Biliary Tract and Liver Complications in Polycystic Kidney...
11
CLINICAL EPIDEMIOLOGY www.jasn.org Biliary Tract and Liver Complications in Polycystic Kidney Disease Parminder K. Judge,* †‡ Charlie H.S. Harper,* † Benjamin C. Storey,* †‡ Richard Haynes,* †‡ Martin J. Wilcock, ‡ Natalie Staplin, † Raph Goldacre, § Colin Baigent,* † Jane Collier, | Michael Goldacre, § Martin J. Landray,* †§ Christopher G. Winearls, ‡ and William G. Herrington †‡ *Medical Research Council–Population Health Research Unit, † Clinical Trial Service Unit and Epidemiological Studies Unit, and § Big Data Institute, Nuffield Department of Population Health, University of Oxford, Oxford, United Kingdom; and ‡ Oxford Kidney Unit and | Department of Gastroenterology, Oxford University Hospitals National Health Service Foundation Trust, Oxford, United Kingdom ABSTRACT Polycystic liver disease is a well described manifestation of autosomal dominant polycystic kidney disease (ADPKD). Biliary tract complications are less well recognized. We report a 50-year single-center experience of 1007 patients, which raised a hypothesis that ADPKD is associated with biliary tract disease. We tested this hypoth- esis using all England Hospital Episode Statistics data (1998–2012), within which we identi fied 23,454 people with ADPKD and 6,412,754 hospital controls. Hospitalization rates for biliary tract disease, serious liver complications, and a range of other known ADPKD manifestations were adjusted for potential confounders. Compared with non- ADPKD hospital controls, those with ADPKD had higher rates of admission for biliary tract disease (rate ratio [RR], 2.24; 95% confidence interval [95% CI], 2.16 to 2.33) and serious liver complications (RR, 4.67; 95% CI, 4.35 to 5.02). In analyses restricted to those on maintenance dialysis or with a kidney transplant, RRs attenuated substantially, but ADPKD remained associated with biliary tract disease (RR, 1.19; 95% CI, 1.08 to 1.31) and perhaps with serious liver complications (RR, 1.15; 95% CI, 0.98 to 1.33). The ADPKD versus non-ADPKD RRs for biliary tract disease were larger for men than women (heterogeneity P,0.001), but RRs for serious liver complications appeared higher in women (heterogeneity P,0.001). Absolute excess risk of biliary tract disease associated with ADPKD was larger than that for serious liver disease, cerebral aneurysms, and inguinal hernias but less than that for urinary tract infections. Overall, biliary tract disease seems to be a distinct and important extrarenal complication of ADPKD. J Am Soc Nephrol 28: 2738–2748, 2017. doi: https://doi.org/10.1681/ASN.2017010084 Autosomal dominant polycystic kidney disease (ADPKD) is the most common inherited kidney disease. 1,2 It is characterized by progressive enlarge- ment of the kidneys with multiple bilateral cysts and eventual loss of kidney function, often causing end-stage renal disease (ESRD) in middle age. 1,3 Ten percent of patients on renal replacement ther- apy (RRT) in the United Kingdom and 5% in the United States have a primary renal diagnosis of ADPKD. 4,5 ADPKD is a multisystem disorder, with polycystic liver being a common extrarenal manifestation. 6–8 The prevalence of liver cysts in people with ADPKD increases with age, with .90% of patients aged .40 years old having at least one cyst. 9 Unlike renal cysts (which are unaffected by sex), liver cysts are more common and numer- ous in premenopausal women with ADPKD than men. 7,9,10 ADPKD is also associated with other Received January 25, 2017. Accepted March 24, 2017. P.K.J., C.H.S.H., C.G.W., and W.G.H. contributed equally to this work. Published online ahead of print. Publication date available at www.jasn.org. Correspondence: Dr. William G. Herrington, Clinical Trial Ser- vice Unit and Epidemiological Studies Unit, Richard Doll Build- ing, Roosevelt Drive, Old Road Campus, Oxford, OX3 7LF, United Kingdom. Email: [email protected] Copyright © 2017 by the American Society of Nephrology 2738 ISSN : 1046-6673/2809-2738 J Am Soc Nephrol 28: 2738–2748, 2017
Transcript of Biliary Tract and Liver Complications in Polycystic Kidney...
CLINICAL EPIDEMIOLOGY www.jasn.org
Biliary Tract and Liver Complications in PolycysticKidney Disease
Parminder K. Judge,*†‡ Charlie H.S. Harper,*† Benjamin C. Storey,*†‡ Richard Haynes,*†‡
Martin J. Wilcock,‡ Natalie Staplin,† Raph Goldacre,§ Colin Baigent,*† Jane Collier,|
Michael Goldacre,§ Martin J. Landray,*†§ Christopher G. Winearls,‡ andWilliam G. Herrington†‡
*Medical Research Council–Population Health Research Unit, †Clinical Trial Service Unit and Epidemiological StudiesUnit, and §Big Data Institute, Nuffield Department of Population Health, University of Oxford, Oxford, UnitedKingdom; and ‡Oxford Kidney Unit and |Department of Gastroenterology, Oxford University Hospitals NationalHealth Service Foundation Trust, Oxford, United Kingdom
ABSTRACTPolycystic liver disease is a well described manifestation of autosomal dominant polycystic kidney disease(ADPKD). Biliary tract complications are less well recognized. We report a 50-year single-center experience of1007patients, which raised ahypothesis thatADPKD is associatedwith biliary tract disease.We tested this hypoth-esis using all England Hospital Episode Statistics data (1998–2012), within which we identified 23,454 people withADPKD and 6,412,754 hospital controls. Hospitalization rates for biliary tract disease, serious liver complications,and a range of other knownADPKDmanifestationswere adjusted for potential confounders. Comparedwith non-ADPKD hospital controls, those with ADPKD had higher rates of admission for biliary tract disease (rate ratio [RR],2.24; 95% confidence interval [95%CI], 2.16 to 2.33) and serious liver complications (RR, 4.67; 95%CI, 4.35 to 5.02).In analyses restricted to thoseonmaintenancedialysis orwith a kidney transplant, RRs attenuated substantially, butADPKD remained associatedwith biliary tract disease (RR, 1.19; 95%CI, 1.08 to 1.31) andperhapswith serious livercomplications (RR, 1.15; 95% CI, 0.98 to 1.33). The ADPKD versus non-ADPKD RRs for biliary tract disease werelarger for men than women (heterogeneity P,0.001), but RRs for serious liver complications appeared higher inwomen (heterogeneity P,0.001). Absolute excess risk of biliary tract disease associated with ADPKD was largerthan that for serious liver disease, cerebral aneurysms, and inguinal hernias but less than that for urinary tractinfections. Overall, biliary tract disease seems to be a distinct and important extrarenal complication of ADPKD.
J Am Soc Nephrol 28: 2738–2748, 2017. doi: https://doi.org/10.1681/ASN.2017010084
Autosomal dominant polycystic kidney disease(ADPKD) is the most common inherited kidneydisease.1,2 It is characterized by progressive enlarge-ment of the kidneys with multiple bilateral cystsand eventual loss of kidney function, often causingend-stage renal disease (ESRD) in middle age.1,3
Ten percent of patients on renal replacement ther-apy (RRT) in the United Kingdom and 5% in theUnited States have a primary renal diagnosis ofADPKD.4,5 ADPKD is a multisystem disorder,with polycystic liver being a common extrarenalmanifestation.6–8 The prevalence of liver cysts inpeople with ADPKD increases with age, with.90% of patients aged.40 years old having at leastone cyst.9 Unlike renal cysts (which are unaffected
by sex), liver cysts are more common and numer-ous in premenopausal women with ADPKD thanmen.7,9,10 ADPKD is also associated with other
Received January 25, 2017. Accepted March 24, 2017.
P.K.J., C.H.S.H., C.G.W., and W.G.H. contributed equally to thiswork.
