Biomarker tests in saliva
3
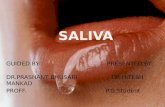
Discussion.—The survey indicates that dental schools in the United States and Canada have increased their teach- ing of direct resin-based composite restoration repair tech- niques. Ten years ago only 71% of the schools included formal lecture teaching of such repair techniques, but the new survey found 88% were currently teaching these methods and potentially 96% of the respondents could be doing so within the next 5 years. This indicates that the future dental care of patients will minimize the use of un- necessary replacements for these restorations. Because the graduates of today will likely be practicing into the 2050s, their experiences in dental school have the potential to influence patient care for many years. Clinical Significance.—Minimally invasive dental techniques can extend the longevity of dental restorations, reduce detrimental effects on teeth caused by more invasive techniques, and save the patient money and discomfort. This better serves patient interests. The ADA should be encouraged to consider including valid minimally invasive techniques such as the repair of resin-based composite restorations in its procedure codes. Lynch CD, Blum IR, Frazier KB, et al: Repair or replacement of defec- tive direct resin-based composite restorations: Contemporary teaching in U.S. and Canadian dental schools. J Am Dent Assoc 143:157-163, 2012 Reprints available from CD Lynch, Restorative Dentistry, Tissue Engi- neering and Reparative Dentistry, School of Dentistry, Cardiff Univ, Heath Park, Cardiff, CF14 4XY, Wales; e-mail: [email protected] Saliva Biomarker tests in saliva Background.—Significant advances have been made in the techniques for detecting biomarker signals in oral sam- ples and in the engineering and development of microflui- dic approaches to oral-based point-of-care methods. Both local and systemic conditions are now targeted for salivary diagnostic efforts. Applications to periodontal disease man- agement, systemic diseases, and pharmacogenomic studies were discussed. Periodontal Disease Management.—Periodontal in- fections have been linked to several other polygenic diseases (Fig 1), making their diagnosis and treatment an important component in overall health care. The diag- nostic methods used in clinical practice today for peri- odontal disease cannot detect the onset of inflammation and identify patients at greatest risk for disease. New point-of-care devices for periodontal surveillance may require less training and fewer resources than current ap- proaches. This could facilitate the wider use of these de- vices and achieve simpler, less intensive treatment, and more cost-effective care. Screening will be accomplished in many settings rather than just within a dental office. Fig 1.—Interrelationship between changes in the skeleton during bone metabolic diseases such as periodontitis and osteoporosis. The release of oral fluid- and saliva-based biomarkers of disease may predict both tooth-site and skeletal bone alterations affected by pathogens, bone turnover, or biomechanical influences (Rios and Giannobile, 2010). (Courtesy of Giannobile WV, McDevitt JT, Niedbala RS, et al: Trans- lational and clinical applications of salivary diagnostics. Adv Dent Res 23:375-380, 2011.) Volume 58 Issue 5 2013 271
Transcript of Biomarker tests in saliva

Discussion.—The survey indicates that dental schoolsin the United States and Canada have increased their teach-ing of direct resin-based composite restoration repair tech-niques. Ten years ago only 71% of the schools includedformal lecture teaching of such repair techniques, but thenew survey found 88% were currently teaching thesemethods and potentially 96% of the respondents could bedoing so within the next 5 years. This indicates that thefuture dental care of patients will minimize the use of un-necessary replacements for these restorations. Becausethe graduates of today will likely be practicing into the2050s, their experiences in dental school have the potentialto influence patient care for many years.
Figrelbolat
Clinical Significance.—Minimally invasivedental techniques can extend the longevity of
1.—Interrelationship between changes in the skeleton during bone mease of oral fluid- and saliva-based biomarkers of diseasemay predict botne turnover, or biomechanical influences (Rios and Giannobile, 2010). (Cional and clinical applications of salivary diagnostics. Adv Dent Res 23:37
dental restorations, reduce detrimental effectson teeth caused by more invasive techniques,and save the patient money and discomfort.This better serves patient interests. The ADAshould be encouraged to consider includingvalid minimally invasive techniques such asthe repair of resin-based composite restorationsin its procedure codes.
Lynch CD, Blum IR, Frazier KB, et al: Repair or replacement of defec-tive direct resin-based composite restorations: Contemporaryteaching in U.S. and Canadian dental schools. J Am Dent Assoc143:157-163, 2012
Reprints available from CD Lynch, Restorative Dentistry, Tissue Engi-neering and Reparative Dentistry, School of Dentistry, Cardiff Univ,Heath Park, Cardiff, CF14 4XY, Wales; e-mail: [email protected]
SalivaBiomarker tests in saliva
Background.—Significant advances have been made inthe techniques for detecting biomarker signals in oral sam-ples and in the engineering and development of microflui-dic approaches to oral-based point-of-care methods. Bothlocal and systemic conditions are now targeted for salivarydiagnostic efforts. Applications to periodontal disease man-agement, systemic diseases, and pharmacogenomic studieswere discussed.
