
biostatistic methods for medicals
74
Stat 538 Biostatistical Methods I for Public Health and Medical Sciences Lecture 1 Michele Guindani University of New Mexico Albuquerque Fall 2009
-
Upload
oyetola-ajayi -
Category
Documents
-
view
20 -
download
0
description
statistics
Transcript of biostatistic methods for medicals

Stat 538Biostatistical Methods I
for Public Health and Medical Sciences
Lecture 1
Michele Guindani
University of New MexicoAlbuquerque
Fall 2009
General information about the class
Instructor: Michele GuindaniOffice: Humanities 441Phone: 277–2564email: [email protected] Hours: TuTh 15:30-17:00 or
by appointment
T.Assistant: Yon LingOffice: Humanities 345Phone: 505-277-5250email: [email protected] Hours: TBA
Classes T & R 9:30-11:30 SOM 2
Website http://www.math.unm.edu/ michele/Teaching/Bio538/bio538.html

Resources.
Textbook:Basic and Clinical Biostatistics (4th ed)by Beth Dawson and Robert G. Trapp.+ Also available at Accessmedicine.
+ Lecture notes by Ron Schrader, EdBedrick, et al. (on the class website)
Software: Minitab 15
. http://estore.e-academy.com/
6 Months Rental Ü $29.99 USD
12 Months Rental Ü $ 49.99 USD

Resources.
Textbook:Basic and Clinical Biostatistics (4th ed)by Beth Dawson and Robert G. Trapp.+ Also available at Accessmedicine.
+ Lecture notes by Ron Schrader, EdBedrick, et al. (on the class website)
Software: Minitab 15
. http://estore.e-academy.com/
6 Months Rental Ü $29.99 USD
12 Months Rental Ü $ 49.99 USD

Another useful free resource (but be careful!)...
Wikipedia, the free encyclopedia
For example, let’s checkhttp://en.wikipedia.org/wiki/Biostatistics

Another useful free resource (but be careful!)...
Wikipedia, the free encyclopedia
For example, let’s checkhttp://en.wikipedia.org/wiki/Biostatistics

What is statistics ?

What is statistics ?

What is statistics ?

What is statistics ?
} There are three kind of lies:lies, damned lies and statistics! ~

What is statistics ?
} Statistics is the science of under-standing data and of making decisionin the face of variability and uncer-tainty.~
}The discipline of Statistics hasevolved in the response to the needsof scientists and others whose dataexhibit variability.The concepts and methods of statis-tics enable the investigator to de-scribe variability and to plan re-search so as to take variability intoaccount.~

What is statistics ?
} Statistics is the science of under-standing data and of making decisionin the face of variability and uncer-tainty.~
}The discipline of Statistics hasevolved in the response to the needsof scientists and others whose dataexhibit variability.The concepts and methods of statis-tics enable the investigator to de-scribe variability and to plan re-search so as to take variability intoaccount.~

What’s the aim of this course ?
+ We’ll study Statistics in order to be able to
understand/read/implement
the statistical concepts and methods commonly used in thescientific research proper of our field (biomedical research,epidemiology, ...)

What’s the aim of this course ?
+ We’ll study Statistics in order to be able to
understand/read/implement
the statistical concepts and methods commonly used in thescientific research proper of our field (biomedical research,epidemiology, ...)
Ex: Interpretation of diagnostic test results.
o A common test for AIDS is the ELISA test.
m When a person carries the virus, the test is positive 97.7% ofthe time.
m When a person does not carry the virus, the test is negative92.6% of the time.
m About 0.5% of the American population carries the virus.
I What’s the probability that a randomly selected individualwould test positive ?
I What’s the probability that a person carries the virus if he/shetests positive twice?
I Would the diagnosis change when the person has some knownrisk factor?

Ex: Interpretation of diagnostic test results.
o A common test for AIDS is the ELISA test.
m When a person carries the virus, the test is positive 97.7% ofthe time.
m When a person does not carry the virus, the test is negative92.6% of the time.
m About 0.5% of the American population carries the virus.
I What’s the probability that a randomly selected individualwould test positive ?
I What’s the probability that a person carries the virus if he/shetests positive twice?
I Would the diagnosis change when the person has some knownrisk factor?

