Bilirubin Secretion, Jaundice and Evaluation of Liver · PDF fileBilirubin Secretion, Jaundice...
24
1 Bilirubin Secretion, Jaundice and Evaluation of Liver Function Howard J. Worman, M. D. Evaluation of Liver Disease and Hepatic Function History Physical Examination Laboratory Tests Sometimes Radiological/Nuclear Medicine Sometimes Liver Biopsy
Transcript of Bilirubin Secretion, Jaundice and Evaluation of Liver · PDF fileBilirubin Secretion, Jaundice...

1
Bilirubin Secretion,Jaundice and Evaluation
of Liver FunctionHoward J. Worman, M. D.
Evaluation of Liver Disease andHepatic Function
HistoryPhysical ExaminationLaboratory TestsSometimes Radiological/Nuclear MedicineSometimes Liver Biopsy

2
Jaundice occurs as a result of excess bilirubin inthe blood. It is a hallmark of liver disease butnot always present in liver disease. Jaundiceoccurs when the liver fails to adequatelysecrete bilirubin from the blood into the bile.To understand how jaundice occurs, you mustfirst understand bilirubin synthesis,metabolism and secretion.

3
BilivirdinReductase
Kikuchi et al.NatureStructuralBiology 8, 221 -225 (2001)
HemeOxygenase
Schuller et al.NatureStructuralBiology 6, 860 -867 (1999)

4
Bilirubin is frequentlydepicted as a lineartetrapyrrole.
However, intramolecularhydrogen bonding fixesit in a rigid structure thatblocks exposure of itspolar groups to aqueoussolvents, making it veryinsoluble in blood.

5
OATP-C?
Bilirubin in Blood is Bound to Albumin: Uptake intoHepatocyte at Basolateral (Sinusoidal) Membrane
Some bilirubinstored in cytosol boundto proteins
Bilurubin UDP-glucuronosyltransferase is localized to the endo-plasmic reticulum; it catalyzes conjugation to a diglucuronide, making it more water soluble.
A: Labeling of periphery of cell hepatocyte nucleusB: Labeling of ER with antibody to UDP-glucuronosyltransferase

6
Alternative RNA splicing of different first exons ofUGT1 gives different isoforms with different substratespecificities, some for bilirubin and others to differentsubstrates, such as phenol.
7
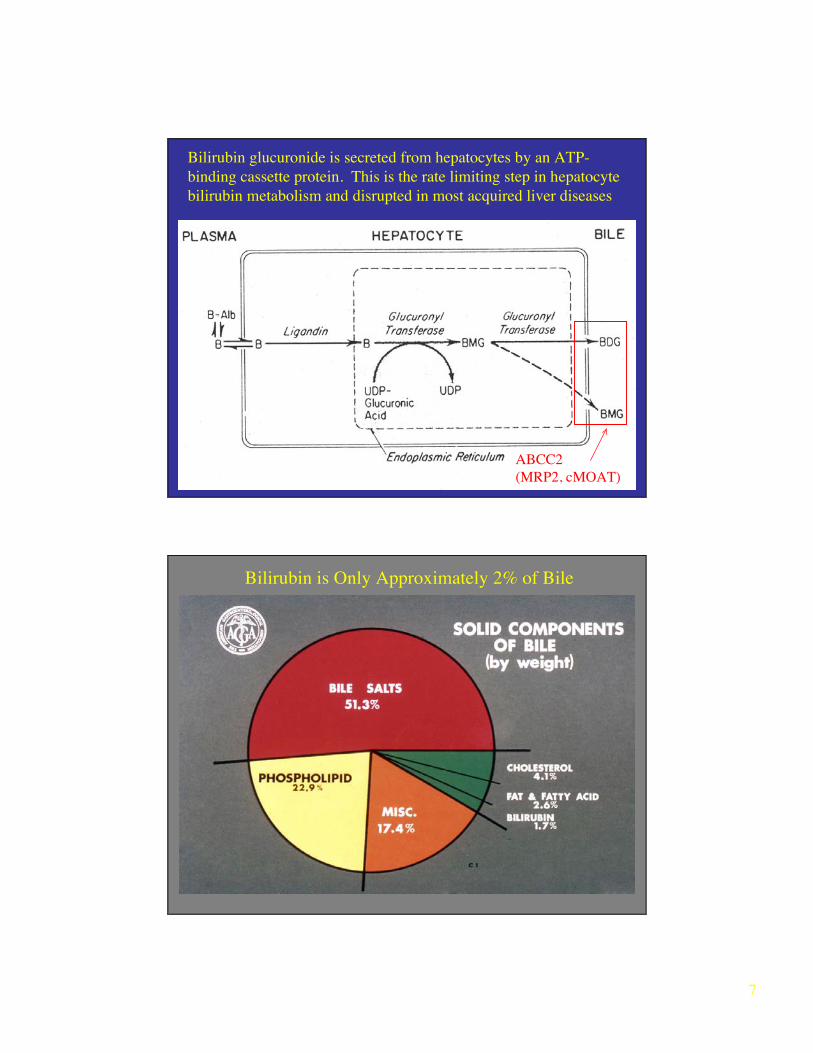
ABCC2(MRP2, cMOAT)
Bilirubin glucuronide is secreted from hepatocytes by an ATP-binding cassette protein. This is the rate limiting step in hepatocytebilirubin metabolism and disrupted in most acquired liver diseases
Bilirubin is Only Approximately 2% of Bile