Published online ahead of print. Publication date available atwww.jasn.org.
Correspondence: Dr. William G. Herrington, Clinical Trial Ser-vice Unit and Epidemiological Studies Unit, Richard Doll Build-ing, Roosevelt Drive, Old Road Campus, Oxford, OX3 7LF,United Kingdom. Email: [email protected]
Copyright © 2017 by the American Society of Nephrology
2738 ISSN : 1046-6673/2809-2738 J Am Soc Nephrol 28: 2738–2748, 2017

abdominal manifestations, including colonic diverticular dis-ease, abdominal wall hernias, and pancreatic cysts.8,10,11 Mildcommon bile duct dilation has also been reported,12 but un-like the much rarer autosomal recessive form of polycystickidney disease, which is associated with nonobstructive intra-hepatic duct dilation (Caroli disease) and recurrent cholangitis,13
clinically significant biliary tract complications are less wellrecognized in ADPKD.
We made an observation at our tertiary center that, in ad-dition to the infective and compressive complications causedby polycystic livers, several patients with ADPKD had repeatedhospitalizations for biliary tract disease. A systematic literaturereview of PubMed from its inception through July 22, 2016identified a total of 662 potentially relevant abstracts, fromwhich 44 full text articles were read and ten relevant reportswere identified (Supplemental Figure 1).12,14–22 These in-cluded six articles reporting obstructive jaundice due to en-larged cysts,17–22 and four reporting six cases of symptomaticcholecystitis, usually with gallstones.12,14–16 We found no re-ports that described the range of presentations of biliary tractdisease in individuals with ADPKD, and we did not find anythat had quantified any excess risk of clinically significant bil-iary tract disease in ADPKD. To explore whether our clinicalobservations reflect a previously undescribed feature ofADPKD, we aimed to report a single tertiary center’s approx-imately 50-year experience of biliary tract disease and seriousliver complications in patients with ADPKD. We then testedthe hypothesis that biliary tract disease is more common inADPKD by using routinely collected English hospital inpa-tient data from 1998 to 2012 to compare hospitalization ratesfor biliary tract disease among people with ADPKD with ratesin non-ADPKD control populations.
RESULTS
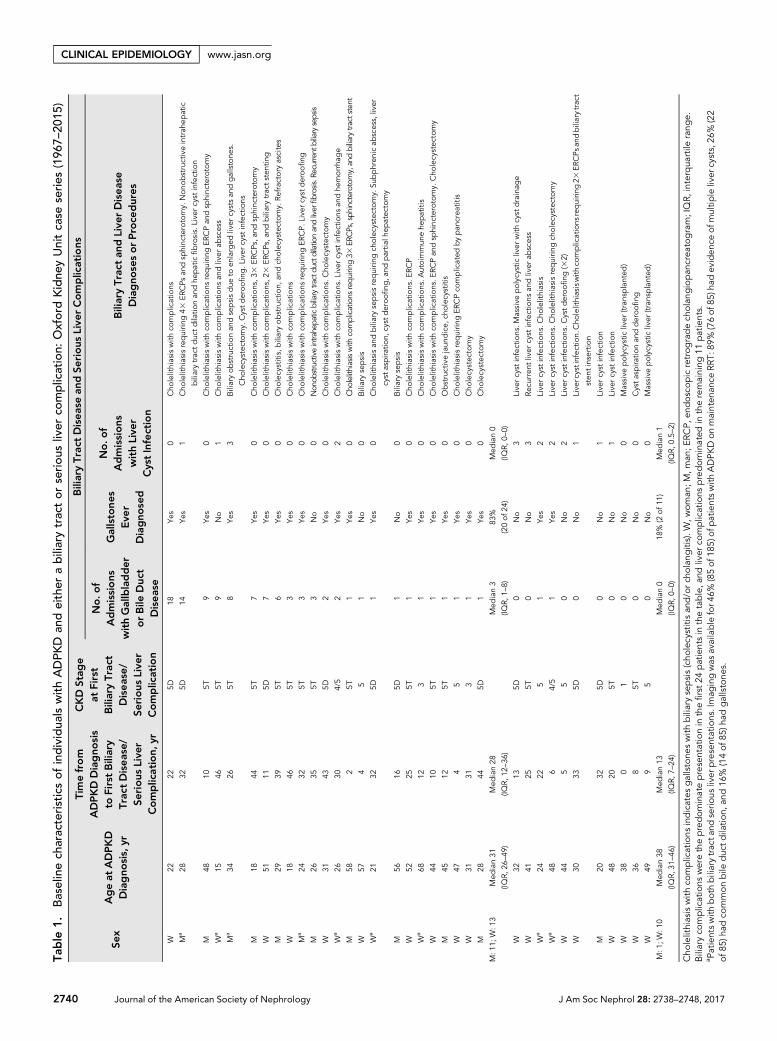
Oxford Kidney Unit Case Series 1967–2015Between 1967 and 2015, 1011 patients with polycystic kidneydisease were cared for at the Oxford Kidney Unit, includingfour patients (0.4%) with autosomal recessive polycystic kid-ney disease. Of the 1007 with presumed ADPKD, 35 patientswere identified as having developed biliary tract disease and/or a liver complication (Table 1). We noted that biliary tractdisease was mostly cholecystitis or other gallstone-relatedcomplications and that this was the prominent presentationin 24 patients. Serious liver complications were the prominentpresentation in 11 patients, mostly representing liver cyst in-fections (Table 1). Nine patients developed both biliary tractdisease and a serious liver complication.
The median ages at presentation with biliary tract diseaseand liver complications were 31 (interquartile range, 26–49)years old and 38 (interquartile range, 31–46) years old, respec-tively (Table 1). These complications tended to manifest inpeople with stage 5 chronic kidney disease (CKD), many ofwhom had started maintenance RRT by the time of their first
such presentation. Similar proportions of women and menwere affected by biliary tract disease (13 of 522 women versus11 of 485 men; P=0.82), but women seemed more likely todevelop a serious liver complication (ten of 522 women versusone of 485 men; P=0.01).
Biliary tract infections accounted for 74% (90 of 121) ofbiliary tract presentations and often recurred (there were 90occurrences among the 21 patients with a biliary tract infec-tion). Escherichia coli and Enterococcus species were the mostcommon causes of biliary tract infection. Liver cyst infectionsoccurred in 67% (12 of 18) of those with a serious liver com-plication, accounting for 38% (22 of 58) of all admissions forserious liver complications. Unlike biliary tract infections, themajority of liver infections were culture negative (Supplemen-tal Figure 2). Management of liver cyst infections was usuallywith antibiotic therapy alone, whereas management of biliarytract disease frequently involved both antibiotics and a rangeof radiologic and surgical interventions (Supplemental Table1). Forty-two percent (11 of 26) of patients with biliary tractdisease had gallstones removed at endoscopic retrogradecholangiopancreatography, five patients required sphincterot-omies, and three had biliary stents inserted (SupplementalTable 1).
Disease Association Study Using All England HospitalEpisode Statistics 1998–2012Wedesigned a disease association study using all EnglandHos-pital Episode Statistics (HES) to test the subsequent hypothesisthat biliary tract disease might be more common in ADPKDthanwould be expected comparedwith the general population.
Using data on 43.2 million people aged over 20 years oldwith at least one hospital admission recorded in linked andanonymized all EnglandHES between 1998 and 2012,we iden-tified 23,454 people admitted with a diagnostic code forADPKD who were unlikely to have autosomal recessive poly-cystic kidney disease (Concise Methods). Median age at thestart of follow-upwas 58 years old (44–70), 10,789 (46%)werewomen, and 20,011 (85%) were white (Table 2). A history ofprior diabetes or vascular disease was recorded in 906 (4%)and 1747 (7%), respectively. In comparison, 6,412,754 hospi-tal controls were identified from an admission for one of avariety of minor conditions (with no mention of polycystickidney disease in any admission). Hospital controls were, onaverage, younger (median age =48 [34–67] years old) and lesslikely to have diabetes (189,858; 3%) or vascular disease(181,832; 3%) (Table 2).
