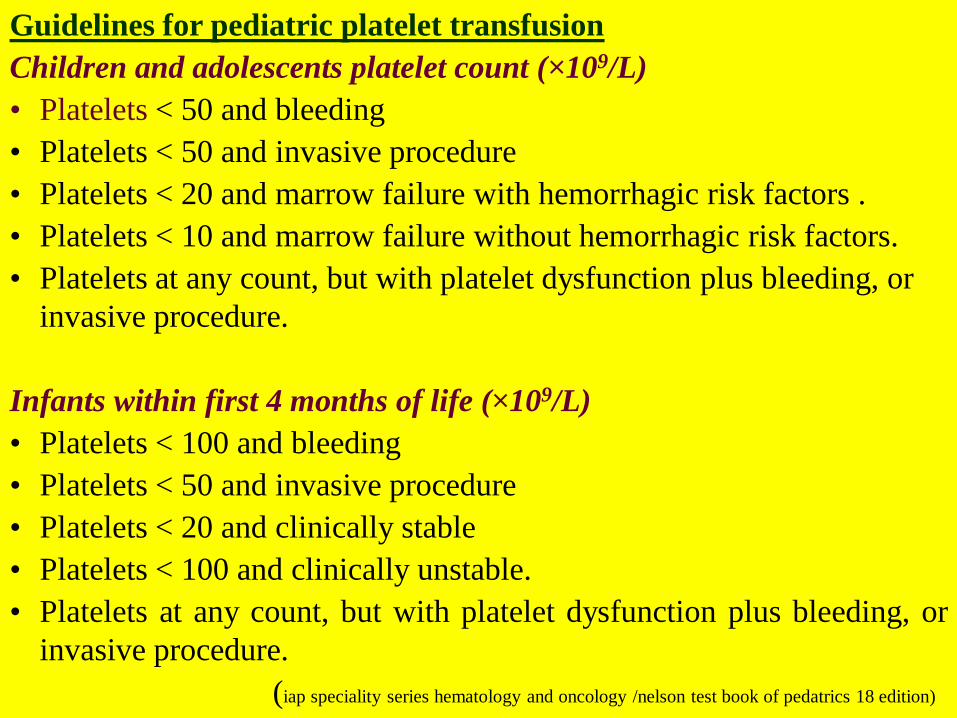
Guidelines for pediatric platelet transfusion
Children and adolescents platelet count (×109/L)
• Platelets < 50 and bleeding
• Platelets < 50 and invasive procedure
• Platelets < 20 and marrow failure with hemorrhagic risk factors .
• Platelets < 10 and marrow failure without hemorrhagic risk factors.
• Platelets at any count, but with platelet dysfunction plus bleeding, or
invasive procedure.
Infants within first 4 months of life (×109/L)
• Platelets < 100 and bleeding
• Platelets < 50 and invasive procedure
• Platelets < 20 and clinically stable
• Platelets < 100 and clinically unstable.
• Platelets at any count, but with platelet dysfunction plus bleeding, or
invasive procedure.
(iap speciality series hematology and oncology /nelson test book of pedatrics 18 edition)
Recommendations for platelet transfusion during infancy
• Sick Preterm :-goal is to keep platelet >50,000/cu mm.
.
Most neonatologists use a platelet count < 50,000/ cu mm as a
transfusion trigger in these circumstances
• platelets should be transfused to any neonate whose platelet count is
<20,000 / cu mm.
• Currently, there are no alternatives to platelet transfusion to treat
thrombocytopenia in neonates.(nelson testbook of pediatrics /mannual of neonatal care 6th edition )
Some important point in thrombocytopenia
Bone marrow aspiration and biopsy can be performed with
sever thrombocytopenia
Lumber puncture,epidural anesthesia platelet count should be
raised to 50,000/cu mm.
Operation in critical situation brain /eye platelet count should
be >1,00,000/cu mm
Immune Thrombocytopenia platelet transfusion should be
reserve with life threatening bleed from G I tract / CNS bleed.

How to transfuse :-
• Do not store platelet in hospital refrigerator.
• Administer through a separate IV line.
• Begin with a slow infusion rate, if there is no reaction, infuse rapidlyso as to complete all platelets within an 30 min.
• Leucodepletion filter sets specific for platelet transfusion are availableand should be used in an affording patients.
Advantages of leucodepletion filter
• Prevents : FNHTR, Transmission of CMV infection..

