
Bipolar Disorders I & II
47
Bipolar Disorders I & II University of Massachusetts, Amherst Nursing 690M Donna Petko, MSN, RN, APN, FNP-BC April 7, 2015
-
Upload
donna-petko -
Category
Health & Medicine
-
view
131 -
download
3
Transcript of Bipolar Disorders I & II

Bipolar Disorders I & IIUniversity of Massachusetts, Amherst
Nursing 690M
Donna Petko, MSN, RN, APN, FNP-BC
April 7, 2015
Objective
• prevalence
• diagnostic criteria
• development
• functional consequences
• cultural issues
• measurements
• diagnostic features
• specifiers
• severity levels
• differential diagnoses
• ICD-10 coding
To increase understanding of Bipolar Disorders I & II listed in the DSM-5 (APA, 2013):

Bipolar Disorders I & II
Bipolar I Disorder
Prevalence (APA, 2013):
• 12-month prevalence estimate in US is 0.6%
• Lifetime male-to-female ratio is 1.1:1

Bipolar I Disorder Cont.
Diagnostic Criteria (APA, 2013):
• At least one lifetime manic episode required for diagnosis
• Manic episode may be preceded/followed by hypomanic or major depressive episode
• Specific criteria must be met for a current/past hypomanic episode and current/past major depressive episode

Bipolar I Disorder Cont.
Manic Episode (APA, 2013):
• Distinct period of abnormally and persistently elevated, expansive, or irritable mood
• Increased energy or activity
• Lasting at least 1 week and present most of the day, nearly every day

Bipolar I Disorder Cont.
Manic Episode cont. (APA, 2013):
• 3 or more of the following (4 if mood is only irritable):• Inflated self-esteem or grandiosity
• Decreased need for sleep
• More talkative than usual
• Flight of ideas
• Distractibility
• Increase in goal-directed activity
• Excessive involvement in risk taking activities
• Spending sprees
• Sexual indiscretions

Bipolar I Disorder Cont.
Manic Episode cont. (APA, 2013):
• Mood disturbance is severe to cause marked impairment in social/occupational functioning or requires hospitalization
• Episode not attributable to the physiological effects of a substance or another medical condition

Bipolar I Disorder Cont.
Hypomanic Episode (APA, 2013):
• Distinct period of abnormally and persistently elevated, expansive, or irritable mood
• Increased activity or energy
• Lasting at least 4 consecutive days and present most of the day, nearly every day
Bipolar I Disorder Cont.
Hypomanic Episode cont. (APA, 2013):
• 3 or more of the following (4 if mood is only irritable):• Inflated self-esteem or grandiosity
• Decreased need for sleep
• More talkative than usual
• Flight of ideas
• Distractibility
• Increase in goal-directed activity
• Excessive involvement in risk taking activities
• Spending sprees
• Sexual indiscretions
Bipolar I Disorder Cont.
Hypomanic Episode cont. (APA, 2013):
• Episode associated with change in functioning• Uncharacteristic when asymptomatic
• Disturbance in mood/change in functioning observed by others
• Not severe enough to cause impairment in social/occupational functioning• Not requiring hospitalization
• Not attributable to the physiological effects of a substance
• Are common in bipolar I but not required for diagnosis
Bipolar I Disorder Cont.
Major Depressive Disorder (APA, 2013):
• 5 or more of the following symptoms during the same 2-week period and represent change from prior functioning:• 1 symptom must be (1) depressed mood or (2) loss of
interest/pleasure
• Depressed mood most of the day, nearly every day per subjective report or observation
• Diminished interest, pleasure in all, or most, activities
• Significant weight-loss or weight-gain
• Insomnia or hypersomnia
• Psychomotor agitation
• Fatigue
Bipolar I Disorder Cont.
Major Depressive Disorder cont. (APA, 2013):• Feelings of worthlessness
• Diminished ability to think/concentrate
• Recurrent thoughts of death, suicidal ideation
• Symptoms cause clinically significant distress/impairment in social, occupational functioning
• Not attributable to the physiological effects of a substance or another medication
• Are common in bipolar I but not required for diagnosis

