Billiary Injury

of 35
-
Upload
drarish-mahmood -
Category
Documents
-
view
221 -
download
0
Transcript of Billiary Injury
-
8/7/2019 Billiary Injury
1/35
-
8/7/2019 Billiary Injury
2/35
-
8/7/2019 Billiary Injury
3/35
Open Cholecystectomy: 0.2%
Laproscopic cholecystectomy 0.6 %
-
8/7/2019 Billiary Injury
4/35
Poor visualisation
Difficult or Varriant anatomy
Unproper techieques
-
8/7/2019 Billiary Injury
5/35
Schwartzs Principles of Surgery, 8th Ed.,McGraw-Hill Companies, 2005.
Mortele, Koenradd et al.,Am J of Roent,August 2001.
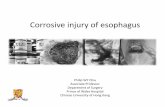
Common variants: A. Low cystic duct insertion, (10%); B. Parallel at least 2-cm
with common hepatic duct (15-25%); F,G,H. Medial cystic duct insertion (10-
17%). Uncommon variants: C. High fusion with hepatic duct; D. Fusion at right
hepatic duct; F. No cystic duct.
-
8/7/2019 Billiary Injury
6/35
Blumgart LH. Surg Clin N Am. 1994.74.4
-
8/7/2019 Billiary Injury
7/35
-
8/7/2019 Billiary Injury
8/35
-
8/7/2019 Billiary Injury
9/35
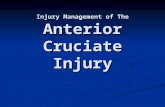
Mortele, Koenradd et al.,Am J of Roent,August 2001.
Common biliary variant in 34-year-old woman with recurrent
cholestasis after cholecystectomy. MRC showing triple confluence of
right anterior duct (small arrowhead), right posterior duct (small arrow),
and left hepatic duct (large arrowhead). Cystic stump (large arrow).
-
8/7/2019 Billiary Injury
10/35
Mortele, Koenradd et al.,Am J of Roent,August 2001.
Uncommon biliary variant in 62-year-old woman after
cholecystectomy. MRC showing high insertion of cystic duct
(arrow) into common hepatic duct (arrowhead).
-
8/7/2019 Billiary Injury
11/35
Mis identificatin: Ecission,incission
,laceration and cliping
Electrocautry: thermal injury causes stricture
Mechaincal trauma
-
8/7/2019 Billiary Injury
12/35
Lahey Clinic, Burlington, MA.1994
-
8/7/2019 Billiary Injury
13/35
-
8/7/2019 Billiary Injury
14/35
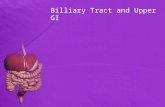
Bismuth classification of bile duct strictures
Lahey Clinic, Burlington, MA.1994
-
8/7/2019 Billiary Injury
15/35
(A) cystic duct leaks or leaks from ducts in
liver beds
(B) occlusion of part of biliary tree almost
aberrant RHD (C) transection without ligation of aberrant
RHD
(D) Lateral injuries to major bile ducts
(E) sub devided as per bismuth classification
-
8/7/2019 Billiary Injury
16/35
Neuhaus P, Humbolt Univ. of BerlinBJS.2005.92. 76-82
-
8/7/2019 Billiary Injury
17/35
-
8/7/2019 Billiary Injury
18/35
CLINCALY PATIENTS R DEVIDED IN 3 GROUPS
(1) Detected Peroperatively
(2)Delayed Presentation >24 hours averagely
7 days
Long symptoms free interval 1 month to 1
year
-
8/7/2019 Billiary Injury
19/35
General malaise
Nausea
Vomiting
Anorexia
Abdominal pain
Low grade fever
With peritonitisWith obstrctive jaundice
-
8/7/2019 Billiary Injury
20/35
Present with obstructive jaundice due to
stricture development
-
8/7/2019 Billiary Injury
21/35
Ultrasound with subsequent aspiration of
collection
MRCP
ERCP
PTC
CT
-
8/7/2019 Billiary Injury
22/35
Is there subhepatic abscess or collection?
Is there ongoing bile leakage ?
What is the level of biliary injury ? Are there associated vascular injuries /
Is there evidence of lobar atrophy ?
-
8/7/2019 Billiary Injury
23/35
An ERC of same patient showing a leak
from the cystic duct stump (arrow). Note
the filling of the pancreatic duct.
Schwartzs Principles of Surgery, 8th Ed.,McGraw-Hill Companies, 2005.
CT scan of patient with bile leak aftercholecystectomy. The short arrows
indicate the intraperitoneal collections.
Both air and bile is seen in the gallbladder
bed (long arrow) as is a surgical clip.
-
8/7/2019 Billiary Injury
24/35
Bile Duct StrictureBile duct stricture at cystic duct origin in 17-year-old boy who presented with
obstructive jaundice 1 month after laparoscopic cholecystectomy that wasconverted to open cholecystectomy because of difficulty in extracting impacted
cystic duct calculus.
