Biomolecular Aspects of Flexor Tendon Healing
60
Transcript of Biomolecular Aspects of Flexor Tendon Healing

������������������� �����
����� �����
���������� �������������� ������������������� ������� ����������������������������
��������� �������������� ������������
���������� !"#
�$$"�%&�%'&()&�$�"�*+,'*%'���'++&('(� �-�.�-�-��-��/�'%()0)�

����������������������� ������� ��������������������������������������������������������������� ��!������ ��������"!��������#���$��%�&�����&'(&)�*���!���������*������*+!����!��,-�������*�#������.��"!�����������/�����������������0/����!�
��������
1��������#��%�&���1������������������*�-�����"���2������������ ����������� ��������������������� �������������� ������������������� �������� ������������������������)����)3����� ���������014�35673&7))�755$%7%�
-���������� ��������8�����*��!��!���,��������/����!�������������������������!�������������!�������� ��.� ��� ��� ������ *�� ��!� �!���**������� ������������� ������� ��������*�!��!��!�����*��������!������������������������������������������������������/��!��!����*�������������� ��������������*������"!������*� �!��������� �!�����/��� ��!��������8������*������!�������*�����������!�������!���!�����!�������������� ����������������������������*�����������������������������!��������*��������
"!�������������������������*�����������**�����*����!���������������������������!�����������*����������������*�������/�!�*����79&�����������������**������/��������*���������������������������������/���������*��!��*������������ ����������!���������������������������
�*���������������������:�����������*��!��*�������������!�*�����������������������*��� ����� �� �� ����� ���� ��������� +���������� /���� ��������� ��������� /��!� �!�� ������������� *� ������� �� �������� �!������ *� �!�� ��*������� ����*����� ��/�!� *����79&/!��!� /��� ��������� ��������� ������ �!�� *����� �/� /����� �*���� ������� �� ���� ������� �����������������������!���!���!���1�!�������������!��������/�!�*��������������*����������/�!�*�������4��������������������������������������/!�����������7�������/�!�*����7&��������� ������ �� �!�� !������ �������� ���������� �������� ���*������ �**����� *� �������������� ��������� ���� ������!� �!���!� ����������� �����������*��������� ���������!�����
#��������������������7&'���4�����������������������������!��!�����!��������!���!��/!������ �!����/�������� �������� ��������*����������������������7'���4�� ������;���������������������������*�������������*��!���������*���*�����������������������������������������������*���������!��!����������������������������*��!����*���������*��������7���������7��������������!/���
���� ����-���������!�������<�/�!�*������#���������������=�������+���������#�*����������2����������!�����#��������
�� ����� ����� �!������ �� � �"#������#���$�#����� �������������� ���� ��%&'()*(������� �������
>�#�����1�������%�&�
�004�&$)&7$%�$�014�35673&7))�755$%7%��(�(��(��(����7&%�'���,!���(??��������?������@��A��(�(��(��(����7&%�'��.

To my family


List of Papers
This thesis is based on the following papers, which are referred to in the text by their Roman numerals.
I Berglund M, Wiig M, Torstensson,M, Reno C, Hart D. Assess-
ment of mRNA levels for matrix molecules and TGF-�1 in rab-bit flexor and peroneus tendons reveals regional differences in steady-state expression.
Journal of Hand Surgery, 2004; 29B:165-169
II Berglund M, Reno C, Hart D, Wiig M. Patterns of mRNA ex-pression for matrix molecules and growth factors in flexor ten-don injury: differences in the regulation between tendon and tendon sheath.
Journal of Hand Surgery, 2006; 31A:1279-1287
III Berglund M, Hart D, Wiig M. The inflammatory response and hyaluronan synthases in the rabbit flexor tendon and tendon sheath following injury.
Journal of Hand Surgery, 2007; 32E:581-587
IV Berglund M, Hart DA, Reno C, Wiig M. Growth factor and pro-tease expression during different phases of healing after rabbit deep flexor tendon repair.
Submitted.
V Berglund M, Hildebrand KA, Zhang M, Hart DA, Wiig M. Neuropeptide, mast cell and myofibroblast expression after rab-bit deep flexor tendon repair.
Submitted.
Reprints were made with permission from the respective publishers.
Cover by Yvonne van den Berg and Michel Danckaarts.


Contents
Introduction ................................................................................................... 11 Anatomy and biology of flexor tendons ................................................... 12
The flexor tendon in the human hand .................................................. 12 Vasculature and nutrition of flexor tendons ........................................ 13 Components of tendon tissue ............................................................... 14 Tendon and load .................................................................................. 16 Phases of the healing process .............................................................. 16 Extrinsic and intrinsic healing ............................................................. 17
Current clinical practice ........................................................................... 18 Flexor tendon rupture versus adhesion formation ............................... 18 Flexor tendon repair ............................................................................. 19 Rehabilitation protocols ....................................................................... 20
Factors affecting tendon healing .............................................................. 21 Experimental models ................................................................................ 24
Cell culture versus animal model ........................................................ 24 Choice of species ................................................................................. 24 The clinical trial ................................................................................... 24
Aims .............................................................................................................. 25
Methods ........................................................................................................ 26 Animals .................................................................................................... 26 Intra- and extrasynovial tendons .............................................................. 26 Flexor tendon injury model ...................................................................... 27 Extraction of RNA ................................................................................... 28 Semiquantification of mRNA ................................................................... 29 Immunohistochemistry ............................................................................. 30 Statistical analysis .................................................................................... 31
Results and discussion .................................................................................. 32 Study I. Differences between intra- and extrasynovial tendons ............... 32 Study II. Matrix molecules and growth factors after tendon repair.......... 33 Study III. Inflammatory molecules and hyaluronan synthases after tendon repair ........................................................................................................ 36 Study IV. Growth factors and proteases in healing flexor tendon and sheath ........................................................................................................ 38

Study V. The myofibroblast-mast cell-neuropeptide fibrosis pathway in flexor tendon healing ................................................................................ 41
Conclusions ................................................................................................... 44
Future prospects ............................................................................................ 45
Summary in Swedish – sammanfattning på svenska .................................... 46 Molekylärbiologiska aspekter på böjsenläkning ...................................... 46
Acknowledgements ....................................................................................... 48
References ..................................................................................................... 49

Abbreviations
�-SMA �-smooth muscle actin ANOVA Analysis of variance bFGF Basic fibroblast growth factor cDNA Complementary deoxyribonucleic
acid COX-2 Cyclooxygenase-2 CTGF Connective tissue growth factor DIP Distal interphalangeal joint FDP Flexor digitorum profundus FDS Flexor digitorum superficialis GAGs Glycosaminoglycans HAS Hyaluronan synthase IGF-1 Insulin-like growth factor-1 IL-1� Interleukin-1� iNOS Inducible nitric oxide synthase MMP Metalloproteinase mRNA Messenger ribonucleic acid NGF Nerve growth factor PIP Proximal interphalangeal joint ROM Range of motion RNA Ribonucleic acid RT-PCR Reverse transcription polymerase
chain reaction SD Standard deviation SE Standard error of the mean SLRPs Small leucine-rich proteoglycans SP Substance P TGF-�1 Transforming growth factor-�1 TIMP Tissue inhibitor of metalloproteinase TNF-� Tumor necrosis factor-� VEGF Vascular endothelial growth factor VBP Vinculum brevis profundus VBS Vinculum brevis superficialis VLP Vinculum longus profundus VLS Vinculum longus superficialis


11
Introduction
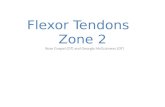
Although less than 1% of hand trauma in the emergency unit is primarily flexor tendon injuries 61, the age and activity level of the affected patients and the time needed for rehabilitation lead to high costs for both society and the afflicted individual 129. The potential severity of the injury is well illu-strated by the view on flexor tendon injuries only a few decades ago. The injured skin, subcutaneous tissues and tendons were regarded as one conti-nuous scar, in which nothing could be gained by primary (direct) repair of the severed tendon. Zone II (Figure 2) was referred to as “no man’s land”. The results of primary repair were so poor that primary complete removal of the injured tendon followed by a later secondary procedure with free tendon grafting was general practice 23. The first reports of successful primary repair are from the 1960s 163. Today, with improved surgical techniques, rehabilita-tion protocols 4, 72, 90, 145, 146 and new insights into the healing capacity of flexor tendon tissue 48, 96, 98, 102, 103, the results and prognosis are all vastly improved. However, despite these improvements, a deep flexor tendon in-jury may still lead to impaired function with a decreased range of motion (ROM) because of adhesion formation (scarring between bone, tendon and tendon sheath) or tendon ruptures 146, 151.
Figure 1. Knife injury to the volar aspect of the hand, with laceration of the deep and superficial flexor tendons of the index and little finger.

12
Figure 2. The zones of the flexor tendons in the hand.
Anatomy and biology of flexor tendons The flexor tendon in the human hand The human hand is capable of finely coordinated movements. Flexion of the fingers is motored by the deep and superficial flexor muscles, innervated by the median nerve (superficial flexor muscle, and deep flexor to index and middle finger) and the ulnar nerve (deep flexor to ring and little finger). The muscles power the deep (flexor digitorum profundus, FDP) and superficial (flexor digitorum superficialis, FDS) tendons, of which the deep flexor ten-don is the most critical to the ROM for the finger, attaching at the base of the distal phalanx and flexing both the proximal (PIP) and distal (DIP) interpha-langeal joints. The superficial tendon is divided into two halves at the level of the proximal phalanx, attaching separately at the proximal part of the middle phalanx, flexing the PIP joint at activation. The thumb, having only

13
one interphalangeal joint (IP), has one flexor muscle and tendon – the polli-cis longus 20. Between the muscle/tendon interface and the FDP insertion at the distal pha-lanx, the surroundings of the FDP change and have been divided into five anatomical zones (Figure 2). In zone I and II, the tendon is surrounded by a fibro-osseous digital sheath, creating a gliding surface for the excursion of the tendons (visceral paratenon on the tendons and parietal paratenon on the inner side of the sheath). The sheath is reinforced by a pulley system (Figure 3) with annular and cruciform pulleys. The annular pulleys give stability and prevent bowstringing of the flexor tendon 20, 41.
Figure 3. The tendon sheath with the annular (A1-A4) and cruciform (C1-C3) liga-ments 20. (With permission from Elsevier.)
Vasculature and nutrition of flexor tendons The arteries supplying part of the nutrition to the flexor tendons are the vin-culum longus superficialis (VLS) at the proximal phalanx, and brevis super-ficialis (VBS) and longus profundus (VLP) at the PIP joint. Vinculum brevis profundus (VBP) is the most distal (Figure 4) 20. The flexor tendons are poorly vascularized, especially between the A2 and A4 pulleys in the volar segments of the tendon, earlier even deemed avascular 97 but now known to have a low vascular density 57. In these areas, they are more dependent on diffusion, i.e. their second source of nutrition. Diffusion of nutrients is sup-plied via the parietal paratenon in the tendon sheath 49, 99.

14
Figure 4. The vasculature of the deep and superficial flexor tendons, with the distri-bution on the palmar (i.e. volar) and dorsal aspect of the tendon 20. (With permission from Elsevier.)
Components of tendon tissue Collagens Tendons are hypocellular dense connective tissues that are composed mainly of collagen (65-80% of tendon dry weight). Soluble tropocollagen molecules are connected to each other by cross-links, becoming insoluble and aggregat-ing into microfibrils, and then fibrils. A collagen fiber, the smallest collagen structure visible with light microscopy and constituting the basic unit of the tendon, is a bundle of collagen fibrils. The fibers are bound together by en-dotenon, a thin connective tissue layer containing nerves and blood vessels, creating primary fiber bundles (subfascicles) that aggregate into secondary bundles (fascicles). Tertiary bundles are groups of collagen fascicles, that in their turn aggregate into the tendon, which is surrounded by the epitenon (Figure 5). The collagen in adult tendons is mainly type I. Apart from the collagen fibers, whose linear arrangement creates a resistance to external forces, the tendon tissue also, to a varying extent, contains elastin fibers (1-2% of tendon dry weight) that contribute to the tendons elastic properties 70.

15
Figure 5. Tendon anatomy with the structure of collagen fibers, as illustrated by Kannus 70.
Extracellular matrix with proteoglycans The collagen and elastin fibers are surrounded by the hydrophilic gel-like ground substance, together forming the extracellular matrix. The ground substance, consisting mainly of water (60-80%), also contains glycosami-noglycans (GAGs), proteoglycans and glycoproteins. GAGs and proteogly-cans contribute to the resistance of tendons to compressive forces through their high water-binding capacity, adding to the elastic properties of the tis-sue 70.
There are two types of proteoglycans in tendon tissue: small leucine-rich proteoglycans (SLRPs) and large proteoglycans (also called modular pro-teoglycans or lecticans) 181. The SLRPs (decorin, biglycan, fibromodulin and lumican) regulate the assembly of collagen, i.e. the fibrillogenesis 123. Dis-turbances in the SLRP distribution can lead to changes in the structure of connective tissues and cause impaired function 37, 67. Some SLRPs can also act as modulators of certain growth factors by binding to them 132. Aggrecan, a large proteoglycan able to resist compressive forces, is more abundant in articular cartilage, but can also be found in tensile regions of tendons. The large proteoglycan versican influences cell proliferation and adhesion, is increased in patellar tendinosis 137 and may have additional functions in the extracellular matrix that are not yet known 172.
Tenocytes Although the tendon is hypocellular, it is a living tissue containing fibrob-lasts with a phenotype specifically adapted to their surroundings – tenocytes and tenoblasts. Tenocytes and tenoblasts constitute 90-95% of the cellular

16
elements of tendons, the remainder being mainly vascular cells and chondro-cytes at pressure and insertion sites 70. In the growing tendon, the majority of cells are tenoblasts that are active during growth and development, with a high synthesis rate of collagens, glycoproteins, proteoglycans and elastic fibers. The tenoblasts transform to tenocytes in the adult tendon, becoming elongated with long cellular processes to maintain contact between cells and matrix components in the aging tissue with a decreasing cell-to-matrix ratio 70. The lower metabolic rate contributes to the endurance of tendon tissues to periods of tensile load with a lower energy supply 161. Tenocytes are believed to play a role in chronic tendon diseases, exhibiting matrix degeneration before the onset of clinical symptoms 31.
Tendon and load Tendon tissue does not have set characteristics: matrix composition and turnover vary in different tendons that are subjected to varying loads 14, 78. The tenocytes can coordinate their response to load, communicating via gap junctions on the cytoplasmatic extensions that regulate their synthesis and adapt the tendon tissue to the forces it is subjected to 169.
In the same tendon, there can be regions with different characteristics. When a tendon passes through a pulley or is wrapped around bone, there is, instead of the usual tensile force, an increase in compressive and shear forces. To protect the integrity of the tendon (preventing wear and tear) the composition of the tendon tissue is altered in the exposed region. The seg-ment adopts a more fibrocartilaginous phenotype, giving it a higher resis-tance to compression. The tenocytes change their appearance, adopting a more chondrocyte-like rounded shape, collagen II increases and the architec-ture of the collagen fibers becomes less linear. There is a shift in proteogly-can production, with higher amounts of the large proteoglycan aggrecan, which can bind water and give more stiffness to the tissue 13, 113, 123, 126, 167, 168. Aggrecan can also be found in smaller amounts in the tensile regions of the tendon, but then appears to have a different structure 167.
The tendon response to load is dynamic. Increased compressive force will stimulate a fibrocartilaginous phenotype with more aggrecan and an elimina-tion of those forces will give the opposite effect 100, 127, 181. A certain amount of load is necessary for the steady state tissue homeostasis in the tendon, which, if deprived of tensile force, will begin to degrade 173.
Phases of the healing process The healing process in tendons is divided into three overlapping phases (in-flammatory, proliferative and remodeling phase) 66, 138, 146.