Ex: Interpretation of diagnostic test results.
o A common test for AIDS is the ELISA test.
m When a person carries the virus, the test is positive 97.7% ofthe time.
m When a person does not carry the virus, the test is negative92.6% of the time.
m About 0.5% of the American population carries the virus.
I What’s the probability that a randomly selected individualwould test positive ?
I What’s the probability that a person carries the virus if he/shetests positive twice?
I Would the diagnosis change when the person has some knownrisk factor?

Ex: Interpretation of diagnostic test results.
o A common test for AIDS is the ELISA test.
m When a person carries the virus, the test is positive 97.7% ofthe time.
m When a person does not carry the virus, the test is negative92.6% of the time.
m About 0.5% of the American population carries the virus.
I What’s the probability that a randomly selected individualwould test positive ?
I What’s the probability that a person carries the virus if he/shetests positive twice?
I Would the diagnosis change when the person has some knownrisk factor?

Ex: Interpretation of diagnostic test results.
o A common test for AIDS is the ELISA test.
m When a person carries the virus, the test is positive 97.7% ofthe time.
m When a person does not carry the virus, the test is negative92.6% of the time.
m About 0.5% of the American population carries the virus.
I What’s the probability that a randomly selected individualwould test positive ?
I What’s the probability that a person carries the virus if he/shetests positive twice?
I Would the diagnosis change when the person has some knownrisk factor?

Ex: Human Papillomavirus study – Souza et al., 2007
l The authors are interested in the relationship betweena risk factor and the occurence of a given outcome.

Ex: Human Papillomavirus study – Souza et al., 2007
l The authors are interested in the relationship betweena risk factor and the occurence of a given outcome.

Association of Oropharyngeal Cancer with Exposure to HPV
The odds ratio provides a way to look at risk in case-controlstudies.
OR =Odds that a person with an adverse outcome was at risk
Odds that a person without an adverse outcome was at risk
The OR is easy to compute when the observations are given in a2× 2 table:

OR =
“Proportion positives among casesProportion negatives among cases
”“
Proportion positives among controlsProportion negatives among controls
”=
57/10043/10014/200186/200
= 57×18643×14 = 17.61
I What does this mean? Is HPV a risk factor for OropharyngealCancer ?

Part I
Study designs in Medical Research


Classification of study designs.
l Study designs in medicine fall into 2 categories:
¬ Observational studies: one or more groups of patients areobserved, and characteristics about the patients are recordedfor analysis.
Experimental studies: involve an intervention – aninvestigator-controlled maneuver, such as a drug, a procedure,or a treatment – and interest lies in the effect the interventionhas on study subjects
+ Of course, both observational and experimental studies mayinvolve animals or objects, but most studies in medicine (andthe ones discussed most frequently in this class) involvepeople.

Classification of study designs.
l Study designs in medicine fall into 2 categories:
¬ Observational studies: one or more groups of patients areobserved, and characteristics about the patients are recordedfor analysis.
Experimental studies: involve an intervention – aninvestigator-controlled maneuver, such as a drug, a procedure,or a treatment – and interest lies in the effect the interventionhas on study subjects
+ Of course, both observational and experimental studies mayinvolve animals or objects, but most studies in medicine (andthe ones discussed most frequently in this class) involvepeople.

Classification of study designs.
l Study designs in medicine fall into 2 categories:
¬ Observational studies: one or more groups of patients areobserved, and characteristics about the patients are recordedfor analysis.
Experimental studies: involve an intervention – aninvestigator-controlled maneuver, such as a drug, a procedure,or a treatment – and interest lies in the effect the interventionhas on study subjects
+ Of course, both observational and experimental studies mayinvolve animals or objects, but most studies in medicine (andthe ones discussed most frequently in this class) involvepeople.

Classification of study designs.
l Study designs in medicine fall into 2 categories:
¬ Observational studies: one or more groups of patients areobserved, and characteristics about the patients are recordedfor analysis.
Experimental studies: involve an intervention – aninvestigator-controlled maneuver, such as a drug, a procedure,or a treatment – and interest lies in the effect the interventionhas on study subjects
+ Of course, both observational and experimental studies mayinvolve animals or objects, but most studies in medicine (andthe ones discussed most frequently in this class) involvepeople.




