
Birth & Beyond California: Continuous Quality Improvement Project Decision Maker Course 2009 Cycle 4...
45
Birth & Beyond California: Continuous Quality Improvement Project Decision Maker Course 2009 Cycle 4 1
-
Upload
juliette-havey -
Category
Documents
-
view
217 -
download
0
Transcript of Birth & Beyond California: Continuous Quality Improvement Project Decision Maker Course 2009 Cycle 4...

Birth & Beyond California:Continuous
Quality Improvement Project
Decision Maker Course
2009
Cycle 41

2
DisclosuresNo one involved in this activity has any relevant financial relationships with commercial interests.
• Julie Barker, CHES, MPH• Carolyn Buenaflor, MPH• Cynthia Fahey, MSN, RN• Suzanne Haydu, MPH, RD• Emily Lindsey, IBCLC• Sheila Marton, RN, IBCLC• Lorraine Miles, RN, FACCE,
IBCLC• Jeanette Panchula, RN,
PHN, IBCLC
• Denise Parker, IBCLC• Karen Peters, MBA, RD,
LCCE, IBCLC• Karen Ramstrom, DO, MSPH• Sadie Sacks, MSN, RN• Carina Saraiva, MPH• Leona Shields, PHN, MN, NP• Ellen Steinberg, RN, LCCE,
IBCLC• Louise Arce Tellalian, RN,
LCCE, FACCE, CLC

Acknowledgements
• Funded from Title V Block Grant, California Department of Public Health, Maternal, Child, Adolescent Division
• In collaboration with – Regional Perinatal Programs of California– Breastfeeding Task Force of Greater LA
• Adapted from Perinatal Services Network, Loma Linda University
3

ObjectivesAfter attending this event, the participant will be able to:
• Describe three model hospital breastfeeding practices which improve breastfeeding rates
• Define the “gap” between any and exclusive breastfeeding rates
• List two hospital practices that discourage exclusive breastfeeding
4
ObjectivesAfter attending this event, the participant will be able to:
• Identify at least one hospital policy the QI Team will address to encourage breastfeeding
• Identify how California Department of Public Health collects exclusive breastfeeding data
• Describe a benefit of a Breastfeeding QI team and process in a hospital
5

Workshop Overview
• Presentation:– Literature review– Breastfeeding rates– Model Breastfeeding Policies– Birth & Beyond Project
• Action Plan Development– Identify the ‘next steps’ to improve
breastfeeding rates in this hospital
6
The Role of theHospital Administrator
• Become familiar with Birth & Beyond CA (BBC)
• Assign key decision makers to participate in the monthly BBC Regional QI Network
• Identify staff that will be part of your hospital Breastfeeding Interdisciplinary QI Team– Include the Team as part of QI or other already existing
structures – Support the Team in decisions taken to improve
breastfeeding rates
• Identify staff to become your hospital Trainers7

Breastfeeding: Important for BabiesReduced Risk of Disease
8
Source: AHRQ, 2007
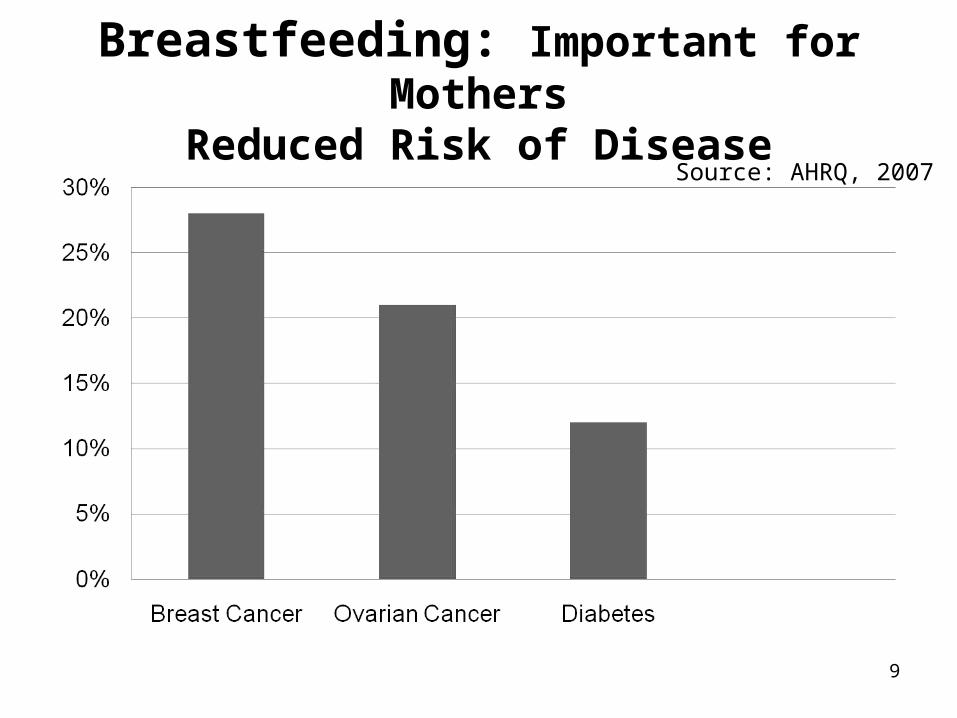
Breastfeeding: Important for MothersReduced Risk of Disease
9
Source: AHRQ, 2007