What to expect after transfusion
• one unit of platelet concentrate raises the platelet count, 1hr
after transfusion, by 5000-10,000/ cu mm / sq.m BSA.
• Life span after infusion in few hrs to maximum 24 hrs.
What can go wrong after transfusion
A part from transfusion complications as detailed later following
can be expected.
• Due to storage temperature of 22°C, there is a higher risk of
FNHTR and bacterial contamination.
Dosage and administration :Standard dose 1 unit / 10 kg.For pediatric patients< 8 kgs, 5 ml/ kg - increase in
platelet count by 50,000/uLFor patients > 8 kg – 1 unit / 10 kg.

Facts about Platelet transfusion to be remembered
• Normal platelets express ABOAg on their surface : they do not
express RhD antigen .
• SDP donor should be of the same blood group.
• RDP of the same blood group is recommended (except in
emergency)
• Rh-negative women in reproductive age group should receive
Anti D if they receive RDP from Rh +ve donor, to prevent Rh
sensitization from contaminating RBs.
• Some amount of RBC contamination is inevitable(do cross
matching if repeated transfusion require)
• .There is no need to keep continuously shaking during the
transfusion.

Granulocyte
Granulocyte transfusion
• Use of recombinant granulocyte colony stimulating factor (G-
CSF) have made it possible to collect excessively large number of
normal neutrophils for transfusion into neutropenic patients who
have life threatening infections.
• must be ABO compatible with because contamination with red
blood cells.
• Prepared from a single donor using apheresis or manually
• contain at least > 1.0 x 1010 granulocytes
• Stimulated can yield 4-8 x 1010 granulocytes
• Stored at 24 deg C
• Infused within 24 hours of collection
Guidelines for transfusion neutrophils
children :
• Neutrophils < 500/ml + bacterial infection + unresponsive to
antibiotics.
• Neutrophils <500/ml + yeast or fungal infection progressing or
appearing during treatment with antimicrobials.
• Neutrophils dysfunction with bacterial, yeast, fungal infection
unresponsive to antimicrobials.
infants < 4 months
• Neutrophils<3000/ml + fulminant sepsis during the first week of life.
• Neutrophils <1000/ml + fulminant sepsis after the first week of life.
(IAP speciality series on hematology & oncology 2006)

Therapeutic approach
Course of treatment - Daily GTx for atleast 4 days is recommended.
- Treatment is based upon clinical judgement and the
response of the patients.
Dosage - Current standards require a minimum of 1×1010
granulocytes per concentrate and at least double this no.
is desirable.
- Neonates may receive upto 1×109
granulocytes/kg/day.
Timing of storage- stored for upto 24 hrs at room temperature without
agitation but show progressive loss of function with
storage and are therefore, transfused as soon as possible
after collection (usually within 6 hrs).
Transfuse within an hour of receipt from blood bank.

How to transfuse
• Transfuse through standard blood filter (don’t use leucoreduction
filter)
•Irradiate to prevent GVHD

FRESH FROZEN PLASMA

Fresh frozen plasma
• The volume from a single donation is about 200ml.
• Single donar plasma – plasma from a single donor, prepared byseparation form whole blood on or before the fifth day after expiry iscalled single donor plasma.
• For preparation of FFP, while collecting blood, the flow should berapid form the start and it is recommended that the total time taken tocollect 450ml of blood should not be more than 10 mins.
• FFP contains Factor 2,5,7, 8 , 9, 11 and fibrinogen.
• FFP should be administered within half an hour after thawing as the
activity of factor 5 and factor 8 are rapidly lost.
• FFP has self life of 1 year if kept at –30°.C
• Dose – Usually a dose of 10-15ml/kg weight is recommended at a
flow rate not exceeding 10ml/min.
• Indication –1).Replacement of coagulation factor in liver disease(abn coagulation
profile eighter prophylactic /control bleeding), deficiency of vitamin
K dependent factors (2,7, 9,10)eg HDN with bleeding , DIC with
bleeding, overdose of oral anticoagulants/ multiple coagulation
factor deficiency.
2.)Specific deficiencies of factors 5, 8 and 11. FFP is the only
available source for factor 5 . There is no factor 5 conc available
.
3.)Urgent replacement of missing hemostatic factor in bleeding
patients when specific concentrate preparations are not available as
in case of haemophilia A, Haemophilia B.4.) anticoagulant protein (protein C and S ) replacement
5.) plasma exchange replacement fluid for thrombotic thrombo -
cytopenic purpura
6) unknown facto deficiency
(iap guidelines 2006/nelson test book 18 edition )