Bipolar I Disorder Cont.
Development and Course (APA, 2013):
• Mean age of onset: 18 years
• Onset may occur throughout the life cycle• Manic symptoms later in life may indicate medical conditions
• > 90% of individuals who have 1 episode experience recurrent
• Approx. 60% of manic episodes occur immediately before a major depressive episode
• Rapid cycling occurs when individuals experience 4 or more mood episodes in 1 year
Bipolar I Disorder Cont.
Functional Consequences (APA, 2013):
• Approx. 30% of individuals experience severe impairment in work role function
• Functional recovery may be slow
• Cognitive impairments may occur
Cultural issues (APA, 2013):
• Little data exists on specific cultural differences
• Lack of transcultural validation
• One U.S. study shows 12-month prevalence significantly lower in Afro-Caribbeans than African Americans and Whites

Bipolar I Disorder Cont.
Measurements (STABLE, 2007):
• The Mood Disorder Questionnaire (MDQ)• Screening tool: present and past episodes of mania/hypomania.
• Includes 13 questions associated with the symptoms of bipolar disorder
• Plus items assessing clustering of symptoms and functional impairment
• May be used in primary care settings
• Efficient way to identify patients most likely to have a bipolar disorder
Bipolar I Disorder Cont.
Measurements cont. (STABLE, 2007):
• The Composite International Diagnostic Interview (CIDI) Bipolar Disorder Screening Scale• Can accurately identify threshold/sub-threshold bipolar disorder
• Scale detected between 67-96% of true cases in clinical studies
• Compares favorably with the MDQ screening scale

Bipolar I Disorder Cont.
Diagnostic Features (APA, 2013):
• Manic Episode:• Euphoric: “feeling on top
of the world”
• Increased activity
• Irritable
• Grandiose delusions
• Decreased need for sleep
• Rapid, pressured speech
• Racing thoughts
• Distractibility
• Marked impairment in social/occupational function
• Rapidly shifting mood to anger or depression
• Depressive symptoms may occur during a manic episode

Brief I Disorder Cont.
Specifiers (APA, 2013):
• With anxious distress
• With mixed features
• With rapid cycling
• With melancholic features
• With atypical features
• With mood-congruent psychotic features
• With mood-incongruent psychotic features
• With catatonia
• With peripartum onset
• With seasonal pattern
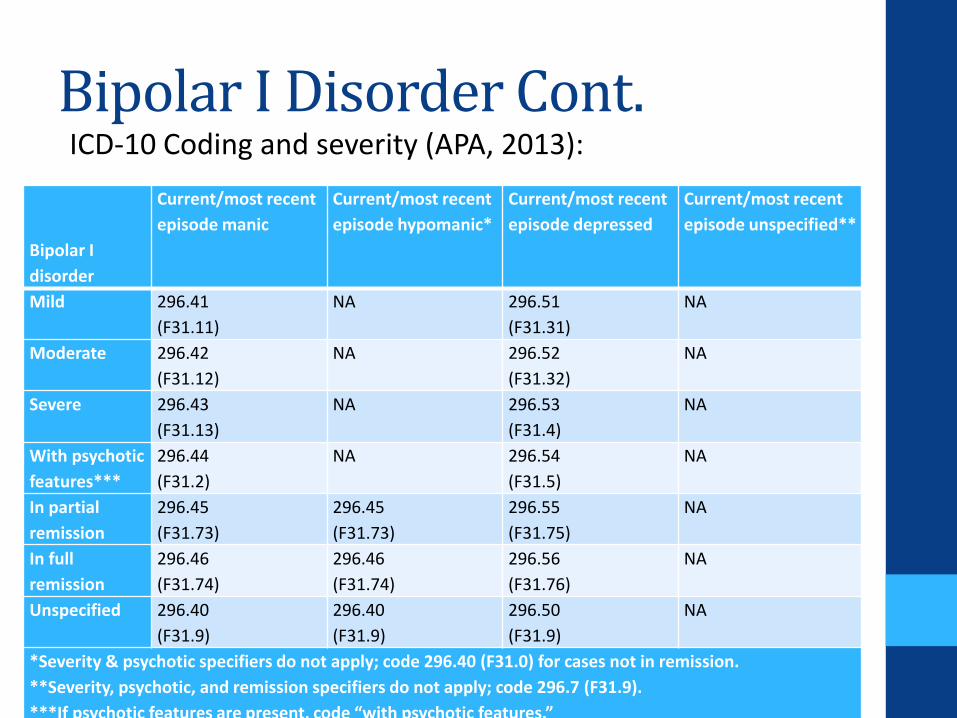
Bipolar I Disorder Cont.ICD-10 Coding and severity (APA, 2013):
Bipolar I
disorder
Current/most recent
episode manic
Current/most recent
episode hypomanic*
Current/most recent
episode depressed
Current/most recent
episode unspecified**
Mild 296.41
(F31.11)
NA 296.51
(F31.31)
NA
Moderate 296.42
(F31.12)
NA 296.52
(F31.32)
NA
Severe 296.43
(F31.13)
NA 296.53
(F31.4)
NA
With psychotic
features***
296.44
(F31.2)
NA 296.54
(F31.5)
NA
In partial
remission
296.45
(F31.73)
296.45
(F31.73)
296.55
(F31.75)
NA
In full
remission
296.46
(F31.74)
296.46
(F31.74)
296.56
(F31.76)
NA
Unspecified 296.40
(F31.9)
296.40
(F31.9)
296.50
(F31.9)
NA
*Severity & psychotic specifiers do not apply; code 296.40 (F31.0) for cases not in remission.
**Severity, psychotic, and remission specifiers do not apply; code 296.7 (F31.9).
***If psychotic features are present, code “with psychotic features.”