17
The inflammatory phase The mechanical trauma with transection of the tendon and the tendon sheath damages blood vessels in the tendon sheath and the surroundings, causing a hematoma. A number of factors are released at the injury site, stimulating vasodilatation and migration of inflammatory molecules. The number of macrophages, neutrophils, monocytes, erythrocytes and platelets increase in the area. There is an increase of various growth factors and tenocyte prolife-ration is initiated, leading to production of components of the extracellular matrix (such as collagens and proteoglycans) and stimulating angiogenesis. Apoptosis of tenocytes increases 179. The inflammatory phase dominates the first week after injury 66, 138, 146. The strength of the repair site relies only on the sutures and a fibrin clot 20.
The proliferative phase The production of collagen and other structural molecules begins a few days after the injury and continues during the first month. Tenocytes increase because of ongoing recruitment as well as proliferation. Collagen III, a large number of cells and high water content, are typical for the newly synthesized extracellular matrix 66, 138, 146. There is inhibitory signaling against tenocyte apoptosis within two to four weeks after tendon injury 179. The tendon repair gains strength when the ten-don gap is bridged by granulation tissue. However, the tendon callus lacks the properties of normal tendon and is characterized by a random collagen pattern with suboptimal mechanical properties 20. During the period of two to four weeks after tendon repair, the tendon is weak with a maximal risk of rupture 42, 151, 152.
The remodeling phase During the remodeling phase, beginning after the first month of tendon heal-ing and continuing until at least nine months after repair, a shift takes place from collagen III to collagen I production. The total cell number and produc-tion of components of the extracellular matrix decrease 66, 138, 146.
The collagen fibers reorganize into a more structured pattern with cross-linking and longitudinal orientation. The tendon now gains higher stiffness and tensile strength 20, 91.
Extrinsic and intrinsic healing Previously it was believed that extrinsic healing with formation of adhesions was a necessary process in flexor tendon healing, providing vital nutrients through the angiogenesis in the adhesions. The tendon was regarded as inert, lacking the ability to synthesize new tissue components for repair. The clas-sic studies by Lundborg 96, 98, which demonstrated the tendons capacity to

18
heal in an avascular synovial environment, completely deprived of adhesion formation, altered the view on tendon healing. The deep flexor tendon is a cellular active tissue in which intrinsic healing with migration and prolifera-tion of tenocytes contributes to the repair of the injury. There is diffusion of nutrients not only from the vascularized adhesions but also from synovial fluid.
We now know that both intrinsic and extrinsic healing mechanisms are needed for optimal tendon healing, and that the balance between them is vital for the final functional result. Excessive extrinsic healing with adhe-sions will decrease tendon excursion, causing an impaired function. The discovery of intrinsic healing has made it possible to counteract adhesion formation through primary repair with atraumatic surgical techniques and early rehabilitation 4, 46, 48, 66, 96, 99, 102, 103.
Current clinical practice Flexor tendon rupture versus adhesion formation The goal of repair and rehabilitation after flexor tendon injury is to achieve a mechanically strong tendon and a good ROM in the injured digit. Potential complications after flexor tendon repair are tendon rupture or tendon adhe-sion. In a review citing outcome reports of primarily repaired flexor tendon injuries, the worldwide rupture rate varied between 4 and 18% 151. To avoid these complications, the clinical treatment of flexor tendon injuries is a bal-ance between protecting and allowing excursion of the newly repaired ten-don. Whereas too much force will result in tendon rupture, insufficient train-ing or immobilization will promote adhesion formation and decreased ROM.
During the past few years, a number of clinical trials and animal models have investigated the strength of different repair techniques (number of su-ture strands, braided or unbraided suture, suture purchase of tendon tissue, type of peripheral suture, etc.), as well as the impact of different rehabilita-tion protocols (immobilization, passive or active training) on rupture rate and ROM 4, 146. There is a trend toward using a stronger four-strand suture me-thod in combination with active rehabilitation protocols 151. Early rehabilita-tion within the limits of the strength of the suture stimulates the healing of the repair site as well as the gliding surface, inhibiting the formation of ad-hesions 4.

19
Flexor tendon repair An atraumatic technique is essential when repairing a flexor tendon injury in order not to unnecessarily provoke adhesion formation. To quote Jin Bo Tang 151:
The outcomes of tendon surgery, particularly primary tendon repairs in the digital sheath area, depend upon the expertise of the surgeons. Therefore, another problem, even in countries with a sufficient number of hand surge-ons, is that these difficult procedures are often thought of as simply “sewing the ends together” by trainees or inexpert surgeons. Primary operation by an inexperienced surgeon can result in destruction of the tendon, sheath, and pulley structures and may render the delayed primary or secondary repairs in-effective, even when performed by an experienced hand surgeon.
Apart from not causing additional unnecessary trauma, compromising re-maining circulation and risking adhesions, optimal sutures with sufficient strength are needed to avoid ruptures. The time frame within which a direct repair of the injured tendon is feasible is not unlimited. When more than two weeks have passed since the injury, a two-stage procedure with tendon grafting may be considered. In an animal model, optimal results with im-mediate repair compared to repair after one to three weeks has been demon-strated 51.
The core suture A strong core suture is necessary to allow active rehabilitation. Many tech-niques are currently in use, with two-, four- or six-strand sutures 19, 130, 146,
149. Therefore, a general recommendation is to reach a strength of 40-50 N (4-5 kg force) to ultimate failure (i.e. the amount of load at which the ten-don reruptures) 4. The repair strength also depends on the tendon purchase, i.e. the amount of tendon tissue encompassed by the suture, which should be 7-10 mm on either side of the laceration 152. The effect of the purchase may not only be due to the amount of tissue in the suture area and the resulting grip on the tendon ends but also to the length of the suture material itself 76. However, when attempting to achieve optimal suture strength through mul-tiple strand sutures with extra tendon purchase, allowing a more active re-habilitation, it is important to be aware of the potentially negative impact the foreign material may have on the tendon. Specifically, this negative impact increases the work of flexion 5 and causes a degradation of tendon tissue with subsequent impaired mechanical properties, counteracting the desired effect 106, 176. The recognition of the superior strength of intact ten-don tissue compared with suture material, as well as the risk of additionally weakening the tissue through the added material, motivates the recommen-dation of only repairing tendon lacerations that sever 50% or more of the tendons cross-sectional area. A limited repair may be indicated if a smaller

20
laceration causes mechanical hindrance (triggering) of the tendon during excursion 20. Triggering may also occur if the annular pulleys are too tight for the excursion of repaired flexor tendon, decreasing the strength of the tendon repair, a complication that may be avoided by preoperatively venting the pulleys 24.
The circumferential suture The circumferential suture has two functions. First, it reduces the bulk of the tendon repair, allowing for easier tendon excursion through the tendon sheath and pulleys with less friction and resistance. Second, it can contribute to the strength of the tendon suture: biomechanical studies show enhanced maximal failure strength, especially with interlocking sutures 84, 140, 148 and a suture purchase of 4 mm 63.
Gap formation Gap formation, an increase in the distance between the sutured flexor tendon stumps during the first weeks of healing, may have an impact on the out-come of tendon repair. Previously, it was believed that even minimal gap formation had a negative influence on healing with increased adhesion for-mation 8, 9, 12, 140. Studies that are more recent have shown no such negative impact through gap formation less than 3 mm in length. Tendons with gaps greater than 3 mm, however, lack the increase in tensile strength at the repair site that usually occurs between four and six weeks postoperatively 52, 142. Gap formation of 2 mm changes the gliding resistance of the tendon, even risking triggering on the annular pulleys if as large as 3 mm. Thus, it is ad-visable to aim for a strong, carefully adapted repair to minimize gap forma-tion 184.
Rehabilitation protocols Post-surgical rehabilitation is a well-motivated health care investment. The increased complication rate that accompanies immobilization after flexor tendon repair causes higher cost for both society and the individual 129. A variety of protocols have been suggested, with different degrees of movement range that is either passive or to some extent active 6, 77, 90, 105, 143, 145. It is im-portant to avoid simultaneous extension at wrist and digits since the com-bined strain may exceed the strength of the core suture. Digital extension should therefore be combined with synergistic wrist flexion, and vice versa 88,
89. Earlier studies supported a tendon excursion of 3 to 5 mm during rehabili-
tation to counteract adhesion formation, but more recent experimental find-ings from animal models indicate that as little as 1.7 mm may be sufficient 141. Although there is now a trend toward more active rehabilitation protocols 151, it is not necessarily true that this promotes an increase in the strength of

21
the healing tendon tissue 17. The protocols currently in practice range from partially passive to active 4. However, as of yet, there are no randomized clinical trials with sufficient evidence to support a general recommendation to mainly use active protocols.
Factors affecting tendon healing Great advances in flexor tendon healing have been achieved through devel-oping suture techniques and rehabilitation protocols, but it is likely that progress has been maximized. Consequently, investigators now aim to influ-ence more directly the healing process on a biomolecular level 19, 66.
Growth factors Transforming growth factor-�1 (TGF-�1) contributes to the initial scar
tissue formation that is essential for wound healing. However, at later stages in the healing process an increased TGF-�1 activity may lead to excessive scarring, with subsequent fibrosis and adhesion formation 16, 79. TGF-�1 sti-mulates collagen III production in flexor tendon and tendon sheath tissue 80,
81 and inhibition of TGF-�1 after deep flexor tendon injury has reduced ad-hesions in animal models 11, 26, 28, 75, 185.
Connective tissue growth factor (CTGF, CCN2) is active in angiogene-sis, tissue repair and fibrosis 139. It mediates some of the profibrotic effects of TGF-�1 64, 108 and is active in fibrotic processes in diverse types of tissue 36,
119. Increased amounts of CTGF have also been seen in load-induced tendi-nopathy models 43, 110. Targeting CTGF has been suggested as one way of modulating the potential fibrotic effects of TGF-�1 in connective tissue 15.
Basic fibroblast growth factor (bFGF, FGF-2) is usually increased in acute connective tissue injuries, but down regulated in chronic wounds, such as pressure ulcers. It is involved in tissue remodeling, the formation of gra-nulation tissue and reepithelialization 10. Tenocytes increase their collagen production and proliferation in vitro when stimulated with bFGF 33, 150, 155, 171 and treatment of flexor tendon injuries with bFGF in animal models has in-creased the biomechanical strength of the healing tendon 55, 153. Aside from potentially decreasing the risk of rupture of the healing tendon through im-proved biomechanical properties, bFGF has been shown to increase gene expression of lubricin and hyaluronan synthase in vitro, which may have positive effects on tendon gliding 157.
Insulin-like growth factor-1 (IGF-1) has dose-dependent effects on ma-trix synthesis, including collagens, is a protector from apoptosis and stimu-lates cell proliferation and migration 1, 3, 33, 134. In animal models of tendinitis, treatment with IGF-1 has improved the outcome 34, 131.
Vascular endothelial growth factor (VEGF) stimulates collagen deposi-tion and angiogenesis, promoting the proliferation and migration of endo-

22
thelial cells 7, 10. Increased amounts of VEGF have been detected after cyc-lical loading of tendons, in tendinitis and in ruptured tendons 110, 122, 136. Treatment with VEGF has been positive in hypoxic environments (e.g. di-abetic wounds) 10. Attempts to optimize Achilles tendon healing with VEGF improved the tensile strength in the early healing period 182, but in vitro VEGF stimulation of canine tenocytes did not lead to an increase in collagen synthesis or cell proliferation 155.
Nerve growth factor (NGF), a neurotrophin previously thought to act on-ly on the peripheral nervous system, has been shown to improve wound heal-ing, stimulating angiogenesis and reinnervation 71, 111. When applied to heal-ing medial collateral ligaments in the knees of rats, it improved the biome-chanical properties and increased the vascularity and nerve density of the connective tissue 101.
Bone morphogenetic proteins (BMPs) stimulate synthesis of tendon tis-sue components and increase the biomechanical properties of repaired Achilles and patellar tendons in animal models 29, 166.
Platelet derived growth factor (PDGF-BB) stimulates tenocyte prolife-ration, synthesis of ECM components and has shown some positive effects on flexor tendon healing in canine models 155, 156, 170.
Cyclooxygenase-2 Inhibition of cyclooxygenase-2 (COX-2) has been found to limit the in-flammatory response after flexor tendon injury and subsequently diminished adhesion formation in animal models 85, 147. Healing rat Achilles tendon lace-rations have been shown to exhibit a smaller transverse area with undimi-nished failure load and increased tensile stress at failure after treatment with COX-2 inhibitors 44. However, they have also been shown to decrease the migration and proliferation of tenocytes 158. Furthermore, lacerated rat Achilles tendons treated with parecoxib or indomethacin in another study healed with decreased strength and stiffness 40. It has been suggested that COX-2 inhibitors may have negative effects on the tendon tissue during the first phases of healing, but improve biomechanical properties at a later re-modeling stage, inhibiting prolonged inflammatory responses 165.
Hyaluronan synthases There are three known hyaluronan synthases (HAS) in mammalian species, of which HAS2 synthesizes high molecular weight and HAS3 low molecular weight hyaluronan 65. Hyaluronan, an endogenous high molecular weight polysaccharide, is active in wound healing, angiogenesis, tumorigenesis and organization of the extracellular matrix 82, 86. Attempts have been made to improve flexor tendon healing and reduce adhesion formation by adding hyaluronan. However, both in vitro and in vivo studies (animal models and clinical studies) have shown contradictory results 54, 92, 109, 125, 174, 175, 186 that