After adjustment for age, sex, ethnicity, social deprivation,region, priordiabetes, prior vascular disease or cancer, and yearof first admission, the rates of admission for a series of diseaseoutcomes were compared among people with ADPKD versuswithout ADPKD (referred to as ADPKD versus non-ADPKDrate ratios [RRs]). Compared with hospital controls, adjustedrates of ESRD were 112 times higher in people with ADPKD(2.82% versus 0.03% per year; RR, 112; 95% confidenceinterval [95%CI], 109 to 116) (Figure 1A). Figure 1A provides
J Am Soc Nephrol 28: 2738–2748, 2017 ADPKD and Biliary/Liver Disease 2739
www.jasn.org CLINICAL EPIDEMIOLOGY
Table
1.Baselinech
aracteristicsof
individua
lswithADPK
Dan
deither
abiliarytractor
seriou
sliver
complication:
OxfordKidne
yUnitcase
series
(196
7–20
15)
Sex
Ageat
ADPKD
Diagno
sis,
yr
Timefrom
ADPKDDiagno
sis
toFirstBiliary
Trac
tDisease/
Serious
Live
rComplication,y
r
CKD
Stag
eat
First
BiliaryTrac
tDisease/
Serious
Live
rComplication
BiliaryTrac
tDiseasean
dSe
rious
Live
rComplications
No.o
fAdmissions
withGallbladder
orBile
Duc
tDisease
Gallstones
Eve
rDiagno
sed
No.o
fAdmissions
withLive
rCystInfection
BiliaryTrac
tan
dLive
rDisease
Diagno
sesorProce
dures
W22
225D
18Ye
s0
Cho
lelithiasiswith
complications
Ma
2832
5D14
Yes
1Cho
lelithiasisrequirin
g43
ERCPs
andsp
hinc
terotomy.
Non
obstructiveintrah
epatic
biliarytrac
tduc
tdilatio
nan
dhe
paticfibrosis.Live
rcyst
infection
M48
105T
9Ye
s0
Cho
lelithiasiswith
complications
requirin
gER
CPan
dsp
hinc
terotomy
Wa
1546
5T9
No
1Cho
lelithiasiswith
complications
andliver
abscess
Ma
3426
5T8
Yes
3Biliaryob
structionan
dsepsisdue
toen
larged
liver
cystsan
dgallstone
s.
Cho
lecystec
tomy.
Cystderoo
fing
.Liver
cyst
infections
M18
445T
7Ye
s0
Cho
lelithiasiswith
complications,3
3ER
CPs
,and
sphinc
terotomy
W51
115D
7Ye
s0
Cho
lelithiasiswith
complications,2
3ER
CPs
,and
biliarytrac
tstenting
M29
395T
6Ye
s0
Cho
lecystitis,biliaryob
struction,
andch
olec
ystectom
y.Re
fractory
ascites
W18
465T
3Ye
s0
Cho
lelithiasiswith
complications
Ma
2432
5T3
Yes
0Cho
lelithiasiswith
complications
requirin
gER
CP.
Live
rcystd
eroo
fing
M26
355T
3No
0Non
obstructiveintrahepa
ticbiliarytractdu
ctdilationandliver
fibrosis.
Recurre
ntbiliarysepsis
W31
435D
2Ye
s0
Cho
lelithiasiswith
complications.C
holecystec
tomy
Wa
2630
4/5
2Ye
s2
Cho
lelithiasiswith
complications.L
iver
cyst
infections
andhe
morrha
ge
M58
25T
1Ye
s0
Cho
lelithiasiswith
complications
requ
iring
33ER
CPs,sph
incterotom
y,andbiliarytra
ctsten
t
W57
45
1No
0Biliarysepsis
Wa
2132
5D1
Yes
0Cho
lelithiasisan
dbiliarysepsisrequirin
gch
olec
ystectom
y.Su
bphren
icab
scess,liver
cyst
aspira
tion,
cyst
deroo
fing
,and
partia
lhep
atec
tomy
M56
165D
1No
0Biliarysepsis
W52
255T
1Ye
s0
Cho
lelithiasiswith
complications.E
RCP
Wa
6812
31
Yes
0Cho
lelithiasiswith
complications.A
utoimmun
ehe
patitis
W44
105T
1Ye
s0
Cho
lelithiasiswith
complications.E
RCPan
dsp
hinc
terotomy.
Cho
lecystec
tomy
M45
125T
1Ye
s0
Obstructivejaun
dice,
cholec
ystitis
W47
45
1Ye
s0
Cho
lelithiasisrequirin
gER
CPco
mplicated
bypan
crea
titis
W31
313
1Ye
s0
Cho
lecystec
tomy
M28
445D
1Ye
s0
Cho
lecystec
tomy
M:1
1;W:1
3Med
ian31
(IQR,
26–49
)
Med
ian28
(IQR,
12–36
)
Med
ian3
(IQR,
1–8)
83%
(20of
24)
Med
ian0
(IQR,
0–0)
W32
135D
0No
3Live
rcyst
infections.M
assive
polycystic
liver
with
cyst
drainag
e
W41
255T
0No
3Re
curren
tliver
cyst
infections
andliver
abscess
Wa
2422
51
Yes
2Live
rcyst
infections.C
holelithiasis
Wa
486
4/5
1Ye
s2
Live
rcyst
infections.C
holelithiasisrequirin
gch
olec
ystectom
y
W44
55
0No
2Live
rcyst
infections.C
ystderoo
fing
(32)
W30
335D
0No
1Live
rcystinfec
tion.Cho
lelithiasiswith
complications
requirin
g23
ERCPs
andbiliarytract
sten
tinsertio
n
M20
325D
0No
1Live
rcyst
infection
W48
205T
0No
1Live
rcyst
infection
W38
01
0No
0Massive
polycystic
liver
(tran
splanted
)
W36
85T
0No
0Cystaspira
tionan
dderoo
fing
W49
95
0No
0Massive
polycystic
liver
(tran
splanted
)
M:1
;W:1
0Med
ian38
(IQR,
31–46
)
Med
ian13
(IQR,
7–24
)
Med
ian0
(IQR,
0–0)
18%
(2of
11)
Med
ian1
(IQR,
0.5–
2)
Cho
lelithiasiswith
complications
indicates
gallstone
swith
biliarysepsis(cho
lecystitisan
d/orc
holang
itis).W
,wom
an;M
,man
;ERC
P,en
dosco
pic
retrog
radech
olan
giopan
crea
togram;IQR,
interqua
rtile
rang
e.Biliaryco
mplications
werethepredom
inatepresentationin
thefirst24
patientsin
thetable,a
ndliver
complications
predom
inated
intheremaining
11patients.
a Patientswith
bothbiliarytrac
tand
serio
usliver
presentations.Imag
ingwas
available
for4
6%(85of
185)
ofpatientswith
ADPKDon
mainten
ance
RRT:
89%
(76of
85)h
adev
iden
ceof
multip
leliver
cysts,26
%(22
of85
)had
commonbile
duc
tdila
tion,
and16
%(14of
85)h
adgallstone
s.