Bipolar I Disorder Cont.
Differential Diagnoses (APA, 2013):
• Major depressive disorder
• Other bipolar disorders
• Generalized anxiety disorder, panic disorder, posttraumatic stress disorder, or other anxiety disorders
• Substance/medication-induced bipolar disorder
• Attention-deficit/hyperactivity disorder
• Personality disorders
• Disorders with prominent irritability
Bipolar II Disorder
Prevalence (APA, 2013):
• 12-month prevalence estimate in US is 0.8%• Internationally 0.3%
Diagnostic Criteria (APA, 2013):
• One hypomanic and one major depressive episode
• Never experienced a manic episode
• Specific criteria must be met for a current/past hypomanic episode and current/past major depressive episode:

Bipolar II Disorder Cont.
Hypomanic Episode (APA, 2013):
• Distinct period of abnormally and persistently elevated, expansive, or irritable mood
• Increased activity or energy
• Lasting at least 4 consecutive days and present most of the day, nearly every day

Bipolar II Disorder Cont.
Hypomanic Episode cont. (APA, 2013):
• 3 or more of the following (4 if mood is only irritable):• Inflated self-esteem or grandiosity
• Decreased need for sleep
• More talkative than usual
• Flight of ideas
• Distractibility
• Increase in goal-directed activity
• Excessive involvement in risk taking activities
• Spending sprees
• Sexual indiscretions

Bipolar II Disorder Cont.
Hypomanic Episode cont. (APA, 2013):
• Episode associated with change in functioning• uncharacteristic when asymptomatic
• Disturbance in mood and change in functioning observed by others
• Not severe enough to cause impairment in social/occupational functioning
• Not requiring hospitalization
• Not attributable to the physiological effects of a substance
Bipolar II Disorder Cont.
Major Depressive Disorder (APA, 2013):
• 5 or more of the following symptoms during the same 2-week period and represent change from prior functioning:• 1 symptom must be (1) depressed mood or (2) loss of
interest/pleasure
• Depressed mood most of the day, nearly every day per subjective report or observation
• Diminished interest, pleasure in all, or most, activities
• Significant weight-loss or weight-gain
• Insomnia or hypersomnia
• Psychomotor agitation
• Fatigue
Bipolar II Disorder Cont.
Major Depressive Disorder cont. (APA, 2013):• Feelings of worthlessness
• Diminished ability to think/concentrate
• Recurrent thoughts of death, suicidal ideation
• Symptoms cause clinically significant distress/impairment in social, occupational functioning
• Not attributable to the physiological effects of a substance or another medication

Bipolar II Disorder Cont.
Development and Course (APA, 2013):
• Can begin in late adolescence
• Average age of onset in mid-20s• Slightly later than bipolar I
• Most often begins with depressive episode and not recognized until hypomanic episode occurs
• May be preceded by anxiety, substance use, or eating disorders
• Lifetime episodes of hypomanic and depressive episodes greater than in bipolar I
Bipolar II Disorder Cont.
Functional Consequences (APA, 2013):
• Most individuals return to fully functional state between episodes
• 15% may continue to have some inter-episode dysfunction
• 20% transition directly into another mood episode without inter-episode recovery
• Functional recovery may be slow
• Cognitive impairments may occur

Bipolar II Disorder Cont.
Cultural Issues (APA, 2013):
• Little data exists on specific cultural differences• Lack of transcultural validation

Bipolar II Disorder Cont.
Measurements (STABLE, 2007):
• The Mood Disorder Questionnaire (MDQ)• Screening tool: present and past episodes of mania/hypomania.
• Includes 13 questions associated with the symptoms of bipolar disorder
• Plus items assessing clustering of symptoms and functional impairment
• May be used in primary care settings
• Efficient way to identify patients most likely to have a bipolar disorder