23
may be due to different methods of delivery, varying concentrations and high versus low molecular weight hyaluronan.
Matrix metalloproteinases and their inhibitors The matrix metalloproteinases is a family of enzymes, designed to degrade components of the extracellular matrix, such as collagens and proteoglycans. The intricate balance between matrix metalloproteinases (MMPs) and the tissue inhibitors of metalloproteinases (TIMPs) is essential for the quality of connective tissues. Excessive amounts of MMPs may cause degradative conditions and a dominance of TIMPS can lead to fibrotic processes 118. When MMP inhibitors have been used in cancer treatment trials, an in-creased incidence of frozen shoulder and other musculoskeletal conditions have been noted 120. Moreover, in animal studies, systemic treatment with the MMP inhibitor doxycycline has weakened the rat Achilles tendon 116, emphasizing the importance of balance.
It is, however, tempting to manipulate the balance to improve the out-come of healing. After surgical tendon repair, there is commonly degrada-tion and weakening of the tissue surrounding the suture material, possibly caused by MMPs 106, 176. Sutures coated in the MMP inhibitor doxycycline have been shown to improve the suture-holding capacity of rat Achilles ten-dons 117.
The myofibroblast-mast cell-neuropeptide pathway Lately, a new pathway in fibrosis has been suggested. After connective tis-sue injury, mast cells increase in the area. The mast cells, reacting to the physical trauma 104 and also being directly stimulated to degranulate by neu-ropeptides 53, release a number of factors that are part of the first inflamma-tory stage of the healing process but also factors with potential profibrotic effects (e.g. TGF-�1) 53, 107. Thus, the mast cells are believed to induce a fibrotic response, activating fibroblasts and myofibroblasts in the connective tissue 53, 104, 162. The myofibroblast is a specialized fibroblast, recognizable by its expression of �-smooth muscle actin (�-SMA). The myofibroblast con-tains fibers allowing it to generate greater amounts of contractile force, alter-ing the character of the connective tissue 39. This is a necessary feature of wound contraction 38, but can cause morbidity when excessive, such as in Dupuytren’s contracture 30, 164.
Increased amounts of myofibroblasts, mast cells and neuropeptides have been found both in skin wound healing models and in joint contractures 58-60. Attempts to modulate this suggested profibrotic myofibroblast-mast cell-neuropeptide fibrosis axis with a mast cell stabilizer (such as ketotifen) have shown some promising results in a model of hypertrophic skin wound heal-ing 47.

24
Experimental models Cell culture versus animal model Cell cultures as a model to study tendons have been very valuable as a start-ing point for investigating the response of tenocytes to interventions (e.g. different mechanical forces and pressures or addition of growth factors) 74,
127, 155. It is, however, not practically possible to create a model of flexor tendon injury using cell cultures. To better mimic the clinical situation, ani-mal models have been necessary 66.
Choice of species Many species have been utilized in the study of flexor tendon injury and healing. These include chickens, mice, rabbits, canines and primates 24, 52, 56,
102, 176. In addition to the ethical issues that call for choosing the lowest poss-ible species, there are some practical considerations. A mouse model of flex-or tendon adhesion has lately been advocated 95, 177, 178, but to create a model that is similar to the repair of human deep flexor tendons in clinical practice, the tendon has to be of a certain size to allow for similar suturing techniques and biomechanical testing 66. Rabbit models have been used in a multitude of studies 3, 26, 56, 175, fulfilling the requirements of the lowest possible species that still has a relevant resemblance to human anatomy and a deep flexor tendon size that makes it possible to design an injury and subsequent repair mimicking the clinical situation.
The clinical trial Clinical trials of flexor tendon healing have been, and are still, difficult to design. The heterogeneity of the group of patients and individual variations in mechanisms of trauma and associated injuries contribute to confounding factors in the interpretation of the data. To minimize variation, it is desirable to have the same surgeon repairing all tendon injuries included in a study, which, however, is rarely possible in the clinical situation and organization. Moreover, the results of the tendon repair largely depend on successful reha-bilitation, which heavily relies on patient compliance.
All these factors contribute to the difficulties of clinical prospective stu-dies of the impact of different interventions on the outcome of flexor tendon repair. There is also a limitation in the instruments available to measure the results. Only tendon rupture rates, ROM, strength and different question-naires can be utilized: there is no method of investigating the potential posi-tive and negative consequences of the intervention on a biomolecular level. It is therefore essential to gather that information in other types of models before implementing a new intervention in a clinical situation.

25
Aims
The general aim of the thesis was to more fully characterize the deep flexor tendon and its response to injury and repair. The outcome of flexor tendon healing can be compromised by tendon rupture or adhesions. Therefore, we focused on factors believed to contribute to tendon strength or extrinsic heal-ing with potential adhesion formation, studying the flexor tendon healing process in a rabbit model, to find potential targets to influence the healing process and improve the outcome. The specific aims of the study were to:
• compare the tissue composition between the intrasynovial
deep flexor tendon, extrasynovial tendon and the tendon sheath.
• describe changes in gene expression of basic components of tendon and tendon sheath tissue after injury.
• study alterations in the inflammatory response in the flexor tendon and tendon sheath during healing.
• determine the pattern of gene expression for VEGF and IGF-1 in the tendon and tendon sheath after injury.
• further describe the temporal pattern of MMP and TIMP
gene expression after tendon injury.
• determine whether the factors of the hypothesized myofi-broblast-mast cell-neuropeptide fibrosis axis are increased in flexor tendon healing.

26
Methods
Animals In all the presented studies, skeletally mature female New Zealand White (NZW) rabbits were used with the approval of the local ethics review board. The rabbits, weighing 3 kg (± 0.3 kg), were allowed unrestricted cage activi-ty and provided with a standard laboratory diet and water ad libitum. After one to two weeks of acclimatization to the new laboratory environment, sur-gery was performed under sterile conditions in an animal operation facility, using microsurgical instruments and magnification. The rabbits were anes-thetized with intramuscular injections of fentanyl-fluanisone (Hypnorm®, Janssen, Beerse, Belgium; 0.3 ml/kg body weight) and midazolam (Dormi-cum®, Roche, Basel, Switzerland; 2 mg/kg body weight). To prevent post-surgical infections, a single intravenous dose of the antibiotic cefuroxime (100 mg; Zinacef®, GlaxoSmithKline, London, UK) was administrated im-mediately before surgery.
At certain time points after surgery or, in the case of the animals in the first study and control animals for the later studies, after one to two weeks acclimatization, the rabbits were euthanized by a lethal dose of either Pento-barbitalnatrium® (Apoteket, Uppsala, Sweden) after first having received a sedative dose of midazolam (Dormicum®, Roche) or fentanyl-fluanisone.
Intra- and extrasynovial tendons In healthy, uninjured rabbits, intra- and extrasynovial tendons were har-vested. The peroneus tendon from the lateral compartment of the lower hind leg was chosen to represent extrasynovial tendons. Two segments of the intrasynovial deep flexor tendons were harvested – one proximal segment at the level of the first annular ligament, where the tendon is subjected to com-pressive force, and one intermediate segment between the first and second annular ligament, with tensile forces acting on the tendon tissue (Figure 6). With the deep flexor tendon, the tendon sheath was also excised and ana-lyzed.

27
Figure 6. The intrasynovial deep flexor tendon of the rabbit paw with the proximal and the intermediate segments indicated.
Flexor tendon injury model The rabbit deep flexor tendon injury model has been designed to mimic deep flexor tendon injury and repair with partially active rehabilitation protocols in clinical practice. The rabbit paw anatomy resembles the human hand, with a superficial and a deep flexor tendon surrounded by a tendon sheath, rein-forced by pulleys (Figure 6). After the hind paws had been prepared with shaving and sterile draping, the flexor tendons were partially divided above the ankle at the site of the ten-don-muscular junction. The division partially unloaded the phalangeal seg-ment of the flexor tendons to allow continued activity without immobiliza-tion of the operated paws in casts and to mimic the either passive or pro-tected unloaded active rehabilitation protocols in current clinical practice, without sustaining an unacceptable rupture rate. Similar methods of unload-ing have been used before in flexor tendon studies 95, 174, 175. The partial un-loading preserves some tension, protecting the tendon from the degradation, which has been shown to occur with complete unloading 173 and which may confound later assessments of the tendon tissue. The zone II segments of the flexor tendons were accessed through a longitudinal incision on the volar side of the proximal phalanx of the third digit. The superficial flexor tendons were resected after carefully opening the flexor tendon sheath between the first and second pulleys and the deep flexor tendons were sharply and trans-versally divided at the intermediate segment (Figure 5). The deep flexor tendons were repaired with a modified Kessler core suture (non-resorbable 5-0 Prolene®, Ethicon, Johnson & Johnson, Sollentuna, Sweden) and a run-

28
ning circumferential peripheral suture (resorbable 6-0 or 7-0 PDS®, Ethi-con). The tendon sheaths were closed with a running 6-0 or 7-0 PDS® suture and the skin with a running non-resorbable suture (5-0 Ethilon®, Ethicon). A single dose of local analgesic was injected into the hind paws for postopera-tive pain release (Marcain®, AstraZeneca, Södertälje, Sweden). After sur-gery, the animals were allowed unrestricted cage activity. At the end point (ranging from three days to six weeks), tendons and tendon sheaths were harvested in 8 mm segments (4 mm proximal and distal to the repair site, respectively). After rinsing in physiological saline, the tendons and tendon sheaths were immediately frozen in liquid nitrogen and stored at -80°C until further analysis (for mRNA measurements) or fixed in formalin (for immunohistochemistry).
Figure 7. Rabbit paw with the third digit incised three weeks after suturing the deep flexor tendon. The tendon sheath has been divided and the repaired tendon lies be-neath.
Extraction of RNA RNA extraction from the tissue samples was performed using the TRIspin method 124, which combines the Trizol method with the RNeasy® Total RNA Kit (Qiagen, MERCK Eurolab, Stockholm, Sweden) and is a reliable method for extracting RNA from hypocellular, dense connective tissues, such as tendon and ligament 21, 93, 94. The frozen tendon tissues were placed in liquid nitrogen-cooled custom-made vials and pulverized using a Braun Mikro-Dismembrator (B. Braun Biotech International, Melsungen, Germa-ny) at 2600 rpm for 30 seconds. The frozen powdered tissue was thawed in 1 ml TRIzol™ (Gibco Life Technologies, Carlsbad, CA, USA) and rotated for five minutes. After addition of 0.3 ml chloroform and centrifugation for 15

29
minutes at 12000 rpm, ethanol (0.6 ml 70%) was added to the upper aqueous phase and total RNA isolated from the samples using the RNeasy® Total RNA Kit. DNase (RNase-Free DNase Set, Qiagen) was added during the procedure to eliminate potential DNA contamination (this was confirmed using no RT controls in a subsequent PCR analysis). The isolated RNA was quantified using the Sybrgreen II reagent (BioWhittaker Application, Invitro, Stockholm, Sweden). Samples of total RNA were stored at -80°C until fur-ther analysis.
Semiquantification of mRNA Reverse transcription (Omniscript RT Kit; Qiagen) was performed with 1 μg of total RNA with random primers. All samples in a given experiment were subjected to reverse transcription at the same time to avoid potential varia-tion. Similarly, all cDNA samples in a given experiment were assessed by PCR at the same time to avoid any potential variation in efficiency and de-tection of the amplicons. Aliquots (15 μl) of cDNA were amplified in a total volume of 50 μl containing 1xpolymerase chain reaction buffer: 1.5 mM MgCl2, 0.2 mM deoxynucleoside triphosphate mixture, 0.5 μM of each pri-mer and 1 U Taq DNA polymerase. Known rabbit sequences, which have been validated in previous studies 21, 59, 93, 133, were used to design the primers (Table 1). To optimize the number of cycles and the temperature during the annealing phase of the PCR, the samples were analyzed at 18 to 30 cycles. The PCR protocol was developed such that product yields were within the linear range of the PCR amplification. Aliquots (20 μl) of the PCR products were analyzed by separation in a 2% agarose gel at 60 V/cm in 1xTris-Acetate-EDTA buffer. The gel was then stained with ethidium bromide and photographed. The photographs were analyzed by densitometry (MasterScan Interpretive Densitometer and RFLPscan, Scanalytics, Billerica, MA, USA) and values determined to be within the linear range of the image analysis system. Values for each gene were then normalized to the housekeeping gene �-actin (Paper I-III) or 18S (Paper IV-V) for each sample.
For some factors in study IV and V, real-time PCR measurements were performed in addition to the semiquantitative method with similar results (TGF-�1, �-SMA and MMP-13). However, semiquantitative PCR was main-ly used in the studies since we do not yet have access to a full range of vali-dated primers for real-time PCR. The methodology of semiquantitative PCR is highly reproducible and the results found to be comparable to those ob-tained by qPCR using an iCycler 115.