Indication of FFP transfusion in neonate
1. Disseminated intravascular coagulopathy
2. Vitamin K deficiency bleeding
3. Inherited deficiencies of coagulation factors
rare indications include patients with afibrinogenemia,
vonWillebrand factor deficiency, congenital antithrombin III
deficiency,
protein C deficiency and protein S deficiency when specific factor
replacement is not available. It is also used for reconstitution of
blood for exchange transfusion.
FFP is not indicated for correction of hypovolumia or
immunoglobulin replacement therapy due to safer
alternative(albumin/saline /immunoglobulin)

CRYOPRECIPITATE
Cryoprecipitate
• Cryoprecipitate are precipitated proteins of plasma rich in
factor 8 factor 13 ,fibronectin , fibrinogen and von
willibrand factor.
• One unit of Cryoprecipitate contains (volume 10-20ml)
80 -120 unit factor 8
• ABO compatible unit is preferable . Rh compatibility
testing is not required.
• Usual dose is 2 unit / 10 kg ( IAP guidelines 2006)

• Indication for cryoprecipitate
1) Cryoprecipitate is used in moderate and severe hemophilia A
in the absence of factor 8
2) Von Willebrands disease .
3) Dysfibrongenemia, hypofibrinogenemia and consumptive
coagulopathies.
4) Intactable bleeding in uremia and platelet storage pool disease.
5) Congenital factor 13 deficiency.
( iap guidelines 2006/ nelson test book of pediatrics 18 edition)
May be beneficial in patients with septicemia or burns because of
fibronectin content.

Specific factor concentrates
• Specific factor concentrates include antihemophilic factor
concentrate (AHF), factor 8, and prothrombin complex.
• They can be stored at 6-8° for 2 years.
• Intermediate purity factor 8 concentrates contain 15-20 IU/ml. It
is the product of choice for moderate and severe hemopilia A.
• The dose and frequency of administration of these products
would need to be tailored to the severity of bleeding
manifestations is an individual patient.

Lesion Level of factor 8
desirable 15 min
after infusion
(IU/dl)
Factor 8
dose/kg
No. of infusions
required
Early hemartheosis
minor external bleeds
10-20 10-15 1-3 times 12
hourly
Severe hemarthrosis
internal haemorrhage
29-70 15-50 3-7 times 12
hourly then 24
hourly
Major surgery serious
accidents
70-100 50-70 12 hourly, until
normal bleeding
and rehabilitation
completed.
• If the facilities of factor assays are not available, PTT can be
used as a rough guide to factor 8 activity. If PTT is in normal
range, the factor 8 level is usually over 30%, if the PTT is
prolonged, factor 8 level will be generally low.
• Prothrombin complex when reconstituted contains 30-100 IU/ml
of all factors in it. It is recommended for replacement therapy in
hemophilia B (factor 9 deficiency) but may also be used for
congenital or acquired deficiency of factors 2, 7 or 10, and
bleeding in hemophiliacs with antibodies against factor 8.
• Antithrombin 3 concentrates are used for treating thrombotic
episodes in patients with congenital AT III deficiency in a dose
of50 units/kg body weight.
ALBUMIN
5% albumin k/a PPF(90%
albumin & 10% globulin) 20% albumin
Burn
Extensive surgery
Hemorrhagic shock waiting
for blood
Partial exchange
Nephrotic syndrome with
anasarca(.5 – 1gm/kg) f/b
diuretic within 15 min of
administration
PPF=plasma protein fraction