2740 Journal of the American Society of Nephrology J Am Soc Nephrol 28: 2738–2748, 2017
CLINICAL EPIDEMIOLOGY www.jasn.org
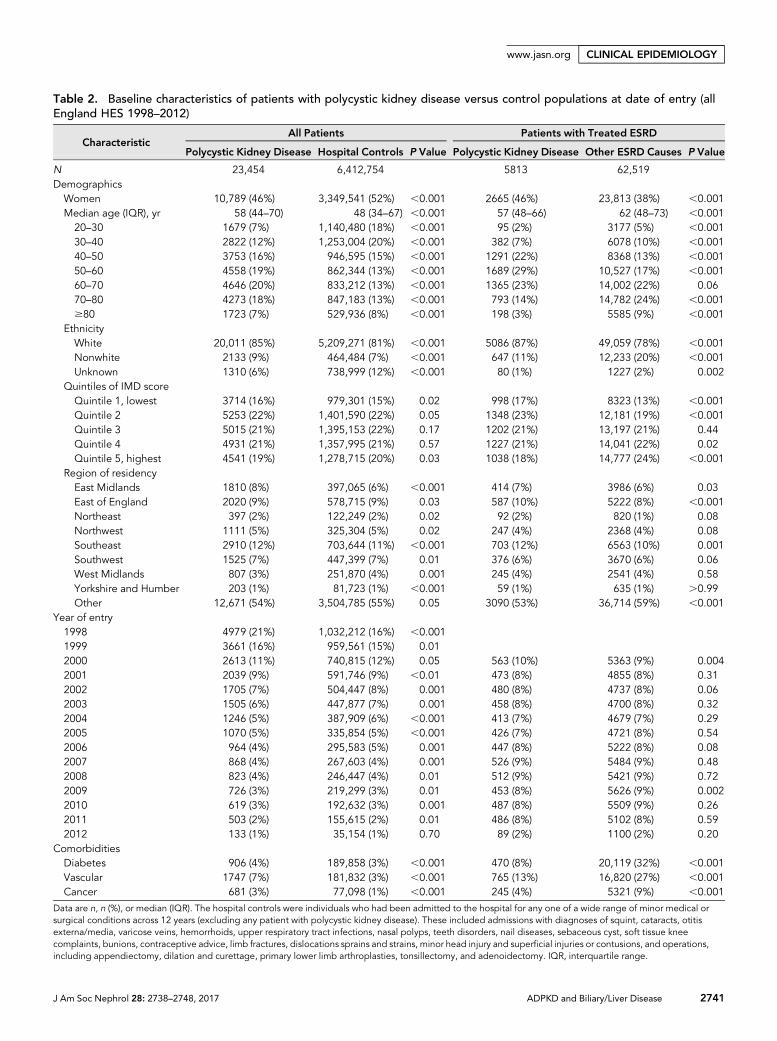
Table 2. Baseline characteristics of patients with polycystic kidney disease versus control populations at date of entry (allEngland HES 1998–2012)
CharacteristicAll Patients Patients with Treated ESRD
Polycystic Kidney Disease Hospital Controls P Value Polycystic Kidney Disease Other ESRD Causes P Value
N 23,454 6,412,754 5813 62,519DemographicsWomen 10,789 (46%) 3,349,541 (52%) ,0.001 2665 (46%) 23,813 (38%) ,0.001Median age (IQR), yr 58 (44–70) 48 (34–67) ,0.001 57 (48–66) 62 (48–73) ,0.00120–30 1679 (7%) 1,140,480 (18%) ,0.001 95 (2%) 3177 (5%) ,0.00130–40 2822 (12%) 1,253,004 (20%) ,0.001 382 (7%) 6078 (10%) ,0.00140–50 3753 (16%) 946,595 (15%) ,0.001 1291 (22%) 8368 (13%) ,0.00150–60 4558 (19%) 862,344 (13%) ,0.001 1689 (29%) 10,527 (17%) ,0.00160–70 4646 (20%) 833,212 (13%) ,0.001 1365 (23%) 14,002 (22%) 0.0670–80 4273 (18%) 847,183 (13%) ,0.001 793 (14%) 14,782 (24%) ,0.001$80 1723 (7%) 529,936 (8%) ,0.001 198 (3%) 5585 (9%) ,0.001
EthnicityWhite 20,011 (85%) 5,209,271 (81%) ,0.001 5086 (87%) 49,059 (78%) ,0.001Nonwhite 2133 (9%) 464,484 (7%) ,0.001 647 (11%) 12,233 (20%) ,0.001Unknown 1310 (6%) 738,999 (12%) ,0.001 80 (1%) 1227 (2%) 0.002
Quintiles of IMD scoreQuintile 1, lowest 3714 (16%) 979,301 (15%) 0.02 998 (17%) 8323 (13%) ,0.001Quintile 2 5253 (22%) 1,401,590 (22%) 0.05 1348 (23%) 12,181 (19%) ,0.001Quintile 3 5015 (21%) 1,395,153 (22%) 0.17 1202 (21%) 13,197 (21%) 0.44Quintile 4 4931 (21%) 1,357,995 (21%) 0.57 1227 (21%) 14,041 (22%) 0.02Quintile 5, highest 4541 (19%) 1,278,715 (20%) 0.03 1038 (18%) 14,777 (24%) ,0.001
Region of residencyEast Midlands 1810 (8%) 397,065 (6%) ,0.001 414 (7%) 3986 (6%) 0.03East of England 2020 (9%) 578,715 (9%) 0.03 587 (10%) 5222 (8%) ,0.001Northeast 397 (2%) 122,249 (2%) 0.02 92 (2%) 820 (1%) 0.08Northwest 1111 (5%) 325,304 (5%) 0.02 247 (4%) 2368 (4%) 0.08Southeast 2910 (12%) 703,644 (11%) ,0.001 703 (12%) 6563 (10%) 0.001Southwest 1525 (7%) 447,399 (7%) 0.01 376 (6%) 3670 (6%) 0.06West Midlands 807 (3%) 251,870 (4%) 0.001 245 (4%) 2541 (4%) 0.58Yorkshire and Humber 203 (1%) 81,723 (1%) ,0.001 59 (1%) 635 (1%) .0.99Other 12,671 (54%) 3,504,785 (55%) 0.05 3090 (53%) 36,714 (59%) ,0.001
Year of entry1998 4979 (21%) 1,032,212 (16%) ,0.0011999 3661 (16%) 959,561 (15%) 0.012000 2613 (11%) 740,815 (12%) 0.05 563 (10%) 5363 (9%) 0.0042001 2039 (9%) 591,746 (9%) ,0.01 473 (8%) 4855 (8%) 0.312002 1705 (7%) 504,447 (8%) 0.001 480 (8%) 4737 (8%) 0.062003 1505 (6%) 447,877 (7%) 0.001 458 (8%) 4700 (8%) 0.322004 1246 (5%) 387,909 (6%) ,0.001 413 (7%) 4679 (7%) 0.292005 1070 (5%) 335,854 (5%) ,0.001 426 (7%) 4721 (8%) 0.542006 964 (4%) 295,583 (5%) 0.001 447 (8%) 5222 (8%) 0.082007 868 (4%) 267,603 (4%) 0.001 526 (9%) 5484 (9%) 0.482008 823 (4%) 246,447 (4%) 0.01 512 (9%) 5421 (9%) 0.722009 726 (3%) 219,299 (3%) 0.01 453 (8%) 5626 (9%) 0.0022010 619 (3%) 192,632 (3%) 0.001 487 (8%) 5509 (9%) 0.262011 503 (2%) 155,615 (2%) 0.01 486 (8%) 5102 (8%) 0.592012 133 (1%) 35,154 (1%) 0.70 89 (2%) 1100 (2%) 0.20
ComorbiditiesDiabetes 906 (4%) 189,858 (3%) ,0.001 470 (8%) 20,119 (32%) ,0.001Vascular 1747 (7%) 181,832 (3%) ,0.001 765 (13%) 16,820 (27%) ,0.001Cancer 681 (3%) 77,098 (1%) ,0.001 245 (4%) 5321 (9%) ,0.001
Data are n, n (%), or median (IQR). The hospital controls were individuals who had been admitted to the hospital for any one of a wide range of minor medical orsurgical conditions across 12 years (excluding any patient with polycystic kidney disease). These included admissions with diagnoses of squint, cataracts, otitisexterna/media, varicose veins, hemorrhoids, upper respiratory tract infections, nasal polyps, teeth disorders, nail diseases, sebaceous cyst, soft tissue kneecomplaints, bunions, contraceptive advice, limb fractures, dislocations sprains and strains, minor head injury and superficial injuries or contusions, and operations,including appendiectomy, dilation and curettage, primary lower limb arthroplasties, tonsillectomy, and adenoidectomy. IQR, interquartile range.