30
Table 1. Primers used for PCR.
Gene Forward primer Reverse primer
18S gtc ccc caa ctt ctt a cac cta cgg aaa cct tgt tac�-SMA gtg tga gga aga gga cag ca tac gtc cag agg cat aga ggAggrecan gag gag atg gag ggt gag gtc ttt ctt cgc ctg tgt agc aga tg�-actin tgc ttc tag gcg gac tgt ta cgt cac atg gca tct cac gaBiglycan gat ggc ctg aag ctc aa ggt tgt tga aga ggc tgCathepsin K agc tgg gga gaa agc tgg gga aac aaa g agg cac aaa caa atg ggg aaa cca aac a Collagen I gat gcg ttc cag ttc gag ta ggt ctt ccg gtg gtc ttg taCollagen III tta taa acc aac ctc ttc ct tat tat agc acc att gag acCOX-2 tca gcc acg cag caa atc ct gtg atc tgg atg tca gca cgCTGF ttg tag ctg atc agt ctt tcc ac caa cta aaa agg tgc aaa cat gta a Decorin tgt gga caa tgg ttc tct gg cca cat tgc agt taa ggt tccbFGF tac aac ttc aag cag aag ag cag ctc tta gca gac att ggHAS2 ggc cgg tcg tct caa att ca cca ccc cat ttt tgc atg atHAS3 aag tgc ctc aca gag acc cc aag atc atc tct gca ttg ccIGF-1 gca tcc tgt cct cct cgc at gtc ttg ggc atg tcg gtg tgIL-1� tac aac aag agc ttc cgg ca ggc cac agg tat ctt gtc gtiNOS cgc cct tcc gca gtt tct tcc agg agg aca tgc agc acLumican ctg cag tgg ctc att cta gac ctc cag gta ata gttMMP-3 gcc aag aga tgc tgt tga tg agg tct gtg aag gcg ttg taMMP-13 ttc ggc tta gag gtg aca gg act ctt gcc ggt gta ggt gtNGF ggt gca tag cgt aat gtc ca ttg ctc ctg tga gtc ctg ttTGF-�1 cgg cag ctg tac att gac tt agc gca cga tca tgt tgg acTIMP-1 gca act ccg acc ttg tca tc agc gta ggt ctt ggt gaa gcTIMP-3 tct gca act ccg aca tcg tg cgg atg cag gcg tag tgt tTNF-� agc cca cgt agt agc aaa ccc ttg atg gca gag agg agg tgg a VEGF gga gta ccc tga tga gat cga ctt tgg tct gca ttc aca ttt gtVersican gat gtg tat tgt tat gtg gat ca cat caa atc tgc tat cag gg
Immunohistochemistry Tissue samples intended for immunohistochemistry were, after fixation in formalin, embedded in paraffin blocks and sagitally cut in 6-μm sections. Five sections from each sample were mounted on glass slides, deparaffinated and rehydrated. Myofibroblasts, mast cells and neuropeptide-containing nerve fibers were measured with a triple labeling protocol 60. Markers used were �-SMA (myofibroblasts), tryptase (mast cells) and SP (neuropeptide-containing nerve fibers). After treatment of the sections with a blocking agent (10% goat serum in PBS for 20 minutes), the primary monoclonal �-SMA antibody (clone 1A4, Sigma-Aldrich, St Louis, MO, USA) was ap-plied. The samples were incubated in 37°C for 60 minutes, washed and treated with the secondary antibody (sheep antimouse IgG HRPO (horsera-dish peroxidase conjugate) in 1:1000 dilution, Röche Molecular Biochemi-cals, Laval, Quebec, Canada) for another 60 minutes at room temperature.

31
After washing, DAB (3,3-diaminobenzidine solution)/peroxide substrate (1:10, Röche) was applied, followed by washing and treatment with polyc-lonal tryptase goat antibodies (1:100, Santa Cruz Biotechnology, Santa Cruz, CA, USA) overnight at 4°C and the secondary anti-goat antibody conjugated with Cy3 (1:1000, Peninsula Laboratories, Houghton, MI, USA) was applied for 60 minutes at room temperature. Polyclonal guinea pig antibodies to SP (1:200, Peninsula Laboratories) were added and incubated at room tempera-ture for two hours. The SP antibodies were followed by application of an anti guinea pig secondary antibody (1:1000) conjugated with Alexa Fluor 488 (Molecular Probes, Eugene, OR, USA) at room temperature for 60 mi-nutes. Slides were then treated with DAPI (4’-6-diamidine-2-phenyl indole, Vector Laboratories, Burlington, Ontario, Canada) and viewed under a Zeiss light microscope (Zeiss, Axioskop 2 plus, Toronto, Ontario, Canada). A digital camera (Zeiss, Axiocam) was used to photograph five areas from each section. The photographs were analyzed with the program Image-Pro Plus (Media Cybernetics, Silver Spring, MD, USA). For each image, blinded counts of the total cell number as well as myofibroblasts (�-SMA), mast cells (tryptase) and neuropeptide-containing nerve fiber (SP) were repeated three times and averaged. This procedure was followed by determining the average for each section and, consequently, each sample.
Statistical analysis All calculations were performed using the Statistica software package 7 (StatSoft, Tulsa, OK, USA). Group data were subjected to standard descrip-tive statistics (mean, standard error and deviation and percentage).
Differences between groups (different tendons and tendon sheaths) at the same time points were determined with Student’s t-test. To detect significant changes within a group over time, analysis of variance (ANOVA) followed by Tukey’s HSD post-hoc test were used. Only differences or changes with a p-value � 0.05 were considered significant.
For a number of variations in expression, significant differences could not be confirmed. The small number of animals in the groups (n=3-7), giving a low power, requires larger differences between groups to lead to significant results.

32
Results and discussion
Study I. Differences between intra- and extrasynovial tendons The aim of study I was to investigate differences in mRNA expression for a number of relevant molecules in the extrasynovial peroneus tendon, two regions of the intrasynovial deep flexor tendon subjected to compressive or tensile loading and the sheath of the flexor tendon. Six NZW rabbits were euthanized and the tissues mentioned above harvested. Measurements of mRNA from extracted RNA were performed using semiquantitative RT-PCR.
The collected data for the pattern of mRNA expression supported pre-vious findings achieved with histological or biomechanical methods. The proximal segment of the intrasynovial rabbit deep flexor tendon is subjected to compressive forces over the metatarsophalangeal joint and subsequently has a distinctive fibrocartilaginous phenotype, separating it from the inter-mediate segment which is subjected to tensile forces 13, 100, 113, 126, 167. Accor-dingly, the proximal segment contained significantly higher levels of mRNA for molecules associated with fibrocartilaginous tissue, such as aggrecan, biglycan and collagen III (Figure 8). The tendon sheath had more total RNA, reflecting a higher cellularity for its role as supplier of nutrition to the tendon tissue, but significantly lower levels of proteoglycan and collagen mRNA as a consequence of a lower load. The growth factor TGF-�1 was higher in the intrasynovial flexor tendon tissue than in the extrasynovial peroneus tendon, mirroring the pattern of collagen I expression it has been shown to stimulate 81. It can also increase the expression of aggrecan and biglycan 127.

33
Figure 8. Expression of mRNA in the different types of tendon and the tendon sheath.
The differences in the patterns of mRNA expression between the regions and types of tissue underline the importance of designing a model of deep flexor tendon injury relevant to the clinical situation. In an injured and repaired deep flexor tendon, different mechanical forces acting on the tendon tissue in separate regions will have an impact on the biomolecular phenotype and influence the results of the study. There are also differences in the composi-tion of intra- and extrasynovial tendons. Further, data from studies of extra-synovial tendons (such as the Achilles tendon) cannot automatically be pre-sumed true for the intrasynovial flexor tendon. In the clinical setting, this has implications for the use of extrasynovial tendons (usually the palmaris lon-gus or the plantaris tendon) as grafts in delayed repair of flexor tendon inju-ries 2. Toe flexors have been suggested as alternative grafts to preserve the character of the tendon tissue suited to the local environment and improve tendon excursion, but are generally not utilized. This lack of utilization of toe flexors may be due to practical considerations or a cautiousness for do-nor site morbidity, although studies claim good results 87, 112.
Study II. Matrix molecules and growth factors after tendon repair In our second study, we investigated the effect a deep flexor tendon injury with subsequent repair has on the mRNA expression of some of the base

34
components (collagens and proteoglycans) of tendon tissue in the tendon and the surrounding tendon sheath. Three growth factors implicated in healing and fibrotic processes in connective tissues were also included. In a rabbit model of deep flexor tendon injury (five groups of NZW rabbits including controls, with n=6 for each group), mRNA levels were analyzed by semi-quantitative RT-PCR at different time points (3, 6, 12 and 24 days) after injury and repair.
After flexor tendon injury, there was a shift in collagen mRNA expression with an increase of collagen type III in both tendon and tendon sheath. In contrast, collagen type I remained unaltered in tendon (Figure 9). This change in expression is in accordance with studies of proliferation and re-modeling of connective tissue (e.g. tendon and ligament) 114, 150 and has been hypothesized to decrease the strength of the tendon tissue 170.
Figure 9. Collagens and TGF-�1 mRNA expression in tendon tissue. Significant differences compared with controls are indicated by an *.
Proteoglycans (decorin, biglycan and lumican) participate in the regulation of collagen fibrillogenesis through binding to collagen fibrils 132. In our study, all proteoglycans except decorin were increased in both tendon tissue and tendon sheath after injury, decorin mRNA instead being markedly down-regulated (Figure 10). Biglycan is believed to be of importance to the composition of flexor tendons, with knockout mice exhibiting flexor tendons with decreased biomechanical properties 128. However, the high levels of biglycan mRNA detected in tendon tissue may have a negative impact on the healing process, biglycan being associated with fibrotic processes 45, 144 and known to accumulate for long periods after other connective tissue injuries

35
121, 154. Decorin levels may be related to the biglycan expression. During de-velopment, decorin knockout mice have increased amounts of biglycan, the SLRPs to some extent being able to compensate for the lack of the other 183. It is possible that they have somewhat different functions in collagen compo-sition, biglycan being the more dominant in rabbit deep flexor tendons dur-ing the first month after injury in our study, resembling the down-regulation seen in rabbit medial collateral ligaments 121. This posttraumatic balance is not necessarily an ideal healing environment. One study has claimed im-proved results of tendon healing with decreased adhesion formation after treating sutured rabbit deep flexor tendons with topically administered deco-rin 180. The potential beneficial effect of decorin can be hypothesized to be both an effect of decreasing the amount of biglycan and of inhibiting TGF-�1 11, 132.
Figure 10. SLRPs mRNA expression in tendon tissue after injury and repair. Signif-icant differences compared with controls are indicated by an *.
We could show that mRNA levels for the large aggregating proteoglycans aggrecan and versican, mediating fibroblast cell proliferation and inflamma-tory cell migration 132, 172, increase after injury. An overexpression of aggre-can and versican could be hypothesized to prolong an inflammatory response and increase adhesion formation, but mRNA expression for both were ap-proaching normal levels at the last time point assessed (24 days).
TGF-�1, a regulator of wound repair and implicated in fibrotic processes 16, 79, exhibited similar patterns of mRNA expression as collagen III in ten-don tissue in our study (Figure 8), which is in accordance with the known stimulatory effect of TGF-�1 on collagen III production 80, 81.
Despite CTGFs connection to TGF-�1 and involvement in fibrotic processes and tendinopathies, the mRNA levels were not significantly al-

36
tered after injury. A possible explanation is the timing of the analysis: a po-tential rapid transient increase in CTGF could exhibit levels already decreas-ing toward normal at the first time point assessed. In a later study, an early increase in CTGF mRNA three days after flexor tendon injury could be demonstrated in a chicken model, but levels were down-regulated after the first week, returning to normal or sub-normal levels 27. Our findings do not indicate that the growth factor would be a likely target to decrease adhesion formation mediated by TGF-�1 in deep flexor tendon healing.
Studies by other investigators have shown conflicting results concerning the endogenous bFGF response to flexor tendon injury. Both increases 25 and decreases or no alterations 27, 73, 159 have been reported. We found, in agree-ment with the majority of studies, a transient increase in bFGF mRNA in flexor tendon tissue three days after repair, the gene expression remaining at normal levels at all time points assessed in the tendon sheaths. This finding supports the hypothesized beneficial effects an exogenous addition of bFGF may have on the tendon tissue composition, reinforcing the tendons’ re-sponse to injury.
Study III. Inflammatory molecules and hyaluronan synthases after tendon repair Earlier intervention studies in animal models of tendon healing have demon-strated some potential for the treatment with anti-inflammatory agents 44, 85,
147. In previous studies, IL-1� has been reported to induce COX-2 mRNA expression in tendon tissue 160. We found similar temporal alterations in the pattern of mRNA expression for IL-1� and COX-2, with the levels reaching a peak three days after tendon repair, and then decreasing after the first week (Figure 11). Although our findings indirectly support the effect of IL-1� on COX-2 expression, the rapid increase in COX-2 with a decline during the first week after injury suggests that any treatment targeting COX-2 would only be relevant during the first week after tendon repair. The effects of COX-2 inhibitors on tendon tissue have mainly been investigated in Achilles tendons; the results from these studies are not consistent, however 40, 44, 158.

37
Figure 11. IL-1� and COX-2 mRNA expression in tendons and tendon sheaths after injury and repair. Significant differences compared with controls are indicated by an *.
TNF-�, which was undetectable, and IL-1� are both known inducers of col-lagenases 32, 160. In the tendon tissue, levels of the collagenase MMP-13 mRNA were increased with maximum levels two weeks after tendon repair. They remained at peak levels in the sheath at the last time point assessed, which is in accordance with earlier reports of a higher MMP production in tendon sheath fibroblasts in in vitro studies 74, a possible component of the inflammatory response associated with extrinsic healing. TIMP-1, an endo-genous regulator of MMP expression 22, exhibited a similar pattern of mRNA expression to MMP-13 in tendon.
Other than anti-inflammatory therapies, exogenous hyaluronan has been advocated as an inhibitor of adhesion formation 92, 109, 125, 186. However, there is little knowledge of the endogenous hyaluronan response to flexor tendon injury. In the present study, two hyaluronan synthases were assessed (HAS2 and HAS3). We could demonstrate that the mRNA expression was in-creased, HAS2 reaching levels seven-fold those of the controls in the tendon tissue. HAS3 demonstrated a lesser increase in tendon tissue but also exhi-bited tendencies to an increase in the sheaths (Figure 12). This observation indicates differences between the regulation of endogenous hyaluronan pro-duction in the tendon and the tendon sheath and that the high molecular weight hyaluronan produced by HAS2 may have a greater role than the low molecular product of HAS3 after deep flexor tendon injury.

