BLBK170-Langley April 6, 2009 14:54 Nutrition: A Lifespan ... · BLBK170-Langley April 6, 2009...
30
Nutrition: A Lifespan Approach Simon Langley-Evans, BSc., Phd., RNutr. Chair in Human Nutrition School of Biosciences University of Nottingham A John Wiley & Sons, Ltd., Publication
Transcript of BLBK170-Langley April 6, 2009 14:54 Nutrition: A Lifespan ... · BLBK170-Langley April 6, 2009...

BLBK170-Langley April 6, 2009 14:54
Nutrition: A Lifespan Approach
Simon Langley-Evans, BSc., Phd., RNutr.Chair in Human NutritionSchool of BiosciencesUniversity of Nottingham
A John Wiley & Sons, Ltd., Publication
i


BLBK170-Langley April 6, 2009 14:54
Nutrition: A Lifespan Approach
Simon Langley-Evans, BSc., Phd., RNutr.Chair in Human NutritionSchool of BiosciencesUniversity of Nottingham
A John Wiley & Sons, Ltd., Publication
i

BLBK170-Langley April 6, 2009 14:54
This edition first published 2009C© 2009 Simon Langley-Evans
Blackwell Publishing was acquired by John Wiley & Sons in February 2007. Blackwell’s publishing programme has beenmerged with Wiley’s global Scientific, Technical, and Medical business to form Wiley-Blackwell.
Registered officeJohn Wiley & Sons Ltd, The Atrium, Southern Gate, Chichester, West Sussex, PO19 8SQ, United Kingdom
Editorial offices9600 Garsington Road, Oxford, OX4 2DQ, United Kingdom2121 State Avenue, Ames, Iowa 50014-8300, USA
For details of our global editorial offices, for customer services and for information about how to apply for permission toreuse the copy r ig ht mater ial in this book please see our website at www.w ile y.com/w ile y-blackwe ll.
The right of the author to be identified as the author of this work has been asserted in accordance with the Copyright,Designs and Patents Act 1988.
All rights reserved. No part of this publication may be reproduced, stored in a retrieval system, or transmitted, in any formor by any means, electronic, mechanical, photocopying, recording or otherwise, except as permitted by the UK Copyright,Designs and Patents Act 1988, without the prior permission of the publisher.
Wiley also publishes its books in a variety of electronic formats. Some content that appears in print may not be available inelectronic books.
Designations used by companies to distinguish their products are often claimed as trademarks. All brand names andproduct names used in this book are trade names, service marks, trademarks or registered trademarks of their respectiveowners. The publisher is not associated with any product or vendor mentioned in this book. This publication is designed toprovide accurate and authoritative information in regard to the subject matter covered. It is sold on the understanding thatthe publisher is not engaged in rendering professional services. If professional advice or other expert assistance is required,the services of a competent professional should be sought.
Library of Congress Cataloging-in-Publication Data
Langley-Evans, S. C.Nutrition : a lifespan approach / Simon Langley-Evans.
p. ; cm.Includes bibliographical references and index.ISBN 978-1-4051-7878-5 (pbk. : alk. paper) 1. Nutrition–Textbooks.
I. Title.[DNLM: 1. Nutritional Requirements. 2. Diet. 3. Growth and Development–physiology. 4. Nutrition
Assessment. 5. Nutritive Value. QU 145 L283n 2009]QP141.L2 2009612.3–dc22
2008053122
A catalogue record for this book is available from the British Library.
Set in 10/12pt Minion by Aptara R© Inc., New Delhi, IndiaPrinted in Singapore
1 2009
ii

BLBK170-Langley April 6, 2009 14:54
Contents
Preface xi
Acknowledgments xii
1. Introduction to Lifespan Nutrition 11.1 The lifespan approach to nutrition 11.2 The concept of balance 2
1.2.1 A supply and demand model 21.2.2 Overnutrition 21.2.3 Undernutrition 4
1.2.3.1 Increased demand 41.2.3.2 The metabolic response to trauma 41.2.3.3 Compromised supply and deficiency 61.2.3.4 Malnutrition 7
1.2.4 Classical balance studies 81.2.5 Overall nutritional status 10
1.3 Nutrition requirements change across the lifespan 101.4 Assessment of nutritional status 11
1.4.1 Anthropometric measures 121.4.2 Estimating dietary intakes 12
1.4.2.1 Indirect measures 121.4.2.2 Direct measures 13
1.4.3 Biomarkers of nutritional status 151.4.4 Clinical examination 16
1.5 Dietary reference values 161.5.1 The UK dietary reference value system 171.5.2 Dietary reference values in other countries 19
2. Before Life Begins 232.1 Introduction 232.2 Nutrition and female fertility 24
2.2.1 Determinants of fertility and infertility 242.2.1.1 The endocrine control of female reproduction 242.2.1.2 Disordered reproductive cycling 252.2.1.3 Polycystic ovary syndrome 252.2.1.4 Assisted reproductive technologies 26
2.2.2 Importance of body fat 262.2.3 Role of leptin 272.2.4 Antioxidant nutrients 282.2.5 Caffeine and alcohol 30
2.3 Nutrition and male fertility 322.3.1 Determinants of fertility and infertility 322.3.2 Obesity 342.3.3 Diabetes 342.3.4 Alcohol 35
iii

BLBK170-Langley April 6, 2009 14:54
iv Contents
2.3.5 Zinc 352.3.6 Antioxidant nutrients 362.3.7 Selenium 372.3.8 Phytoestrogens and environmental estrogens 37
2.3.8.1 Phthalates 372.3.8.2 Phytoestrogens 382.3.8.3 Pesticides 38
2.4 Preparation for pregnancy 392.4.1 Why prepare for pregnancy? 392.4.2 Vitamin A and liver 402.4.3 Folic acid and neural tube defects 41
2.4.3.1 Supplementation with folic acid 422.4.3.2 Fortification with folic acid 43
3. Pregnancy 473.1 Introduction 473.2 Physiological demands of pregnancy 48
3.2.1 Maternal weight gain and body composition changes 493.2.2 Blood volume expansion and cardiovascular changes 493.2.3 Renal changes 503.2.4 Respiratory changes 503.2.5 Gastrointestinal changes 513.2.6 Metabolic adaptations 51
3.3 Nutrient requirements in pregnancy 523.3.1 Energy, protein, and lipids 523.3.2 Micronutrients 54
3.3.2.1 Iron 543.3.2.2 Calcium and other minerals 553.3.2.3 Vitamin D 56
3.4 Diet in relation to pregnancy outcomes 573.4.1 Miscarriage and stillbirth 573.4.2 Premature labor 58
3.4.2.1 Pre-pregnancy BMI and pregnancy weight gain 583.4.2.2 Alcohol and caffeine consumption 593.4.2.3 Oral health 60
3.4.3 Hypertensive disorders of pregnancy 603.4.3.1 The etiology of PE 603.4.3.2 Nutrition-related factors and PE 62
3.4.4 Abnormal labor 623.5 Nausea and vomiting of pregnancy (NVP) 63
3.5.1 NVP as a normal physiological process 633.5.2 Hyperemesis gravidarum 65
3.6 Cravings and aversions 663.6.1 Pica 66
3.7 Gastrointestinal disturbances in pregnancy 673.8 High-risk pregnancies 68
3.8.1 Gestational diabetes 683.8.2 Multiple pregnancies 693.8.3 Fetal alcohol spectrum disorders 71

BLBK170-Langley April 6, 2009 14:54
Contents v
4. Fetal Nutrition and Disease in Later Life 754.1 Introduction 754.2 The developmental origins of adult disease 75
4.2.1 The concept of programming 754.2.2 Fetal programming and human disease 76
4.3 Evidence linking maternal nutrition to disease in later life 794.3.1 Epidemiology 794.3.2 Criticisms of the programming hypothesis 814.3.3 Experimental studies 82
4.3.3.1 Global undernutrition 834.3.3.2 Micronutrients 834.3.3.3 Macronutrients 83
4.4 Mechanistic basis of fetal programming 854.4.1 Thrifty phenotypes and genotypes 854.4.2 Predictive adaptive responses 874.4.3 Tissue remodeling 874.4.4 Endocrine imbalance 894.4.5 Nutrient–gene interactions 904.4.6 Epigenetic regulation 92
4.5 Implications of the programming hypothesis 934.5.1 Public health interventions 934.5.2 Trans-generational transmission of disease risk 93
5. Lactation and Infant Feeding 995.1 Introduction 995.2 The physiology of lactation 99
5.2.1 Anatomy of the breast 995.2.1.1 The nipple and areola 995.2.1.2 The lactiferous ducts 995.2.1.3 The lactiferous sinuses 995.2.1.4 The alveolar cells 1005.2.1.5 The rooting reflex 100
5.2.2 Synthesis of milk 1015.2.2.1 Foremilk and hindmilk 1015.2.2.2 Time of day 1015.2.2.3 Course of lactation 1025.2.2.4 Synthesis of carbohydrates 1025.2.2.5 Origins of milk fats 1025.2.2.6 Milk proteins 103
5.2.3 Endocrine control of lactation 1045.2.3.1 The breast during pregnancy 1045.2.3.2 Established lactation 1045.2.3.3 The breast after weaning 105
5.2.4 Maintenance of lactation 1055.2.5 Nutritional demands of lactation 106
5.3 The advantages of breast-feeding 1075.3.1 Advantages for the mother 1075.3.2 Advantages for the infant 1095.3.3 Recommendation to feed to 6 months 112