Periodontal Disease Management.—Periodontal in-fections have been linked to several other polygenic
diseases (Fig 1), making their diagnosis and treatmentan important component in overall health care. The diag-nostic methods used in clinical practice today for peri-odontal disease cannot detect the onset of inflammationand identify patients at greatest risk for disease. Newpoint-of-care devices for periodontal surveillance mayrequire less training and fewer resources than current ap-proaches. This could facilitate the wider use of these de-vices and achieve simpler, less intensive treatment, andmore cost-effective care. Screening will be accomplishedin many settings rather than just within a dental office.
etabolic diseases such as periodontitis and osteoporosis. Theh tooth-site and skeletal bone alterations affected by pathogens,ourtesy of Giannobile WV, McDevitt JT, Niedbala RS, et al: Trans-5-380, 2011.)
Volume 58 � Issue 5 � 2013 271

More personalized treatments may also be developedthrough large-scale screening efforts. The newer devicesoffer the potential for more readily identifying at-riskgroups and increasing access to treatment for underservedcommunities, which will improve public oral health ingeneral.
The emerging technologies include lab-on-a-chip(LOC) technologies that were originally developed for sys-temic diseases. Proteomic or multianalyte approaches toidentifying periodontal diseases may reveal periodontaldisease ‘‘signatures’’ denoting risk status. Disease predictioncan be based on detecting a panel of salivary biomarkers.Matrix metalloproteinase-8, microbial factors, and proinflam-matory cytokines such as interleukin-1 beta are amongthe salivary biomarkers now available. Oral fluid-based bio-markers in local oral wound fluids help predict responses totherapies such as periodontal surgery combined with matrixmetalloproteinase inhibitionor tissueengineering constructs.Wound repair biomarkers also help in determining tissuehealing responses with intraoral soft tissue transplantationprocedures.
Because periodontal disease is a multifactorial disease,biologic phenotypes may be valuable because theycapture the microbial and inflammatory status at the individ-ual patient level. Knowing this will help develop disease clas-sifications to which targeted therapeutic approaches areattached. Recent data on the genetic, microbial, and proteinsaliva-based biomarkers support the predictive value of a pro-pensity for gingival inflammation or periodontal bonydestruction.
Obstacles to be addressed before using salivary bio-markers for periodontal disease management includebenchmarking validation of periodontal diagnostics withexisting gold standards of disease, including alveolar boneheight and clinical attachment level. Oral healthcare pro-viders also need to accept these new techniques and theconcept of providing mass screening of populations fororal and systemic disease. If more efficient periodontal ther-apy is the outcome, clinicians will be more likely to use thenew approaches. More emphasis will be needed on clini-cian education in diagnostics, disease risk, and disease pre-vention through the public health sector before the newdiagnostics will be incorporated into routine clinicalpractice.
Early Diagnosis of Systemic Disease.—The outra-geous expenses of medical care provide the motivationfor developing new tools to help achieve more affordablehealth care. Promising bridges between health care and mi-croelectronics have been made with microfluidic LOC ap-proaches. In addition, the micro-total analysis systemparadigm has helped to define important goals. However,
272 Dental Abstracts
broad-based release of workable devices remains to beachieved. The network of macroscopic laboratory-basedinfrastructure needed to process samples, detect analytes,process data, and handle reagents dictates that theplatforms developed will be better described as ‘‘chips-in-a-lab’’ rather than true LOC. Work is also needed ondeveloping universal mini-detection ensembles that permitrapid prototyping and readily adapt to newly validatedbiomarkers.
A programmable-bio-nano-chip (PBNC) has beendeveloped that synergizes components and achievementsfrom nanotechnology, clinical chemistry, bioinformatics,microfluidics, optics, image analysis, and pattern recogni-tion. The PBNC system uses approximately 300-mm-diam-eter bead sensors composed of agarose nanonets thatpopulate a microelectromechanical support structurewith integrated microfluidic elements. The beads are anefficient and selective protein capture medium that per-mits the analysis of complex fluid samples. The PBNCuses a flexible assay design and offers a diverse collectionof validated analytes. Its modular design means newbiomarker samples can be rapidly deployed. The assaysfor nucleic acids, proteins, and cells are arranged to createanalytical test modalities for various disease types. Currentstudies are exploring this system for detecting majorcardiac diseases as well as oral, ovarian, and prostatecancers.