38
Figure 12. Hyaluronan synthases mRNA expression in tendons and tendon sheaths after injury and repair. Significant differences compared with controls are indicated by an *.
Study IV. Growth factors and proteases in healing flexor tendon and sheath This fourth study demonstrated a steady-state expression of IGF-1 mRNA in uninjured tissues that was markedly higher in the tendon sheaths, with in-creased levels after injury in the tendons reaching the essentially unaltered levels of the sheaths after 42 days (Figure 13). Previous studies have found different patterns of IGF-1 expression depending on the type of pathology affecting the tendon tissue. Chronic conditions (tendinosis induced chemical-ly or by overuse) caused a slow but prolonged increase 35, 135, whereas acute mechanical injury resulted in an early transient increase in studies monitor-ing a shorter time 27, 83. Whether the differences are due to type of animal or tendon, or the time points chosen, remain to be determined. However, our findings could support the concept of IGF-1, a known stimulator of tenocyte cell proliferation and collagen synthesis, as a potential agent to improve the mechanical properties of the tendon, decreasing the risk of tendon rupture without stimulating adhesion formation.

39
Figure 13. IGF-1 and VEGF mRNA expression presented as a normalized ratio to housekeeping gene 18S. Significant differences compared with control values are indicated by an * and significant differences between tendon and sheath at the same time point by a †.
Other investigators have demonstrated a transient increase of the angiogenet-ic growth factor VEGF during the first or second week after tendon injury, but have no data for the later healing phase 18, 27. In our study, VEGF tended to increase in the inflammatory phase after three days in tendon and tendon sheath, but was significantly decreased at later time points when the poorly vascularized deep flexor tendon has a higher risk of rupture. We could not demonstrate any significant increases, that if pronounced could contribute to the extrinsic healing response with adhesion formation. Thus, exogenous addition of VEGF, which does not seem to be overexpressed in normal flex-or tendon healing, may strengthen the compromised healing tendon tissue without stimulating adhesions.
We could also demonstrate that the neuropeptide NGF, addition of which has had positive effects on ligament healing in animal studies 101, was present in both healing and uninjured tendon and tendon sheath tissues. There were no significant changes in expression after injury to support the

40
concept of NGF as an active contributor in deep flexor tendon healing, but that does not exclude the possibility that an engineered increase of NGF may have beneficial effects.
In our third study, we found an increase in MMP-13 during the first three weeks after tendon repair. We could now confirm this increase and show that it remains after six weeks, consistent with the continued breakdown of colla-gens during the remodeling phase. This finding is in contrast to MMP-3 mRNA expression, which is down-regulated already by the end of the first week after injury in the tendon tissue, with no significant increase at all in the sheath. An earlier study by Oshiro et al 114 demonstrated a more marked and prolonged increase in MMP-3, but involved complete unloading of the tendon tissue, which will have an impact on MMP expression. However, the mRNA levels do not necessarily mirror the levels of active MMPs in the tissue and therefore must be interpreted with caution. TIMP-1 mRNA ex-pression was increased after three weeks, whereas TIMP-3 remained at sub-normal levels six weeks after tendon injury in the sheath, with no changes in the tendon tissue (Figure 14). A down-regulation of TIMP-3 over a longer period may have negative effects, being associated with chronic tendinopa-thies in rotator cuff and Achilles tendons 69, 94.
Figure 14. MMP and TIMP mRNA expression, presented as a normalized ratio to housekeeping gene 18S. Significant differences compared with control values are indicated by an *.

41
Study V. The myofibroblast-mast cell-neuropeptide fibrosis pathway in flexor tendon healing In our fifth study, we demonstrated significantly increased numbers of myo-fibroblasts, mast cells and neuropeptide-containing nerve fibers in rabbit deep flexor tendon tissue after injury. In the normal uninjured controls, they constituted less than 10% of the total cell population as compared with levels reaching 33-50% after tendon repair, which is comparable with results from joint capsule contractures in previous studies 59, 60. The increase remained at the last included time point (six weeks after surgery) with similar patterns for all factors assessed (Figure 15).
Figure 15. Myofibroblasts, mast cells and neuropeptide-containing nerve fibers in tendon tissue – percentage of total cell count in controls and at different time points after tendon repair. Significant differences compared with uninjured controls are indicated by an *.

42
Figure 16. Immunohistochemical staining for total cell count (DAPI), myofibrob-lasts (�-SMA), mast cells (tryptase) and neuropeptide-containing nerve fibers (SP) in tendon tissue in controls and at different time points after injury and repair. Block arrows indicate a blood vessel, black arrows groups of myofibroblasts and white arrows corresponding areas with co-localization of mast cells and neuropeptide-containing nerve fibers.
Mast cells, which we have shown increase in number after deep flexor ten-don injury, can stimulate TGF-�1, which up-regulates �-SMA in fibroblasts and induces the myofibroblast phenotype 62, 68, 162. In the present study, we demonstrated increased mRNA levels of both TGF-�1 and �-SMA in the repaired tendons (Figure 17). In contrast, the mRNA levels of TGF-�1 and �-SMA remained essentially unaltered in the sheaths.
Recently, a profibrotic myofibroblast-mast cell-neuropeptide pathway has been suggested in the development of posttraumatic capsular fibrosis with joint contracture 53, 59, 60. In our rabbit model of deep flexor tendon injury and repair, all three factors implicated in the suggested myofibroblast-mast cell-neuropeptide pathway exhibited similar patterns of increase, remaining high at all time points during the study and thus indirectly supporting the theory of interdependence in expression. This finding may have implications for adhesion formation as well as ultimate tendon strength after repair, and rais-es questions on the possible significance for the homeostasis and profibrotic effects in surrounding tissues, such as the digital interphalangeal joint cap-sules.

43
Figure 17. The mRNA expression of �-SMA and TGF-�1 in tendon tissue as per-centages of uninjured control values. Significant differences compared with controls are indicated by an *.

44
Conclusions
• The gene expression for collagens, proteoglycans and TGF-�1 varies between different regions of intrasynovial tendon, extrasynovial tendon and tendon sheath.
• After flexor tendon injury and repair, a shift occurs in colla-
gen gene expression from type I to type III. Most proteogly-cans are up-regulated in response to injury, with the notable exception of decorin.
• No increase of CTGF gene expression was observed after
tendon injury. CTGF, although involved in fibrotic processes in other types of tissue, may not be a factor in flexor tendon healing.
• Hyaluronan synthase mRNA is present in deep flexor ten-
dons and tendon sheaths. After injury, both HAS2 and HAS3 mRNA increase in the tendon tissues, with the high molecu-lar weight hyaluronan producing HAS2 reaching the highest levels.
• IGF-1 exhibits a late increase and VEGF a down-regulation
in gene expression after injury.
• MMP-3, MMP-13, TIMP-1 and TIMP-3 exhibit different temporal gene expression patterns after tendon injury. MMP-13 mRNA remains increased six weeks after injury in both tendon and sheath, suggesting its active role in all phases of the healing process.
• There is an increase of the factors implicated in the profi-
brotic myofibroblast-mast cell-neuropeptide pathway after deep flexor tendon injury, suggesting its involvement in flexor tendon healing.

45
Future prospects
The major goal of flexor tendon healing is to achieve a strong tendon (de-creasing the risk of rupture) without adhesions (optimizing tendon excursion; ROM). The current challenge is to stimulate certain aspects of the healing process in order to reinforce tendon strength but not simultaneously increase the extrinsic healing mechanisms and subsequent adhesion formation, and vice versa.
Several paths of action can be considered. We can focus on agents that limit the inflammatory response and any potential excessive cell prolifera-tion (counteracting extrinsic healing and adhesion formation), such as anti-inflammatory or anti-proliferative drugs, or antibodies to growth factors, but will they weaken the tendon and increase the risk of rupture? We can add exogenous growth factors, supporting the endogenous response to traumatic injury, but will that cause excessive healing with scarring?
One patent solution that fits all kinds of deep flexor tendon injuries is un-likely. However, the compiled knowledge of the behavior of the flexor ten-dons after injury steadily increases, and maybe we are not far from a com-mercially available growth factor cocktail (possibly containing VEGF, bFGF and IGF-1) to add during surgery, that could stimulate a faster and stronger repair of the tendon tissue, facilitate active rehabilitation and decrease the risk of tendon ruptures, even when compliance fails. For patients with crush injuries, concomitant fractures or extensive soft tissue damage, a tendon wrapping material that includes hyaluronan and antifibrotic agents (such as antibodies to TGF-�1) could limit excessive scarring and adhesion forma-tion.
The finding of factors in the profibrotic myofibroblast-mast cell-neuropeptide pathway in tendon tissue after injury introduces some tantaliz-ing questions. Would their increase be even more pronounced in a flexor tendon injury model that provokes adhesion by post-operative immobiliza-tion? What is their expression pattern in finger joint capsules and to what extent may the extension defects with stiffness of the PIP and DIP joint after flexor tendon injury be connected to an activation of this pathway? Would mast cell stabilizers have positive effects on ROM after flexor tendon injury where the patients’ compliance or concomitant injuries necessitate immobi-lization?

46
Summary in Swedish – sammanfattning på svenska
Molekylärbiologiska aspekter på böjsenläkning Böjsenorna är centrala för handens funktion och bidrar till människans väl utvecklade finmotorik som möjliggör sysslor som kräver hög precision. Vid skador som drabbar handens böjsenor i området mellan handflatans böjveck och den yttersta fingerleden är risken större att senan antingen går av igen efter reparation, eller att den ärrar fast mot sin omgivning och fingret blir stelt. I detta område är böjsenan omgiven av en senskida, som bidrar till senans näringsförsörjning. När böjsenan läker efter en skada kan det bildas sammanväxningar mellan sena, senskida och ben. Sammanväxningarna hindrar senans rörelse och minskar det drabbade fingrets rörlighet. På grund av den stora risken för ärrbildning med sammanväxningar reparerades tidiga-re inte böjsenskador inom senskideområdet, som till och med benämndes ingenmansland (”no man’s land”). Först på 1960-talet började man reparera böjsenor direkt efter skadan, istället för att i ett senare skede operera bort ärrvävnaden och transplantera in en ny sena. Sammanväxningarna ansågs tidigare vara nödvändiga för att böjsenan skulle läka, men genom studier av bland annat Göran Lundborg upptäcktes att böjsenan är en levande vävnad, med celler och egen tillverkning av de byggstenar som behövs för att läka en skada, samt att den även får näring via diffusion från senskidan och inte en-dast från inväxande kärl. Dagens behandlingsmetoder syftar till att motverka sammanväxningar. De senaste decennierna har resultaten av direkta repara-tioner av böjsenskador förbättrats med nya rehabiliteringsprinciper (sjuk-gymnastisk träning istället för immobilisering i gips, vilket minskar sam-manväxningarna) och nya kirurgiska tekniker (skonsammare behandling av vävnaden, samt starkare suturer som tillåter träning och minskar risken för re-rupturer).
Trots de framsteg som skett kan en böjsenskada fortfarande innebära stora kostnader för både samhället och för den drabbade individen. Förutom en lång rehabiliteringsperiod kan den ge bestående rörelseinskränkning med nedsatt handfunktion. För att ytterligare kunna optimera resultaten av böj-senkirurgi studeras nu olika aspekter av böjsenan på molekylärbiologisk nivå i djurmodeller.

47
Denna avhandling är baserad på fem studier med syftet att bidra till kart-läggningen av böjsenans uppbyggnad och reaktion på skada. I samtliga stu-dier har en kaninmodell använts.
I den första studien jämförde vi olika delar av den intrasynoviala böjsenan (omgiven av en senskida) med den extrasynoviala peroneussenan (saknar senskida) och senskidevävnad. Vi fann att mRNA uttrycket för vanliga byggstenar i senvävnad (kollagener och proteoglykaner) varierade mellan olika regioner av böjsenan som utsätts för olika typer av belastningar. Kom-primerande tryck ger högre nivåer av proteoglykaner och typ III kollagen vilket resulterar i en mer broskliknande vävnad. I de regioner där tensions-krafter dominerar var uttrycket av proteoglykaner lägre. Vi fann även skill-nader mellan den intrasynoviala böjsenan och den extrasynoviala peroneus-senan, vilket ytterligare stödjer att böjsenan är unik och att kunskap om andra typer av senor inte kan förutsättas gälla även för böjsenan.
Den andra studien fokuserade på förändringar i genuttryck i böjsenan och dess senskida efter att senan skadats och reparerats. Den oskadade böjsenan är uppbyggd av framför allt typ I kollagen men under den första delen av läkningsprocessen dominerade typ III kollagen. Proteoglykaner hade kraftigt ökade mRNA nivåer, med undantaget decorin som istället nedreglerades. Vi fann även att mRNA för tillväxtfaktorn bFGF, som tros kunna förbättra se-nans läkning och hållfasthet, endast kortvarigt uppreglerades under den för-sta veckan av läkningsprocessen.
I den tredje studien kunde vi visa att böjsenan ökade uttrycket av mRNA för komponenter i den endogena hyaluronsyreproduktionen efter en skada. Vi fann även en ökning av mRNA för faktorer involverade i det inflammato-riska svaret (COX-2 och IL-1�) men det var kortvarigt med normaliserade nivåer redan efter den första veckan.
Den fjärde studien följde böjsenans läkningsförlopp över en längre tidspe-riod och inkluderade början på remodelleringsprocessen sex veckor efter skadan. Vi kunde visa att kollagenaset MMP-13 hade höga mRNA nivåer under hela perioden och därmed verkar delta i alla delar av läkningsproces-sen, till skillnad mot MMP-3 som nedreglerades redan efter en vecka. Till-växtfaktorer som kan vara positiva för senans styrka uppvisade antingen en nedreglering av mRNA (VEGF) eller en sen ökning (IGF-1), vilket ytterliga-re styrker hypotesen att en tillförsel utifrån av dem skulle kunna optimera böjsenläkning. Vi fann även att tillväxtfaktorn NGF fanns i både oskadad och skadad böjsena, men att dess mRNA uttryck inte påverkades av en ska-da.
I den avslutande femte studien undersökte vi om faktorer involverade i en hypotetisk fibrosstimulerande cykel ökar även efter böjsenskada. Vi visade att andelen myofibroblaster, mast celler och nervfibrer med neuropeptider blev större i den skadade senvävnaden, en ökning som varade minst sex veckor. Detta kan ha betydelse för både böjsenan och dess omgivande leder.