BLBK170-Langley April 6, 2009 14:54
vi Contents
5.4 Trends in breast-feeding behavior 1125.4.1 Reasons why women do not breast-feed 1145.4.2 Promoting breast-feeding 115
5.5 Situations in which breast-feeding is not advised 1175.6 Alternatives to breast-feeding 118
5.6.1 Cow’s milk formulas 1185.6.1.1 Milk stages and follow-on milk 119
5.6.2 Preterm formulas 1205.6.3 Soy formulas 1215.6.4 Hydrolyzed protein and amino-acid-based formulas 1215.6.5 Other formulas 121
6. Nutrition and Childhood 1246.1 Introduction 1246.2 Infancy (birth to five) 124
6.2.1 The key developmental milestones 1246.2.2 Nutrient requirements 126
6.2.2.1 Macronutrients and energy 1266.2.2.2 Micronutrients 128
6.2.3 Nutrient intakes and infants 1296.2.4 Transition to an adult pattern of food intake 129
6.2.4.1 Weaning 1306.2.4.2 Nutrition-related problems 1326.2.4.3 Barriers to healthy nutrition 134
6.3 Childhood (five to thirteen) 1396.3.1 Nutrient requirements of the older child 1396.3.2 School meals and the promotion of healthy eating 1396.3.3 The importance of breakfast 140
6.4 Obesity in children 1416.4.1 The rising prevalence of obesity 1416.4.2 The causes of obesity in childhood 142
6.4.2.1 Physical activity 1436.4.2.2 Food intake 1436.4.2.3 Genetic disorders 146
6.4.3 The consequences of childhood obesity 1476.4.3.1 Immediate health consequences 1486.4.3.2 Tracking of obesity: consequences for the future 148
6.4.4 Treatment of childhood obesity 1506.4.5 Prevention of childhood obesity 152
7. Nutrition and Adolescence 1587.1 Introduction 1587.2 Physical development 158
7.2.1 Growth rate 1587.2.2 Body composition 1597.2.3 Puberty and sexual maturation 1597.2.4 Bone growth 163
7.3 Psychosocial development 165

BLBK170-Langley April 6, 2009 14:54
Contents vii
7.4 Nutritional requirements in adolescence 1667.4.1 Macronutrients and energy 1667.4.2 Micronutrients 167
7.5 Nutritional intakes in adolescence 1687.5.1 Factors that influence food choice 1697.5.2 Food consumed out of the home 1707.5.3 Meal skipping and snacking 171
7.6 Potential problems with nutrition 1727.6.1 Dieting and weight control 1727.6.2 The vegetarian teenager 1727.6.3 Sport and physical activity 1737.6.4 Eating disorders 174
7.6.4.1 Anorexia nervosa 1747.6.4.2 Bulimia nervosa 176
7.6.5 The pregnant teenager 1767.6.6 Alcohol 1787.6.7 Tobacco smoking 1807.6.8 Drug abuse 181
8. The Adult Years 1858.1 Introduction 1858.2 Changing needs for nutrients 1858.3 Guidelines for healthy nutrition 1868.4 Disease states associated with unhealthy nutrition and lifestyle 189
8.4.1 Obesity 1898.4.1.1 Classification of overweight and obesity 1898.4.1.2 Prevalence and trends in obesity 1898.4.1.3 Causes of obesity in adulthood 1908.4.1.4 Treatment of obesity 191
8.4.2 Type 2 diabetes 1928.4.3 The metabolic syndrome 1958.4.4 Cardiovascular disease 196
8.4.4.1 What is cardiovascular disease? 1968.4.4.2 Risk factors for cardiovascular disease 1998.4.4.3 Nutrition-related factors and risk of cardiovascular disease 199
8.4.5 Cancer 2078.4.5.1 What is cancer? 2078.4.5.2 Diet is the main determinant of cancer risk 2088.4.5.3 Nutritional epidemiology and cancer 2098.4.5.4 Dietary factors that may promote cancer 2138.4.5.5 Dietary factors that may reduce cancer risk 217
9. Nutrition, Aging, and the Elderly 2279.1 Introduction 2279.2 The aging population 2279.3 The aging process 228
9.3.1 Impact on physiological systems 2289.3.2 Mechanisms of cellular senescence 228

BLBK170-Langley April 6, 2009 14:54
viii Contents
9.3.2.1 Oxidative senescence 2309.3.2.2 The role of p53 activation 2319.3.2.3 Telomere shortening 2319.3.2.4 The INK4a/ARF axis 231
9.3.3 Nutritional modulation of the aging process 2329.3.3.1 Caloric restriction and lifespan 2329.3.3.2 Fetal programming of lifespan 2339.3.3.3 Supplementary antioxidants 233
9.4 Nutrient requirements of the elderly 2349.4.1 Macronutrients and energy 2349.4.2 Micronutrients 2349.4.3 Specific guidelines for the elderly 234
9.5 Barriers to healthy nutrition in the elderly 2359.5.1 Malnutrition and the elderly 2359.5.2 Poverty 2369.5.3 Social isolation 2379.5.4 Education 2379.5.5 Physical changes 2389.5.6 Combating malnutrition in the elderly 238
9.6 Common nutrition-related health problems 2399.6.1 Bone disorders 239
9.6.1.1 Bone mineralization and remodeling 2399.6.1.2 Osteoporosis pathology and prevalence 2419.6.1.3 Risk factors for osteoporosis 2419.6.1.4 Dietary interventions for osteoporosis prevention 2429.6.1.5 Paget’s disease of bone 244
9.6.2 Immunity and infection 2449.6.3 Digestive tract disorders 245
9.6.3.1 Mouth and esophagus 2459.6.3.2 Stomach 2469.6.3.3 Small intestine 2469.6.3.4 Large intestine 246
9.6.4 Anemia 2479.6.4.1 Iron deficiency anemia 2489.6.4.2 Vitamin B12 deficiency 2489.6.4.3 Folic acid deficiency 2499.6.4.4 Cognitive impairment and anemia 249
10. Personalized Nutrition 25410.1 Introduction 25410.2 The individual response to variation in food intake 255
10.2.1 Genes may determine food intake 25610.2.1.1 Regulation of food intake 25710.2.1.2 Regulation of macronutrient intake 25710.2.1.3 Regulation of taste 257
10.2.2 Genes may determine nutrient bioavailability and utilization 25810.2.3 Nutritional regulation of gene expression 258

BLBK170-Langley April 6, 2009 14:54
Contents ix
10.3 Identifying disease risk biomarkers 26010.3.1 Nutrigenomics 26010.3.2 Proteomics 26110.3.3 Metabolomics 263
10.4 Genetic influences on response to nutrients and disease risk 26310.4.1 Obesity 26310.4.2 Cardiovascular disease 26410.4.3 Cancer 265
10.5 Nutrient–gene interactions—a lifespan approach 26610.6 The future of nutritional advice? 268
Glossary of Terms 271
Index 291
Additional resources are published on the book’s web site(www.wiley.com/go/langleyevans)

BLBK170-Langley April 6, 2009 14:54
x

BLBK170-Langley April 6, 2009 14:54
Preface
The modern science of nutrition has arisen from hum-ble beginnings, moving from a poorly respected side-shoot of many older established disciplines to becomean active entity in its own right. Nutrition is nowrightly seen as being at the forefront of modern un-derstanding of health and disease. Many of the aca-demics in the field have come to nutrition tangentiallythrough many disparate routes, usually becoming im-mersed in the subject through research interests basedin other fields. My own background was in biochem-istry and microbiology, and my early interest in nutri-tion came from tantalizing, but sadly vague, mentionsin textbooks that suggested that key processes such asthe development of cancers might be, “regulated bynutrition”.
The lack of specific nutrition training of the cur-rent crop of academics in the field reflects the fact that20–30 years ago there were no degree courses in thesubject. Interest in nutrition has increased exponen-tially since the early 1990s and it is pleasing to see thatdegrees in nutrition have blossomed across all regions.In the UK alone, a prospective undergraduate consid-ering training in nutrition will be faced with a choiceof over 250 university courses with a nutrition com-ponent. Nutrition is also recognised as a key elementin the training of all health professionals. But whatis nutrition? In my view it is a hybrid subject whichcrosses over disciplines as disparate as politics and eco-nomics (which are the global drivers determining thefood security of populations), food science and agri-culture, the social sciences, psychology and sociology(which govern eating behaviors and food choices ofindividuals), biochemistry, physiology, medicine, andpharmacology. This book aims to provide a basic text
for undergraduate students in all disciplines that im-pinge upon the nutritional sciences, including thosetraining as health professionals as well as those read-ing nutrition as their core subject. It covers nutritionfrom a range of perspectives including those of thephysiologist, the molecular biologist and the publichealth nutritionist. I have assumed that the readerwill have an understanding of the basics of the sub-ject, namely, the properties and sources of nutrient,and have focused my attention upon how nutrition-related factors shape human health and disease acrossall stages of the life-course.
One of the main challenges for the modern nutri-tionist is to translate complex scientific concepts intosimple advice about food and health that can be un-derstood by the lay public. The conditional nature ofthe subject, namely, the way in which our understand-ing advances and throws up controversies and contra-dictions, is a constant theme running through thisbook. For each chapter I have attempted to providea balanced view of the evidence base, but inevitablythe chapters will reflect my own personal view of thesubject matter. The reader is directed to the extensivebibliographies that accompany each chapter to ob-tain a more detailed perspective. My profound wishis that students who use this book will emerge withsignificantly more understanding of how nutritionregulates metabolism and contributes to health anddisease, than I did from those tantalizing sentences Iencountered in my own training.
Simon Langley-EvansUniversity of Nottingham
xi

BLBK170-Langley April 6, 2009 14:54
Acknowledgments
The writing of this textbook has been a massive un-dertaking for me and during that time, a numberof colleagues have provided comments, support andencouragement for which I am extremely grateful. Iwould particularly like to thank Professor Andy Salterand Dr Sarah McMullen at the University of Notting-
ham, for their understanding during the times whenwriting has displaced other calls on my time. Specialthanks go to my family, Alison, Effie, Hugh and Hebe,for their immense patience and vital inputs to theprocess.
xii

