
Birth trauma & Intracranial haemorhhage
93
MODERATOR : Dr. Anish Chatterjee. SPEAKER : Dr. Soumalya Kundu.(Dr.B.C Roy PGIPS)
-
Upload
soumalya-kundu -
Category
Health & Medicine
-
view
289 -
download
1
Transcript of Birth trauma & Intracranial haemorhhage

MODERATOR : Dr. Anish Chatterjee.
SPEAKER : Dr. Soumalya Kundu.(Dr.B.C Roy PGIPS)

An impairment of the infants body function or structure due to adverse influences that occur at birth.
(By National vital statistics report).
#Morbidity rate : 2.8/1000 live births(AAP data)

Primiparity
Small maternal stature
Maternal pelvic anomalies
Prolonged or unusually rapid labor
Oligohydramnios
Malpresentation of the fetus
Use of mid forceps or vaccum extraction
Versions and Breech extractions
Very low birth weight or extreme prematurity
Fetal macrosomia or large fetal head
Fetal anomalies

Head and neck injuries
Nerve injury
Facial injuries
Fractures
Intra-abdominal injury
Soft tissue injuries


CAPUT SUCCEDANEUM
CEPHAL HEMATOMA
SUBGALEAL HEMORRHAGE

Diffuse, sometimes ecchymotic, edematous swelling of the soft tissues of the scalp involving the portion presenting during vertex delivery.
It may extend across the midline and across suture lines.
The edema disappears within the first few days of life.
Analogous swelling, discoloration, and distortion of the face are seen in face presentations.
No specific treatment is needed, but if there are associated extensive ecchymoses or rarely hyperbilirubinaemia – phototherapy.

It is a subperiosteal haematoma most commonly lies over one parietal bone.
It may result from difficult vacuum or forceps extraction
it is always limited to the surface of one cranial bone.
Management:
- It usually resolves spontaneously.
- Vitamin K 1 mg IM.
- hyperbilirubinemia – photo therapy.
#ASPIRATION IS CONTRAINDICATED


Subgaleal hemorrhage is bleeding between the galeaaponeurosis of the scalp and the periosteum.
firm-to-fluctuant mass that crosses suture lines.
Typically noted within 4 hours of birth.
These lesions typically resolve over a 2–3 week period
MNAGEMENT:
-No specific therapy
-Transfusions may be required if blood loss is significant.
- SGB with skin abrations – Antibiotics.


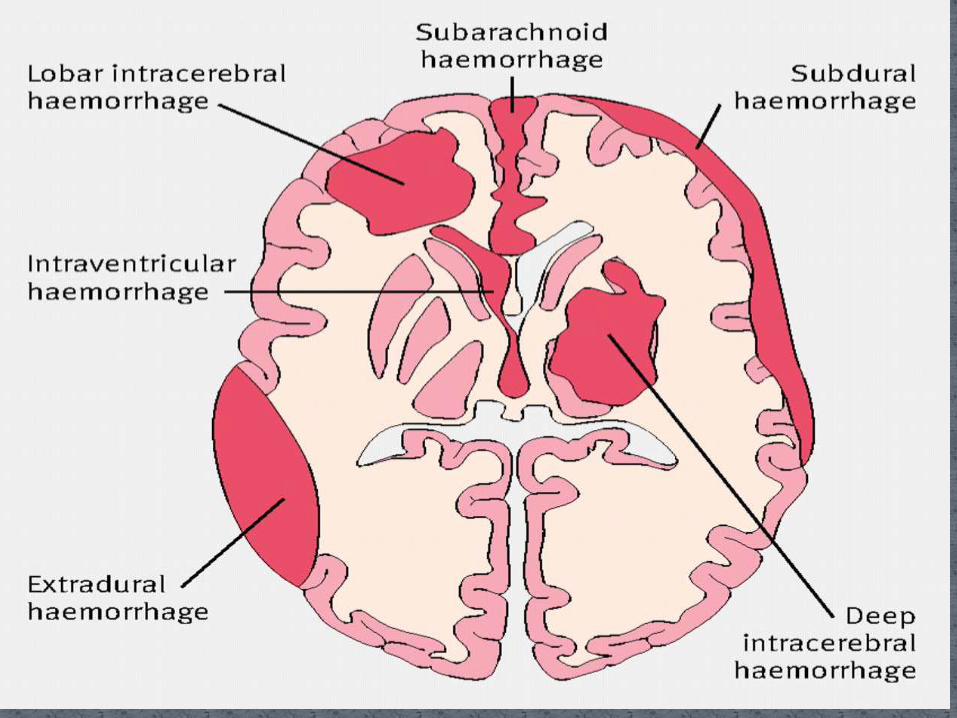
Epidural hemorrhage(T>PT)
Subdural hemorrhage (T>PT)
Subarachnoid hemorrhage(UNKNOWN)
Intraparenchymal haemorrhage(PT>T)
Germinal matrix hemorrhage / intraventricularhaemorrhage(PT>T)

