Bipolar Disorder: Harnessing Brain Plasticity for Improved Overall … · 2019. 12. 17. · o n t r...
25
Husseini K Manji Global Therapeutic Head for Neuroscience Johnson & Johnson (previously Director of NIMH Mood & Anxiety Disorders Program) Bipolar Disorder: Harnessing Brain Plasticity for Improved Overall Outcomes
Transcript of Bipolar Disorder: Harnessing Brain Plasticity for Improved Overall … · 2019. 12. 17. · o n t r...

Husseini K ManjiGlobal Therapeutic Head
for NeuroscienceJohnson & Johnson
(previously Director of NIMHMood & Anxiety Disorders
Program)
Bipolar Disorder: Harnessing BrainPlasticity for Improved Overall Outcomes

Neuroscience Therapeutic Area
0 10 20 30 40
Mental Illness*
Injuries, including self-inflicted
Alcohol and drug use
Malignant neoplasms (cancer)
Cardiovascular disease
Respiratorydisease
Musculoskeletal disease
Sense organ disease
Digestive disease
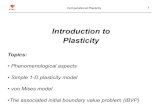
Serious Mental Illnesses are Major Causes of Disability Worldwide: GlobalBurden of Disease (DALYs)
(U.S., Canada, and Western Europe 15-44 years old)Disability-Adjusted Life Year (DALY)
Leading Individual Disease (DALY)
Disability-Adjusted Life Year (DALY)
Leading Disease Categories (DALY)
> 35,000 deathsby suicideannually in theUS
Mental Illness* 1. Unipolar Depression
1

Mood Disease Area Strategy
The unmet need is tremendous: why has thedevelopment of better treatments been so slow?
2
Time
• Sheer complexity ofdiseases
• Higher order brain functiondifficult to modelpreclinically
• * Brain is “inaccessible”
• * Our classification system doesn’tdistinguish between subtypes
Arguably the most challenging field to come up withcompletely novel treatments
Up to 12 years
• Generally don’t know until you are intrials with hundreds of patients if itis going to work

33
Neuroscience (esp Psychiatry) is ready forbreakthroughs…………………………
Method of the year, 2010
Recent advances referredto as “the biggestbreakthroughs in
Psychiatry in 40 years”NIMH Director

4
Major mood disorders are among the mostheritable of ALL ILLNESSES
Tw
inP
rob
an
dw
ise
Con
cord
an
ce
72 44 82 103 268 377 433 629 639 906 45 36 259 424
n/Pairs
*Source data from “The Genetics of Complex Human Behaviors,” Science, Vol. 264, 17 June 1994
***
Parkinson’sDisease
BreastCancer
ChronicObstructivePulmonaryDisorder
Hypertension IschemicHeart Disease
Autism MajorMood
Disorders
4

5
“intervention to bring abouta positive change in
cortico-cortical connectivity”
Tremendous Advances in Neuroscience
MultimodalIntegration
MEG fMRIVisualizing plasticity
Neurogenesis
**
(A)
(B)
(C)
(D)

6
Severe Mood Disorders arise from abnormalities of synapticplasticity: not “too much/too little individual neurotransmitter”
Old Model
From Rick Huganir
Leading to completely novel treatments

7
Can we rapidly regulate synaptic plasticity by targeting AMPA & NMDAreceptor subunits? FASTER ONSET? MORE ROBUST?

Neuroscience Therapeutic Area
• Replicated in multiple studies• Same effects seen in BPD
Replicated with additional distinctmolecules
13%
35%
53%56%
71%
58%53%
62-65%
35%
40Minutes.
80Minutes
110Minutes
230Minutes
1Days
2Days
3Days
7Days
8Weeks
Ketamine Placebo Venlafaxine SSRIBupropion
Acute AntidepressantEffect of very low dose Ketamine*
PBO
Drug
Robust and Rapid Antidepressant Effects of Low Dose NMDAAntagonists in Treatment-Resistant Major Depression
Response rate at 1 day in this extremelyrefractory population > 8 weeks with
current Rx in non-refractory populations
8
*Zarate et al. Arch Gen Psychiatry 2006

9
1DiazGranadose et a.l JCP 2010
Baseline Scale Suicidal Ideation(SSI)
Minutes
-60 0 60 120 180 2400
2
4
6
8
10
12
Scale
for
Su
icid
alId
eati
on
(S
SI)
]
]
]
]
]
]
]
]
]
]
High SSI (>4) (n=10)Low SSI (<3) (n=23)
Acute Effect of very low doseKetamine on Suicidal Ideation1
NMDA Antagonists Exert Robust &Rapid Antisuicidal Effects
9
Tremendous Advances in Biomarkersto identify responders to Rx
Non-Resp
PostKet
PreKet
1.6
1.4
1.2
1.0
0.8
0.6
0.4
0.2
Responders
PostKet
PreKet
1.6
1.4
1.2
1.0
0.8
0.6
0.4
0.2
2Cornwell, Salvadore et al., Biol Psychiatry, In Press
?? Neuroactive cytokines
* *

10
Ketamine also exerts Rapid Antidepressant Effects inBipolar Depression in two independent studies
• Once again, a highlyrefractory population
• Had failed multipleprevious treatments
• Did not trigger manicepisodes

MIND AND BODY:
MOOD DISORDERSAFFECT
MULTIPLE ORGANSYSTEMS

12
CRP
SAAIL-6SAA
CRH
EPI / NE
CortisolNE
Proinflammatory state
Insulin Resistance
Inflammation
Hyperinsulinemia& dyslipidemia
MoodDisorders
?? Neuroactive cytokines
From PW Gold, 2008