J Am Soc Nephrol 28: 2738–2748, 2017 ADPKD and Biliary/Liver Disease 2741
www.jasn.org CLINICAL EPIDEMIOLOGY

adjusted rates and ADPKD versus non-ADPKD RRs for arange of other known manifestations of ADPKD. These in-clude cerebral aneurysms, inguinal and other abdominal wallhernias, urinary tract infections, cardiac valve disease, and di-verticular disease (Supplemental Table 2 provides outcomedefinitions), all of which were positively associated withADPKD.
Compared with hospital controls, the rates of admissionfor biliary tract disease were 2.2 times higher in people withADPKD (1.31% versus 0.59% per year; RR, 2.24; 95% CI,2.16 to 2.33) and 4.7 times higher for serious liver compli-cations (0.31% versus 0.07% per year; RR, 4.67; 95%CI, 4.35to 5.02) (Figure 1A). These equate to an absolute excess riskof biliary tract disease associated with ADPKD of 0.73% peryear (95% CI, 0.68% to 0.78% per year), which was largerthan the absolute excess risk for serious liver disease (0.24%per year; 95% CI, 0.21% to 0.28% per year), cerebral aneu-rysms (0.11% per year; 95% CI, 0.09% to 0.14% per year),inguinal hernias (0.11% per year; 95% CI, 0.08% to 0.14%per year), or abdominal wall hernias (0.35% per year;95% CI, 0.32% to 0.38% per year); similar to the excess riskfor colonic diverticular disease (0.73% per year; 95% CI,0.67% to 0.79% per year); and much less than for urinarytract infections (2.20% per year; 95% CI, 2.10% to 2.31%per year).
On average, hospital controls are likely to have better kidneyfunction than people with ADPKD, which is important toconsider in secondary analyses, because CKD might mediatesome of the positive associations between ADPKD and out-comes. We, therefore, repeated analyses just among the 68,332people who had started maintenance RRT, which effectivelyadjusts for any effect of advanced CKD.
Within the treated ESRD population, 9% (5813 of 68,332)were recorded as having ADPKD. People with ESRD due toADPKD were, on average, younger (57 versus 62 years old),more likely to be women (46% versus 38%), and less likely tohave a history of prior diabetes (8% versus 32%) or vasculardisease (13% versus 27%) than those with ESRD due to othercauses (Table 2).
After restricting analyses to those with treated ESRD,ADPKD versus non-ADPKD RRs for the positive control dis-eases were attenuated (Figure 1B). Nevertheless, comparedwith those with other causes of ESRD, rates of hospitalizationamong people with ADPKDwere 2.2 times higher for cerebralaneurysms (0.13% versus 0.06% per year; RR, 2.23; 95% CI,1.53 to 3.26), 2.5 times higher for other abdominal wall her-nias (1.23% versus 0.50% per year; RR, 2.47; 95% CI, 2.19 to2.80), and about 60%–70% higher for both inguinal hernias(1.00% versus 0.59% per year; RR, 1.70; 95% CI, 1.49 to 1.95),and colonic diverticular disease (2.70% versus 1.64% per year;RR, 1.65; 95% CI, 1.52 to 1.79) (Figure 1B). Rates forserious cardiac valve disease, however, were similar amongpeople with ESRD due to ADPKD and people with othercauses of ESRD (1.47% versus 1.63% per year; RR, 0.90;95% CI, 0.81 to 1.00).
The RRs for biliary tract disease and serious liver com-plications were also substantially attenuated when analyseswere restricted to those with treated ESRD, but ADPKDremained positively associated with biliary tract disease.Compared with those with other causes of ESRD, rates ofbiliary tract disease were 19% higher among people withADPKD (1.92% versus 1.61% per year; RR, 1.19; 95% CI,1.08 to 1.31) and 15% higher for serious liver complications(0.70% versus 0.62% per year; RR, 1.15; 95% CI, 0.98 to1.33) (Figure 1B).
Among people on maintenance RRT, the absolute excessrisk of biliary tract complications (0.31% per year; 95% CI,0.13% to 0.49% per year) in people with ADPKD remainedlarger than for serious liver complications (0.09% per year;95% CI, 20.02% to 0.2% per year) and cerebral aneurysms(0.07% per year; 95% CI, 0.03% to 0.12% per year); becamesimilar to the absolute excess risk for inguinal hernias (0.41%per year; 95% CI, 0.29% to 0.54% per year); and was some-what smaller than for other abdominal wall hernias (0.73%per year; 95% CI, 0.59% to 0.87% per year), colonic divertic-ular disease (1.06% per year; 95% CI, 0.85% to 1.27% peryear), and urinary tract infections (1.36% per year; 95% CI,1.01% to 1.72% per year).
In analyses performed separately for different age groupsand by sex, compared with hospital controls, ADPKD versusnon-ADPKD RRs for serious liver complications were higherin women than in men (heterogeneity P,0.001), confirmingthe observation from our case series. However, the reverse wasobserved for biliary tract disease (heterogeneity P,0.001)(Figure 2A). RRs for serious liver disease were larger amongyounger people with ADPKD (trend P,0.001), but the reversewas also true for biliary tract disease (trend P,0.001) (Figure2A). In analyses restricted to people with treated ESRD,ADPKD versus non-ADPKD RRs for biliary tract disease be-came similar in both sexes (heterogeneity P=0.22), but RRs forserious liver complications remained higher in women than inmen (heterogeneity P,0.001) (Figure 2B). There was no dif-ference in RRs for either complication by age in people withtreated ESRD (Figure 2B).
In sensitivity analyses, results were similar when repeatedwith the exclusion of secondary diagnoses to define diseaseoutcomes (Supplemental Figures 3 and 4) or the exclusionof people with a serious liver complication (which reducesany overascertainment of biliary tract disease identifiedincidentally during any liver investigations; data notshown).
Cause-Specific Mortality among People with ADPKDBiliary tract or liver disease is an uncommon underlying causeof death among people with ADPKD, except among those whowere hospitalized in the cohort for either biliary tract disease orserious liver complications, in whom it accounted for 8% ofdeaths (Supplemental Figure 5). This proportion was similarin women and men (9% versus 6%, respectively; P=0.06)(Supplemental Figure 6).