Bipolar II Disorder Cont.
Measurements cont. (STABLE, 2007):
• The Composite International Diagnostic Interview (CIDI) Bipolar Disorder Screening Scale• Can accurately identify threshold/sub-threshold bipolar disorder
• Scale detected between 67-96% of true cases in clinical studies
• Compares favorably with the MDQ screening scale

Bipolar II Disorder Cont.
Diagnostic Features (APA, 2013):
• Recurring mood episodes:• 1 or more major depressive episodes
• Episode lasting at least 2 weeks
• At least 1 hypomanic episode
• Episode lasting at least 4 days
• During episode(s), required number of symptoms must be present most of the day, nearly every day
• A manic episode precludes the diagnosis of bipolar II
• Individuals typically present for treatment during major depressive episode

Bipolar II Disorder Cont.
Specifiers and Severity(APA, 2013):
• Specify current or most recent episode:• Hypomanic
• Depressed
• Specify if (APA, 2013):• With anxious distress
• With mixed features
• With rapid cycling
• With mood-congruent psychotic features
• With mood-incongruent psychotic features
• With catatonia
• With peripartum onset
• With seasonal pattern

Bipolar II Disorder Cont.
• Specify course if full criteria for a mood episode not currently met (APA, 2013):• In partial remission
• In full remission
• Specify severity if full criteria for a mood episode are currently met (APA, 2013):• Mild
• Moderate
• Severe
Bipolar II Disorder Cont.
Differential diagnoses (APA, 2013):
• Major depressive disorder
• Cyclothymic disorder
• Schizophrenia spectrum and other related psychotic disorders
• Panic disorder or other related anxiety disorders
• Substance use disorders
• Attention-deficit/hyperactivity disorder
• Personality disorders
• Other bipolar disorders
Bipolar II Disorder Cont.
ICD-10 (APA, 2013, p. 111):
• Bipolar II disorder has only one diagnostic code:• 296.89 (F31.81)
• Severity, presence of psychotic features, course, and other specifiers cannot be coded but should be indicated in writing

Differences Between Bipolar I & II
Bipolar I• At least 1 manic or mixed
episode
Bipolar II• Never had a manic episode
• At least 1 hypomanic episode
• At least 1 major depressive episode
Bipolar Disorders I & II Cont.