Bleeding can occur - External to the brain into the epidural, subdural or
subarachnoid space
In to the parenchyma of the cerebrum or cerebellum
Into the ventricles from the subependymal germinal matrix or choroid plexus
INCIDENCE: 2% to 30% in newborns depending on GA @birth and type of ICH.

Epidural hemorrhage primarily arises from injury to the middle meningeal artery, and is frequently associated with a cephalhematoma or skull fracture.

C/F:
Diffuse neurologic symptoms
Increased intracranial pressure
Bulging fontanels
Localized symptoms,
Lateralizing seizures
Eye deviation.
DIAGNOSIS:
cranial computed tomography showing a high-density lentiform lesion in the temporoparietal region
Skull radiographs
MANAGEMENT:
Surgical mainly
Most frequent intracranial hemorrhage related to birth trauma.
Laceration of the tentorium, with rupture of the straight sinus, vein of Galen,transverse sinus, or infratentorial veins causing a posterior fossa clot and brainstem compression
Laceration of the falx, with rupture of the inferior sagittal sinus resulting in a clot in the longitudinal cerebral fissure.

Laceration of the superficial cerebral vein, causing bleeding over the cerebral convexity.
OCCIPITAL OSTEODIASTASIS:
- with rupture of the occipital sinus, resulting in a posterior fossa clot.
-direct laceration of the cerebellum.
- mainly occur in breech delivery.


C/F: Respiratory symptoms such as apnea Seizures Focal neurologic deficits Lethargy Hypotonia Other neurologic symptoms.
DIAGNOSIS: Cranial computed tomography Cranial ultrasonography(Insufficient) MRI. Coagulation profile.
#ALWAYS TO RULE OUT SEPSIS & BLEEDING DIATHESIS IN CASES OF LARGE SDH.
#LUMBAR PUNCTURE NOT TO PERFORM BEFORE CT SCAN –IF SUSPICION OF LARGE SDH(MAINLY @ PST. FOSSA OR SUPRATENTORIAL)

MANAGEMENT:
Mostly supportive with daily monitoring of OFC.
If signs of progressive brainstem dysfuntion:
- urgent CT scan of brain.
- Neurosurgical consultation.
Large SDH : open surgical evacuation of clot.

Intra cerebral
Causes:
rupture of an av malformation or aneurysm
coagulation disturbances
extracorporeal membrane oxygenation therapy(ECMO)
secondary to a large ICH in any other compartment
Intra cerebellar :
more common in preterm than the term babies. May be a primary haemorrhage or may result from venous hemorrhagic infarction or from extension of GMH/ IVH

In the preterm infant Clinically silent, unless the hemorrhage is quite large,
In the term infant, manifestations are- Seizures
Hemiparesis
Gaze preference
Irritability
Depressed level of consciousness

DIAGNOSIS:
CT Scans.
MRI(best modality,demonstares extent and age)
Cranial ultrasonography(Also through mastoid or post fontanelle for post. fossa)
MANAGEMENT:
Symptomatic treatment and supportive.

GMH/IVH is found principally in the preterm infant, where the incidence is currently 20% to 30% in infants born at <32 weeks' GA.
Risk inversely related to GA and birth wt.
-1001-1500 gm 7%(grade II or IV)
-751-1000 gm 14%
-<750 gm 24%
#PVL 3% (<1000 gm)
Uncommon in the term newborn.
The etiology and pathogenesis are different for term and preterm infants.