Case–Control Studies.
l Case– control studies begin with the absence or presence of anoutcome and then look backward in time to try to detectpossible causes or risk factors
l The cases in case–control studies are individuals selected onthe basis of some disease or outcome
l The controls are individuals without the disease or outcome.
l The history or previous events of both cases and controls areanalyzed in an attempt to identify a characteristic or riskfactor present in the cases’ histories but not in the controlshistories.The are also colled retrospective studies and are longitudinalin nature (the analysis spans a certain period of time)



Advantages of case–control studies
l Case–control studies are appropriate for studying rare diseasesor events, for examining conditions that develop over a longtime, and for investigating a preliminary hypothesis;
l Quick and inexpensive; ideal for obtaining and analyzingpreliminary data;
l Good also if someone needs to complete a clinical researchproject in a specific amount of time.

Disadvantages of Case–Control Studies
l Possible biases or errors;
l They depend completely on high-quality existing records(require often compromise between what researchers wish tostudy and what they are able to study.
l One of the greatest problems in a case–control study isselection of an appropriate control group. The cases in acase–control study are relatively easy to identify, but decidingon a group of persons who provide a relevant comparison ismore difficult.
Some statisticians have recommended the use of two controlgroups: one control group similar in some ways to the cases(eg, having been hospitalized during the same period of time)and another control group of healthy subjects.
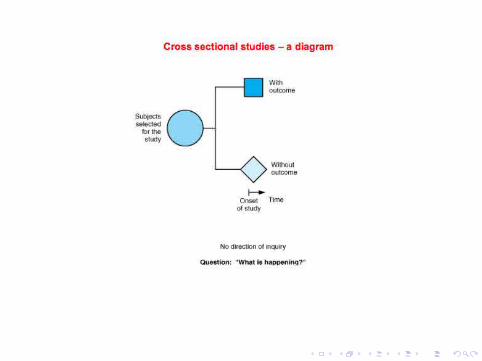
Cross-sectional (surveys, epidemiologic , prevalence)studies
l Cross-sectional studies analyze data collected on a group ofsubjects at one time rather than over a period of time.
l Cross-sectional studies are designed to determine “What ishappening?” right now.
Subjects are selected and information is obtained in a shortperiod of time. Because they focus on a point in time, theyare sometimes also called prevalence studies. Surveys andpolls are generally cross-sectional studies.


Advantages & Disadvantages of Cross-Sectional Studies
l Best for determining the status quo of a disease or condition,such as the prevalence of HIV in given populations, and forevaluating diagnostic procedures.
l Quick to complete, and relatively inexpensive.
l But they provide only a ”snapshot in time” of the disease orprocess (can be misleading).
Ex: Framingham cohort study showed that patients who werefollowed over a period of several years were observed to haveincreased diastolic blood pressure as they grew older (Gordonet al, 1959).Before, clinicians used to believe that diastolicblood pressure, unlike systolic pressure, does not increase aspatients grow older. This belief was based on cross-sectionalstudies that had shown mean diastolic blood pressure to beapproximately 80 mm Hg in all age groups.

Disadvantages specific to surveys
l A common problem with survey research is obtainingsufficiently large response rates; many people asked toparticipate in a survey decline. The conclusions are thereforebased on a subset of people; is this subset representative ofthe entire population?.
The problem of representative participants is common toother studies whenever subjects are selected or asked toparticipate and decline or drop out.
l Another issue is the way questions are posed to participants; ifquestions are asked in a leading or emotionally inflammatoryway, the responses may not truly represent the participants’feelings or opinions.

Cohort Studies
l A cohort is a group of people who have something in commonand who remain part of a group over an extended time.
In medicine, the subjects in cohort studies are selected bysome defining characteristic (or characteristics) suspected ofbeing a precursor to or risk factor for a disease or healtheffect.
l Cohort studies ask the question ”What will happen?” andthus, the direction in cohort studies is forward in time.Researchers select subjects at the onset of the study and thendetermine whether they have the risk factor or have beenexposed. All subjects are followed over a certain period toobserve the effect of the risk factor or exposure.Because the events of interest transpire after the study isbegun, these studies are sometimes called prospective studies.



Advantages & Disadvantages of Cohort Studies
l They are usually implemented to study the causes of a condition, thecourse of a disease, or the risk factors because they are longitudinal andfollow a group of subjects over a period of time.
l In well-designed cohort studies, investigators can control many sources ofbias related to patient selection and recorded measurements.
l But, they may require many years to be completed.
l Extended time periods make such studies costly.
l They also make it difficult for investigators to argue causation becauseother events occurring in the intervening period may have affected theoutcome.
l Cohort studies that require a long time to complete are especiallyvulnerable to problems associated with patient follow-up, particularlypatient attrition (patients stop participating in the study) and patientmigration (patients move to other communities). This is one reason thatthe Framingham study, with its rigorous methods of follow-up, is such arich source of important information.