BLBK170-Langley April 6, 2009 14:56
1Introduction to Lifespan Nutrition
Learning objectives
By the end of this chapter, the reader should be able to:
� Describe what is meant by a lifespan approach to thestudy of nutrition and health.
� Discuss the meaning of the term “nutritional status”and describe how optimal nutrition requires a balanceof nutrient supply and demand for nutrients in physio-logical and metabolic processes.
� Show an awareness of the factors that contribute toundernutrition, including limited food supply and in-creased demands due to trauma or chronic illness.
� Discuss global strategies for the prevention of malnu-trition.
� Describe how nutritional status is influenced by thestage of life due to the variation in specific factorscontrolling nutrient availability and requirements, asindividuals develop from the fetal stage through toadulthood.
� Show an appreciation of how anthropometry, dietaryassessment, measurements of biomarkers, and clinicalexamination can be used to study nutritional status inindividuals and populations.
� Discuss the need for dietary standards in making as-sessments of the quality of diet or dietary provision, inindividuals or populations.
� Describe the variation in the basis and usage of dietaryreference value systems in different countries.
1.1 The lifespan approach to nutrition
The principal aim of this book is to explore re-lationships between nutrition and health, and thecontribution of nutrition-related factors to disease.In tackling this subject, there are many differentapproaches that could be taken, for example, consid-ering diet and cardiovascular disease, nutrition anddiabetes, obesity or immune function as separate anddiscrete entities, each worthy of their own chapter.The view of this author, along with many others inrecent times (Ben-Shlomo and Kuh, 2002) is thatthe final stages of life, that is, the elderly years, areeffectively the products of events that occur throughthe full lifespan of an individual. Aging is in actualitya continual, lifelong process of ongoing change anddevelopment from the moment of conception untilthe point of death. It is therefore inappropriate toconsider how diet relates to chronic diseases thataffect adults without allowance for how the earlierlife experiences have shaped physiology. The lifespanapproach that is used to organize the material in thisbook essentially asserts three main points:
1 All stages of life from the moment of conceptionthrough to the elderly years are associated with aseries of specific requirements for nutrition.
2 The consequences of less than optimal nutrition ateach stage of life will vary, according to the life stageaffected.
3 The nature of nutrition-related factors at earlierstages of life will determine how individuals growand develop. As a result, the relationship betweendiet and health in later stages of adult life, to someextent, depends upon events earlier in life. As aresult the nature of this relationship may be highlyindividual.
Although we tend to divide the lifespan into a seriesof distinct stages, such as infancy, adolescence, earlyadulthood, middle age, and older adulthood, few ofthese divisions have any real biological significanceand they are therefore simply markers of particularperiods within a continuum. There are, however, keyevents within these life stages, such as weaning, theachievement of puberty, or the menopause, which aresignificant milestones that mark profound physiolog-ical and endocrine changes and have implications for
1

BLBK170-Langley April 6, 2009 14:56
2 Nutrition: A Lifespan Approach
the nature of the nutrition and health relationship.On a continual basis, at each stage of life, individualsexperience a series of biological challenges, such asinfection or exposure to carcinogens that threaten todisturb normal physiology and compromise health.Within a lifespan approach, it is implicit that theresponse of the system to each challenge will influ-ence how the body responds at later life stages. Vari-ation in the quality and quantity of nutrition is oneof the major challenges to the maintenance of op-timal physiological function and is also one of themain determinants of how the body responds to otherinsults.
In considering the contribution of nutrition-relatedfactors to health and disease across the lifespan, it isnecessary to evaluate the full range of influences uponquality and quantity of nutrition and upon physio-logical processes. This book therefore takes a broadapproach and includes consideration of social or cul-tural influences on nutrition and health, the metabolicand biochemical basis of the diet–disease relation-ships, the influence of genetics, and, where necessary,provides overviews of the main physiological and cel-lular processes that operate at each life stage. Whilethe arbitrary distinctions of childhood, adolescence,and adulthood have been used to divide the chapters,it is hoped that the reader will consider this work as awhole. In this opening chapter, we consider some ofthe basic terms and definitions used in nutrition andlay the foundations for understanding more complexmaterial in the following chapters.
1.2 The concept of balance
Balance is a term frequently used in nutrition and, un-fortunately, the precise meaning of the term may differaccording to the context and the individual using it. Itis common to hear the phrase “a balanced diet” and,indeed, most health education literature that goes outto the general public urges the consumption of a dietthat is “balanced.” In this context, we refer to a dietthat provides neither too much nor too little of thenutrients and other components of food that are re-quired for normal functioning of the body. A balanceddiet may also be viewed as a diet providing foods of avaried nature, in proportions such that foods rich insome nutrients do not limit intakes of foods rich inothers.
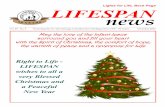
1.2.1 A supply and demand modelThere is another way of viewing the meaning ofbalance or a balanced diet, whereby the relationshipbetween nutrient intake and function is the main con-sideration. A diet that is in balance is one where thesupply of nutrients is equal to the requirement of thebody for those nutrients. Essentially, balance could beviewed as equivalent to an economic market, in whichsupply of goods or services needs to be sufficient tomeet demands for those goods or services. Figure 1.1summarizes the supply and demand model of nutri-tional balance.
Whether or not the diet is in balance will be a keydeterminant of the nutritional status of an individ-ual. Nutritional status describes the state of a person’shealth in relation to the nutrients in their diet and sub-sequently within their body. Good nutritional statuswould generally be associated with a dietary patternthat supplies nutrients at a level sufficient to meetrequirements, without excessive storage. Poor nutri-tional status would generally (though not always) beassociated with intakes that are insufficient to meetrequirements.
The supply and demand model provides a usefulframework for thinking about the relationship be-tween diet and health. As shown in Figure 1.1, main-taining balance with respect to any given nutrient re-quires the supply of the nutrient to be equivalent to theoverall demand for that nutrient. Demand comprisesany physiological or metabolic process that utilizes thenutrient and may include use as an energy-releasingsubstrate, as an enzyme cofactor, as a structural com-ponent of tissues, a substrate for synthesis of macro-molecules, as a transport element, or as a compo-nent of cell–cell signaling apparatus. The supply sideof the balance model comprises any means throughwhich nutrients are made available to meet demand.This goes beyond delivery through food intake andincludes stores of the nutrient that can be mobilizedwithin the body, and quantities of the nutrient thatmight be synthesized de novo (e.g., vitamin D is syn-thesized in the skin through the action of sunlight).
1.2.2 OvernutritionWhen supply does not match demand for a nutrient,then the system is out of balance and this may haveimportant consequences in terms of health and dis-ease. Overnutrition (Figure 1.1) will generally arise

BLBK170-Langley April 6, 2009 14:56
Introduction to Lifespan Nutrition 3
SupplyIntake, stores
DemandMetabolic,
physiologicalactivity
Balance
SupplyIntake, stores
DemandMetabolic,
physiologicalactivity
SupplyIntake, stores
DemandMetabolic,
physiologicalactivity
Overnutrition
Undernutrition
Figure 1.1 The concept of balance. The demands for nutrientscomprise metabolic and physiological processes that utilize nu-trients. Supply is determined by intakes of food, availability ofnutrient stores, and de novo production of nutrients.
because the supply of a nutrient is excessive relative todemand. This is either because intake of foods con-taining that nutrient increases, because the individualconsumes supplements of that nutrient, or becausedemand for that nutrient declines with no equiva-lent adjustment occurring within the diet. The latterscenario particularly applies to the elderly, for whomenergy requirements fall due to declining physical ac-tivity levels and resting metabolic rate (Rivlin, 2007).Commonly, intakes of energy that were appropriatein earlier adulthood will be maintained, resulting inexcessive energy intake.
The consequences of overnutrition are generallynot widely considered in the context of health anddisease, unless the nutrient concerned is directly toxicor harmful when stored in high quantities. The obvi-ous example here is, again, energy, where overnutri-tion will result in fat storage and obesity. For manynutrients, overnutrition within reasonable limits hasno adverse effect as the excess material will either bestored or excreted. At megadoses, however, most nu-
trients have some capacity to cause harm. Accidentalconsumption of iron supplements or iron overloadassociated with inherited disorders is a cause of dis-ease and death in children. At high doses, iron willimpair oxidative phosphorylation and mitochondrialfunction, leading to cellular damage in the liver, heart,lungs, and kidneys. Excess consumption of vitamin Ahas been linked to development of birth defects in theunborn fetus (Martinez-Frias and Salvador, 1990).
Overnutrition for one nutrient can also have ef-fects upon nutritional status with respect to othernutrients, and can impact on physiological processesinvolving a broader range of nutrients. For example,regular consumption of iron supplements can im-pact upon absorption of other metals such as zincand copper, by competing for gastrointestinal trans-porters and hence promote undernutrition with re-spect to those trace elements. Having an excess of aparticular nutrient within the body can also promoteundernutrition with respect to another by increasingthe demand associated with processing the excess. For