In the term newborn
IVH typically originates in the choroid plexus.
In association with venous (± sinus) thrombosis and
thalamic infarction,
IVH may also occur in the small remnant of the
subependymal germinal matrix.

In the preterm infant, GMH/IVH originates from the fragile involuting vessels
of the subependymal germinal matrix .
Maternal factors - infection/inflammation - hemorrhage-lack of antenatal steroids.
External factors- mode of delivery - neonatal transport to another hospital, -genetic factors
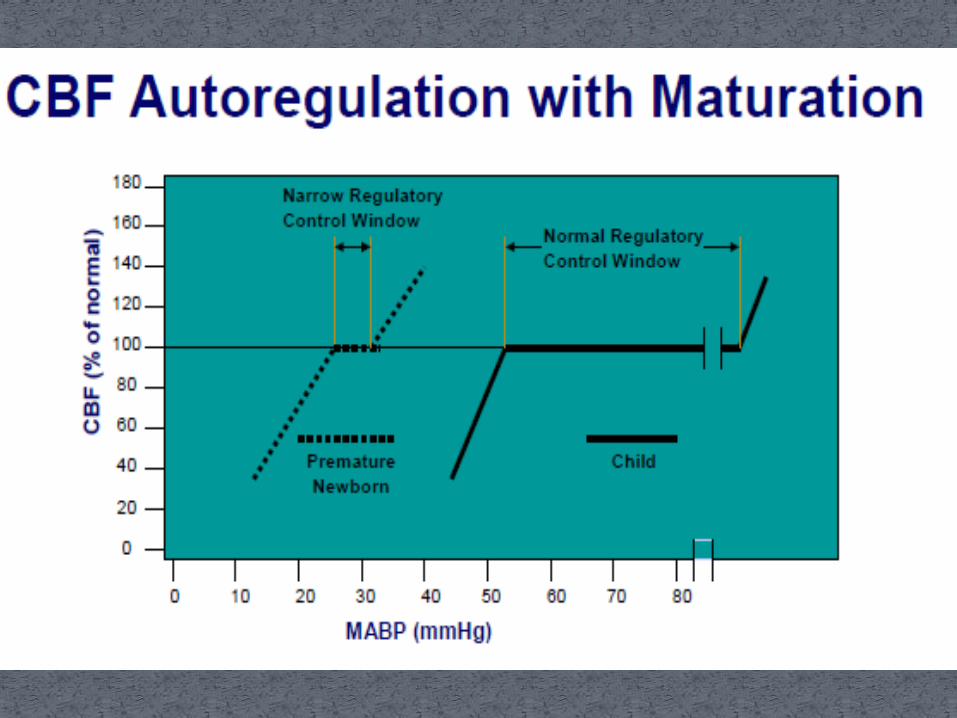
All these relates to alterations in cerebral blood flow(CBF) and coagulation. So devided in to intra-vascular, vascular, and extravascular causes.