Case–control vs cohort studies
l Both case–control and cohort studies evaluate risks andcauses of disease, and the design an investigator selectsdepends in part on the research question.
l Results from a well-designed cohort study generally carry moreweight in understanding a disease than do results from acase–control study.
l In fact, a large number of possible biasing factors can play arole in case–control studies.
However, case–control studies are frequently used in medicineand can provide useful insights if well designed. They can becompleted in a much shorter time than cohort studies and arecorrespondingly less expensive to undertake. Case–controlstudies are especially useful for studying rare conditions ordiseases that may not manifest themselves for many years.


Experimental Studies – Clinical trials
l Recall: Experimental studies involve an intervention – aninvestigator-controlled maneuver, such as a drug, a procedure,or a treatment – and interest lies in the effect the interventionhas on study subjects
l They are generally easier to identify than observational studiesin the medical literature.
l Authors of medical journal articles reporting experimentalstudies tend to state explicitly the type of study design usedmore often than do authors reporting observational studies.
l Experimental studies in medicine that involve humans arecalled clinical trials because their purpose is to drawconclusions about a particular procedure or treatment.

Statement of the research questions
l The first step in performing a clinical trial is to formulate themajor research question.
l This question, usually referred to as the hypothesis, is refinedto determine important study parameters, for example,
I the types of interventions to be compared,
I the nature of the outcomes to be assessed,
I the number of subjects in each treatment group,
I and the eligibility requirements for enrollment.

Statement of the research questions
l The first step in performing a clinical trial is to formulate themajor research question.
l This question, usually referred to as the hypothesis, is refinedto determine important study parameters, for example,
I the types of interventions to be compared,
I the nature of the outcomes to be assessed,
I the number of subjects in each treatment group,
I and the eligibility requirements for enrollment.
Statement of the research questions
l The first step in performing a clinical trial is to formulate themajor research question.
l This question, usually referred to as the hypothesis, is refinedto determine important study parameters, for example,
I the types of interventions to be compared,
I the nature of the outcomes to be assessed,
I the number of subjects in each treatment group,
I and the eligibility requirements for enrollment.

Statement of the research questions
l The first step in performing a clinical trial is to formulate themajor research question.
l This question, usually referred to as the hypothesis, is refinedto determine important study parameters, for example,
I the types of interventions to be compared,
I the nature of the outcomes to be assessed,
I the number of subjects in each treatment group,
I and the eligibility requirements for enrollment.

Statement of the research questions
l The first step in performing a clinical trial is to formulate themajor research question.
l This question, usually referred to as the hypothesis, is refinedto determine important study parameters, for example,
I the types of interventions to be compared,
I the nature of the outcomes to be assessed,
I the number of subjects in each treatment group,
I and the eligibility requirements for enrollment.

Statement of the research questions
l The parameter that is measured that will provide the answerto the most important question of the clinical trial is calledthe primary end point.
l When determining the primary end point, clinical researchersmust consider the following questions:
1. Which end points are most important clinically?
2. Which end points can be measured in a reasonably unbiasedmanner?
3. What practical constraints exist, such as population size,financial resources of the research study, and ability to followpatients on a long-term basis?

Statement of the research questions
l The parameter that is measured that will provide the answerto the most important question of the clinical trial is calledthe primary end point.
l When determining the primary end point, clinical researchersmust consider the following questions:
1. Which end points are most important clinically?
2. Which end points can be measured in a reasonably unbiasedmanner?
3. What practical constraints exist, such as population size,financial resources of the research study, and ability to followpatients on a long-term basis?

Clinical trials with/without control
l Clinical trials fall into two categories: those with and thosewithout controls.
l Controlled trials are studies in which the experimental drug orprocedure is compared with another drug or procedure,sometimes a placebo and sometimes the previously acceptedtreatment.
l Uncontrolled trials are studies in which the investigators’experience with the experimental drug or procedure isdescribed, but the treatment is not compared with anothertreatment, at least not formally.
l Controlled studies are viewed as having far greater validity inmedicine than uncontrolled studies.