Khalid, Tahir et al.,Am J of Roent, December 2001; 177:1347-1352.
MRCP showing moderate intrahepatic and
extrahepatic biliary dilatation caused by short tight
stricture (arrow) of common bile duct where cystic
duct origin once began. Intact distal bile duct
segment is seen below stricture.
PTC showing stricture (arrow) that was
subsequently balloon-dilated.
-
8/7/2019 Billiary Injury
25/35
Excisional Injury
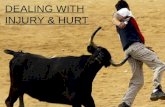
Khalid, Tahir et al.,Am J of Roent, December 2001; 177:1347-1352.
Excision injury with ligation in 35-y/o woman who presented 1
week after laparoscopic cholecystectomy with right upperquadrant pain and jaundice.
ERCP image showing distal one third of bile duct
with abrupt cutoff (arrow) and multiple surgical
clips in subhepatic area.
MRCP showing moderate intrahepatic biliary
dilatation and cutoff approx. 1 cm distal to
bifurcation caused by ligation injury. Segment of
extrahepatic bile duct 1.8 cm long is missing
(arrows).
-
8/7/2019 Billiary Injury
26/35
Cystic Duct Leak
Khalid, Tahir et al.,Am J of Roent, December 2001; 177:1347-1352.
ERCP image confirming subhepatic bile leak (arrow).MRCP showing fluid collection (curved
arrows) adjacent to cystic duct remnant
(straight arrow).
-
8/7/2019 Billiary Injury
27/35
Right Aberrant Duct Excision
Park, Mi-Suk et al.,Am J of Roent, December 2004.
Hepatobiliary
scintigram obtained 90
min after injection of
iminodiacetic acid, 2
months after MRCP,
shows photon-defect
area (arrows) in right
lobe of liver.
56-y/o man with mild abdominal discomfort for 21 days after laparoscopic cholecystect
Coronal MRCP obtained
before mangafodipir
trisodium (MnDPDP)enhancement with thick-
slice half-Fourier RARE
sequence showing
mildly dilated and
disconnected right
posterior duct (arrow).
Max-intensity image from
coronal 3D volumetric
interpolated T1-weightedgradient-echo image
obtained 30 min after
injection of MnDPDP
showing opacification of
right posterior duct (arrow)
suggesting possible partial
ligation of aberrant right
posterior duct.
ERCP image with
right posterior duct
not seen.
-
8/7/2019 Billiary Injury
28/35
Stricture with Cystic Duct Leak
Park, Mi-Suk et al.,Am J of Roent, December 2004.
ERCP image showingpartial stricture (thin arrow)
of common bile duct with
bile leakage (thick arrow).
35-y/o man with abdominal pain and fever for 10 days after laparoscopic cholecystect
Coronal MRC obtainedbefore mangafodipir
trisodium (MnDPDP)
enhancement with thin-
section half-Fourier RARE
sequence shows narrowing
of common bile duct (thin
arrow) with abnormal fluid
collection (thick arrow).
Coronal 3D volumetricinterpolated T1-weighted
gradient-echo image obtained 30
min after injection of MnDPDP
showing enhanced extrahepatic
duct, in spite of a narrowing
segment (thin arrow), with
extravasation of contrast agent
(thick arrow).
-
8/7/2019 Billiary Injury
29/35
Biliary catheter decompression bile tract and
to control bile leaks
Percutaneuos drainage of bile collection
-
8/7/2019 Billiary Injury
30/35
Balloon dilation and stents for strictures
T-Tube placement
Primary end to end anastomosis
Biliary anastomosis with jejunal loops
-
8/7/2019 Billiary Injury
31/35
Blumgart LH, Surg of the Liver & Biliary tract, 1994
-
8/7/2019 Billiary Injury
32/35
Lahey Clinic, Burlington, MA.1994
-
8/7/2019 Billiary Injury
33/35
Blumgart LH : Surg N Am; 1994, vol. 74 no. 4
A. Percutaneous trans-enteric
B. Percutaneous transhepatic
C. U tube
D. Internal small silicone stentanchored to mucosa
-
8/7/2019 Billiary Injury
34/35
Blumgart LH,Surgery of the Liver and Biliary Tract, 1994
Burried Subcutaneous
Stoma, marked by clip
Open skin stoma
Warko Karnadihardja-BDG
-
8/7/2019 Billiary Injury
35/35
Preventive measures
Use 30 degree high quality image
laproscope
Apply cephalic traction to fundus and
lateral traction to infundibulum
Expose critical view of safety
Dissect cystic duct where it joins
G.bladderPerform routine intra operative
cholangiography