2742 Journal of the American Society of Nephrology J Am Soc Nephrol 28: 2738–2748, 2017
CLINICAL EPIDEMIOLOGY www.jasn.org
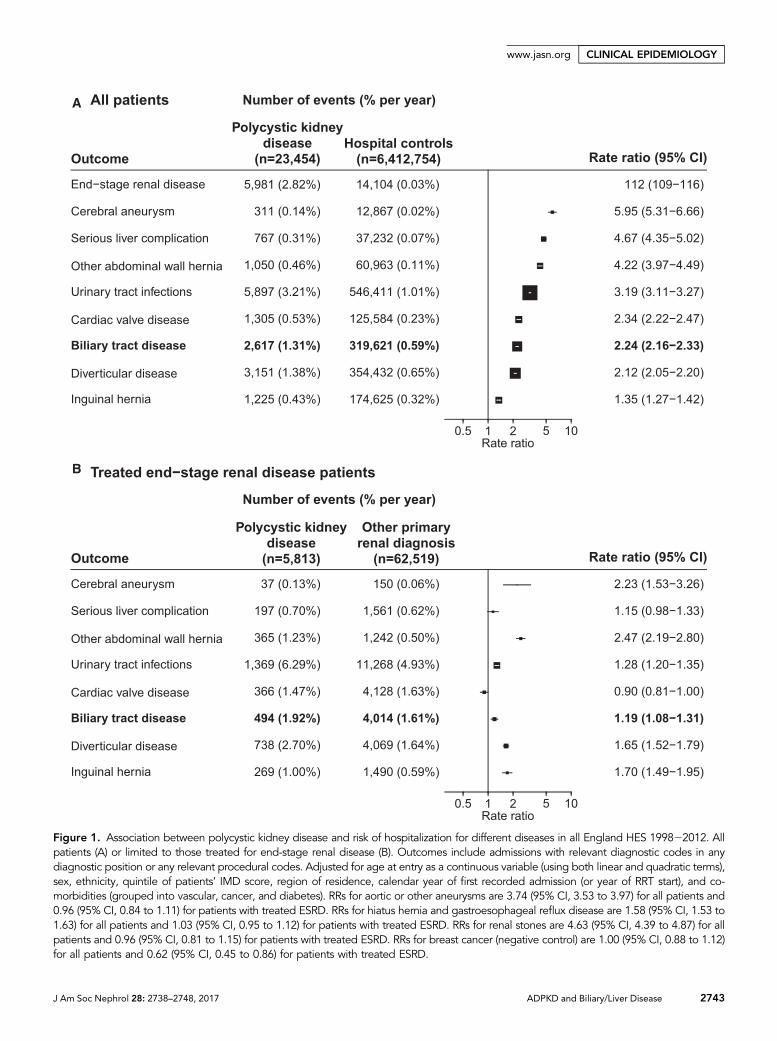
Figure 1. Association between polycystic kidney disease and risk of hospitalization for different diseases in all England HES 199822012. Allpatients (A) or limited to those treated for end-stage renal disease (B). Outcomes include admissions with relevant diagnostic codes in anydiagnostic position or any relevant procedural codes. Adjusted for age at entry as a continuous variable (using both linear and quadratic terms),sex, ethnicity, quintile of patients’ IMD score, region of residence, calendar year of first recorded admission (or year of RRT start), and co-morbidities (grouped into vascular, cancer, and diabetes). RRs for aortic or other aneurysms are 3.74 (95% CI, 3.53 to 3.97) for all patients and0.96 (95% CI, 0.84 to 1.11) for patients with treated ESRD. RRs for hiatus hernia and gastroesophageal reflux disease are 1.58 (95% CI, 1.53 to1.63) for all patients and 1.03 (95% CI, 0.95 to 1.12) for patients with treated ESRD. RRs for renal stones are 4.63 (95% CI, 4.39 to 4.87) for allpatients and 0.96 (95% CI, 0.81 to 1.15) for patients with treated ESRD. RRs for breast cancer (negative control) are 1.00 (95% CI, 0.88 to 1.12)for all patients and 0.62 (95% CI, 0.45 to 0.86) for patients with treated ESRD.
J Am Soc Nephrol 28: 2738–2748, 2017 ADPKD and Biliary/Liver Disease 2743
www.jasn.org CLINICAL EPIDEMIOLOGY
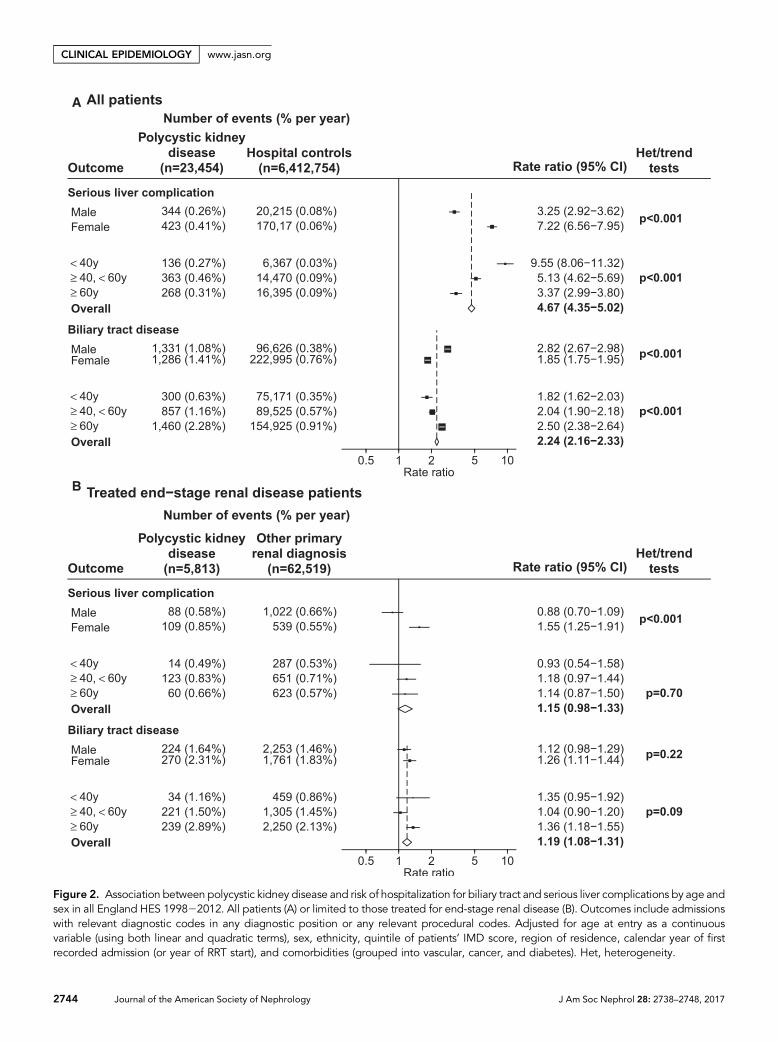
Figure 2. Association between polycystic kidney disease and risk of hospitalization for biliary tract and serious liver complications by age andsex in all England HES 199822012. All patients (A) or limited to those treated for end-stage renal disease (B). Outcomes include admissionswith relevant diagnostic codes in any diagnostic position or any relevant procedural codes. Adjusted for age at entry as a continuousvariable (using both linear and quadratic terms), sex, ethnicity, quintile of patients’ IMD score, region of residence, calendar year of firstrecorded admission (or year of RRT start), and comorbidities (grouped into vascular, cancer, and diabetes). Het, heterogeneity.
2744 Journal of the American Society of Nephrology J Am Soc Nephrol 28: 2738–2748, 2017
CLINICAL EPIDEMIOLOGY www.jasn.org

DISCUSSION
We have reported a case series and a large disease associationstudy including over 23,000 patients with ADPKD. Our caseseries findings suggested that biliary tract disease is as frequentinpeoplewithADPKDas serious liver complications and that ithas a distinct clinical presentation and sex distribution. Ourdisease association study confirmed that hospitalization forbiliary tract disease is more common among people withADPKD than people without and that the absolute excessrisk was larger than for serious liver complications and a rangeof other better described extrarenal manifestations of ADPKD.
The Halt Progression of Polycystic Kidney Disease Study A(HALT-PKD-A) has characterized the biliary tract and liverimaging features of ADPKD.23 Common bile duct dilationwaspresent in 17% of the cohort, but it was the only biliary tractabnormality described. These data corroborate earlier obser-vations from a Japanese study of 55 people with ADPKD,where the prevalence of common bile duct dilation was 40%compared with 7% in controls.12 A higher prevalence of com-mon bile duct dilation in the Japanese study may be accountedfor by more advanced ADPKD, because one half of the Japa-nese patients with ADPKD had started hemodialysis, whereasall HALT-PKD-A participants had an estimated glomerularfiltration rate .60 ml/min per 1.73 m2. In addition to thesestudies, our systematic literature review identified a few casereports of biliary tract complications in ADPKD (Supplemen-tal Figure 1),12,14–16 but no study assessed if there was an excessrisk of clinically significant biliary tract disease associated withADPKD. The presented results, therefore, represent the firstquantification of the association between ADPKD and seriousbiliary tract disease.