BLBK170-Langley April 6, 2009 14:56
4 Nutrition: A Lifespan Approach
example, a diet rich in the amino acid methionine willtend to increase circulating and tissue concentrationsof homocysteine. Processing of this damaging inter-mediate increases the demand for B vitamins, folicacid, vitamin B6, and vitamin B12, which are all in-volved in pathways that convert homocysteine to lessharmful forms (Lonn et al., 2006).
1.2.3 UndernutritionUndernutrition arises when the supply of nutrient failsto meet demand. This can occur if intakes are poor,or if demands are increased (Figure 1.1). In the short–medium term, low intakes are generally cushioned bythe fact that the body has reserves of all nutrients thatcan be mobilized to meet demand. As such, for adults,it will usually require prolonged periods of low intaketo have a significantly detrimental effect on nutritionalstatus.
1.2.3.1 Increased demandThere are a number of situations that may arise to in-crease demand in such a way that undernutrition willarise if supply is not also increased accordingly. Theseinclude pregnancy, lactation, and trauma. Trauma en-compasses a wide range of physical insults to the body,including infection, bone fracture, burns, surgery,and blood loss. Although diverse in nature, all ofthese physiological insults lead to the same metabolicresponse. This acute phase response (Table 1.1) islargely orchestrated by the cytokines including tumornecrosis factor-α, interleukin-6, and interleukin-1(Grimble, 2001). Their net effect is to increase de-mand for protein and energy and yet paradoxically
they have an anorectic effect. Thus, demand increasesand supply will be impaired leading to protein–energymalnutrition. While in many developing countries,we associate protein–energy malnutrition with star-vation in children, in developed countries such asthe UK protein–energy malnutrition is most com-monly noted in surgical patients and patients recov-ering from major injuries (Allison, 2005).
1.2.3.2 The metabolic response to traumaThe human body is able to adapt rates of metabolismand the nature of metabolic processes to ensuresurvival in response to adverse circumstances. Themetabolic response to adverse challenges will dependupon the nature of the challenge. Starvation leads toincreased metabolic efficiency, which allows reservesof fat and protein to be utilized at a controlled ratethat prolongs survival time and hence maximizes thechances of the starved individual regaining access tofood. In contrast, the physiological response to traumagenerates a hypermetabolic state in which reserves offat and protein are rapidly mobilized in order to fendoff infection and promote tissue repair (Table 1.1).Physiological stresses to the body, including infection,bone fracture, burns, or other tissue injury, elicit acommon metabolic response regardless of their na-ture. Thus, a minor surgical procedure will producethe same pattern of metabolic response as a viral in-fection. It is the magnitude of the response that isvariable and this is largely determined by the severityof the trauma (Romijn, 2000).
The hypermetabolic response to trauma is drivenby endocrine changes that promote the catabolism of
Table 1.1 The acute phase inflammatory response to trauma or infection
Acute phase response Markers of the response
Metabolic change Catabolism of protein, muscle wastage. Amino acids converted to glucose for energy, or used tosynthesize acute phase proteins. Catabolism of fat for energy
Fever Body temperature rises to kill pathogens. Hypothalamic regulation of food intake disrupted, leading toloss of appetite
Hepatic protein synthesis Acute phase proteins synthesized to combat infection (e.g., C-reactive protein, α1-proteinase inhibitor,and ceruloplasmin). Liver reduces synthesis of other proteins, including transferrin and albumin
Sequestration of trace elements Zinc and iron taken up by tissues to remove free elements that may be utilized by pathogens
Immune cell activation B cells produce increased amounts of immunoglobulins. T cells release cytokines to orchestrate theinflammatory response
Cytokine production Tumor necrosis factor-α and the interleukins 1, 2, 6, 8, and 10 work to produce a hypermetabolic state thatfavors production of substrates for immune function, but inhibits reproduction and spread of pathogens

BLBK170-Langley April 6, 2009 14:56
Introduction to Lifespan Nutrition 5
protein and fat reserves. Following the initial phys-iological insult, there is an increase in circulatingconcentrations of the catecholamines, cortisol, andglucagon. Increased cortisol and glucagon serve tostimulate rates of gluconeogenesis and hepatic glu-cose output, thereby maintaining high concentrationsof plasma glucose. The breakdown of protein to aminoacids provides gluconeogenic substrates and also leadsto greatly increased losses of nitrogen via the urine.Lipolysis is stimulated and circulating free fatty acidconcentrations rise dramatically. These are used asenergy substrates, along with glucose.
The response to trauma is essentially an inflamma-tory process and, as such, the same metabolic drivesare noted in individuals suffering from long-term in-flammatory diseases including cancer and inflamma-tory bowel disease (Richardson and Davidson, 2003).The inflammatory response serves two basic func-tions. Firstly, it activates the immune system, raisesbody temperature, and repartitions micronutrients inorder to create a hostile environment for invadingpathogens (Table 1.1). Secondly, it allocates nutrientstoward processes that will contribute to repair andhealing.
The inflammatory response is orchestrated bythe pro-inflammatory cytokines (e.g., TNF-α, IL-1,and IL-6) and the anti-inflammatory cytokines (e.g.,IL-10). Whenever injury or infection occurs, thepro-inflammatory species are released by monocytes,macrophages, and T helper cells. The level of cytokinesproduced is closely related to the severity of the trauma(Lenz et al., 2007). The impact of pro-inflammatorycytokines is complex. On the one hand, they acti-vate the immune system and protect the body fromgreater trauma. On the other, at the local level ofany injury, they increase damage by stimulating theimmune system to release damaging oxidants and
other agents that indiscriminately destroy invadingpathogens and the body’s own cells. The productionof pro-inflammatory cytokines therefore has to becounterbalanced as an excessive response can lead todeath (Grimble, 2001). This is the role of the anti-inflammatory cytokines and some of the acute phaseresponse proteins, several of which inhibit the pro-teinases released during inflammation and thereforelimit the breakdown of host tissues.
In addition to stimulating proteolysis and lipoly-sis within muscle and adipose tissue, the cytokineshave a number of actions that impact upon nutri-tional status. Firstly, they increase the basal metabolicrate. An element of creating a hostile environment forpathogens includes raising the core temperature of thebody (fever). This greatly increases energy demands.The capacity to meet those demands through feedingis reduced as cytokines also act upon the gut and thecenters of the hypothalamus that regulate appetite,effectively switching off the desire to eat. As can beseen in Table 1.2, the increased metabolic rate asso-ciated with the response to trauma greatly increasesthe demands of the body for both energy and pro-tein. In severe cases, requirements can be doubled,even though the critically ill patient will be immo-bilized and not expending energy through physicalactivity. This can pose major challenges for cliniciansmanaging such cases as the injured patient maybeunable to feed normally, and due to the anorectic in-fluences of pro-inflammatory cytokines, the capacityto ingest sufficient energy, protein, and other nutri-ents is greatly reduced. Enteral or parenteral feedingare therefore a mainstay of managing major injuries.
With more severe trauma, the mobilization of re-serves can produce marked changes in body com-position. Muscle wasting may occur as the calcium-dependent calpains and ubiquitine-proteasome break
Table 1.2 The metabolic response to injury and infection increases requirements for energy and protein
Nature and severity of trauma Increase in energy requirement (× basal) Increase in protein requirement (× basal)
Minor surgery or infection 1.1 1.0–1.5Major surgery or moderate infection 1.3–1.4 1.5–2.3Severe infection, multiple or head injuries 1.8 2.0–2.8Burns (20% BSAB) 1.5 –Burns (20–40% BSAB) 1.8 2.0–2.8a
BSAB, body surface area burned.a Dependent upon level of nitrogen losses in tissue exudates and age of patient. Children with burns have higher require-ments.

BLBK170-Langley April 6, 2009 14:56
6 Nutrition: A Lifespan Approach
down proteins rapidly to make amino acids avail-able for gluconeogenesis and the synthesis of im-portant antioxidants such as glutathione (Grimble,2001). Body composition changes are beneficial tothe injured patient as they primarily generate glucose.This is the optimal energy substrate for these circum-stances, not least because it can be metabolized anaer-obically to produce ATP in tissues where blood flowmay be compromised and oxygen delivery impaired.
In the short term, the hypermetabolic response andthe accompanying anorexia of illness are unlikely toimpact significantly upon the nutritional status of anindividual, although nutritional status prior to onsetof trauma would be an important consideration. Forexample, the nutritional consequences of a fracturedfemur in a young, fit adult male may be dramaticallydifferent to those in a frail elderly woman. Prolongedperiods of disease accompanied by inflammatory re-sponses that drive hypermetabolism will, however,promote states of protein–energy malnutrition, suchas kwashiorkor, or can produce the emaciated state ofcachexia. Cachexia is characterized by loss of weight,decline in appetite, and muscle atrophy due to mo-bilization of muscle protein. It is generally associatedwith underlying chronic illnesses such as cancer, tu-berculosis, or untreated AIDS. Nutritional support(i.e., supplemental feeding) of chronically ill individ-uals or those who have suffered more acute traumacan limit the impact of the hypermetabolic responseupon body composition and overall nutritional status.
However, the catabolic metabolism cannot be reverseduntil the injury or illness is resolved, so the priorityin these scenarios is limiting weight loss and loss ofmuscle mass, rather than achieving weight gain.
1.2.3.3 Compromised supply and deficiencyClearly, there is a direct relationship between the sup-ply of a nutrient to the body and the capacity of thebody to carry out the physiological functions that de-pend upon the supply of that nutrient. As can be seenin Figure 1.2, the range of nutrient intakes over whichoptimal function is maintained is likely to be verybroad and there are a number of stages before func-tionality is lost. It is only when function can no longerbe maintained that the term nutritional deficiency canbe accurately used.
A nutrient deficiency arises when the supply of anutrient through food intake is compromised to theextent that clinical or metabolic symptoms appear.The simplest example to think of here relates to irondeficiency anemia in which low intakes of iron resultin a failure to maintain effective concentrations ofred blood cell hemoglobin, leading to compromisedoxygen transport and hence the clinical symptoms ofdeficiency that include fatigue, irritability, dizziness,weakness, and shortness of breath. Iron deficiencyanemia, like all deficiency disorders, reflects only thelate stage of the process that begins with a failure ofsupply through intake to meet demands (Table 1.3).Once the body can no longer maintain function using
Low risk of disease. Demands met
Danger of diseasedue to excess
Danger of deficiency disease
Incr
easi
ng n
utrie
nt in
take
Marginally high intake
Marginally low intakeFigure 1.2 The association between nutrition and health.The requirements of the body for nutrients will be met by abroad range of intakes. Very low and very high intakes ofany nutrient will be associated with ill health. The transitionfrom intakes that are meeting demands and at which riskof disease is low to intakes that would be associated withdisease is not abrupt.