Immunoglobulins
Normal :-mix of IgG – obtain
by fractionation of plasma
(IV/IM)
Specific:- from donor with high
specific Ab against pathogen (IM)
Prevention & treatment of disease (hep B, varicella,measles,tetanus
,rabies)
Replacement therapy (Hypogamglobulinemia)
Immune disorder ( ITP, kawasaki disease, AIDP)
Myasthenia gravis,life threatening lupus
Sever sepsis in neonate
Prevention of sensitization in Rh neg women by administrating anti D
INDICATION
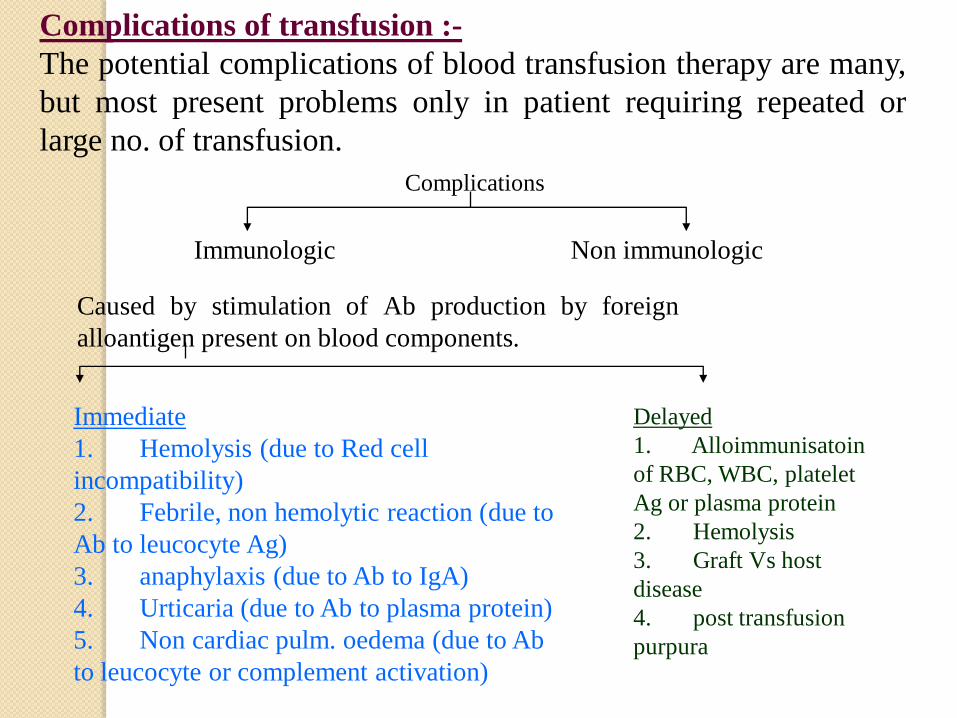
Complications of transfusion :-
The potential complications of blood transfusion therapy are many,
but most present problems only in patient requiring repeated or
large no. of transfusion.
Complications
Immunologic Non immunologic
Caused by stimulation of Ab production by foreign
alloantigen present on blood components.
Immediate
1. Hemolysis (due to Red cell
incompatibility)
2. Febrile, non hemolytic reaction (due to
Ab to leucocyte Ag)
3. anaphylaxis (due to Ab to IgA)
4. Urticaria (due to Ab to plasma protein)
5. Non cardiac pulm. oedema (due to Ab
to leucocyte or complement activation)
Delayed
1. Alloimmunisatoin
of RBC, WBC, platelet
Ag or plasma protein
2. Hemolysis
3. Graft Vs host
disease
4. post transfusion
purpura
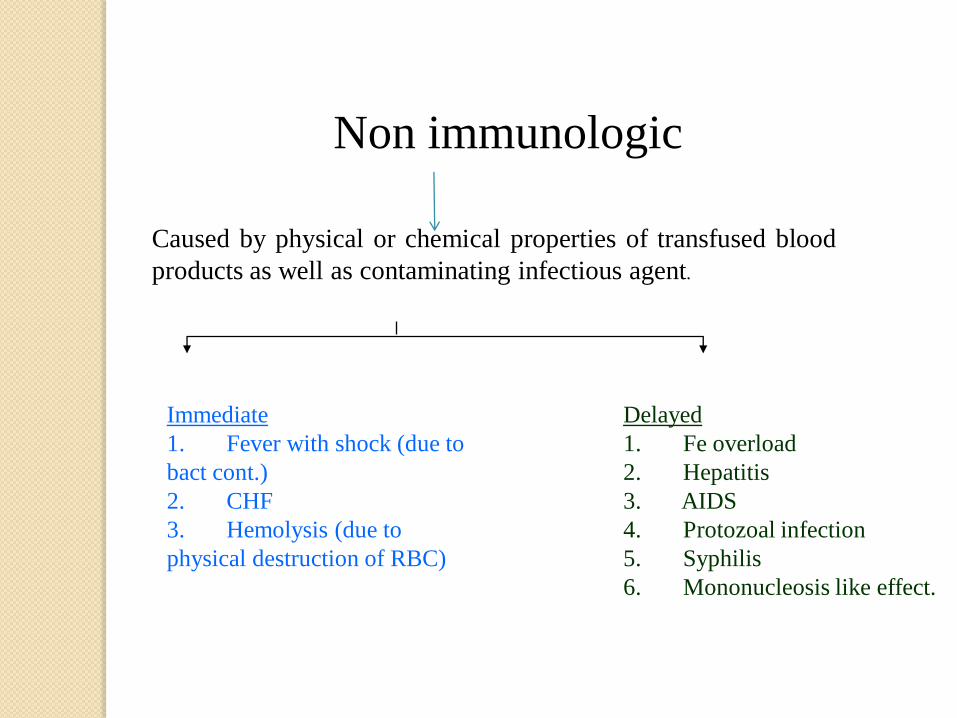
Caused by physical or chemical properties of transfused blood