Pharmacogenomic Applications.—Pharmacogenom-ics seeks to define the primary outcomes of clinicalresponse and differentiation; risk identification; dose se-lection guidance; susceptibility, resistance, and differen-tial disease diagnosis; and polymorphic drug targets.Therefore, the results of a pharmacogenomics test aremuch more informative than traditional therapeuticdrug monitoring. These results can help guide physi-cians on the best therapeutic selection for a particularperson, including dose adjustment based on a metabolicprofile. Adverse reactions or death through accidentaloverdose may be avoided by using these tests. Pharma-cogenomics is based on collecting cells from whichDNA can be extracted, amplified, and analyzed. Themouth routinely sheds cells or they can easily be loos-ened with a brush.
Several components must be in place to expand the useof oral-based diagnostics. First, the DNAmust remain stablethroughout collection and storage. Commercial kits for thisare expensive and not very user-friendly. New collectors willbe needed. Second, standard procedures must be devel-oped to isolate the DNA from the collector and simplifyrelevant genes efficiently. The information currently ob-tained is limited. Third, the outcomes from testing mustbe equivalent to current practices.

Clinical Significance.—Various milestonesremain to be achieved before oral testing willbecome a standard approach. The literaturemust show that blood or oral fluids are viablefor pharmacogenomics. The costs for oral fluidcollection and processing will have to becompetitive with those for handling blood.Finally, oral fluids must be included in pharma-cogenomics regulations or guidance docu-ments. Nonscientists will look at suchdocuments to avoid legal difficulties. Healthcare systems must also be able to pay for thesampling and testing. Further, carefullycontrolled studies will be needed to create the
FigSalan
body of evidence supporting regulatoryapproval.
Giannobile WV, McDevitt JT, Niedbala RS, et al: Translational andclinical applications of salivary diagnostics. Adv Dent Res 23:375-380, 2011
Reprints available from D Malamud, Dept of Basic Sciences, NewYork Univ College of Dentistry, and Dept of Medicine, New YorkUniv School of Medicine, New York, NY 10010; e-mail:[email protected]
Salivary diagnostics
.—Discovery cycle. (Courtesy of Slavkin HC, Fox CH, Meyer DM:ivary diagnostics and its impact in dentistry, research, education,d the professional community. Adv Dent Res 23:381-386, 2011.)
Background.—Salivary diagnostics is a biomedicalinnovation that offers the potential to create practical,point-of-care (POC) clinical instruments that offer conve-nience, practicality, and comfort in use for both dentistsand medical practitioners. Patient care is currently shapedby individual insurance coverage and adoption decisions,with health care providers and payers serving as gate-keepers and determinants of the acceptance and usefulnessof biomedical interventions. The oral-systemic healthconnection is well established, but it is now being realizedthat the oral cavity contains a wealth of information aboutthe individual’s overall health. Scientific discoveries havecome from cellular, developmental, and molecular biologyand changed the understanding of biologic processes, hu-man genetic variations, adaptability, and the causes and pro-cesses involved in human disease. Many scientific advancesrequire major revisions in how one learns, what can belearned, and how information is integrated into health pro-fessions. A gap exists currently between scientific andbehavioral research and the physicians, dentists, nurses,and pharmacists who serve on the front lines. The processof translating research into clinical practice was explainedwith respect to salivary diagnostics.
Research Process.—Since serum components werediscovered in saliva, scientists have been pursuing diag-nostic applications in oral diseases, systemic diseases, in-fectious diseases, hormone levels, malignancy, and drugmonitoring. For research to advance, the components ofthe discovery cycle must be properly positioned (Fig).People are needed to generate research hypotheses anddesign appropriate experiments to test those hypotheses.A pipeline of researchers is also needed. If experiments or
interventions are to be conducted, the appropriate infra-structure must be in place—not just buildings and facil-ities but an environment conducive to and supportive ofresearch. Funding then needs to be in place, which willguide decisions concerning research priorities. After theresearch is completed and data have been collected andanalyzed, there must be a method for scientific exchange.Finally, information transfer must take place so that prac-titioners and consumers can benefit from the findings. Asignificant challenge exists with respect to shorteningthe time between basic research and commercializationof new products. Currently, there are salivary diagnosticproducts in the market to detect HIV and human papillo-mavirus and to monitor drug and alcohol use. The com-mercial use of saliva for detecting local cancer (oralsquamous cell carcinoma) is quickly approaching and fordetecting more distant cancer (breast and pancreatic) ison the distant horizon.
Volume 58 � Issue 5 � 2013 273




![Realising the Potential of Urine and Saliva as Diagnostic ... · quality, and with the total protein content in saliva less than 1 % [52], expressing a salivary biomarker as a ratio](https://static.fdocuments.net/doc/165x107/5e3fdad8edf722015d02e05e/realising-the-potential-of-urine-and-saliva-as-diagnostic-quality-and-with.jpg)