Another important finding in both our case series and dis-ease association study is that the relative sizes of the ADPKDversus non-ADPKD RRs for serious liver complications werehigher among women than men, but the reverse was true forbiliary tract disease associations. Other ADPKD studies, in-cluding the HALT-PKD-A, have also found that the prevalenceof liver cysts is higher in women with ADPKD compared withmen.9,23 Estrogen receptors are expressed in the epithelium ofliver cysts,1,8,24,25 and in women, exogenous estrogen use andpregnancy both seem to increase cyst cell proliferation andliver cyst size.1,8,24,25 However, liver enlargement in ADPKDresults from both cystic change and increased liver parenchy-mal volume, and men with ADPKD have been found to haverelatively increased height-adjusted liver parenchymal volumecompared to women.23 The differing patterns of associationsin our subgroup analyses by age and sex suggest that cysticchange in the liver—which has been reported to cause ob-structive jaundice17–22—is not the key cause of biliary tractcomplications in ADPKD. Polycystin complexes localize toprimary cilia in the kidney and biliary tract. In the biliarytract, cilia may act as mechanosensors, maintaining thedifferentiated state of cholangiocyte epithelia and detectingchanges in bile flow and composition.26,27 Mutations in
polycystin-encoding genes in ADPKD may, therefore, affectcholangiocyte cilia, resulting in abnormal bile tract function(with biliary stasis and duct dilation) and/or bile duct glandcyst formation.15,28 A shared biliary phenotype between mu-tations that cause autosomal recessive and ADPKD has alsobeen suggested.29–31
Biliary tract disease has featured in the results of recentrandomized trials of treatments aimed at inhibiting renalcyst cell proliferation and fluid secretion. In a trial of a somato-statin analog, ocreotide, the rate of kidney volume increasewasslowed compared with placebo,32 and post hoc analyses sug-gested that octreotide may also reduce liver parenchyme andcyst expansion.33 However, it also led to increased numbers ofnonserious reports of gallstones (octreotide: ten of 40 [25%]versus placebo: zero of 39 [0%]) and biliary sand (octreotide:seven of 40 [18%] versus placebo: one of 39 [3%]). The tworeported serious cases of acute cholecystitis in this study wereboth among those allocated octreotide.32 These results areconsistent with previous reports of octreotide-associated gall-stones, which are attributed to reduced postprandial gallblad-der contractility and biliary stasis (indicated by increasedfasting gallbladder volumes).34 Octreotide exerts its beneficialeffects on cysts through inhibition of the secondary messengercyclic adenosine monophosphate in biliary epithelial cells.However, inhibiting this pathway with the vasopressin V2-receptor blocker, tolvaptan, significantly reduces the rate of in-crease in total kidney volume compared with placebo withoutany reported excess of upper abdominal pain, gallstones, orbiliary tract adverse events.35
Although not our primary aim, these data represent thelargest confirmatory study of the size of associations betweenADPKD and a range of previously described extrarenal man-ifestations.8,36 Interestingly, we also found that, despite aknown increased prevalence of incompetent mitral and aorticvalves in ADPKD,37 after taking account of renal function,serious cardiac valve disease was no more common in peoplewith ADPKD and ESRD than in those with other causes ofESRD. These findings may influence how nephrologists coun-sel patients with ADPKD. Testing other hypotheses, we alsofound no evidence that ADPKD was associated with increasedrisk of hospitalization with gastroesophageal reflux disease,renal stones, or aortic aneurysms among those with treatedESRD (Figure 1 footnote).
This study uses big data to test bedside observations madeover approximately 50 years, but there are certain limitations.First, predialysis CKD stages are not well recorded in HES, andthere is no informationon laboratory data; therefore, it was notpossible to assess comprehensively how much reduced renalfunction may explain associations with ADPKD. However,HES can be used to identify treated ESRD, and analyses focusedonmaintenance RRTeffectively adjust for advanced CKD, par-tially overcoming this limitation. Secondly, no information onbody mass index—which has been positively associated withcholelithiasis—was available for adjustment. Thirdly, distin-guishing sources of infection in admissions for sepsis is often
J Am Soc Nephrol 28: 2738–2748, 2017 ADPKD and Biliary/Liver Disease 2745
www.jasn.org CLINICAL EPIDEMIOLOGY

difficult, and therefore, rates of infection from particularsources may be underestimates. Lastly, ADPKD definitionswere not directly confirmed. Nevertheless, excellent agree-ment between nurse-recorded primary renal diagnosis andADPKD recorded in HES data has been shown previously,and therefore, any misclassification is unlikely to have led tomuch underestimation in the size of RRs.38,39
In summary, we raised and tested the hypothesis thatADPKD is associated with clinically significant biliary tractdisease as well as serious liver complications. We found thatwomen with ADPKD are at higher relative risk of a liver com-plication than men, but the reverse was observed for the pos-itive association between ADPKD and biliary tract disease,suggesting that liver and biliary complications of ADPKDhave distinct disease mechanisms. The absolute excess risksof biliary tract complications in people with ADPKD are sim-ilar to the absolute excess risks of some of the better establishedcomplications, and therefore, biliary tract disease should be akey differential diagnosis in patients with ADPKD presentingwith abdominal pain or sepsis.
CONCISE METHODS
Oxford Kidney Unit Case Series (1967–2015)All patientswithpresumedADPKDcared for by theOxfordKidneyUnit
between1967andAugust of2015were included.Biliary tract disease and
serious liver complications were ascertained by systematic physician
review of diagnoses, procedures, and investigation reports on the unit’s
electronic patient record system and local radiology, microbiology, and
histopathology systems. After identified, detailed information on each
biliary tract disease or serious liver complication was extracted by med-
ical notes review, which included demographics, age and renal status at
the time of the complication, details of the clinical presentation, includ-
ing microbiologic findings, and clinical management.
Disease Association Study Using All England HospitalEpisode Statistics (1998–2012)Ethical approval for analysis of the record linkage study data was
obtained from the Central and South Bristol Multi-Centre Research
Ethics Committee (04/Q2006/176). We used anonymized linked all
England HES inpatient records with additional linkage to national
mortality records.40 Since 1998, HES have recorded information on
all hospital inpatient activity in England, including dates of admission
and discharge; demographics (including age, sex, and ethnicity);
measures of social deprivation; the primary diagnostic reason for
admission with relevant secondary diagnoses coded using the Inter-
national Statistical Classification of Diseases and Related Health
Problems Revision 10 (ICD-10)41; and all procedures coded using
the Office of Population Censuses and Surveys Classification of Sur-
gical Operations and Procedures (OPCS), version 4.
Identification of Patients with ADPKDA patient with any mention of ICD-10 codes Q61.2 or Q61.3 in HES
was presumed to have a diagnosis of ADPKD. The validity of using
these codes has been directly shownpreviously as part of a clinical trial
among patients with kidney transplants, in which there was an excel-
lent level of agreement (k statistic .0.9) between nurse-reported
primary renal diagnosis of cystic kidney disease and ADPKD coded
in HES.38,39 To reduce the chances of including autosomal recessive
polycystic kidney disease in analyses, people hospitalized or starting
RRT before 20 years of age were excluded.
Identification of Control PopulationsTwo control populations with no mention of ADPKD codes in
any admission were derived from HES. The first was a large
group of patients admitted for minor diagnoses or procedures (a
complete list is in Table 2). The second was any patient who was
treated with maintenance RRT (i.e., long-term dialysis or kidney
transplant) for ESRD and survived for at least 90 days from the start
of RRT.