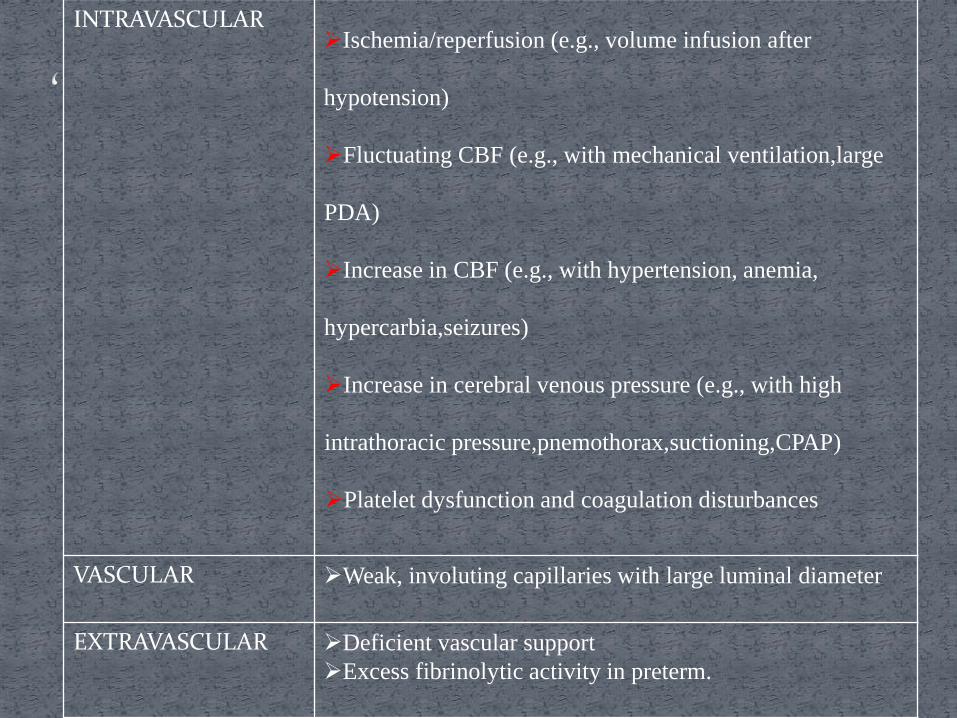
INTRAVASCULARIschemia/reperfusion (e.g., volume infusion after
hypotension)
Fluctuating CBF (e.g., with mechanical ventilation,large
PDA)
Increase in CBF (e.g., with hypertension, anemia,
hypercarbia,seizures)
Increase in cerebral venous pressure (e.g., with high
intrathoracic pressure,pnemothorax,suctioning,CPAP)
Platelet dysfunction and coagulation disturbances
VASCULAR Weak, involuting capillaries with large luminal diameter
EXTRAVASCULAR Deficient vascular support
Excess fibrinolytic activity in preterm.

Ischemia/reperfusion:- when a premature
infant may have hypovolemia or hypotension that is treated with infusion of colloid, normal saline, or hyperosmolar solutions such as sodium bicarbonate.
Rapid infusions of such solutions are thought to be particularly likely to contribute to GMH/IVH.
Fluctuating CBF:- Infants breathing out of
synchrony with the ventilator
-large patent ductus arteriosus
-hypotension

Increase in CBF:- Sustained increases in CBF may contribute to GMH/IVH ,as occurs in
seizures,
hypercarbia,
Anemia,
hypoglycemia,
(these factors results in a compensatory increase in CBF)
Increase in cerebral venous pressure:-intrathoracic pressure is high e.g.,
high continuous positive airway pressure
pneumothorax,
tracheal suctioning,
labor and delivery, where there was fetal head compression
Preterm with longer duration of labor .

Platelet dysfunction and coagulation disturbances:-
- impaired coagulation
-platelet dysfunction are also intravascula
Vascular factors
fragile nature of the involuting vessels of the
germinal matrix.
no muscularis mucosa and little adventitia in this
area of relatively large diameter,
thin-walled vessels;(make the vessels particularly
susceptible to rupture.)

Extra vascular factors
-deficient extravascular support
-likely excessive fibrinolytic activity in preterm
infants.

clinically “Silent syndrome” and thus is recognized only when a routine CUS is performed. Mainly occur within 72 hours after birth.
SYMPTOMS :
decreased levels of consciousness
spontaneous movements,
hypotonia,
abnormal eye movements
coma,
lack of spontaneous movements,
generalized tonic posturing (that is often thought to be seizure, but does not have an electrographic correlate by electroencephalogram.)

seizures, Apnea irritability or lethargy, vomiting with dehydration, worsening respiratory status,
ON EXAMINATION: Sudden onset pallor Decreased muscle tone. splitting of sutures, increasing head growth (crossing
percentiles on the growth chart) If PVD bulging fontanelle sunsetting sign feeding difficulties. ##. FAILURE OF HEMATOCRIT TO INCREASE AFTER PRBC TRANSFUSION

Primitive cellular region ventrolateral to LV
– prominent: 26-32 weeks
– involuted: term
Contains pluripotential migrating cells
– neurons, astrocytes, oligodendroglia
Contains immature blood vessels:
– thin walls (lack muscularis layer)
– immature cell junctions & basal laminae

Routine CUS :
Timing:
-on Day 7, 30 and 60 .
-In <1500 gm with <32 wks on day 3
-In VLBW and very sick babies – within 24hrs.
On follow up – MRI for associted abnormalities.