48
Acknowledgements
I would like to express my sincere gratitude to everyone that made this doc-toral thesis possible. In particular I would like to thank:
Monica Wiig, my supervisor, for introducing me to the world of hand sur-gery and flexor tendons and for your professional guidance.
David Hart, my co-author and mentor, for never-ending patience, invalua-ble feedback and support. Olle Nilsson, my co-supervisor, for your guidance and encouragement. Carol Reno, for brilliant technical support and patiently answering all my questions. Britt-Marie Andersson and Mei Zhang, for skilful technical assistance. Kevin Hildebrand, my co-author, for generously sharing his knowledge. Stephan Wilbrand, Head of Department of Hand Surgery, for giving me the time and support to complete my thesis. Everyone at the Department of Hand Surgery, Uppsala University Hos-pital, for your friendship, support and encouragement. You make work fun! Bertil Vinnars, for valuable advice and inspiring enthusiasm. All my friends, with special thanks to Pauline Englund and Dina Giese, for keeping things in perspective, and Kristin Elf, for valuable advice. My parents Inga-Lill and Bengt, and my brother Mathias, for always being there for me. And finally, Lukas Brandts, for always supporting me and being an endless source of encouragement. Ik hou van jou!

49
References
1. Abrahamsson SO, Lundborg G, Lohmander LS. Long-term explant culture of rabbit flexor tendon: effects of recombinant human insulin-like growth factor-1 and serum on matrix metabolism. J Orthop Res 1991; 9(4):503-515.
2. Abrahamsson SO, Gelberman RH, Amiel D, Winterton P, Harwood F. Auto-genous flexor tendon grafts: fibroblast activity and matrix remodeling in dogs. J Orthop Res 1995; 13(1):58-66.
3. Abrahamsson SO, Lohmander S. Differential effects of insulin-like growth factor-1 on matrix and DNA synthesis in various regions and types of rabbit tendons. J Orthop Res 1996; 14(3):370-376.
4. Amadio P, An KN, Ejeskär A, Guimberteau JC, Harris S, Savage R et al. IFSSH Flexor Tendon Committee Report. J Hand Surg 2005; 30B:100-116.
5. Aoki M, Manske PR, Pruitt DL, Larson BJ. Work of flexion after tendon repair with various suture methods. A human cadaveric study. J Hand Surg 1995; 20B:310-313.
6. Bainbridge LC, Robertson C, Gillies D, Elliot D. A comparison of post-operative mobilization of flexor tendon repairs with “passive flexion – active extension” and “controlled active motion” techniques. J Hand Surg 1994; 19B:517-521.
7. Bao P, Kodra A, Tomic-Canic M, Golinko MS, Ehrlich HP, Brem H. The role of vascular endothelial growth factor in wound healing. J Surg Res 2009; 153(2):347-358.
8. Barmakian JT, Lin H, Green SM, Posner MA, Casar RS. Comparison of a su-ture technique with the modified Kessler method: resistance to gap formation. J Hand Surg 1994; 19A:777-781.
9. Barrie KA, Tomak SL, Cholewicki J, Wolfe SW: The role of multiple strands and locking sutures on gap formation of flexor tendon repairs during cyclical loading. J Hand Surg 2000; 25A:714-720.
10. Barrientos S, Stojadinovic O, Golinko MS, Brem H, Tomic-Canic M. Growth factors and cytokines in wound healing. Wound Repair Regen 2008; 16(5):585-601.
11. Bates SJ, Morrow E, Zhang AY, Pham H, Longaker MT, Chang J. Mannose-6-phosphate, an inhibitor of transforming growth factor-beta, improves range of motion after flexor tendon repair. J Bone Joint Surg Am 2006; 88(11):2465-2472.
12. Becker H, Davidoff M. Eliminating the gap in flexor tendon surgery. A new method of suture. Hand 1977; 9(3):306-311.
13. Benjamin M, Ralphs JR. Fibrocartilage in tendons and ligaments – an adapta-tion to compressive load. J Anat 1998; 193:481-494.
14. Birch HL. Tendon matrix composition and turnover in relation to functional requirements. Int J Exp Path 2007; 88(4):241-248.

50
15. Blom IE, Goldschmeding R, Leask A. Gene regulation of connective tissue growth factor: new targets for antifibrotic therapy? Matrix Biol 2002; 21(6):473-482.
16. Border WA, Noble NA. Transforming growth factor � in tissue fibrosis. N Engl J Med 1994; 331:1286-1292.
17. Boyer MI, Gelberman RH, Burns ME, Dinopoulos H, Hofem R, Silva MJ. Intrasynovial flexor tendon repair: An experimental study comparing low and high levels of in vivo force during rehabilitation in canines. J Bone Joint Surg Am 2001; 83(6):891-899.
18. Boyer MI, Watson JT, Lou J, Manske PR, Gelberman RH, Cai SR. Quantitative variation in vascular endothelial growth factor mRNA expression during early flexor tendon healing: an investigation in a canine model. J Orthop Res 2001; 19(5):869-872.
19. Boyer MI. Flexor tendon biology. Hand Clin 2005; 21(2):159-166. 20. Boyer MI. Flexor tendon injury. In: Green DP (Ed.) Green’s operative hand
surgery. Philadelphia, Elsevier, 2005, Vol. 1:219-240. 21. Boykiw R, Sciore P, Reno C, Marchuk L, Frank CB, Hart DA. Altered levels of
extracellular matrix molecule mRNA in healing rabbit ligaments. Matrix Biol 1998; 17(5):371-378.
22. Brew K, Dinakarpandian D, Nagase H. Tissue inhibitors of metalloproteinases: evolution, structure and function. Biochim Biophys Acta 2000; 1477(1-2):267-283.
23. Bunnell S. Repair of tendons in the fingers and description of two new instru-ments. Surg Gynecol Obstet 1918; 26:103-110.
24. Cao Y, Tang JB. Strength of tendon repair decreases in the presence of an intact A2 pulley: biomechanical study in a chicken model. J Hand Surg 2009; 34A:1763-1770.
25. Chang J, Most D, Thunder R, Mehrara B, Longaker MT, Lineaweaver WC. Molecular studies in flexor tendon wound healing: the role of basic fibroblast growth factor gene expression. J Hand Surg 1998; 23A:1052-1058.
26. Chang J, Thunder R, Most D, Longaker MT, Lineaweaver WC. Studies in flex-or tendon wound healing: neutralizing antibody to TGF-�1 increases postopera-tive range of motion. Plast Reconstr Surg 2000; 105(1):148-155.
27. Chen CH, Cao Y, Wu YF, Bais AJ, Gao JS, Tang JB. Tendon healing in vivo: gene expression and production of multiple growth factors in early tendon heal-ing period. J Hand Surg 2008; 33A:1834-1842.
28. Chen CH, Zhou YL, Wu YF, Cao Y, Gao JS, Tang JB. Effectiveness of micro-RNA in down-regulation of TGF-� gene expression in digital flexor tendons of chickens: in vitro and in vivo study. J Hand Surg 2009; 34A:1777-1784.
29. Chhabra A, Tsou D, Clark RT, Gaschen V, Hunziker EB, Mikic B. GDF-5 deficiency in mice delays Achilles tendon healing. J Orthop Res 2003; 21(5):826-835.
30. Chiu HF, McFarlane RM. Pathogenesis of Dupuytren’s contracture: a correla-tive clinical-pathological study. J Hand Surg 1978; 3A:1-10.
31. Clegg PD, Strassburg S, Smith RK. Cell phenotypic variation in normal and damaged tendons. Int J Exp Pathol 2007; 88(4):227-235.
32. Corps AN, Curry VA, Buttle DJ, Hazleman BL, Riley GP. Inhibition of inter-leukin-1�-stimulated collagenase and stromelysin expression in human tendon fibroblasts by epigallocatechin gallate ester. Matrix Biol 2004; 23(3):163-169.
33. Costa MA, Wu C, Pham BV, Chong AK, Pham HM, Chang J. Tissue engineer-ing of flexor tendons: optimization of tenocyte proliferation using growth factor supplementation. Tissue Eng 2006; 12(7):1937-1943.

51
34. Dahlgren LA, van der Meulen MC, Bertram JE, Starrak GS, Nixon AJ. Insulin-like growth factor-1 improves cellular and molecular aspects of healing in a col-lagenase-induced model of flexor tendinitis. J Orthop Res 2002; 20(5):910-919.
35. Dahlgren LA, Mohammed HO, Nixon AJ, Temporal expression of growth fac-tors and matrix molecules in healing tendon lesions. J Orthop Res 2005; 23(1):84-92.
36. Daniels A, van Bilsen M, Goldschmeding R, van der Vusse GJ, van Nieuwenhoven FA. Connective tissue growth factor and cardiac fibrosis. Acta Physiol 2009; 195(3):321-338.
37. Danielson KG, Baribault H, Holmes DF, Graham H, Kadler KE, Iozzo RV. Targeted disruption of decorin leads to abnormal collagen fibril morphology and skin fragility. J Cell Biol 1997; 136(3):729-743.
38. Desmoulière A. Factors influencing myofibroblast differentiation during wound healing and fibrosis. Cell Biol Int 1995; 19(5):471-476.
39. Desmoulière A, Chaponnier C, Gabbiani G. Tissue repair, contraction, and the myofibroblast. Wound Repair Regen 2005; 13(1):7-12.
40. Dimmen S, Engebretsen L, Nordsletten L, Madsen JE. Negative effects of pare-coxib and indomethacin on tendon healing: an experimental study in rats. Knee Surg Sports Traumatol Arthrosc 2009; 17(7):835-839.
41. Doyle JR. Anatomy of the finger flexor tendon sheath and pulley system. J Hand Surg 1988; 13A:473-484.
42. Elliot D, Barbieri CH, Evans RB, Mass D, Tang JB. IFSSH Flexor Tendon Committee Report 2007. J Hand Surg 2007; 32E:346-356.
43. Feodorczyk JM, Barr AE, Rani S, Gao HG, Amin M, Amin S et al. Exposure-dependent increases in IL-1beta, substance P, CTGF, and tendinosis in flexor digitorum tendons with upper extremity repetitive strain injury. J Orthop Res 2010; 28(3):298-307.
44. Forslund C, Bylander B, Aspenberg P. Indomethacin and celecoxib improve tendon healing in rats. Acta Orthop Scand 2003; 74(4):465-469.
45. Funderburgh JL, Mann MM, Funderburgh ML. Keratocyte phenotype mediates proteoglycan structure: a role for fibroblasts in corneal fibrosis. J Biol Chem 2003; 278(46):45629-45637.
46. Furlow LT Jr. The role of tendon tissues in tendon healing. Plast Reconstr Surg 1976; 57(1):39-49.
47. Gallant-Behm CL, Hildebrand KA, Hart DA. The mast cell stabilizer ketotifen prevents development of excessive skin wound contraction and fibrosis in red Duroc pigs. Wound Repair Regen 2008; 16(2):226-233.
48. Gelberman RH, Van de Berg JS, Lundborg G, Akeson WH. Flexor tendon heal-ing and restoration of the gliding surface. An ultrastructural study in dogs. J Bone Joint Surg Am 1983; 65(1):70-80.
49. Gelberman RH. Flexor tendon physiology: tendon nutrition and cellular activity in injury and repair. Instr Course Lect 1985; 34:351-360.
50. Gelberman RH, Manske PR, Akeson WH, Woo SL, Lundborg G, Amiel D. Flexor tendon repair. J Orthop Res 1986; 4(1):119-128.
51. Gelberman RH, Siegel DB, Woo SL, Amiel D, Takai S, Lee D. Healing of digital flexor tendons: Importance of the interval from injury to repair: A bio-mechanical, biochemical, and morphological study in dogs. J Bone Joint Surg Am 1991; 73(1):66-75.
52. Gelberman RH, Boyer MI, Brodt MD, Winters SC, Silva MJ. The effect of gap formation at the repair site on the strength and excursion of intrasynovial flexor tendons. An experimental study on the early stages of tendon-healing in dogs. J Bone Joint Surg Am 1999; 81(7):975-982.