BLBK170-Langley April 6, 2009 14:56
Introduction to Lifespan Nutrition 7
Table 1.3 The three stages of iron deficiency
Stage Biochemical indicators and reference ranges
Normal iron status Hemoglobin 14–18 g/dL (men), 12–16 g/dL (women). Serum ferritin 40–280 µg/L, transferrin saturation 31–60%
Depleted iron stores Falling serum ferritin. Normal ranges for hemoglobin and transferrin saturation. Ferritin 13–20 µg/L
Iron deficiency Transferrin saturation falls as transport of iron declines. Hemoglobin normal. Serum ferritin <12 µg/L. Transferrinsaturation <16%
Iron deficiency anemia Hemoglobin synthesis cannot be maintained and declines to <13.5 g/dL (men), <12 g/dL (women). Serum ferritin<10 µg/L. Transferrin saturation <15%
nutrient supply directly from the diet, it will mobilizestores. In the case of iron, this will involve the releaseof iron bound to the protein, ferritin, to maintainhemoglobin concentrations. No change in functionwill occur at this stage but the individual will nowbe in a state of greater vulnerability to deficiency. Afurther decline in supply through intake may not bematched through mobilization of stores and so full de-ficiency becomes more likely. This situation in whichintakes are sufficiently low that, although there areno signs of deficiency, biochemical indicators showthat nutrition is subnormal is generally referred to asmarginal nutrition, or subclinical malnutrition.
1.2.3.4 MalnutritionMalnutrition describes the state where the level of nu-trient supply has declined to the point of deficiencyand normal physiological functions can no longer bemaintained. The manifestations of malnutrition willvary depending on the type of nutrient deficienciesinvolved and the stage of life of the malnourished in-dividual. In adults, malnutrition is often observed asunintentional weight loss or as clinical signs of spe-cific deficiency. In children, it is more likely to manifestas growth faltering, with the affected child being ei-ther underweight for their age (termed wasted) or ofshort stature for their age (termed stunted). Specificpatterns of growth are indicative of different formsof protein–energy malnutrition. Wasting is associ-ated with marasmus where a weight less than 60%of standard for age is used as a cutoff. Edema with aweight less than 80% of standard for age is indicativeof kwashiorkor.
From a clinical perspective, protein–energy mal-nutrition is the most serious undernutrition-relatedsyndrome. Marasmus and kwashiorkor are classicaldefinitions of this form of malnutrition. Historically,marasmus was considered to be a pure energy defi-
ciency and kwashiorkor to be protein deficiency, butit is now clear that the two are different manifestationsof the same nutritional problems. Marasmic wastingis a sign of an effective physiological adaptation tolong-term undernutrition. It is characterized by a de-pletion of fat reserves and muscle protein, along withadaptations to reduce energy expenditure. Childrenwho become wasted in this way, if untreated, will gen-erally die from infection as their immune functionscannot be maintained during the period of starvation.Kwashiorkor is a more rapid process, often triggeredby infection alongside malnutrition. The metabolicchanges with kwashiorkor are strikingly different tomarasmus as the adaptation to starvation is ineffec-tive. Fat accumulates in the liver and expansion ofextracellular fluid volume, driven by low serum al-bumin concentrations, leads to edema. Micronutri-ent deficiencies often occur alongside protein–energymalnutrition and may partly explain why individualswith kwashiorkor, unlike those with marasmus, areunable to adapt successfully to malnutrition.
The causes of malnutrition are complex and are notsimply related to a limited food intake. Where intakeis reduced, this is often due to food insecurity asso-ciated with famine, poverty, war, or natural disasters.Reduced food intake can also arise due to chronic ill-ness leading to loss of appetite or feeding difficulties.Malnutrition will also arise from malabsorption of nu-trients from the digestive tract. This, again, could be aconsequence of chronic disease or be driven by infec-tion of the tract. Losses of nutrients are an importantconsequence of repeated diarrheal infections in areaswhere there is no access to clean water and adequatesanitation. Malnutrition may also be driven by situa-tions that increase the demand for nutrients includingtrauma (as described above), pregnancy, and lacta-tion, if those increased demands cannot be matchedby intake.

BLBK170-Langley April 6, 2009 14:56
8 Nutrition: A Lifespan Approach
Malnutrition is most common and most deadly inthe developing countries, where it is the major causeof death in children. Stunting and wasting amongmalnourished children have long-term consequencestoo, as often the reduction in stature is not recovered,leading to reduced physical strength and capacity towork in adult life. As poverty is the most frequentcause of malnutrition, a self-perpetuating cycle canbe established, as the stunted child becomes the adultwith reduced earning capacity, whose children willlive in poverty. Stunted, underweight women will alsohave children who are at risk due to lower weight atbirth. Pregnancy is a time of high risk for malnutritionin women living in developing countries. Stunting iscommonplace among women in South and South-east Asia, and is often accompanied by underweight.For example, in India and Bangladesh, up to 40% ofwomen of childbearing age have a body mass index(BMI) of less than 18.5 kg/m2 (Black et al., 2008). Irondeficiency anemia is endemic among pregnant womenin developing countries, with prevalence of between60% and 87% in the countries of southern Asia(Seshadri, 2001). Maternal and childhood malnutri-tion are believed to cause 3.5 million deaths amongthe under-fives every year (Black et al., 2008).
Developed countries also have a burden of malnu-trition among vulnerable groups. At greatest risk arethe elderly, who may develop protein–energy malnu-trition or micronutrient deficiencies due to specificmedical conditions, or through low intakes associ-ated with frailty or loneliness. Surgical patients are atrisk of protein–energy malnutrition as a result of theinflammatory response to trauma. As in the develop-ing countries, poverty increases the risk of malnutri-tion among children and immigrant groups. There aremany ways of targeting these at-risk groups, for ex-ample, monitoring the growth of infants, or includingregular weighing and nutritional assessments of hos-pital patients. Malnutrition is easily treated throughappropriate nutritional support.
The prevention of malnutrition is a major publichealth priority on a global scale. While a lack of foodsecurity and the risk of protein–energy malnutritionremains a major issue for many populations, therehave been a number of success stories in the battle toprevent clinically significant malnutrition. The basicapproaches that can be used to prevent nutrient defi-ciency are diet diversification, supplementation of at-risk individuals, and fortification. The basis for theseapproaches and their use in the attempt to eradicate
vitamin A deficiency is described in Research high-light 1. Similar strategies have been used to reduce theoccurrence of iodine and iron deficiency diseases.
Iodine deficiency is an important issue for pop-ulations in all continents except Australasia. Avail-ability of iodine is essentially limited by the iodinecontent of the soil and hence uptake by plants and an-imals. Iodine deficiency disorders, including cretinismand goiter, are a major manifestation of malnutrition,with approximately 740 million affected individualsworldwide. Fortification has been the cornerstone ofthe fight against iodine deficiency, with the UniversalSalt Iodization program providing iodized salt (20–40 mg iodine per kg salt) to 70% of households inaffected areas. Where the iodized salt is consumed,marked improvements in iodine status of the popula-tion are rapidly noted (Sebotsa et al., 2005). Althoughthere are still significant numbers of individuals atrisk of iodine deficiency disorders, due to lack of cov-erage of the USI program (Maberly et al., 2003), thisfortification approach is widely considered to be apublic health nutrition success for the World HealthOrganization (WHO).
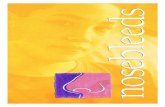
1.2.4 Classical balance studiesNutritional status with respect to a specific nutrientcan be measured using balance studies. These haveclassically been used to determine requirements forsome nutrients in humans. Essentially, the balancemethod involves the accurate measurement of nutri-ent intake, for comparison with accurate measuresof all possible outputs of that nutrient via the urine,feces, and other potential routes of loss (Figure 1.3). Ifthere is a state of balance, that is, intake and output areat equilibrium, it can be assumed that the body is sat-urated with respect to that nutrient and has no needfor either uptake or storage. This technique can be ap-plied to almost any nutrient and by repeating balancemeasures at different levels of intake it is possible todetermine estimates of requirements for specific nu-trients. The balance model works on the assumptionthat in healthy individuals of stable weight, the bodypool of a nutrient will remain constant. Day-to-dayvariation in intake can be compensated by equivalentvariation in excretion. The highest level of intake atwhich balance can no longer be maintained will indi-cate the actual requirement of an individual for thatnutrient.
Nitrogen balance studies were used to determinehuman requirements for protein (Millward et al.,