GRADING IVH/PVH (PAPILE) –by CT Scan
• Grade 1: GM hemorrhage only
• Grade 2: GM hemorrhage extending into LV without ventriculomegaly
• Grade 3: IVH with ventriculomegaly
• Grade 4: Intraparenchymal hemorrhage vs. Periventricular hemorrhagic infarction





Prevention (primary goal)
Antenatal administration of glucocorticoids hasclearly been shown to decrease the incidence ofGMH/IVH.
Antenatal phenobarbital, vitamin K, and magnesiumsulfate - not conclusive.
Minimizing risk factors as infusions of colloid orhyperosmolar solutions should be given slowly.
Avoiding hypotension and large fluctuations orsustained increases in arterial blood pressure
Elimination of CBF fluctuation related to mechanicalventilation

Supportive care should be directed toward maintaining stable
cerebral perfusion by maintaining normal blood pressure,
circulating volume, electrolytes, and blood gases.
Transfusions of PRBCs may be required in cases of large IVH
to restore normal blood volume and hematocrit.
Thrormbocytopenia or coagulation disturbances should be
corrected.
Treatment of seizure during acute phase.
Management of PVD and PVHI.

SHORT TERM :
-PVD/PHH
-PVHI
LONG TERM :
-birth weight of <1000 gm- there is severe neurologic impairment.(acc. to Bayley scales of infant development II –Mental developmental index<70,psychomotor developmental index <70,Cerebral palsy,blindness or deafness)
• GRADE I – 40%
• GRADE II – 50%
• GRADE III -55%
• GRADE IV – 70%

For Term Newborns:
-Uncomplicated IVH has favorable prognosis.
-But if associated with other lesions such as THALAMIC HAEMORRHAGIC INFARCTION,HYPOXIC ISCHAEMIC INJURY OR SINUS VENOUS THROMBOSIS, then they are at high risk for significant cognitive impairments.

PVHI(periventricular haemorrhagic infarction) has previously been considered an extension of a large IVH.
Recent concept: it’s a separate lesion consisting of a venous hemorrhagic infarction.
Neuropathologic studies demonstrate the fan-shaped appearance of a typical hemorrhagic venous infarction in the distribution of the medullary veins that drain into the terminal vein, resulting from obstruction of flow in the terminal vein by the large ipsilateral IVH.

Terminal vein passes through germinal matrix
Increased pressure from germinal matrix hemorrhage obstructs venous flow.


PVHI occurs on the side of the larger IVH, ( Doppler US -decreased or absent flow in the terminal vein on the side of the large IVH )
The EPENDYMAL LINING of the lateral ventricle separating IVH and PVHI has been observed to remain intact in some cases, demonstrating that the IVH did not ""extend" into the adjacent cerebral parenchyma.
Risk factors for the development of PVHI :- low birth GA- low Apgar scores, - early life acidosis,- patent ductus arteriosus, - pneumothorax,- pulmonary hemorrhage,

Posthemorrhagic ventricular dilation (PVD).or posthemorrhagic hydrocephalus (PHH), may occur days to weeks following the onset of GMH/IVH.
PATHOGENESIS:
-Impaired CSF resorption and/or obstruction of the aqueduct or the foramina of Luschka or Magendieby particulate clot.
-High levels of Transforming growth factor β-1(TGFβ-1) are found in the CSF following IVH. It upregulates genes for extracellular matrix proteins that elaborate a "scar," which may obstruct CSF flow and/ or CSF reabsorption

Pathogenesis of the brain injury in PVD :
-Regional hypoxia-ischemia and mechanical distension of the periventricular white matter.
-The presence of non-protein-bound iron in the CSF of infants with PVD generation of reactive oxygen species injury of immature oligodendrocytes in the white matter.


Measure of resistance to blood flow indicates decrease in cerebral compliance and perfusion.
Helps in the treatment of PVD.
Measured by DOPPLER US(usually in the anterior cerebral artery) by obtaining systolic and diastolic flow velocities.
Formula : RI = (systolic – diastolic)/systolic
Normal = <0.7
>0.9 indicate compromise in the diastolic flow.-Indication for CSF removal.


• Erb-Duchenne palsy
• Klumpke’s palsy
• Injury to the upper plexus/Brachial palsy,
It is due to over traction on
the neck as in: • Shoulder dystocia.
• After-coming head in breech delivery.