8
Stercobilins/Urobilins in Stool
Some urobilinogenexcreted by kidney
Diagnostic Consequences ofEnterohepatic Circulation of Bilirubin
• In hepatocyte dysfunction (hepatocellular)– May see increased urobilinogen in urine because it is
less efficiently reabsorbed by hepatocytes• In biliary obstruction
– Stools may appear white because bilirubin does not getinto intestine and therefore not converted tostercobilins/urobilins
– No urobilinogen detected in urine

9
Measurement of Bilirubin in Blood
• Normally ≤17 µM (1 mg/dl)– >35 µM: can begin to detect jaundice clinically, (sclera,
mucus membranes early)– Discoloration of skin with higher concentrations
• When measured precisely (e. g. by HPLC), around96% of serum bilirubin is unconjugated
• Clinical laboratory generally “overestimates” amountof conjugated bilirubin (up to 30%) because of method– reported as “total,” “direct” (approximates conjugated) and
“indirect” (approximates unconjugated)
van den Berghand
MullerReaction (1916)
Using this method,20% to 30% serumdirect bilirubin isnormal value
R R
CONJUGATED
BILIRUBIN
UNCONJUGATED
BILIRUBIN
N+
N
SO3H
+ + ACCELERATOR
(ALCOHOL, CAFFEINE)
TOTAL – DIRECT INDIRECT=
TOTAL DIAZO REACTION OF PLASMA

10
Excess conjugated bilirubin in serum may be excreted by kidneys (dark urine).Albumin-bound unconjugated bilirubin cannot be excreted by kidneys.
With longstanding elevated serum conjugated bilirubin, less is in urine because of covalent binding to albumin.
Causes ofHyperbilirubinemia and
Jaundice

11

12

13
Most Common Cause of UnconjugatedHyperbilirubinemia Western Countries
Gilbert syndrome is not really a “disease” but a normal variant.

14
High blood concentrations of lipid solubleunconjugated bilirubin in infants that alsohave poorly developed blood-brain barrier
can lead to kernicterus (brain damagecaused by bilirubin deposition).
Treatments include exchance transfusionand phototherapy. Heme oxygenase
inhibitors are also being studied for thisindication.
Treatment of Neonatal Jaundice by Phototherapy
Less intramolecular hydrogen bonding of E diasteriomers make them more aqueous soluble for renal excretion.
15
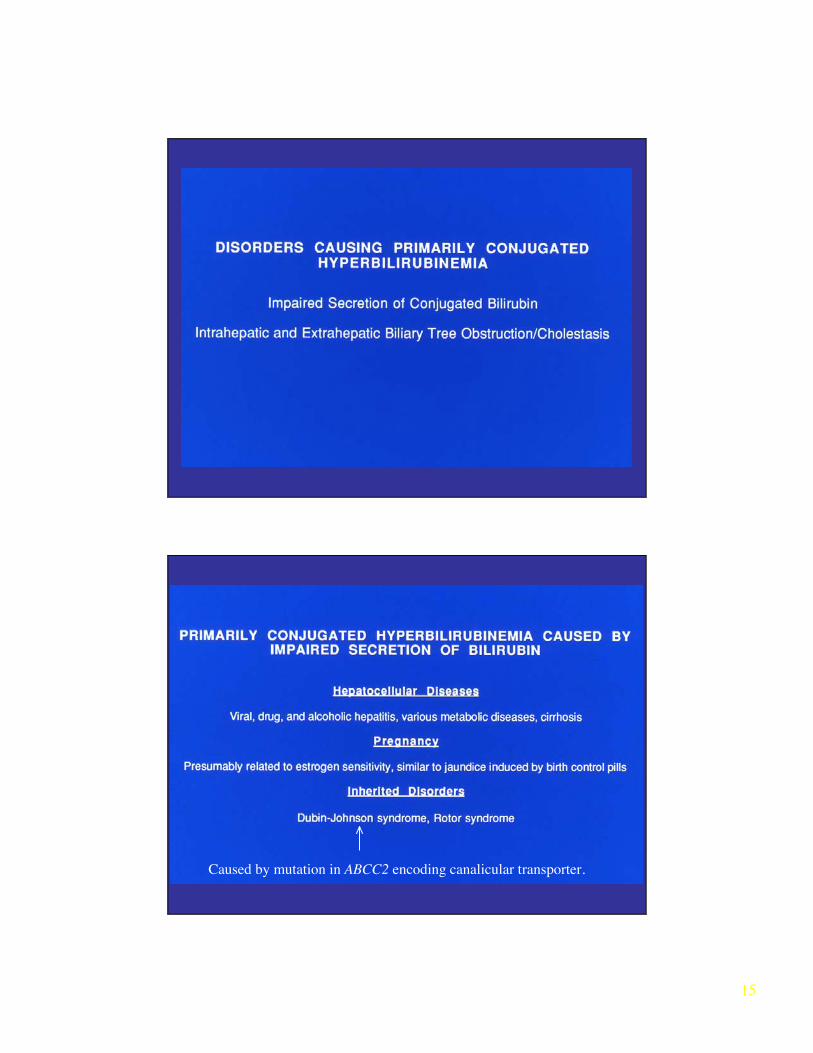
Caused by mutation in ABCC2 encoding canalicular transporter.

16
With abnormal secretion from hepatocytes, most excess bilirubin inblood is conjugated by can get “mixed picture” because of
“backup” of unconjugated bilirubin.

17
Laboratory Tests inLiver Diseases

18
19
20
“Liver Enzymes”
21

22

23

24
Liver Biopsy in the Evaluation of Liver Disease
Dr. Lefkowitch Next