BLBK170-Langley April 6, 2009 14:56
Introduction to Lifespan Nutrition 9
Research Highlight 1 Strategies for combating vitamin A deficiency (VAD)
VAD is one of the most common forms of malnutrition on a globalscale (West, 2003), with greatest prevalence in Africa, Central andSouth America, South and Southeast Asia. Subclinical VAD blightsthe lives of up to 200 million children every year and is a causalfactor in up to half a million cases of childhood blindness and up toa million deaths of children under the age of 5 years. VAD is alsoresponsible for stunted growth in children and may cause blindnessin women with increased demands for vitamin A, due to pregnancyor lactation. In 1990, the World Health Organization pledged itself tothe virtual elimination of VAD by the year 2000. The strategies usedto achieve this goal provide useful examples of how all commonnutrient deficiencies might be prevented at a population level. Threemain approaches have been used to tackle VAD:
1 Diet diversification. For many populations in areas where VADis common, the range of staple foods consumed is very limited.For example, rice is the basis of most meals for many in SoutheastAsia. Rice is a poor vitamin A source. Diversification programs in-clude health education and promotion of consumption of a greaterrange of foodstuffs and the development of home gardening toprovide vitamin A sources. Faber et al. (2002) showed that ahome gardening program in South Africa increased knowledgeand awareness of VAD, improved availability of vitamin A sourcesand increased serum retinol concentrations in young children.
2 Supplementation. Inmost countries where VAD is common,children are now supplemented with vitamin A, using an oil cap-
sule, two or three times a year, often coupling supplement doseswith other public health activities such as immunizations. Bergeret al. (2008) highlighted the major disadvantage of supplementa-tion, which is that it fails to reach all those in need of supplements.For VAD, those most at risk are preschool children who have lessaccess to school-based supplementation programs. Often the poorand those most in need of supplements are least likely to receivethem. Supplementation is expensive, which may reduce efficacyof the approach in impoverished countries (Neidecker-Gonzaleset al., 2007).
3 Fortification. Fortification involves the addition of nutrients tostaple foods at the point of their production, thereby increasingthe amount of nutrient delivered to all consumers of that foodstuff.VAD in several countries has been tackled using this strategy. Redpalm oil is widely available in many VAD-affected areas and is arich source of ß-carotene. In India and parts of Africa, the additionof this oil to other oils traditionally used in cooking, and to snacks,has been shown to effectively increase vitamin A intake by thegeneral population (Sarojini et al., 1999). Zagre et al. (2003)showed that introducing red palm oil to a population in BurkinaFaso was highly effective in reducing occurrence of VAD. A similarapproach involves increasing the vitamin A content of crops suchas rice, either through genetic modification (e.g., “golden rice”)or traditional plant breeding (Mayer, 2007).
1997). Such studies involved experiments in whichhealthy subjects were recruited and allocated to con-sume dietary protein at specified levels of intake. After4–6 days of habituation to these diets, urine and fe-ces were collected for determination of nitrogen lossesover periods of 2–3 days. On this basis, it was possi-ble to state dietary protein requirements for different
stages of life as being the lowest level of protein intakethat maintained nitrogen balance in healthy individu-als, maintaining body weight and engaging in modestlevels of physical activity. Nitrogen balance studies areproblematic in several respects, including the fact that24-h urine collections used in such studies are oftenincomplete, because studies may fail to allow sufficient
Total body poolInputMeasured level of nutrient intake
OutputMeasured losses via urine, feces, skin, and hair.
Nutrient balance = Input−Output
Balance=0 indicates that there is no net storage or loss of nutrient.
Positive balance indicates that there is net deposition of nutrient to the body pool.
Negative balance indicates that there is net loss of nutrient.
Figure 1.3 Determining nutrient requirementsusing the balance method. Precise measure-ments of nutrient intake and of output by allpossible routes enable determination of nutri-ent requirements. The highest level of intake atwhich balance can no longer be maintained willindicate the actual requirement of an individualfor that nutrient.

BLBK170-Langley April 6, 2009 14:56
10 Nutrition: A Lifespan Approach
time for subjects to habituate to their experimentaldiet and because factors such as unobserved infection,stress, or exercise may increase demand for protein.It has also been impossible to use balance studies toexamine protein requirements for all age groups andin all health situations, so requirements for pregnantand lactating women and for children are based onbalance studies in young adults and make estimatesof allowances for tissue deposition, growth, and milksynthesis and secretion.
1.2.5 Overall nutritional statusThe diet delivers a multitude of components ratherthan single nutrients, and it is unlikely that any indi-vidual will have a diet that perfectly achieves balancefor all of them. For example, an individual can bein balance for protein, while consuming more energythan is required and insufficient iron to meet demand.Hence, it is often not appropriate to discuss overall nu-tritional status of an individual without considerationof nutritional status with respect to specific nutrients.
Whether considering the overall nutritional statusof an individual, examining nutritional status withrespect to a specific nutrient, or investigating the nu-tritional status of a population, it is important to takeinto account a broad range of factors. It should beclear from the above discussions that intake is justone component of the supply side of the balancemodel. Nutritional status is only partly determinedby the food that is being consumed. Nutritional sta-tus also depends upon the activities and health statusof the individuals concerned. Trauma and high lev-els of physical activity will increase demand, whilea sedentary lifestyle will decrease demand. Most im-portant though is the stage of life of the individualsunder consideration. Physiological demands for nu-trients vary to a wide degree, depending on age, bodysize, and gender. The impact of variation within thediet upon health and well-being is largely, therefore,governed by age and sex.
1.3 Nutrition requirements change acrossthe lifespan
Nutritional status is determined by the balance be-tween the supply of nutrients and the demand forthose nutrients in physiological and metabolic pro-cesses. So far in this chapter, we have seen that both
sides of the supply–demand balance equation can beperturbed by a variety of different factors. Intake, forexample, can be reduced in circumstances of poverty,while demand is elevated by physiological trauma. Themain determinants of demand are, however, shapedby other factors such as the level of habitual physicalactivity (which will increase energy requirements), bygender, by body size, and by age. It is this latter factorthat provides the focus of this book.
The demand for nutrients to sustain function be-gins from the moment of conception. The embryonicand fetal stages of life are the least understood in termsof the precise requirements for nutrition, but it is clearthat they are the life stages that are most vulnerablein the face of any imbalance. Demands for nutrientsare high in order to sustain the rapid growth and theprocess of development from a single-celled zygote toa fully formed human infant. An optimal balance ofnutrients is essential, but the nature of what is trulyoptimal is difficult to dissect out from the competingdemands of the maternal system and the capacity ofthe maternal system to deliver nutrients to the fetus.The embryo and fetus represent a unique life stagefrom a nutritional perspective, as there are no nu-trient reserves and there is a total dependence upondelivery of nutrients, initially by the yolk sac and laterby the placenta. The consequences of undernutritionat this stage can be catastrophic, leading to miscar-riage, failure of growth, premature birth, low weightat birth, or birth defects (MRCVitamin Study Group,1991, Godfrey et al., 1996; El-Bastawissi et al., 2007).All of these are immediate threats to survival, but it isalso becoming clear that less than optimal nutrition atthis stage of life may also increase risk of disease lateron in life (Langley-Evans, 2006).
After birth the newborn infant has incredibly highnutrient demands that, in proportion to body weight,may be two to three times greater than those of anadult. These demands are again related to growth andthe maturation of organ systems as in fetal life. Growthrates in the first year of life are more rapid than atany other time, and the maturation of organs such asthe brain and lung continues for the first 3–8 yearsof life. Initially, the demands for nutrients are metby a single food source, milk, with reserves accruedfrom the mother toward the end of fetal life compen-sating for any shortfall in supply of micronutrients.In later infancy, there is the challenge of the tran-sition to a mixed diet of solids (weaning), which is

BLBK170-Langley April 6, 2009 14:56
Introduction to Lifespan Nutrition 11
a key stage of physiological and metabolic develop-ment. The consequences of imbalances in nutritioncan be severe. Infants are very vulnerable to protein–energy malnutrition and to micronutrient deficien-cies, which will contribute to stunting of growth andother disorders. Iodine deficiency disorders and irondeficiency anemia can both impact upon brain de-velopment, producing irreversible impairment of thecapacity to learn. Obesity is now recognized as a majorthreat to the health of children in the developed coun-tries. In this age group, it is not simply a product ofexcessive energy intake and low-energy expenditure.Increasingly, we are seeing that the type or form offoods consumed at this time can influence long-termweight gain, with breast-fed infants showing a lowerpropensity for obesity than those who are fed artificialformula milks (Arenz et al., 2004; Bayol et al., 2007).
Beyond infancy, nutrient demands begin to fall rel-ative to body weight, but still remain higher than seenin adulthood through the requirement for growth andmaturation. These demands are at their greatest at thetime of puberty when the adolescent growth spurtproduces a dramatic increase in height and weightthat is accompanied by a realignment of body compo-sition. Proportions of body fat decline and patterns offat deposition are altered in response to the metabolicinfluences of the sex hormones. Proportions of muscleincrease and the skeleton increases in size and degreeof mineralization. Nutrient supply must be of highquality to drive these processes, and in absolute terms(i.e., not considered in proportion to body size), thenutrient requirements of adolescence are the great-est of any life stage. However, adolescents normallyhave extensive nutrient stores and are therefore moretolerant of periods of undernutrition than preschoolchildren (1–5 years).
The adult years have the lowest nutrient demandsof any stage of life. As growth is complete, nutrientsare required solely for the maintenance of physiolog-ical functions. The supply is well buffered throughstores that protect those functions against adverse ef-fects of undernutrition in the short term to mediumterm. In developed countries, and increasingly so indeveloping countries, the main nutritional threat isoverweight and obesity, as it is difficult for adults toadjust energy intakes against declining physiologicalrequirements and the usual fall in levels of physicalactivity that accompany aging. Reducing energy in-take, while maintaining adequate intakes of micronu-
trients, is a major challenge in elderly individuals.Chronic illnesses associated with aging can promoteundernutrition through increased nutrient demands,while limiting appetite and nutrient bioavailability.
For women, pregnancy and lactation represent spe-cial circumstances that may punctuate the adult yearsand which increase demands for energy and nutrients.Nutrition is in itself an important determinant of fer-tility and the ability to reproduce (Hassan and Killick,2004). In pregnancy, provision of nutrients must beincreased for the growth and development of the fe-tus and to drive the deposition of maternal tissues.For example, there are requirements for an increasein size of the uterus, for preparation of the breasts forlactation and for formation of the placenta. To someextent, the mobilization of stores and adaptations thatincrease absorption of nutrients from the gut serveto meet these increased demands, but as describedabove, imbalances in nutrition may adversely impactupon the outcome of pregnancy. Lactation is incred-ibly demanding in terms of the energy, protein, andmicronutrient provision to the infant via the milk. Aswith pregnancy, not all of the increase in supply for thisprocess depends upon increased maternal intakes, andin fact women can successfully maintain lactation evenwith subclinical malnutrition. Adaptations that sup-port and maintain breast-feeding may impact uponmaternal health. For example, calcium requirementsfor lactation may be met by mobilization of bonemineral, and if not replaced once lactation has ceased,could influence later bone health. However, althoughnutritionally challenging, most evidence suggests thatlactation is of benefit for maternal health and actuallycontributes to reduced risk of certain cancers and os-teoporosis (Ritchie et al., 1998; Danforth et al., 2007).
Lifespan factors clearly impact upon nutritionalstatus as they are a key determinant of both nutrientrequirements and the processes that determine nu-trient supply. In studying relationships between diet,health, and disease, one of the major challenges is toassess the quality of nutrition in individuals and atthe population level. Tools used for these nutritionalassessments will be described in the next section.
1.4 Assessment of nutritional status
The assessment of nutritional status is necessary in avariety of different settings. Working with individuals