products as well as contaminating infectious agent.
Immediate
1. Fever with shock (due to
bact cont.)
2. CHF
3. Hemolysis (due to
physical destruction of RBC)
Delayed
1. Fe overload
2. Hepatitis
3. AIDS
4. Protozoal infection
5. Syphilis
6. Mononucleosis like effect.
Non immunologic
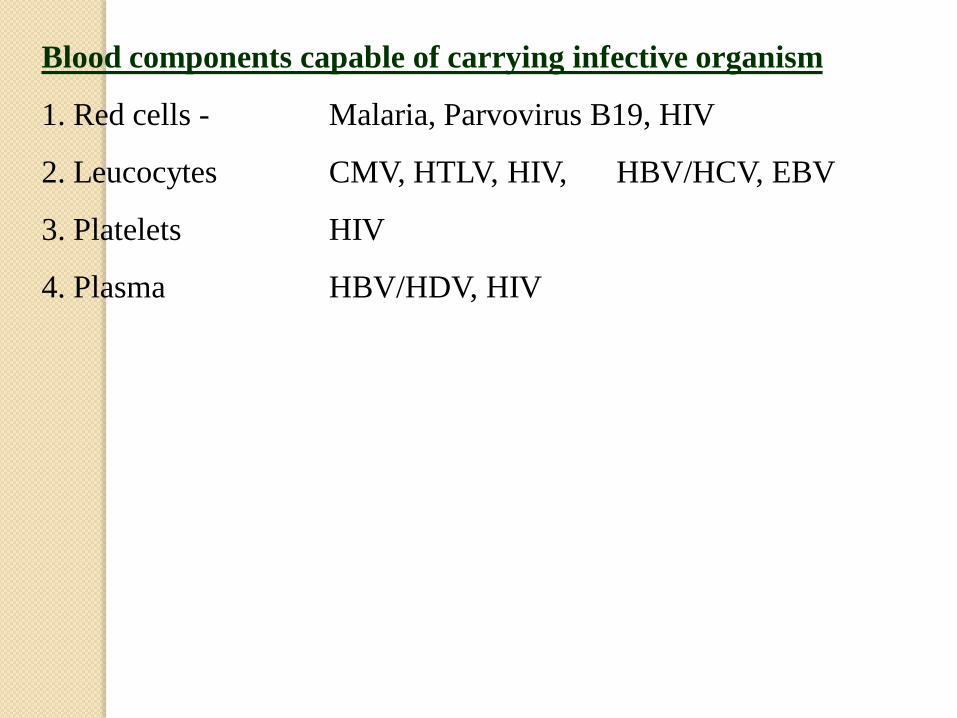
Blood components capable of carrying infective organism
1. Red cells - Malaria, Parvovirus B19, HIV
2. Leucocytes CMV, HTLV, HIV, HBV/HCV, EBV
3. Platelets HIV
4. Plasma HBV/HDV, HIV
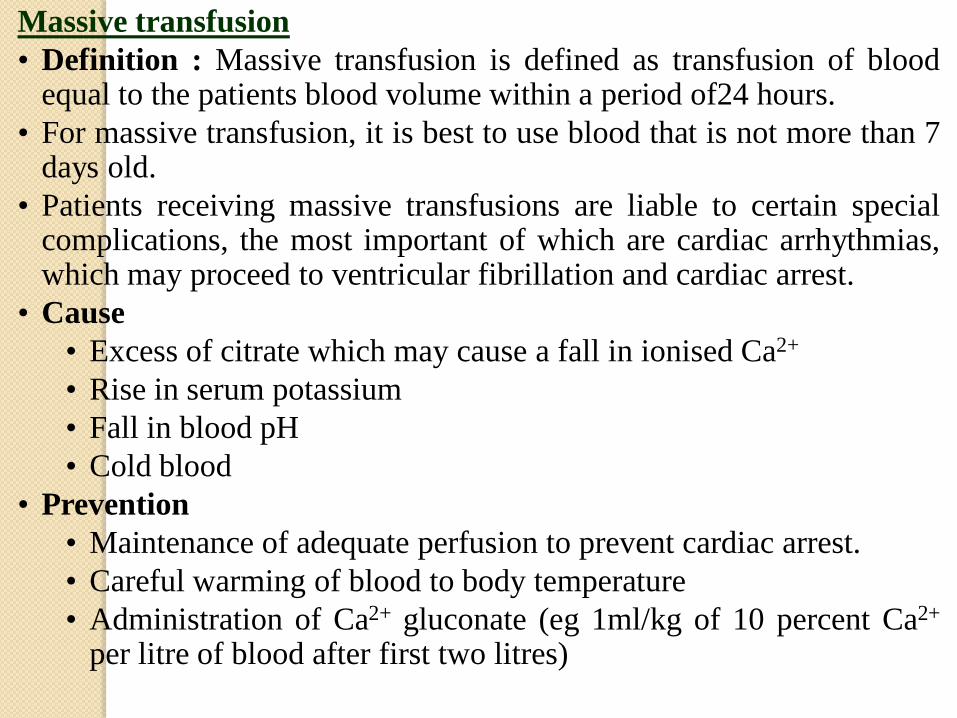
Massive transfusion
• Definition : Massive transfusion is defined as transfusion of bloodequal to the patients blood volume within a period of24 hours.
• For massive transfusion, it is best to use blood that is not more than 7days old.
• Patients receiving massive transfusions are liable to certain specialcomplications, the most important of which are cardiac arrhythmias,which may proceed to ventricular fibrillation and cardiac arrest.
• Cause
• Excess of citrate which may cause a fall in ionised Ca2+
• Rise in serum potassium
• Fall in blood pH
• Cold blood
• Prevention
• Maintenance of adequate perfusion to prevent cardiac arrest.
• Careful warming of blood to body temperature
• Administration of Ca2+ gluconate (eg 1ml/kg of 10 percent Ca2+
per litre of blood after first two litres)