In-Hospital Breastfeeding Data Source:Newborn Screening Program
• Administered by the Genetic Disease Screening Program (GDSP)
• Primary purpose is to collect infant blood samples to screen for genetic diseases
• Staff complete the forms following the instructions provided by GDSP
• Summary data is sent to the Epidemiology staff of the Maternal, Child and Adolescent Health Program and made available on-line
10California Department of Public HealthMaternal, Child, and Adolescent Health Program

Breastfeeding Categories
• “ANY BREASTFEEDING” – Includes infants fed only human milk and infants fed a
combination of human milk and formula
• “EXCLUSIVE BREASTFEEDING” – Infants fed only human milk– Recommended by American Academy of Pediatrics, American
College of Obstetricians and Gynecologists, Academy of Family Physicians, American Dietetic Association
– In-hospital exclusive breastfeeding is associated with breastfeeding duration after discharge
11

California Any and Exclusive In-Hospital Breastfeeding: 1994-2007
43%43%44% 44% 43% 44% 44% 44% 43% 43% 43% 42% 42% 42%
87%87%86%86%86%85%84%84%83%82%80%79%77%77%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
1994 1995 1996 1997 1998 1999 2000 2001 2002 2003 2004 2005 2006 2007
Exclusive Breastfeeding Any Breastfeeding
12Data Source: California Department of Public Health, Genetic Disease Screening Program, Newborn Screening Database 1994-2007 Prepared by: California Department of Public Health, Maternal, Child and Adolescent Health Program Note: Includes cases with feeding marked ‘BRO’ (Breast Only), ‘FOO’ (Formula Only), or ‘BRF’ (Breast & Formula)
The “GAP” is Growing