52
53. Gottwald T, Coerper S, Schäffer M, Köveker G, Stead RH. The mast cell–nerve axis in wound healing: a hypothesis. Wound Rep Regen 1998; 6(1):8-20.
54. Hagberg L. Exogenous hyaluronate as an adjunct in the prevention of adhesions after flexor tendon surgery: a controlled clinical trial. J Hand Surg 1992; 17A:132-136.
55. Hamada Y, Katoh S, Hibino N, Kosaka H, Hamada D, Yasui N. Effects of mo-nofilament nylon coated with basic fibroblast growth factor on endogenous intrasynovial flexor tendon healing. J Hand Surg 2006; 31A:530-540.
56. Hanff G, Hagberg L. Prevention of restrictive adhesions with expanded polyte-trafluoroethylene diffusable membrane following flexor tendon repair: an expe-rimental study in rabbits. J Hand Surg 1998; 23A:658-664.
57. Harrison RK, Jones ME, Clayton E, Grobbelaar AO, Sanders R. Mapping of vascular endothelium in the human flexor digitorum profundus tendon. J Hand Surg 2003; 28A:806-813.
58. Hildebrand KA, Zhang M, van Snellenberg W, King GJ, Hart DA. Myofibrob-last numbers are elevated in human elbow capsules after trauma. Clin Orthop Rel Res 2004; 419:189-197.
59. Hildebrand KA, Zhang M, Germscheid NM, Wang C, Hart DA. Cellular, matrix and growth factor components of the joint capsule are modified early in the process of posttraumatic contracture formation in a rabbit model. Acta Orthop 2008; 79(1):116-125.
60. Hildebrand KA, Zhang M, Salo PT, Hart DA. Joint capsule mast cells and neu-ropeptides are increased within four weeks of injury and remain elevated in chronic stages of posttraumatic contractures. J Orthop Res 2008; 26(10):1313-1319.
61. Hill C, Riaz M, Mozzam A, Brennen MD. A regional audit of hand and wrist injuries. A study of 4873 injuries. J Hand Surg 1998; 23B:196-200.
62. Hindman HB, Marty-Roix R, Tang JB, Jupiter JB, Simmons BP, Spector M. Regulation of expression of �-smooth muscle actin in cells of Dupuytren’s con-tracture. J Bone Joint Surg Br 2003; 85(3):448-455.
63. Hirpara KM, Sullivan PJ, O’Neill B, O’Sullivan M. The optimum length of the Silfverskiöld circumferential cross stitch. J Hand Surg 2009; 34E:651-655.
64. Igarashi A, Okochi H, Bradham DM, Grotendorst GR. Regulation of connective tissue growth factor gene expression in human skin fibroblasts and during wound repair. Mol Biol Cell 1993; 4(6):637-645.
65. Itano N, Kimata K. Mammalian hyaluronan synthases. IUBMB Life 2002; 54(4):195-199.
66. James R, Kesturu G, Balian G, Chhabra AB. Tendon: biology, biomechanics, repair, growth factors, and evolving treatment options. J Hand Surg 2008; 33A:102-112.
67. Jepsen KJ, Wu F, Peragallo JH, Paul J, Roberts L, Ezura Y et al. A syndrome of joint laxity and impaired tendon integrity in lumican- and fibromodulin-deficient mice. J Biol Chem 2002; 277(38):35532-35540.
68. Jiang D, Jiang Z, Li Z, Zhang Y. Suppression of the production of extracellular matrix and �-smooth muscle actin induced by transforming growth factor-�1 in fibroblasts of the flexor tendon sheath by hepatocyte growth factor. Scand J Plast Reconstr Surg Hand Surg 2008; 42(4):169-173.
69. Jones GC, Corps AN, Pennington CJ, Clark IM, Edwards DR, Bradley MM et al. Expression profiling of metalloproteinases and tissue inhibitors of metallo-proteinases in normal and degenerate human Achilles tendon. Arthritis Rheum 2006; 54(3):832-842.

53
70. Kannus P. Structure of tendon connective tissue. Scand J Med Sci Sports 2000; 10(6):312-320.
71. Kawamoto K, Matsuda H. Nerve growth factor and wound healing. Prog Brain Res 2004; 146:369-384.
72. Kessler I, Nissim F. Primary repair without immobilization of flexor tendon division within the digital sheath. An experimental and clinical study. Acta Or-thop Scand 1969; 40(5):587-601.
73. Khan U, Edwards JC, McGrouther DA. Patterns of cellular activation after tendon injury. J Hand Surg 1996; 21B:813-820.
74. Khan U, Occleston NL, Khaw PT, McGrouther DA. Differences in proliferative rate and collagen lattice contraction between endotenon and synovial fibrob-lasts. J Hand Surg 1998; 23A:266-273.
75. Khan U, Kakar S, Akali A, Bentley G, McGrouther DA. Modulation of the formation of adhesions during the healing of injured tendons. J Bone Joint Surg Br 2000; 82(7):1054-1058.
76. Kim JB, de Wit T, Hovius SE, McGrouther DA, Walbeehm ET. What is the significance of tendon suture purchase? J Hand Surg 2009; 34E:497-502.
77. Kitis PT, Buker N, Kara IG. Comparison of two methods of controlled mobili-sation of repaired flexor tendons in zone 2. Scand J Plast Reconstr Surg Hand Surg 2009; 43(3):160-165.
78. Kjær M, Langberg H, Heinemeier K, Bayer ML, Hansen M, Holm L et al. From mechanical loading to collagen synthesis, structural changes and function in human tendon. Scand J Med Sci Sports 2009; 19(4):500-510.
79. Klass BR, Grobbelaar AO, Rolfe KJ. Transforming growth factor �1 signalling, wound healing and repair: a multifunctional cytokine with clinical implications for wound repair, a delicate balance. Postgrad Med J 2009; 85:9-14.
80. Klass BR, Rolfe KJ, Grobbelaar AO. In vitro flexor tendon cell response to TGF-�1: a gene expression study. J Hand Surg 2009; 34A:495-503.
81. Klein MB, Yalamanchi N, Pham H, Longaker MT, Chang J. Flexor tendon healing in vitro: effects of TGF-� on tendon cell collagen production. J Hand Surg 2002; 27A:615-620.
82. Knudson CB, Knudson W. Hyaluronan-binding proteins in development, tissue homeostasis, and disease. FASEB J 1993; 7(13):1233-1241.
83. Kobayashi M, Itoi E, Minagawa H, Miyakoshi N, Takahashi S, Tuoheti Y et al. Expression of growth factors in the early phase of supraspinatus tendon healing in rabbits. J Shoulder Elbow Surg 2006; 15(3):371-377.
84. Kubota H, Aoki M, Pruitt DL, Manske PR. Mechanical properties of various circumferential tendon suture techniques. J Hand Surg 1996; 21B:474-480.
85. Kulick MI, Smith S, Hadler K. Oral ibuprofen: evaluation of its effect on peri-tendinous adhesions and the breaking strength of a tenorrhaphy. J Hand Surg 1986; 11A:110-120.
86. Laurent TC, Fraser JR. Hyaluronan. FASEB J 1992; 6(7):2397-2404. 87. Leversedge FJ, Zelouf D, Williams C, Gelberman RH, Seiler JG 3rd. Flexor
tendon grafting to the hand: an assessment of the intrasynovial donor tendon – a preliminary single-cohort study. J Hand Surg 2000; 25A:721-730.
88. Lieber RL, Amiel D, Kaufman KR, Whitney J, Gelberman RH. Relationship between joint motion and flexor tendon force in the canine forelimb. J Hand Surg 1996; 21A:957-962.
89. Lieber RL, Silva MJ, Amiel D, Gelberman RH. Wrist and digital joint motion produce unique flexor tendon force and excursion in the canine forelimb. J Biomech 1999; 32(2):175-181.

54
90. Lister GD, Kleinert HE, Kutz JE, Atasoy E. Primary flexor tendon repair fol-lowed by immediate controlled mobilization. J Hand Surg 1977; 2A:441-451.
91. Liu SH, Yang RS, al-Shaikh R, Lane JM. Collagen in tendon, ligament, and bone healing. A current review. Clin Orthop Relat Res 1995; 318:265-278.
92. Liu Y, Skardal A, Shu XZ, Prestwich GD. Prevention of peritendinous adhe-sions using a hyaluronan-derived hydrogel film following partial-thickness flexor tendon injury. J Orthop Res 2008; 26(4):562-569.
93. Lo I, Marchuk L, Hart DA, Frank CB. Comparison of mRNA levels for matrix molecules in normal and disrupted human anterior cruciate ligaments using re-verse transcription-polymerase chain reaction. J Orthop Res 1998; 16(4):421-428.
94. Lo I, Marchuk L, Hollinshead R, Hart DA, Frank CB. Matrix metalloproteinase and tissue inhibitor of matrix metalloproteinase mRNA levels are specifically altered in torn rotator cuff tendons. Am J Sports Med 2004; 32(5):1223-1229.
95. Loiselle AE, Bragdon GA, Jacobson JA, Hasslund S, Cortes ZE, Schwarz EM et al. Remodeling of murine intrasynovial tendon adhesions following injury: MMP and neotendon gene expression. J Orthop Res 2009; 27(6):833-840.
96. Lundborg G. Experimental flexor tendon healing without adhesion formation – a new concept of tendon nutrition and intrinsic healing mechanisms. A prelimi-nary report. The Hand 1976; 3:235-238.
97. Lundborg G, Myrhage R, Rydevik B. The vascularization of human flexor ten-dons within the digital synovial sheath region – structureal and functional as-pects. J Hand Surg 1977; 2A:417-427.
98. Lundborg G. Rank F. Experimental intrinsic healing of flexor tendons based upon synovial fluid nutrition. J Hand Surg 1978; 3A:21-31.
99. Lundborg G, Holm S, Myrhage R. The role of the synovial fluid and tendon sheath for flexor tendon nutrition. An experimental tracer study on diffusional pathways in dogs. Scand J Plast Reconstr Surg 1980; 14(1):99-107.
100. Malaviya P, Butler DL, Boivin GP, Smith FN, Barry FP, Murphy JM et al. An in vivo model for load-modulated remodeling in the rabbit flexor tendon. J Or-thop Res 2000; 18(1):116-125.
101. Mammoto T, Seerattan RA, Paulson KD, Leonard CA, Bray RC, Salo PT. Nerve growth factor improves ligament healing. J Orthop Res 2008; 26(7):957-964.
102. Manske PR, Lesker PA. Nutrient pathways of flexor tendons in primates. J Hand Surg 1982; 7(5):436-444.
103. Manske PR, Gelberman RH, Van de Berg JS, Lesker PA. Intrinsic flexor tendon repair. A morphological study in vitro. J Bone Joint Surg Am 1984; 66(3):385-396.
104. Maurer M, Theoharides T, Granstein RD, Bischoff SC, Bienenstock J, Henz B et al. What is the physiological function of mast cells? Exp Dermatol 2003; 12(6):886-910.
105. May EJ, Silfverskiöld KL, Sollerman CJ. Controlled mobilization after flexor tendon repair in zone II: a prospective comparison of three methods. J Hand Surg 1992; 17A:942-952.
106. McDowell CL, Marqueen TJ, Yager D, Owen J, Wayne JS. Characterization of the tensile properties and histologic/biochemical changes in normal chicken tendon at the site of suture insertion. J Hand Surg 2002; 27A:605-614.
107. Metcalfe DD, Baram D, Mekori YA. Mast cells. Physiol Rev 1997; 77(4):1033-1079.

55
108. Mori T, Kawara S, Shinozaki M, Hayashi N, Kakinuma T, Igarashi A et al. Role and interaction of connective tissue growth factor with transforming growth fac-tor-beta in persistent fibrosis: A mouse fibrosis model. J Cell Physiol 1999; 181(1):153-159.
109. Moro-oka T, Miura H, Mawatari T, Kawano T, Nakanishi Y, Higaki H et al. Mixture of hyaluronic acid and phospholipid prevents adhesion formation on the injured flexor tendon in rabbits. J Orthop Res 2000; 18(5):835-840.
110. Nakama LH, King KB, Abrahamsson S, Rempel DM. VEGF, VEGFR-1, and CTGF cell densities in tendon are increased with cyclical loading: An in vivo tendinopathy model. J Orthop Res 2006; 24(3):393-400.
111. Nithya M, Suguna L, Rose C. The effect of nerve growth factor on the early responses during the process of wound healing. Biochim Biophys Acta 2003; 1620(1-3):25-31.
112. Noguchi M, Seiler JG 3rd, Boardman ND 3rd, Tramaglini DM, Gelberman RH, Woo SL. Tensile properties of canine intrasynovial and extrasynovial flexor tendon autografts. J Hand Surg 1997; 22A:457-463.
113. Okuda Y, Gorski JP, An KN, Amadio PC. Biochemical, histological, and bio-mechanical analyses of canine tendon. J Orthop Res 1987; 5(1):60-68.
114. Oshiro W, Lou J, Xing X, Tu Y, Manske PR. Flexor tendon healing in the rat: a histologic and gene expression study. J Hand Surg 2003; 28A:814-823.
115. Parreno J, Hart DA. Molecular and mechano-biology of collagen gel contraction mediated by human MG-63 cells: involvement of specific intracellular signaling pathways and the cytoskeleton. Biochem Cell Biol 2009; 87(6):895-904.
116. Pasternak B, Fellenius M, Aspenberg P. Doxycycline impairs tendon repair in rats. Acta Orthop Belg 2006; 72(6):756-760.
117. Pasternak B, Missios A, Askendal A, Tengvall P, Aspenberg P. Doxycycline-coated sutures improve the suture-holding capacity of rat Achilles tendon. Acta Orthop 2007; 78(5):680-686.
118. Pasternak B, Aspenberg P. Metalloproteinases and their inhibitors – diagnostic and therapeutic opportunities in orthopedics. Acta Orthop 2009; 80(6):693-703.
119. Phanish MK, Winn SK, Dockrell ME. Connective tissue growth factor – (CTGF, CCN2) – a marker, mediator and therapeutic target for renal fibrosis. Nephron Exp Nephrol 2010; 114(3):e83-92.
120. Peterson JT. Matrix metalloproteinase inhibitor development and the remode-ling of drug discovery. Heart Fail Rev 2004; 9(1):63-79.
121. Plaas AH, Wong-Palm S, Koob T, Hernandez D, Marchuk L, Frank CB. Pro-teoglycan metabolism during repair of the ruptured medial collateral ligament in skeletally mature rabbits. Arch Biochem Biophys 2000; 374(1):35-41.
122. Pufe T, Petersen W, Tillmann B, Mentlein R. The angiogenic peptide vascular endothelial growth factor is expressed in foetal and ruptured tendons. Virchows Arch 2001; 439(4):579-585.
123. Rees SG, Dent CM, Caterson B. Metabolism of proteoglycans in tendon. Scand J Med Sci Sports 2009; 19(4):470-478.
124. Reno C, Marchuk L, Sciore P, Frank CB, Hart DA. Rapid isolation of total RNA from small samples of hypocellular, dense connective tissues. Biotechni-ques 1997; 22(6):1082-1086.
125. Riccio M, Battiston B, Pajardi G, Corradi M, Passaretti U, Atzei A et al. Effi-ciency of Hyaloglide in the prevention of the recurrence of adhesions after teno-lysis of flexor tendons in zone II: a randomized, controlled, multicentre clinical trial. J Hand Surg 2010; 35E:130-138.
126. Robbins JR, Vogel KG. Regional expression of mRNA for proteoglycans and collagen in tendon. Eur J Cell Biol 1994; 64(2):264-270.