Bibliography
IAP Text book of pediatrics 4th edition
Nelson test book of pediatrics(18th edition)
Wintrobes’s Hematology 21st Edition.
IAP Specialty series on pediatric hematology and oncology.
(Under IAP president action plan 2006)
Recent advances in Neonatology (Publication of NNF)
Advances in pediatrics-1 (Indian Journal of Paediatrics)
Transfusion medicine technical manual (Makroo& Saran)
De-Gruchy’s clinical Hematology in Medical Practice, 5th Ed.
Workshop of hematology (Held in Mumbai Pedicon 2007 on 9th
Jan2007).

Guidelines for packed red blood cells (PRBCs)
Transfusion(neonate)
Thresholds for preterm neonates
Less than 28 days of age and
1. Assisted ventilation with FiO2 more than 0.3: Hb 12.0 gm/dL or
PCV less than 40%
2. Assisted ventilation with FiO2 less than 0.3: Hb 11.0 g/dL or PCV
less than 35%
3. CPAP: Hb less than 10 gm/dL or PCV less than 30%
More than 28 days of age and
1. Assisted ventilation: Hb less than 10 gm/dL or PCV less than 30%
2. CPAP: Hb less than 8 gm/dL or PCV less than 25% red cell transfusion in
neonate
Any age, breathing spontaneously and
1. On FiO2more than 0.21: Hb less than 8 gm/dL or PCV less than
25%
2. On Room Air: Hb less than 7 gm/dL or PCV less than 20%

Graft vs Host Disease
• It occurs in patients following transfusion who are severely
immunosuppressed, such as those being intensively treated with
chemotherapy and radiation.
• It is also a rare event in infants who receive intrauterine
transfusions followed by exchange transfusion for haemolytic
disease of new born.
• Mechanism : GVH disease occurs if donor functional
lymphocytes engraft and multiply. These engrafted donor cells
react against the foreign tissue of the host (recipient).