Percent Any/Exclusive In Hospital Breastfeeding: 2007
81%86%
83%87%
43%
24%30%
35%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
California Average LA County Average Orange County Average Central Valley Average
Any BF Exclusive BF
13
Gap
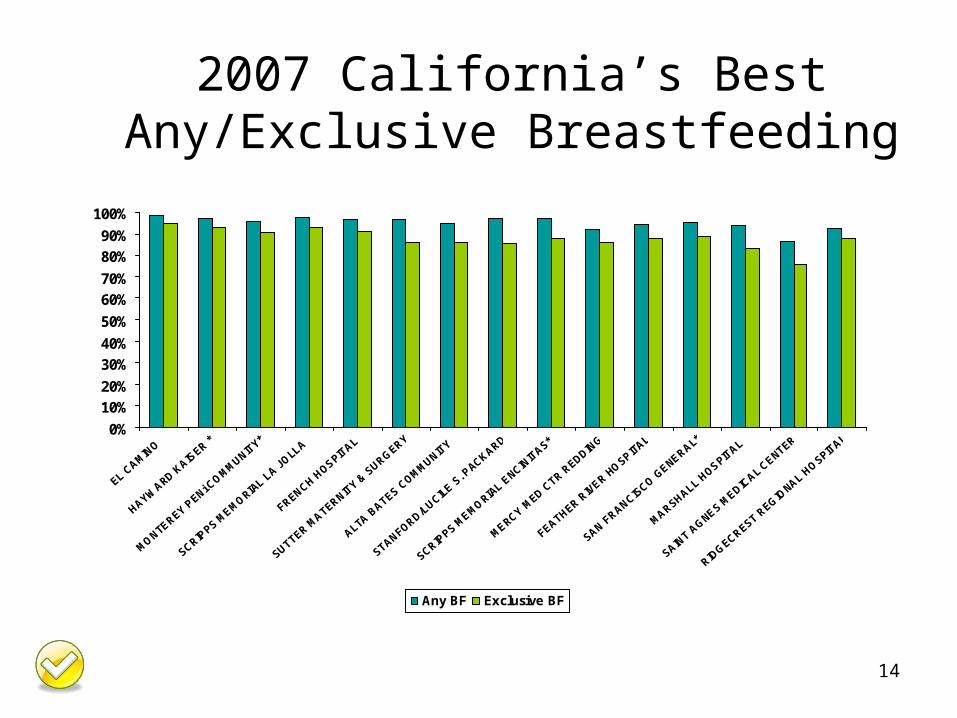
2007 California’s BestAny/Exclusive Breastfeeding
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
EL CAMIN
O
HAYWARD K
AISER *
MONTEREY P
ENi COMMUNIT
Y*
SCRIPPS M
EMORIAL L
A JOLL
A
FRENCH HOSPIT
AL
SUTTER MATERNIT
Y & S
URGERY
ALTA B
ATES COMMUNIT
Y
STANFORD/LUCILE
S. P
ACKARD
SCRIPPS M
EMORIAL E
NCINIT
AS*
MERCY MED C
TR REDDIN
G
FEATHER RIV
ER HOSPITA
L
SAN FRANCIS
CO GENERAL*
MARSHALL HOSPIT
AL
SAINT A
GNES MEDIC
AL CENTER
RIDGECREST R
EGIONAL H
OSPITAL
Any BF Exclusive BF
14
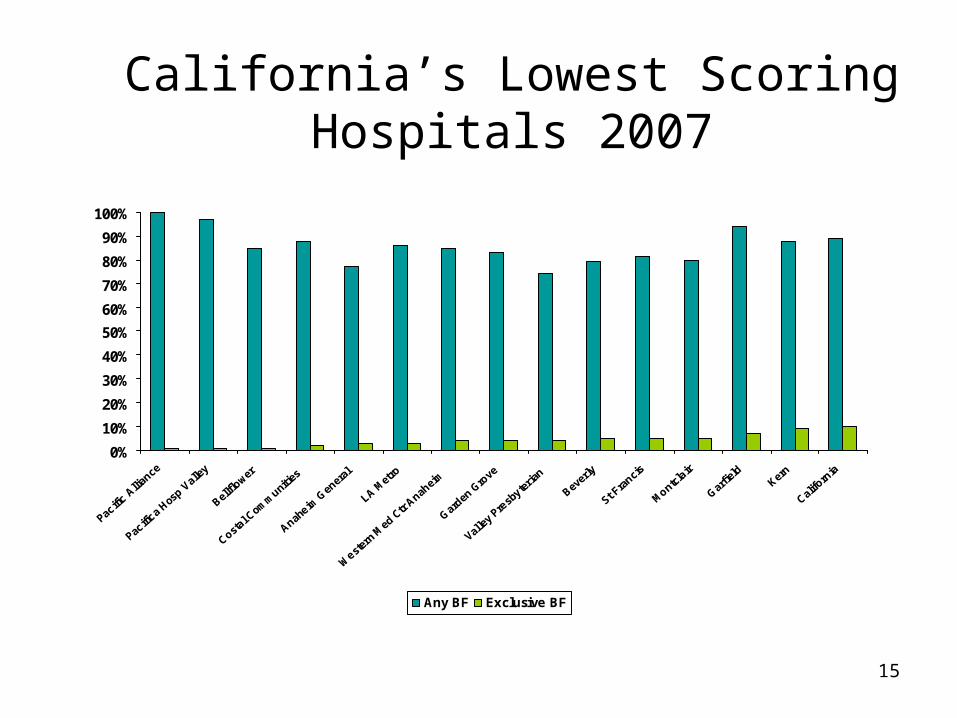
California’s Lowest Scoring Hospitals 2007
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Pacific
Allia
nce
Pacific
a Hos
p Vall
ey
Bellflo
wer
Costal C
omm
unities
Anaheim
Gen
eral
LA Met
ro
Weste
rn M
ed C
tr Anah
eim
Garden
Gro
ve
Valley
Pre
sbyter
ian
Bever
ly
St Fra
ncis
Montclair
Garfie
ldKer
n
Califo
rnia
Any BF Exclusive BF
15