Trials with Independent Concurrent Controls
l A trial can be controlled by having two groups of subjects:one that receives the experimental procedure (theexperimental group) and the other that receives the placeboor standard procedure (the control group).
The experimental and control groups should be treated alikein all ways except for the procedure itself + plan interventionsfor both groups for the same time period in the same study(concurrent control).
l Researchers can design double-blind trials in which neithersubjects nor investigators know whether the subject is in thetreatment or the control group. When only the subject isunaware, the study is called a blind trial.

Randomized Clinical trials
l Another issue is how to assign some patients to the experimentalcondition and others to the control condition; the best method ofassignment is random assignment.
l With randomization, the determination of assignment to treatmentgroup is based on probability alone and is not influenced by thepreference of the physician or patient.
l The assignment to a treatment group for each patient isindependent of (not influenced by) the assignment for all otherpatients.
l The purpose of randomization is to achieve “equality” of baselinecharacteristics of treatment groups, so that the comparison oftreatments is considered fair. To assess the equality of thetreatment groups, demographic and prognostic factors may becompared between groups. If patients have been randomlyallocated, it is expected that the groups will be similar indemographic and prognostic features.

Block Randomization
l If we want to ensure that similar numbers of patients withcertain important prognostic characteristics are included ineach treatment group, we can account for that in therandomization process.
Suppose we want equal percentages of males and females ineach treatment group. We could then proceed with blockrandomization:
I The order in which the two treatments are assigned to groups of 4
patients of the same sex could be random: first 4 male patients
would be assigned to either the control or experimental group and
the 4 four males to the other group (same for females).
l The purpose of randomization in blocks of patients is toprotect against imbalanced treatment assignment (due to”luck of the draw”) with respect to prognostically importantpatient subgroups.

Block Randomization
l If we want to ensure that similar numbers of patients withcertain important prognostic characteristics are included ineach treatment group, we can account for that in therandomization process.
Suppose we want equal percentages of males and females ineach treatment group. We could then proceed with blockrandomization:
I The order in which the two treatments are assigned to groups of 4
patients of the same sex could be random: first 4 male patients
would be assigned to either the control or experimental group and
the 4 four males to the other group (same for females).
l The purpose of randomization in blocks of patients is toprotect against imbalanced treatment assignment (due to”luck of the draw”) with respect to prognostically importantpatient subgroups.

Block Randomization
l If we want to ensure that similar numbers of patients withcertain important prognostic characteristics are included ineach treatment group, we can account for that in therandomization process.
Suppose we want equal percentages of males and females ineach treatment group. We could then proceed with blockrandomization:
I The order in which the two treatments are assigned to groups of 4
patients of the same sex could be random: first 4 male patients
would be assigned to either the control or experimental group and
the 4 four males to the other group (same for females).
l The purpose of randomization in blocks of patients is toprotect against imbalanced treatment assignment (due to”luck of the draw”) with respect to prognostically importantpatient subgroups.


Ethical Issues Concerning Clinical Trials
l The investigator who contemplates entering a patient into a randomizedclinical trial is faced with several ethical dilemmas.
l Is the method of the randomized clinical trial ethically acceptable? Acaregiver should prescribe the optimal treatment for a patient; if aclinician has thinks a treatment is superior, shouldn’t the patient beoffered that treatment?
l The clinical trial must be conducted as most ethically as possible:
1. None of the treatment options included in a randomized trial should beknown to be inferior to another treatment option based on previousrandomized studies (a standard treatment regimen should be used as thecontrol).
2. The trial should address a question that is of clinical importance and forthe sake of future health patients
3. Patients should be informed in understandable language about alltreatment options, the risks and benefits of participation, and the natureof randomization.





Meta Analysis and Review Papers
l Meta Analysis is neither observational nor experimental;
l Meta-analysis uses published information from other studiesand combines the results so as to permit an overallconclusion.
Meta-analysis is similar to review articles, but additionallyincludes a quantitative assessment and summary of thefindings. studies or experiments is called meta-analysis.
l Meta-analysis can be done for observational studies orexperiments; however, it should report the findings for thesetwo types of study designs separately.
l This method is especially appropriate when the studies thathave been reported have small numbers of subjects or come todifferent conclusions.



![TRAINING PROGRAMME POST HARVEST HACCP PROCEDURES … · , Sanitation [SOP’s & SSOP’s, Medicals, Pest Control, Records [ shipping, temperature, quality control etc.] Conduct Quality](https://static.fdocuments.net/doc/165x107/5ec002bbd00dd6062c127cb2/training-programme-post-harvest-haccp-procedures-sanitation-sopas-ssopas.jpg)