• Symptoms – Include fever, skin rashes, hepatitis, diarrhea, bone
marrow suppression and other infections.
• Outcome is usually fatal.
• Prevention – pre transfusion irradiation of all blood components
containing lymphocytes will prevent GVH disease. The
functions of red cells, granulocytes and platelets are not affected
by such irradiation; but irradiation slightly decreases the ability
of red cells to tolerate storage. For this reason it is recommended
that irradiated red cells not be stored for more than 28 days.
Irradiation is required for infants weighing less than 2kg. Blood
irradiators are capable of delivering 15-30GY over 1-5 minutes
per unit; this dose effectively inactivates immunocompitent T
cells.
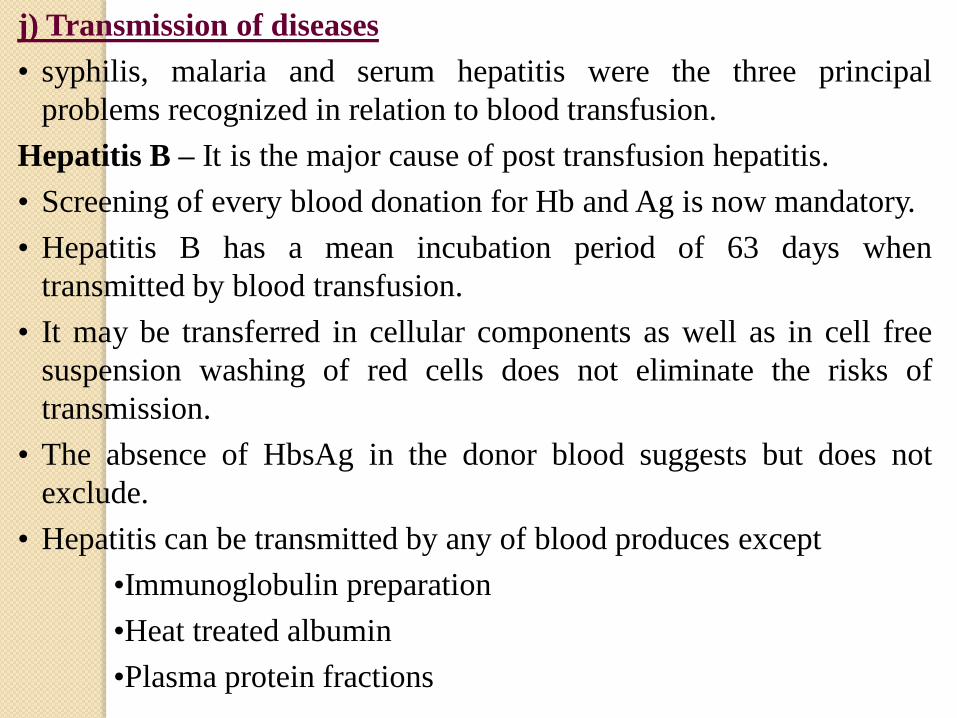
j) Transmission of diseases
• syphilis, malaria and serum hepatitis were the three principal
problems recognized in relation to blood transfusion.
Hepatitis B – It is the major cause of post transfusion hepatitis.
• Screening of every blood donation for Hb and Ag is now mandatory.
• Hepatitis B has a mean incubation period of 63 days when
transmitted by blood transfusion.
• It may be transferred in cellular components as well as in cell free
suspension washing of red cells does not eliminate the risks of
transmission.
• The absence of HbsAg in the donor blood suggests but does not
exclude.
• Hepatitis can be transmitted by any of blood produces except
•Immunoglobulin preparation
•Heat treated albumin
•Plasma protein fractions

• Testing of blood for anti Hbc in addition to HbsAg would reduce
the incidence of HBV from HBsAg negative blood by about 50%.
Hepatitis C
• After the introduction of routine screening for hepatitis B, the
great majority of hepatitis following transfusion was found to be
related to non A, non B hepatitis (NANBH) ; hepatitis C virus has
been found to be the major cause of such cases.
• Hepatitis C can be transmitted by blood and blood products
including IVIg, albumin and factor VIII concentrates.
Cytomegalovirus
• Was first recognize as a cause of post transfusion pyrexia and
hepatiis in patients undergoing open heart surgery.
• Significance CMV induced disease is much more common in
recipients who are immunosuppresed.


