Bipolar Disorders I & II Cont.
Treatment Options for Bipolar I & II (Epocrates, 2015):
• Pharmacologic:• Mood stabilizers
• Atypical antipsychotic
• Typical antipsychotic
• Alternative antipsychotic
• Neuroleptic
• Other neurologic
• Benzodiazepine
• Antidepressants
Bipolar I & II Disorders Cont.
Treatment cont. (Epocrates, 2015):
• Education to recognize and manage early symptoms
• Psychotherapies:• Cognitive behavioral therapy
• Family-focused therapy
• Interpersonal social rhythm therapy
• Psychoeducation
• Electroconvulsive therapy (ECT)
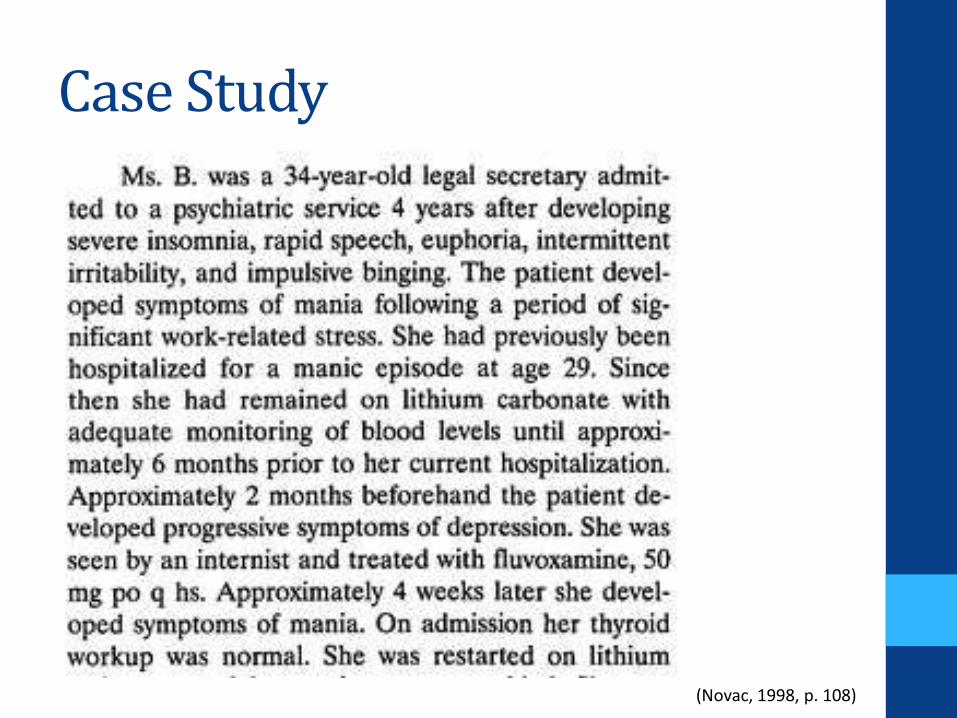
Case Study
(Novac, 1998, p. 108)
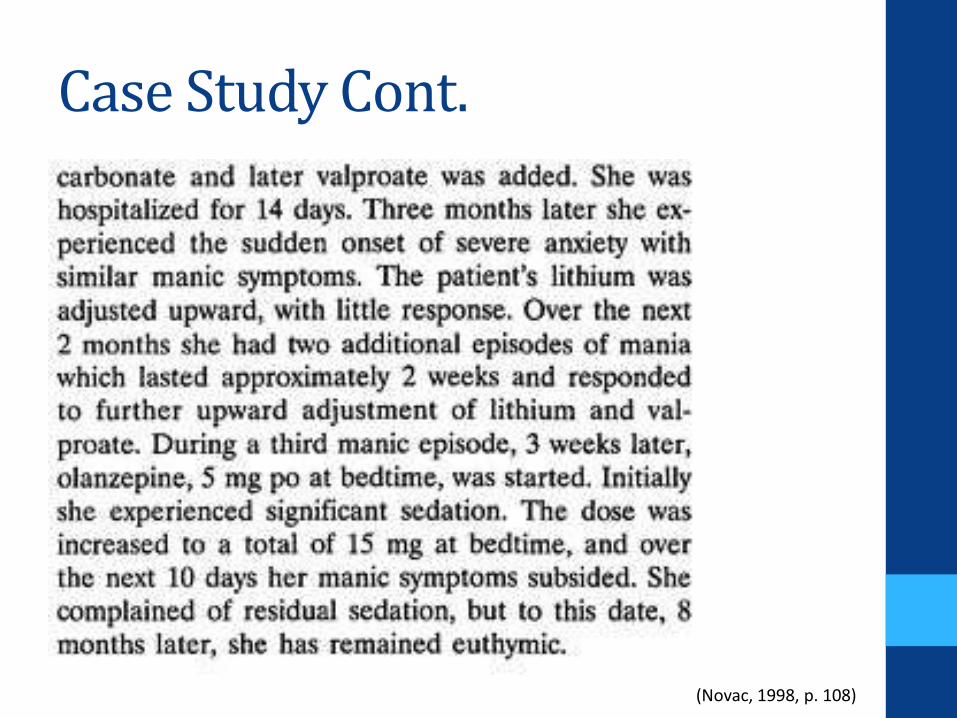
Case Study Cont.
(Novac, 1998, p. 108)
Case Study Cont.
Did you recognize the symptoms of Bipolar I Disorder?
• Mania:• Insomnia
• Rapid speech
• Euphoria
• Intermittent irritability
• Hospitalized for a previous manic episode
• Depression 2 months prior and treated with SSRI• Antidepressants can worsen mania and cause rapid cycling
• Rapid cycling

The End

References
American Psychiatric Association. (2013). Clinician-rated dimensions of psychosis symptom severity. Retrieved from http://www.psychiatry.org /File%20Library/ Practice/DSM/DSM-5/ClinicianRatedDimensionsOf
PsychosisSymptomSeverity.pdf
American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Washington D.C.: Author.
Epocrates. (2015). Bipolar disorder in adults. Retrieved from https://online.epocrates.com/u/2942488/Bipolar+disorder+in+adults/Treatment/Tx+Details

References Cont.
Novac, A. (1998). Atypical antipsychotics as enhancement therapy in rapid cycling mood states: A case study. Retrieved from http://link.springer.com/article/ 10.1023/A%3A1022398104353
Stable National Coordinating Council. (2007). Stable resource toolkit. Retrieved from http://www.integration.
samhsa.gov/images/res/STABLE_toolkit.pdf


