BLBK170-Langley April 6, 2009 14:56
12 Nutrition: A Lifespan Approach
in a clinical setting, it may be necessary to assess di-etary adequacy in order to plan the management ofdisease states, or to make clinical diagnoses. Publichealth nutritionists require data on dietary adequacyat a group level, in order to make assessments of thecontribution of nutritional factors to disease risk inthe population and to develop public health policiesor intervention strategies. Nutritional assessment isalso a critical research tool used in determining therelationships between diet and disease. These situa-tions, which rely on considerations of the likelihoodof nutritional deficit or excess at the individual orpopulation level, use tools that aim either to measureintakes of nutrients, or the physiological manifesta-tions of nutrient deficit or excess within the body.Tools for nutritional assessment include anthropo-metric measures, dietary assessments, determinationof biomarkers, and clinical examination.
1.4.1 Anthropometric measuresAnthropometric methods make indirect measure-ments of the nutritional status of individuals andgroups of individuals, as they are designed to esti-mate the composition of the body. Table 1.4 providesa summary of the commonly used anthropometrictechniques. Information about relative fatness or lean-ness can be a useful indicator of nutritional status since
excess fat will highlight storage of energy consumedin excess, while declining fat stores and loss of musclemass are indicative of malnutrition. Extremes withinanthropometric measures, for example, the emacia-tion of cachexia, or morbid obesity, are useful indi-cators of disease risk or progression in a clinical set-ting. In children, serial measures of height and weightcan provide sensitive measures of growth and devel-opment that can be used to highlight and monitornutritional problems.
1.4.2 Estimating dietary intakesEstimation of dietary intakes, either to determine in-takes of specific macro- or micronutrients, or to assessintakes of particular foods, is a mainstay of humannutrition research. A range of different methods areapplied, depending on the level of detail required. Allapproaches are highly prone to measurement error.
1.4.2.1 Indirect measuresThe least accurate measures of intake are those thatmake indirect estimates of the quantities of foodstuffsconsumed by populations. These techniques are usedto follow trends in consumption between nationalpopulations, or within a national population over aperiod of time.
Table 1.4 Anthropometric measures used to estimate body composition and nutritional status
Component of bodyTechnique composition estimated Limitations
Body mass index (weight/height2) Weight relative to height Does not distinguish between lean and fat mass. Does notmeasure the composition of the body
Skinfold thicknesses Fat mass Requires skill in measurement. Makes assumptions about theeven distribution of fat in the subcutaneous layer
Waist circumference or waist–hip ratio Fat distribution A good indicator of abdominal fat deposition. Requires setprotocols for measurement
Mid-upper arm circumference Muscle mass Prone to measurement error. Unsuitable for some groups(e.g., adolescents) with rapidly changing fat and musclepatterns. Good indicator of acute malnutrition
Bioimpedance Fat mass Influenced by hydration status of subjects
Underwater weighing Body density, fat, and lean mass Requires subjects to undergo training for an unpleasantprocedure. Underestimates fat mass in muscular individuals
Isotope dilution Body water Influenced by fluid intake of subject. Analytically difficult andexpensive
Scanning techniques (NMR, DXA) Proportions and distribution oflean and fat mass
Expensive, restricted access to scanners. Use ionizingradiation, so unsuitable for children and pregnant women

BLBK170-Langley April 6, 2009 14:56
Introduction to Lifespan Nutrition 13
020
406080
100120140160
180200
N. Am
erica
Europe
N. Afri
ca
Form
er U
SSR
M. Eas
t
Ocean
ia
S. Am
erica
C. Am
erica
SE Asia
and C
hina
S. Asia
W. A
frica
S. Afri
ca
Sub-S
ah A
frica
Pro
tein
ava
ilab
ility
g/d
/cap
ita
Plant proteinAnimal protein
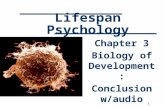
Figure 1.4 Availability of animal and plant pro-tein by world region. Per capita availability of pro-tein from plant and animal sources calculated fromthe 2004 FAO global food balance sheets.
Food balance sheets are widely used by the UnitedNations Food and Agriculture Organization (FAO) tomonitor the availability of foods, and hence nutrients,within most nations of the world and are publishedon an annual basis. They allow temporal trends to bemonitored easily and apply a standardized methodol-ogy on a global scale. A food balance sheet is essentiallycompiled from government records of the total pro-duction, imports, and exports of specific foodstuffs.This allows the quantity of that foodstuff available tothe population to be calculated (available food = pro-duction + imports – exports). Dividing that figureby the total number of people in the population al-lows the daily availability per capita to be estimated.Figure 1.4 shows data abstracted from the 2004 FAOfood balance sheets, indicating how daily availabilityof protein from plant and animal sources varies withdifferent regions of the world.
Food balance sheets are subject to considerable er-ror due to assumptions that are made in their compi-lation. It will be assumed that the nutrient composi-tion of a food will be the same regardless of where itis produced, which is clearly incorrect. For example,the selenium content of cereals from North Americais considerably greater than in the same cereals fromEurope. The balance sheets also assume that all avail-able food will be completely consumed by humansand do not allow for wastage, or feeding to animals. Itis also fallacious to assume that available food will beequally distributed to all people in a population andthe sheets make no distinction between food availableto men and women, to adults and children, or to richand poor.
Food accounts are a similar approach to estimat-ing food availability, but instead of collecting data on anational scale, they are used to measure the food avail-able to a household or an institution (e.g., a nursinghome). By compiling an inventory of food stored atthe start of a survey, monitoring food entering thesetting (often measured by looking at invoices and re-ceipts from food shopping) and taking into accountany food grown in the setting, it is possible to calculatethe food available per person over the period of thesurvey. As with the food balance sheet, this methoddoes not allow accurate estimation of individual foodintakes and does not allow for food wastage, but thefood account can provide data on dietary patterns offamilies or similar groups at low cost and over anextended period of time.
1.4.2.2 Direct measuresDirect measures of nutrient intake collect data fromindividuals or groups of individuals and, in additionto their obvious application to clinical circumstances,are well suited to research in human nutrition andepidemiology. Although more robust than the indi-rect estimates described above, all direct measures ofintake are prone to bias and error and results mustalways be interpreted with caution.
Dietary recall methodsThe dietary recall method is not only one of the bestmethods for examining nutrient intakes in a clinicalsetting, but it may also be used in research. One ofthe major disadvantages of the method is the need fora trained interviewer to spend a period of time with

BLBK170-Langley April 6, 2009 14:56
14 Nutrition: A Lifespan Approach
the patient or research subject to elicit detailed infor-mation on all food and drink consumed over a recentperiod of time. Most dietary recalls will be based uponintakes over the preceding 24 h, but in some cases maylook at 48-h or 72-h periods. Information obtainedin this way can then be coded for detailed analysis ofenergy and nutrient intakes using appropriate nutri-tional analysis software or food tables. Dietary recallmethods can generate detailed information on typesof food consumed and portion sizes. The use of pho-tographic food atlases showing portion sizes for com-monly consumed foods can enhance the quality of thisquantitative information. Spending time interviewinga subject also makes it relatively easy to obtain recipesused in cooking, and information about cooking tech-niques (e.g., use of oils in frying). Like all methods ofestimating nutrient intake, the dietary recall is proneto inaccuracy due to underreporting and overreport-ing of food intake by certain groups of people. It isalso dependent upon the memory of the subject andso loses accuracy when attempting to estimate habit-ual intakes.
Food record methodsFood records, or diaries, administered to subjects forcompletion in their own time are widely regarded asthe most powerful tool for estimation of nutrient in-takes. Subjects keep records for extended periods oftime (usually 3–7 days) and note down all foods andbeverages consumed at the time they are consumed.Portion sizes can be recorded in a number of differentways, with the subject most frequently either noting anestimated intake in simple household measures (e.g.,2 tablespoons of rice, 1 cup of sugar), or an intakeestimated through comparison to a pictorial atlas ofportion sizes. To improve the quality of the data, intakecan be accurately determined by weighing the food onstandardized scales, taking into account any wastage (aweighed food record). Frobisher and Maxwell (2003)found that in studying intakes of children aged 6–16, afood record with a photographic atlas of portion sizesgave a good level of agreement with weighed records.In some settings, it is possible for a researcher to do theweighing, thereby reducing influences upon the sub-ject consuming the food. Inaccuracies in estimates ofportion sizes are a major problem associated with foodrecord methods, particularly with some subgroups inthe population, and methods should be chosen thatbest serve the purpose of the dietary survey. Surveys of
small groups of well-motivated people in a metabolicunit lend themselves well to weighed record methods,while in large surveys of free-living individuals, theseare rarely practical.
Food records have a number of strengths comparedto other methods of estimating intake. Complex dataon meal patterns and eating habits can be obtainedthrough study of food diaries and this information cansupplement estimates of nutrient intake. By obtainingrecords for periods of 5–7 days, the intakes of mostmicronutrients can be estimated with some degree ofconfidence, in addition to energy and macronutrients.For some nutrients, it is suggested that records of 14or more days may be required (Block, 1989). The ma-jor disadvantage of the food record approach is thereliance upon the subject to complete the record fullyand accurately. Maintaining a food record is burden-some and it is often noted that the degree of detailand hence accuracy will be greater in the first 2–3 daysof a 7-day record compared to later days. The act ofrecording intake, especially if a weighed record is used,can change the eating behavior of subjects and hencelead to an underestimate of habitual intakes.
Like other direct methods, the food record is proneto underreporting and overreporting of energy andnutrient intakes among certain subgroups in thepopulation, due to the tendency of individuals to re-port intakes that will reflect them in the best pos-sible light to the researcher. Bazelmans et al. (2007)studied a group of elderly individuals, comparing self-reported intakes on a 24-h food record to estimatesof likely energy intake based upon the subjects basalmetabolic rates calculated using the Schofield equa-tion. It was found that approximately 20% of men and25% of women significantly underreported or overre-ported their energy intakes. Subjects with a BMI under25 kg/m2 (i.e., in the ideal weight range) were mostlikely to overreport, while 13% of those with BMI inthe overweight range and 27% of those with a BMIin the obese range were found to have underreportedtheir energy intake. Obese and overweight women arefrequently found to underreport intakes in dietarysurveys.
Food frequency questionnaire methodsFood frequency questionnaire methods involve theadministration of food checklists to individuals, orgroups of individuals, as a means of estimating theirhabitual intake of foods, or groups of foods. Subjects