13
Plasma levels ofIL-1β (A) and TNFa (B) fromuntreateddepressedsubjects with MDD(N=267) orbipolar disorder(N=166) andhealthy controls(N=207) fromLundbeck-sponsored trials
Jones, K.A., Thomsen, C.,Mol. Cell. Neurosci. (2012)

1414
Targeting Specific Neuroactive Cytokines Exerts Major Effects on Synaptic andNeural Plasticity (Not just Brain Inflammation)
Su
rfa
ce
Glu
R1
(%
Co
ntr
ol)
Untreated TNF
200
150
100
0
50
250TNF TreatedUntreated
Hz
(Fre
q.)
&p
A(A
mp
)
20
15
100
5
0
Untreated
TNFR1
Frequency Amplitude
*
*
Targeting Specific Neuroactive Cytokines Reverses DepressivePhenotype in Several Different Robust Models
REVERSAL OF DEPRESSIVE Sx
(C) IL6
Control
0.8
0.6
0.4
0.0
0.2
10
lL6 abs
*
REVERSAL OF DEPRESSIVE SYMPTOMS(A) IL 1b
Pre-1Ra
Pre-PBS
4030
20
010
90
50607080
Pre-Severe Stress Post-Severe Stress
CUS+1Ra
CUS+PBS
**##
DEPRESSIVE SYMPTOMS(B) NFkB
0
50
300
100
150
200
250
CTRL
*
CUS
#
SC+CUS
Malenka et al
Duman, Russo and Nestler

15
Preliminary evidence suggests that targeting cytokines may bebeneficial in the treatment of mood disorders
Etanercept for depressive sx in psoriasis(Tyring et al, Lancet, 2006)
Infliximab in MDD (Change in CRP byresponder status; Raison et al 2013)

Genes
Manic-Depressive Illness (Bipolar Disorder and RecurrentDepression): targeting the Biology of Recurrence
EnvironmentalFactors
Pe
rce
nta
ge
of
Tim
eIll
Mania Depression0
5
10
15
20
25
30
35
(4.53x) (2.47x)
Before Li+
After Li+
~6X reduction insuicide
Molecules whose “job” it is to helpnerve cells grow & survive

17
Nestler et al, Nature NeuroscienceDrevets et al Nature, 1997
Recurrent Mood Disorders are Not Classical NeurodegenerativeDisease, but Have Atrophic Changes in Discrete Brain Regions
Mood Disorders
Control
PFC
volu
me
(m
m3
)
Control Bipolar Unipolar
300
200
100
0
*
*
~40%reduced grey
matter insubgen PFCx
17

Neuroscience Therapeutic Area
Control
Chronic lithium robustly regulates regional Bcl-2 levels
Lithium
Anterior Cingulate
Dentate Gyrus
Striatum
In animal studies,increasing Bcl-2protects against:
StrokeAlzheimer’s toxinsParkinson’s toxinsStress-induced damageFree radicals
?? Human data

19
A genetic variant associated with Bipolar Susceptibility &Antidepressant Response has major effects on Bcl-2 ProteinLevels, Susceptibility to “cell death” & Gray Matter Volumes
GG >> AA VentralStriatum Gray Matter
Gray Matter VolumeBcl-2 Protein Levels
**
Bcl-
2P
rote
inLevel
(%
of
GG
)
AA AG GG
200
150
100
0
50
Apoptosis
THAPS
Ap
op
toti
cC
ell
s(%
)
45
0
40
35
30
25
20
15
10
5
AA0 1 5
AG0 1 5
*
**
GG0 1 5

Neuroscience Therapeutic Area
Atrophic neurons
Reversal ofatrophy
Lithium – via its effects on “neurotrophic molecules”appears to enhance neuronal resilience
20
Hippocampal volume PFCx volume: in px only

21
Increasing levels of keyneurotrophic molecules increases
resilience & enhances recovery
Reducing levels of key neurotrophicmolecules reduces resilience &
increases susceptibility
Mice Developing Depressive Symptoms (%)
Normal Bcl-2
Lower Bcl-2
Normal BAG-1 levels
High BAG-1 levels
Dep
ressiv
eP
hen
oty
pe
30
20
10
0
Day1
Day3
Day8
Day2
RapidRecovery
RemainDepressed
*
21
100
Depressed
*Non-
Depressed
40
10
0
60
50
30
20
70
90
80

22
tBid Bcl-2
Dep
ressiv
eP
hen
oty
pe
Similar effects seen in5 different models
without toxicity
*
InducedPhenotype
LL44 Bl-2A7
60
0
50
40
30
20
10
Saline
Scrambled
Active
22
Does enhancing neurotrophic function enhanceresilience and recovery?

We need holistic solutions not just pills: we are dealingwith individuals with ‘real lives ’, not isolated neurons!
Software basedcognitive remediation
Patient ManagementPrograms
Treat underlyingBiology plus….
Remote monitoring topre-empt relapses
Y Interventions toengage appropriateexperiential circuitry

Neuroscience Therapeutic Area
Severe Mood Disorders: Unique Challenges
• Serious mental illnesses are the most disabling and costlydisorders globally; mood disorders the highest
• Targeting synaptic plasticity and cellular resilience hasthe potential for markedly improved treatments
• Move the paradigm to “pre-emption” – prevent theravages of the illness
• We need to move beyond the notion of single magicbullets and develop holistic, integrated solutions thatmake a real difference in patients’ lives
• This is a shared societal responsibility – we are only goingto succeed by working together
“There is no health without mental health”