Best LA HospitalsExclusive Breastfeeding 2007
89%92%94%92%91%
95%
69%66% 61%
55% 53% 51%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
St Johns Santa Monica Holy Cross* UCLA Cedars San Dimas
Any BF Exclusive BF
16

Percent Any/Exclusive In Hospital Breastfeeding: 2007
Closing the Gap
17
Closed the GapClosed the Gap
Closing

Hospital X2004- 2007
Any/Exclusive Breastfeeding
90%89%91%89%
54.3%50.0%
52.2%47.9%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
2004 2005 2006 2007
Any BF Exclusive BF
18

Hospital Policy is Key
• Hospitals with written policy have better breastfeeding outcomes at 2 weeks
• Administrative prioritization of breastfeeding support drives the hospital practices that lead to improved breastfeeding
• Monitor improvements in breastfeeding support over time
19
Rosenberg, Breastfeeding Medicine, 2008

Hospital Practices:
Associated with breastfeeding duration
0 25 50 75 100
Baby breastfed in 1st hour after birth
Baby fed only breastmilk in hospital
Baby stayed in same room with mother
Baby did not use pacifier in hospital
Hospital gave mother phone number to call forbreastfeeding help
Percent
No
Yes
20Murray ,Murray , Birth, Birth, 20072007

Hospital Policies: Increased number of “Baby-Friendly” Hospital
practices in place decreases risk of breastfeeding cessation
DiGirolamo, Pediatrics, 2008
21
Steps measured: Early bf initiation Exclusive breastfeeding
Rooming-in On-demand feedings
No pacifiers Information provided
Breastfeeding Duration
• Breastfeeding at 6 months was associated with – Exclusive breastfeeding in hospital– Not receiving a gift pack with formula at
hospital discharge
22
Dabritz, J Hum Lact, 2008

Hospital Policies: Affect all ethnicities & income levels • Breastfeeding rates in US Baby-Friendly
Hospitals exceed state and regional rates across all ethnicities and income levels
• Breastfeeding rates are high in these hospitals even among populations who do not traditionally breastfeed
23
Merewood, Pediatrics, 2005
CDC Guide to Breastfeeding Interventions
• Evidence Based Maternity Care Interventions
• Improve breastfeeding rates
Shealy, CDC, 2005
24
• Providing Breastfeeding Support: Model Hospital Policy Recommendations
• Model Hospital Policy Recommendations Toolkit
cdph.ca.gov/Breastfeeding
25
California Model Hospital Policy Recommendations Toolkit
• Basic information and guidance to revise policies that affect the breastfeeding mother
• Rationale and references are included as education for those unfamiliar with current breastfeeding recommendations
26
cdph.ca.gov/Breastfeedingcdph.ca.gov/Breastfeeding

Why Formula Was Used
• Provided without the mother asking for it or the doctor prescribing it.64%
• Formula was requested by the mother 13%
• Don’t Know 10%
• Formula not given 9%
• Doctor prescribed formula 4%
27
SLAHP Breastfeeding Peer Counselor Support Project SLAHP Breastfeeding Peer Counselor Support Project Baseline Report 2004Baseline Report 2004

Did mothers get what they wanted?
0.00%
10.00%
20.00%
30.00%
40.00%
50.00%
60.00%
70.00%
80.00%
Plan Actual - 2 wks PP Actual - 3 months PP
Exclusive BF Combo Exclusive Formula
28SLAHP Breastfeeding Peer Counselor Support Project SLAHP Breastfeeding Peer Counselor Support Project Baseline Report 2004Baseline Report 2004