BLBK170-Langley April 6, 2009 14:56
Introduction to Lifespan Nutrition 15
work through the checklist and, for each foodstuff,indicate their level of consumption (i.e., number ofportions) on a daily, weekly, or monthly basis. Semi-quantitative food frequency questionnaires also col-lect information on typical portion size.
Food frequency questionnaires can vary in theircomplexity and length. Often a questionnaire will con-sist of 100–150 food items and will therefore allowfor a comprehensive coverage of the dietary patternsof a subject. Some questionnaires are much shorterand may be focused upon a particular food groupor the main sources of a specific type of nutrient.For example, Block and colleagues (1989) developeda questionnaire with just 13 items in order to identifyindividuals who had high intakes of fat. This was usedas a preliminary screening tool to select subjects for amore detailed investigation.
Food frequency questionnaires have many desirableattributes for researchers wishing to estimate intakesin large populations. They are self-administered bythe subject, are generally not time consuming, andare unlikely to influence eating behaviors. Data en-try can sometimes be automated, reducing the ana-lytical burden for the researcher. Moreover, the foodfrequency questionnaire provides an estimate of ha-bitual intake over a period of months or even years, asopposed to the snapshot obtained by looking at a foodrecord representing just a few days. However, the foodfrequency questionnaire can be a weak tool when con-sidering portion sizes and is therefore less effective forestimating micronutrient intakes than a food record.Food frequency questionnaires must also be valid forthe population to be studied as the range of foodsconsumed will vary with age and various other socialand demographic factors. For example, if attemptingto survey nutrient intakes in a population with a wideethnic diversity, the foods and food groups includedon the questionnaire needs to reflect that level of diver-sity. A questionnaire that fails to include staple foodsconsumed by particular ethnic groups will inevitablyunderestimate their intake.
1.4.3 Biomarkers of nutritional statusBiomarkers of nutritional status are measures of eitherthe biological function of a nutrient, or the nutrientitself, in an individual, or in samples taken from indi-viduals. These measures can often provide the earliestindicator of a nutrient deficit as they register subnor-mal values ahead of any clinical symptoms. Biomark-
ers are therefore useful in monitoring the prevalenceof nutrient deficiency, measuring the effectiveness ofthe treatment of deficiency, and assessing preven-tive strategies. Given the huge difficulties of makingaccurate assessments of dietary intakes, as describedabove, biomarkers provide a useful means of validat-ing dietary data and are often measured as adjuncts todietary surveys. For example, in the UK National Dietand Nutrition Survey of preschool children (Gregoryet al., 1995), measurements of circulating iron sta-tus were used to back up food record data collectedon iron intakes. The doubly labeled water method(Koebnick et al., 2005) can be used to validate en-ergy intakes estimated using dietary records or othermeans.
Biomarkers of nutritional status are often regardedas being more objective than other indices. They in-clude functional tests, and measurements of nutrientconcentration in easily obtained body fluids or othermaterial. The latter type of measurement can be astatic test, which is performed on one occasion, ormay be repeated at intervals to monitor change overtime. The relative merits of these approaches will bediscussed later in this section.
Functional tests measure biological processes thatare dependent upon a specific nutrient. If that nutrientis present at suboptimal concentrations in the body,then it would be expected that the specific functionwould decline. The dark adaptation test is classic ex-ample of a functional test, which determines vitaminA status. The dark adaptation test measures visualacuity in dim light after exposure to a bright lightthat densensitizes the eye. Reformation of rhodopsinwithin the retina is dependent upon the generation ofcis-retinol and thus the visual adaptation in the darkwill be related to vitamin A status. Measurement of theexcretion of xanthurenic acid is a functional test forvitamin B6 (pyridoxine) status. Xanthurenic acid isa breakdown product of tryptophan and kynurenineand is formed via pyridoxine-dependent reactions.
Nonfunctional measures of biomarkers typicallyinvolve direct measures of specific nutrients in simplyobtained samples from individuals. These are mostcommonly samples of blood (plasma, serum, or redcells), or urine, but could include feces, hair, or, morerarely, biopsy material from adipose tissue or muscle.Static tests provide a snapshot of the nutrient con-centration in the sample at a given point in time andcould be misleading as they often provide an indicator

BLBK170-Langley April 6, 2009 14:56
16 Nutrition: A Lifespan Approach
of immediate intake rather than habitual intake. Forexample, plasma zinc concentrations will vary hugelyfrom day to day, reflecting ongoing metabolic fluxes,and fall by up to 20% following a meal (King, 1990).Wherever possible, repeated tests should be taken toincrease confidence in the measured biomarker, ortests should be performed in a sample that providesa stronger indicator of habitual intake. In the caseof zinc, plasma measurements are of limited value asmost zinc is held in functional forms within tissuesand less than 1% of the total pool is in circulation. Redor white blood cell zinc concentrations could be usedas a more robust biomarker, as could white cell met-allothionein concentrations (metallothionein is a keyzinc-binding protein). Hair zinc concentrations givea better intake of long-term status. Zinc is depositedin hair follicles slowly over time and so using thissample source removes the influence of shorter termfluctuations in status. Similarly, the EURAMIC study(Kardinaal et al., 1993) used measures of α-tocopheroland ß-carotene in biopsies of adipose tissue to assessintakes of these vitamins. As fat-soluble vitamins arestored in this tissue, this gave an indicator of habitualintake over several weeks.
The levels of a measured biomarker are only use-ful in estimating nutritional status if there is a linearrelationship between the measurement and intake. Inaddition to this, and the need to make measurementsin a relevant sample, it is important to appreciate thenondietary influences on the biomarker that couldskew the interpretation of any measurement. Somemeasurements could be perturbed by the presence ofdisease, or the use of medications to treat disease. Forexample, serum albumin concentration can be used asa marker of dietary protein intake. Serum albumin de-clines with low protein intakes and in clinical settingscan provide a predictor of morbidity and mortality as-sociated with protein–energy malnutrition. However,as described earlier in this chapter, serum albuminconcentrations also fall with infection and inflamma-tion, and in seriously ill patients, albumin could beadministered as an element of any intravenous fluidinfusion. Either situation would render albumin use-less as a marker of nutritional status. Like any mea-sure of nutritional status, biochemical indices can lackspecificity and should ideally be used as part of abattery of tests based upon dietary assessments, bio-chemical measures, anthropometry, and, if appropri-ate, clinical assessment.
1.4.4 Clinical examinationPerforming a thorough physical examination and ob-taining a detailed patient history is an effective methodof determining symptoms associated with malnutri-tion in individuals. This approach can be most use-ful when dealing with children, where the paucity ofnutrient stores can mean that clinical symptoms de-velop very quickly, as opposed to in adults where thesymptoms are generally a sign of chronic malnutri-tion. Obtaining a patient history can highlight keypoints that are missed when assessing dietary intake,or using anthropometric measures. Reported loss ofappetite, loss of blood, occurrence of diarrhea, steat-orrhea, or nausea and vomiting may all be indicatorsof potential causes of malnutrition and should triggerfurther investigation. Physical examination can assessthe degree of emaciation of a potentially malnour-ished individual. Careful assessment of the hair, skin,nails, eyes, lips, tongue, and mouth can also highlightspecific nutrient deficiencies. Bleaching of the hair isindicative of protein malnutrition, while cracking ofthe lips can suggest deficiency of B vitamins such asriboflavin. Pallor of the skin and spooning of the nailsare clinical signs of iron deficiency. Evidence of roughspots on the conjunctiva of the eye will accompanyearly stages of vitamin A deficiency.
1.5 Dietary reference values
Dietary reference values (DRVs) are standards thatare set by the health departments of governments ina number of countries around the world. DRVs areguidelines that can be used to define the compositionof diets that will maintain good health. There are manycomplex systems of DRVs used in different countries.These vary according to national health priorities andpolicies, according to predominant health status, so-cioeconomic status, body mass and rates of growth,and with local factors, for example, the compositionof foods or other lifestyle influences, that determinethe absorption and hence bioavailability of nutrients(Pavlovic et al., 2007).
DRVs are used in a variety of different ways. Whilesome systems, such as those developed for the UK, aregenerally intended to be used only with populationsor subgroups within populations, others (e.g., the USDietary Reference Intakes) are used in providing di-etary guidance for individuals. On a population level,