It is the most common type, due to injury to C5 and C6roots(occasionally c7) – approx. 90%
The arm is adducted and internally rotated at shoulder with extension and pronation of elbow and flexion of wrist and fingures.(policeman’s or waiter’s tip hand).
Moro reflex -absent on the affected side .
There may be some sensory impairment on the outer aspect of the arm.
The power in the forearm and the hand grasp are preservedunless the lower part of the plexus is also injured;
(the presence of the hand grasp is a favorable prognostic sign).


It is less common( < 1%)
Due to injury to C7 and C8 and 1st thoracic roots(T1)
It leads to paralysis of the intrinsic muscles of the hand and weakness of the wrist and fingers' flexors.
Grasp reflex is absent here.
Sensory impairment on the ulnar side of forearm.
(Horner syndrome)
If the sympathetic fibers of the 1st thoracic root are also injured : paralyzed hand and ipsilateral ptosisand miosis.

Injury to the brachial plexus may cause paralysis of the upper arm with or without paralysis of the forearm or hand or, more commonly, paralysis of the entire arm.
Approximately 45% are associated with shoulder dystocia.
These injuries occur in :
-Macrosomic infants
- When the arms are extended over the head in a breech presentation,
-When excessive traction is placed on the shoulders.

Depends on whether the nerve was merely injured or was lacerated.
If the paralysis was due to edema and hemorrhage of the nerve fibers, function should return within a few months.
If due to laceration, permanent damage may result.

Initial treatment is conservative.
The arm is immobilized across the upper abdomen during the first week
Physical therapy with passive range-of-motion exercises at the shoulder, elbow and wrist should begin after the first week.
Infants without recovery by 3 to 6 months of age may be considered for surgical exploration
-neuroplasty,
-neurolysis,
-end-to-end anastomosis,
-nerve grafting
#PROGNOSIS FOR FULL RECOVARY IS EXCELLENT(>90%)

RISK FACTORS:
forceps delivery
prolonged second stage of labor
CLINICAL FEATURES:
weakness of both upper and lower facial muscles.
At rest, the nasolabial fold is flattened
eye remains persistently open on the affected side.
During crying, there is inability to wrinkle the forehead or close the eye on the ipsilateral side
the mouth is drawn away from the affected side.

TYPES:
CENTRAL FACIAL NV INJURY- lower half of face on contralateral side.
PERIPFERAL INJURY: entire half of face (LMN type)
PERIPHERAL NV BRANCH INJURY: paralysis limited to only one grp of muscles.
D/D:
Mobius syndrome
ICH
Congenital hypoplasia of depressor anguli oris.
Congenital absense of facial muscles.

Protection of the involved eye by application of artificial tears and patching to prevent corneal injury.
Neurosurgical repair of the nerve should be considered only after lack of resolution after 5 weeks of observation (complete clinical and electrophysicalparalysis – on EMG)

The phrenic nerve arises from the third through fifth cervical nerve roots.(C3,C4,C5)
Injury to the phrenic nerve leads to paralysis of the ipsilateral diaphragm.

respiratory distress, with diminished breath sounds on the affected side.
Chest radiographs show elevation of the affected diaphragm, with mediastinal shift to the contralateralside.
Ultrasonography or fluoroscopy can confirm the diagnosis by showing paradoxical diaphragmatic movement during inspiration.

Initial treatment is supportive
Oxygen
Respiratory failure may be treated with continuous positive airway pressure(CPAP) or mechanical ventilation.
Gavage feedings.
Plication of the diaphragm(refractory cases)
Phrenic nv pacing in B/L paralysis.
#RECOVARY – IN 1-3 MONTHS WITHOUT PERMANENT SEQUELE.

Symptoms:
Stridor`
respiratory distress
hoarse cry
dysphagia,
Aspiration
Diagnosis is made by direct laryngoscopy

MANAGEMENT:
Small frequent feedings may be required to decrease the risk of aspiration.
Intubation
Tracheostomy
Bilateral paralysis tends to produce more severe distress, and therefore requires intubation and tracheostomy placement more frequently

Clinical findings: 3 types, HIGH CIRVICAL: respiratory
depression,shock,hypothermia,poor prognosis.
UPPER OR MID-CERVICAL:- central respiratory depression.-decreased or absent spontaneous movement-absent deep tendon reflexes- Urinary retension,absent sensation in the lower half.
INJURY @ C7 OR BELOW IT: may be reversible-lack of response to painful stimuli below the
level of the lesion.