29
Birth & Beyond California
• Quality Improvement– Support for your QI team– Policy revision technical assistance– Technical assistance and tools for data
collection and analysis tailored to your hospital• BBC Regional QI Network meetings
– Monthly• Training
– 2 hour Decision Maker – 16 hour Learner Workshop– 16 hour Train the Trainer

Birth & Beyond CaliforniaParticipating Hospitals
California Hospital Medical Center
Good Samaritan HospitalHenry Mayo Medical
CenterHuntington Memorial
HospitalLong Beach Memorial:
Miller Children’s Hospital
Northridge Hospital Medical Center
Olive View – UCLA Medical Center
Pomona Valley Hospital Medical Center
Providence Holy Cross Medical Center
Providence St. Joseph Medical Center
Providence Tarzana Medical Center
St. Francis Hospital Lynwood
Torrance Memorial Hospital
30

Restoring the Original Paradigm
The original “model or pattern”Miriam-Webster Dictionary
DVD by Nils Bergman, MD
31

The physiologic norm is easier
• Skin to skin triggers – Infant competence – Appropriate maternal responses
• Exclusive breastfeeding in the early days promotes a cascade of breastfeeding successes
• Mother/baby togetherness in the early days enhances parental competence
32Moore, Cochrane Review, 2007Chiu, Breastfeeding Medicine, 2008

Our Goal
To help your staff
get better results with
less time & effort
33

Benefits of Breastfeeding Quality Improvement
• Mother & Baby– Increased attachment & bonding– Optimal infant nutrition & health– Patient satisfaction
• Hospital– Joint Commission – Continuous Quality Improvement– Increased staff competence and self-efficacy– Supports marketing– Increased teamwork– Worksite Lactation Support: Reduced absenteeism
• Others?34

Costs of Breastfeeding Quality Improvement
• Staff Education– Nurses’ time for training– Trainers’ time– Back up staff during trainings– Classroom supplies
• Data collection
• Facility Improvements
• Others?
35

36

Breastfeeding Makes Good Business Sense
• Lower Absenteeism Rates
• Lower Healthcare Costs
• Lower Turnover Rates
• Higher Employee Productivity and Morale
• Higher Employer Loyalty
• Recognition as a “Family Friendly” Business
37

Role of Your Breastfeeding Interdisciplinary QI Team
• Work with key staff to interpret results of the self-appraisal tool
• Develop breastfeeding policies• Facilitate training & systems change • Monitor policy adherence & evaluation
data• Technical assistance available from the
Regional Perinatal Programs of California38

Team
• Required Members1. Physician
2. Administration
3. Nursing
4. Quality Improvement
5. Nutrition
6. Lactation
• Optional Members– Pharmacy– OT– OB/Peds
Clinics– Others?
39

Role of theBBC Network
• Who?– MCH Directors, QI Team Members, Nurse Managers,
Trainers
• What?– Monthly interactive discussion
• Why?– Support – Information sharing – Celebrating successes – Keep staff motivated!
40

Role of Your BBC Trainers
• Attend the Learner Workshop – Observe Master Trainers presenting the model 16
hour BBC Course– Provide onsite coordination – Participate with colleagues in the learner centered
activities
• Attend the 16 hour Train-the-Trainer Workshop– Improve knowledge of teaching adults– Practice using the BBC Curriculum & tools– Plan for sustainability of training activities
41

Training Sustainability
Recommendations for Maximum Impact • Budget for and plan mandatory training for all
mother baby staff within the first year– 16 hours didactic– 3 hours clinical
• Plan on repeating the 16 hour course– Annually, biannually, quarterly– Depending on your new hire training requirements
42

Medical Staff Training Ideas
– Identify physician champions and CME programs
– Committee Meetings– Grand Rounds– Self Study Modules– Hospital staff providing “lunch & learn”
sessions to medical office staff
43

Action Plan
• Immediate Action Steps?
44
Thank You!
45
Please complete the Post Test &
Evaluation form


