56
127. Robbins JR, Evanko SP, Vogel KG. Mechanical loading and TGF-� regulate proteoglycan synthesis in tendon. Arch Biochem Biophys 1997; 342(2):203-211.
128. Robinson PS, Huang TF, Kazam E, Iozzo RV, Birk DE, Soslowsky LJ. Influ-ence of decorin and biglycan on mechanical properties of multiple tendons in knockout mice. J Biomech Eng 2005; 127(1):181-185.
129. Rosberg HE, Carlsson KS, Höjgård S, Lindgren B, Lundborg G, Dahlin LB. What determines the costs of repair and rehabilitation of flexor tendon injuries in zone II? A multiple regression analysis of data from southern Sweden. J Hand Surg 2003; 28B:106-112.
130. Savage R, Risitano G. Flexor tendon repair using a “six strand” method of re-pair and early active mobilization. J Hand Surg 1989; 14B:396-399.
131. Schnabel LV, Lynch ME, van der Meulen M, Yeager AE, Kornatowski MA, Nixon AJ. Mesenchymal stem cells and insulin-like growth factor-1 gene-enhanced mesenchymal stem cells improve structural aspects of healing in equine flexor digitorum superficialis tendons. J Orthop Res 2009; 27(10):1392-1398.
132. Schönherr E, Hausser H-J. Extracellular matrix and cytokines: a functional unit. Dev Immunol 2000; 7(2-4):89-101.
133. Sciore P, Boykiw R, Hart DA. Semiquantitative reverse transcription-polymerase chain reaction analysis of mRNA for growth factors and growth factor receptors from normal and healing rabbit medial collateral ligament tis-sue. J Orthop Res 1998; 16(4):429-437.
134. Scott A, Khan KM, Duronio V. IGF-1 activates PKB and prevents anoxic apop-tosis in Achilles tendon cells. J Orthop Res 2005; 23(5):1219-1225.
135. Scott A, Cook JL, Hart DA, Walker DC, Duronio V, Khan KM. Tenocyte res-ponses to mechanical loading in vivo: a role for local insulin-like growth factor 1 signaling in early tendinosis in rats. Arthritis Rheum 2007; 56(3):871-881.
136. Scott A, Lian Ø, Bahr R, Hart DA, Duronio V. VEGF expression in patellar tendinopathy: a preliminary study. Clin Orthop Relat Res 2008; 466(7):1598-1604.
137. Scott A, Lian Ø, Roberts CR, Cook JL, Handley CJ, Bahr R et al. Increased versican content is associated with tendinosis pathology in the patellar tendon of athletes with jumper’s knee. Scand J Med Sci Sports 2008; 18(4):427-435.
138. Sharma P, Maffulli N. Biology of tendon injury: healing, modeling and remode-ling. J Musculoskel Neuronal Interact 2006; 6(2):181-190.
139. Shi-Wen X, Leask A, Abraham D. Regulation and function of connective tissue growth factor/CCN2 in tissue repair, scarring and fibrosis. Cytokine Growth Factor Rev 2008; 19(2):133-144.
140. Silfverskiöld KL, Andersson CH. Two new methods of tendon repair: an in vitro evaluation of tensile strength and gap formation. J Hand Surg 1993; 18A:58-65.
141. Silva MJ, Brodt MD, Boyer MI, Morris TS, Dinopoulos H, Amiel D et al. Ef-fects of increased in vivo excursion on digital range of motion and tendon strength following flexor tendon repair. J Orthop Res 1999; 17(5):777-783.
142. Silva MJ, Boyer MI, Gelberman RH. Recent progress in flexor tendon healing. J Orthop Sci 2002; 7(4):508-514.
143. Small JO, Brennen MD, Colville J. Early active mobilisation following flexor tendon repair in zone 2. J Hand Surg 1989; 14B:383-391.
144. Stokes MB, Hudkins KL, Zaharia V, Taneda S, Alpers CE. Up-regulation of extracellular matrix proteoglycans and collagen type I in human crescentic glo-merulonephritis. Kidney Int 2001; 59:532-542.

57
145. Strickland JW, Glogovac SV. Digital function following flexor tendon repair in Zone II: A comparison of immobilization and controlled passive motion tech-niques. J Hand Surg 1980; 5A:537-543.
146. Strickland JW. Development of flexor tendon surgery: twenty-five years of progress. J Hand Surg 2000; 25A:214-235.
147. Szabo RM, Younger E. Effects of indomethacin on adhesion formation after repair of zone II tendon lacerations in the rabbit. J Hand Surg 1990; 15A:480-483.
148. Takeuchi N, Mitsuyasu H, Hotokezaka S, Miura H, Higaki H, Iwamoto Y. Strength enhancement of the interlocking mechanism in cross-stitch peripheral sutures for flexor tendon repair: biomechanical comparisons by cyclic loading. J Hand Surg 2010; 35E:46-50.
149. Tang JB, Wang B, Chen F, Pan CZ, Xie RG. Biomechanical evaluation of flex-or tendon repair techniques. Clin Orthop Relat Res 2001; 386:252-259.
150. Tang JB, Xu Y, Ding F, Wang XT. Tendon healing in vitro: promotion of colla-gen gene expression by bFGF with NF-�B gene activation. J Hand Surg 2003; 28A:215-220.
151. Tang JB. Tendon injuries across the world: treatment. Injury 2006; 37(11):1036-1042.
152. Tang JB. Indications, methods, postoperative motion and outcome evaluation of primary flexor tendon repairs in zone 2. J Hand Surg 2007; 32E:118-129.
153. Tang JB, Cao Y, Zhu B, Xin KQ, Wang XT, Liu PY. Adeno-associated virus-2-mediated bFGF gene transfer to digital flexor tendons significantly increases tendon strength: an in vivo study. J Bone Joint Surg Am 2008; 90(5):1078-1089.
154. Thomopoulos S, Hattersley G, Rosen V, Mertens M, Galatz L, Williams GR et al. The localized expression of extracellular matrix components in healing ten-don insertion sites: an in situ hybridization study. J Orthop Res 2002; 20(3):454-463.
155. Thomopoulos S, Harwood FL, Silva MJ, Amiel D, Gelberman RH. Effect of several growth factors on canine flexor tendon fibroblast proliferation and col-lagen synthesis in vitro. J Hand Surg 2005; 30A:441-447.
156. Thomopoulos S, Das R, Silva MJ, Sakiyama-Elbert S, Harwood FL, Zampiakis E et al. Enhanced flexor tendon healing through controlled delivery of PDGF-BB. J Orthop Res 2009; 27(9):1209-1215.
157. Thomopoulos S, Das R, Sakiyama-Elbert S, Silva MJ, Charlton N, Gelberman RH. bFGF and PDGF-BB for tendon repair: controlled release and biologic ac-tivity by tendon fibroblasts in vitro. Ann Biomed Eng 2010; 38(2):225-234.
158. Tsai WC, Hsu CC, Chou SW, Chung CY, Chen J, Pang JH. Effects of celecoxib on migration, proliferation and collagen expression of tendon cells. Connect Tissue Res 2007; 48(1):46-51.
159. Tsubone T, Moran SL, Amadio PC, Zhao C, An KN. Expression of growth factors in canine flexor tendon after laceration in vivo. Ann Plast Surg 2004; 53(4):393-397.
160. Tsuzaki M, Guyton G, Garrett W, Archambault JM, Herzog W, Almekinders L et al. IL-1� induces COX2, MMP-1, -3, and-13, ADAMTS-4, IL-1� and IL-6 in human tendon cells. J Orthop Res 2003; 21(2):256-264.
161. Vailas AC, Tipton CM, Laughlin HL, Tcheng TK, Matthes RD. Physical activi-ty and hypophysectomy on the aerobic capacity of ligaments and tendon. J Appl Physiol 1978; 44(4):542-546.
162. Vaughan MB, Howard EW, Tomasek JJ. Transforming growth factor-�1 pro-motes the morphological and functional differentiation of the myofibroblast. Exp Cell Res 2000; 257(1):180-189.

58
163. Verdan C. Primary repair of flexor tendons. J Bone Joint Surg Am 1960; 42:647-657.
164. Verjee LS, Midwood K, Davidson D, Essex D, Sandison A, Nanchahal J. Myo-fibroblast distribution in Dupuytren’s cords: correlation with digital contracture. J Hand Surg 2009; 34A:1785-1794.
165. Virchenko O, Skoglund B, Aspenberg P. Parecoxib impairs early tendon repair but improves later remodeling. Am J Sports Med 2004; 32(7):1743-1747.
166. Virchenko O, Fahlgren A, Skoglund B, Aspenberg P. CDMP-2 injection im-proves early tendon healing in a rabbit model for surgical repair. Scand J Med Sci Sports 2005; 15(4):260-264.
167. Vogel KG. What happens when tendons bend and twist? Proteoglycans. J Mus-culoskel Neuron Interact 2004; 4(2):202-203.
168. Vogel KG, Peters JA. Histochemistry defines a proteoglycan-rich layer in bo-vine flexor tendon subjected to bending. J Musculoskelet Neuronal Interact 2005; 5(1):64-69.
169. Wall ME, Banes AJ. Early responses to mechanical load in tendon: role for calcium signaling, gap junctions and intercellular communication. J Muscu-loskelet Neuronal Interact 2005; 5(1):70-84.
170. Wang XT, Liu PY, Tang JB. Tendon healing in vitro: genetic modification of tenocytes with exogenous PDGF gene and promotion of collagen gene expres-sion. J Hand Surg 2004; 29A:884-890.
171. Wang XT, Liu PY, Xin KQ, Tang JB. Tendon healing in vitro: bFGF gene transfer to tenocytes by adeno-associated viral vectors promotes expression of collagen genes. J Hand Surg 2005; 30A:1255-1261.
172. Wight TN. Versican: a versatile extracellular matrix proteoglycan in cell biolo-gy. Curr Opin Cell Biol 2002; 14(5):617-623.
173. Wiig M, Hanff G, Abrahamsson SO, Lohmander LS. Division of flexor tendons causes progressive degradation of tendon matrix in rabbits. Acta Orthop Scand 1996; 67(5):491-497.
174. Wiig M, Abrahamsson SO, Lundborg G. Tendon repair – cellular activities in rabbit deep flexor tendons and surrounding synovial sheaths and the effects of hyaluronan: an experimental study in vivo and in vitro. J Hand Surg 1997; 22A:818-825.
175. de Wit T, de Putter D, Tra WM, Rakhorst HA, van Osch GJ, Hovius SE et al. Auto-crosslinked hyaluronic acid gel accelerates healing of rabbit flexor ten-dons in vivo. J Orthop Res 2009; 27(3):408-415.
176. Wong JK, Cerovac S, Ferguson MW, McGrouther DA. The cellular effect of a single interrupted suture on tendon. J Hand Surg 2006; 31B:358-367.
177. Wong JK, Bennett W, Ferguson MW, McGrouther DA. Microscopic and histo-logical examination of the mouse hindpaw digit and flexor tendon arrangement with 3D reconstruction. J Anat 2006; 209(4):533-545.
178. Wong JK, Lui YH, Kapacee Z, Kadler KE, Ferguson MW, McGrouther DA. The cellular biology of flexor tendon adhesion formation: an old problem in a new paradigm. Am J Pathol 2009; 175(5):1938-1951.
179. Wu YF, Chen CH, Cao Y, Avanessian B, Wang XT, Tang JB. Molecular events of cellular apoptosis and proliferation in the early tendon healing period. J Hand Surg 2010; 35A:2-10.
180. Xiong Y, Zhang Z. Experimental studies on decorin in suppression of postoper-ative flexor tendon adhesion in rabbits. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2006; 20(3):251-255.
181. Yoon JH, Halper J. Tendon proteoglycans: biochemistry and function. J Muscu-loskelet Neuronal Interact 2005; 5(1):22-34.

59
182. Zhang F, Liu H, Stile F, Lei MP, Pang Y, Oswald TM et al. Effect of vascular endothelial growth factor on rat Achilles tendon healing. Plast Reconstr Surg 2003; 112(6):1613-1619.
183. Zhang G, Ezura Y, Chervoneva I, Robinson PS, Beason DP, Carine ET et al. Decorin regulates assembly of collagen fibrils and acquisition of biomechanical properties during tendon development. J Cell Biochem 2006; 98(6):1436-1449.
184. Zhao C, Amadio PC, Tanaka T, Kutsumi K, Tsubone T, Zobitz ME et al. Effect of gap size on gliding resistance after flexor tendon repair. J Bone Joint Surg Am 2004; 86(11):2482-2488.
185. Zhao C, Zobitz ME, Sun YL, Predmore KS, Amadio PC, An KN et al. Surface treatment with 5-fluorouracil after flexor tendon repair in a canine in vivo mod-el. J Bone Joint Surg Am 2009; 91(11):2673-2682.
186. Özgenel GY. The effects of a combination of hyaluronic acid and amniotic membrane on the formation of peritendinous adhesions after flexor tendon sur-gery in chickens. J Bone Joint Surg Br 2004; 86(2):301-307.

����!��/ ��������!������������������� �������������� ������������������� ������� ����������������������������
����� -��1�#�������1������2���������
������ ������� �������� ����1������2���������3�!������!��/ ���23����������2�������� 2���������. ������� �4����5���������1����������� �������� �6��������7� �$5���1 �� 1���. � ��3�51����1������ 2������������� �.������ ���������2��1 ���1��1�� ���#�������8��� 1���/$���� ������!�������#��� ��������� ����1������2��������4�9: �� ����;���� 23�())�3��1�� ���5�����.���1���� ��1������<8��� 1���/�$���� ������!������#��� ��������� ����1������2���������=4>
#��� �.�����-���.��������4��4�� �-�.�-�-��-��/�'%()0)�
������������������� �����
����� �����