Prognosis depends on severity and location of injury.
CT scan and MRI helpful.
MANAGEMENT:
If cord injury is suspected in the delivery room, the head, neck, and spine should be immobilized.
Therapy is supportive.
Neurosurgical consultancy.

Most common fracture is CLAVICULAR FRACTURE(3%)
2nd most common are long bone fractures(Femoral fracture > humeral fracture.)

Risk factors:
higher birth weight
prolonged second stage of labor
shoulder dystocia
instrumented deliveries
Clinical features:
Greenstick fractures may be asymtomatic.
First sign may be callus @ 7-10 days of age
Complete # may have crepitus or palpable bony irregularity.

MANAGEMENT:
-Asymptomatic incomplete fractures require no treatment.
- Complete fractures are treated with immobilization of the arm for 7 to 10 days.
#PROGNOSIS – Excellent.

Due to direct pressure on the organs.
Most common is liver injury.
Other injuries are Splenic injury and Adrenal haemorrhage.
Subcapsular hematomas are asymptomatic.
Anemia, poor feeding, tachypnea, and tachycardia
Jaundice during the 1st 3 days.
Rupture of the hematoma – discolouration of the abdominal wall, circulatory collapse and shock.
MANAGEMENT:
-volume replacement,
-correction of coagulation disturbences
- Surgical consultation.

Similar to hepatic rupture.
A mass is sometimes palpable in the left upper quadrant.
MANAGEMENT:
-Expectant mainly with observation.
-if bleebing has not stopped- Em laparotomy after Sxconsultancy.
#Abdominal paracentesis is diagnostic if a hemoperitoneum is present
#Adrenal haemorrhage can also present as a flank mass.

Fractures of mandible,maxilla and lacrimal bones.
Presents as facial asymmetry with ecchymosis,oedema,crepitance or respiratory distress.
Major concern is to maintain the airway.
Plastic surgery and ENT consultancy.
Maxillary fracture heal within 7-10 days
Mandibular fracture repair at 10-14 days

Nasal septal dislocation involves dislocation of the triangular cartilaginous portion of the septum from the vomerine groove.
Airway obstruction.
deviation of the nose to one side
The nares are asymmetric, with flattening of the side of the dislocation (Metzenbaum’s sign).
Application of pressure on the tip of the nose (Jeppesen and Windfeld test) causes collapse of the nostrils, and the deviated septum becomes more apparent

MANAGEMENT:
Definitive diagnosis can be made by rhinoscopy
Manual reduction performed by an otolaryngologist using a nasal elevator.
Reduction should be performed by 3 days of age

Rupture of Descemet’s membrane of the cornea
lid lacerations
hyphema (blood in anterior chamber)
vitreous hemorrhage
Purtscher’s retinopathy
corneal edema,
corneal abrasion
Retinal haemorhage- resolves within 1-5 days
Subcojunctival haemorrhages- resolves within 2 weeks.
Petechiae and ecchymoses
Lacerations and abrasions
Subcutaneous fat necrosis

Injury to sternocleidomastoid muscle(SCM)
Due to compartment syndrome resulting from intrauterine positioning.
Atrophic muscle fibers surrounded by collagen and fibroblasts.
Tearing of the muscle fibers or fascial sheath with hematoma formation and subsequent fibrosis.

Clinical features:
The head is tilted toward the side of the lesion and rotated to the contralateral side
chin is slightly elevated.
If a mass is present, it is firm, spindle-shaped, immobile, and located in the midportion of the sternocleidomastoid muscle, without accompanying discoloration or inflammation.

Diagnosis:
physical examination
Radiographs - to rule out abnormalities of the cervical spine.
Ultrasonography - useful both diagnostically and prognostically.
Management:
Conservative.
Stretching of the involved muscle by Physiotherapy.
Recovery by 3-4 months if persisting for 6 months then Surgery.



