OutcomesOutcomes for relevant diseases were identified using information
encoded in any diagnostic position (primary or secondary) or any
recorded procedure. These included (1) treated ESRD; (2) a group
of other positive control diseases that have previously been report-
ed to be extrarenal manifestations of ADPKD8,36 (including com-
plications or treatment of cerebral aneurysms, abdominal wall
hernias [separated into inguinal and other], urinary tract infec-
tions, serious cardiac valve disease, and colonic diverticular dis-
ease); (3) a group of liver diagnoses and procedures associated
with ADPKD, including liver abscess and liver deroofing,
resection, and transplantation; (4) biliary tract diagnoses and pro-
cedures, including cholecystitis, biliary tract stones, and cholecys-
tectomy (Supplemental Table 2 has full list of ICD-10 and OPCS
codes used to define outcomes); and (5) a negative control disease
(breast cancer), which has previously been reported as not asso-
ciated with ADPKD.42 In addition, sensitivity analyses were per-
formed excluding diagnostic information recorded as secondary
diagnoses and after excluding people who ever had a serious liver
complication.
CovariatesThe following patient characteristics were extracted from HES: age,
sex, ethnicity (white, nonwhite, and unknown), region of residence,
English Index of Multiple Deprivation (IMD) score,43 and comor-
bidity (diabetes, vascular, or cancer considered separately). For hos-
pital control analyses, comorbidity was derived from diagnoses and
procedures recorded on the first admission. For the ESRD cohort,
comorbidity was derived from the date of the start of RRT and any
admission in the preceding 2 years.
Statistical MethodsBaseline characteristics for each derived cohort were expressed as
numbers (percentages) or medians (interquartile ranges) and com-
pared with standard chi-squared or Kruskal–Wallis tests, respectively.
The follow-up time for each outcome began from the index date
(defined as the date of the first admission) and ended at the earliest
of date of a relevant outcome, death, or end of the cohort follow-up
2746 Journal of the American Society of Nephrology J Am Soc Nephrol 28: 2738–2748, 2017
CLINICAL EPIDEMIOLOGY www.jasn.org

(March 31, 2012). Rates for each outcome were then calculated using
Poisson regression adjusted for age as a continuous variable (using
both linear and quadratic terms), sex, ethnicity (three groups as
above), quintiles of IMD score, region of residence (nine groups),
prior reported diabetes, vascular disease (excluding subarachnoid
hemorrhage), or cancer (excluding breast cancer). Changes in coding
practice over timewere controlled for by adjustment for calendar year
of first admission (or where relevant, year of start of maintenance
RRT).
Primary analyses compared patients with ADPKD with gen-
eral hospital controls to quantify the full effect of ADPKD on
risk of outcomes. Secondarily, we assessed how much advanced
CKD may affect ADPKD versus non-ADPKD RRs by repeating
analyses only among those who had already started RRT for
ESRD (with the index date increased to the date of start of main-
tenance RRT).
RRs and their 95% CIs were calculated using standard statistical
methods. Separate ADPKD versus non-ADPKD RRs for men and
women and by age groups were calculated and compared using stan-
dard tests forheterogeneity and trend, respectively.Analyses usedSAS,
version 9.3 (SAS Institute, Cary, NY) and R version 3.2.1 (www.
r-project.org).
ACKNOWLEDGMENTS
We acknowledge the large number of coders and technicians who
have created and curated Hospital Episode Statistics. This study was
supported by core-funding to the Medical Research Council-
PopulationHealthResearchUnit and theClinicalTrial ServiceUnit and
Epidemiological Studies Unit (CTSU), University of Oxford.
DISCLOSURESThe Medical Research Council–Population Health Research Unit receives
core funding from the United KingdomMedical Research Council. The CTSU
receives funding from the British Heart Foundation and Cancer Research
United Kingdom. The CTSU has a staff policy of not accepting honoraria or
other payments from the pharmaceutical industry, expect for the reimburse-
ment of costs to participate in scientific meetings (www.ctsu.ox.ac.uk).
REFERENCES
1. Torres VE, Harris PC, Pirson Y: Autosomal dominant polycystic kidneydisease. Lancet 369: 1287–1301, 2007
2. Willey CJ, Blais JD, Hall AK, Krasa HB, Makin AJ, Czerwiec FS: Preva-lence of autosomal dominant polycystic kidney disease in the EuropeanUnion [published online ahead of print June 19, 2016]. Nephrol Dial
Transplant doi:10.1093/ndt/gfw2403. Shaw C, Simms RJ, Pitcher D, Sandford R: Epidemiology of patients in
England andWales with autosomal dominant polycystic kidney diseaseand end-stage renal failure. Nephrol Dial Transplant 29: 1910–1918,2014
4. Gilg J, Caskey F, Fogarty D: UK Renal Registry 18th annual report:Chapter 1 UK renal replacement therapy incidence in 2014: Nationaland centre-specific analyses. Nephron 132[Suppl 1]: 9–40, 2016
5. Saran R, Li Y, Robinson B, Abbott KC, Agodoa LY, Ayanian J, Bragg-Gresham J, Balkrishnan R, Chen JL, Cope E, Eggers PW, Gillen D,Gipson D, Hailpern SM, Hall YN, He K, Herman W, Heung M, Hirth RA,Hutton D, Jacobsen SJ, Kalantar-Zadeh K, Kovesdy CP, Lu Y, MolnarMZ,Morgenstern H, Nallamothu B, NguyenDV,O’Hare AM, Plattner B,Pisoni R, Port FK, Rao P, Rhee CM, Sakhuja A, Schaubel DE, SelewskiDT, Shahinian V, Sim JJ, Song P, Streja E, Kurella Tamura M, Tentori F,White S,Woodside K, Hirth RA: US Renal Data System2016 annual datareport: Epidemiology of kidney disease in the United States. Am J
Kidney Dis 69: A7–A8, 20176. Milutinovic J, Fialkow PJ, Rudd TG, Agodoa LY, Phillips LA, Bryant JI:
Liver cysts in patients with autosomal dominant polycystic kidney dis-ease. Am J Med 68: 741–744, 1980
7. Chauveau D, Fakhouri F, Grünfeld JP: Liver involvement in autosomal-dominant polycystic kidney disease: Therapeutic dilemma. J Am Soc
Nephrol 11: 1767–1775, 20008. Pirson Y: Extrarenal manifestations of autosomal dominant polycystic
kidney disease. Adv Chronic Kidney Dis 17: 173–180, 20109. Bae KT, Zhu F, Chapman AB, Torres VE, Grantham JJ, Guay-Woodford
LM, Baumgarten DA, King BF Jr., Wetzel LH, Kenney PJ, Brummer ME,Bennett WM, Klahr S, Meyers CM, Zhang X, Thompson PA, Miller JP;Consortium for Radiologic Imaging Studies of Polycystic Kidney Dis-ease (CRISP): Magnetic resonance imaging evaluation of hepatic cystsin early autosomal-dominant polycystic kidney disease: The Consor-tium for Radiologic Imaging Studies of Polycystic Kidney Disease co-hort. Clin J Am Soc Nephrol 1: 64–69, 2006
10. Torres VE, Harris PC: Autosomal dominant polycystic kidney disease:The last 3 years. Kidney Int 76: 149–168, 2009
11. Mikolajczyk AE, TeHS, ChapmanAB:Gastrointestinal manifestations ofautosomal-dominant polycystic kidney disease. Clin Gastroenterol
Hepatol 15: 17–24, 201712. Ishikawa I, Chikamoto E, Nakamura M, Asaka M, Tomosugi N, Yuri T:
High incidence of common bile duct dilatation in autosomal dominantpolycystic kidney disease patients. Am J Kidney Dis 27: 321–326, 1996
13. Adeva M, El-Youssef M, Rossetti S, Kamath PS, Kubly V, Consugar MB,Milliner DM, King BF, Torres VE, Harris PC: Clinical and molecular char-acterization defines a broadened spectrum of autosomal recessive poly-cystic kidney disease (ARPKD). Medicine (Baltimore) 85: 1–21, 2006
14. Andreoni KA, Pelletier RP, Elkhammas EA, Davies EA, Bumgardner GL,Henry ML, Ferguson RM: Increased incidence of gastrointestinal sur-gical complications in renal transplant recipients with polycystic kidneydisease. Transplantation 67: 262–266, 1999
15. Kolodziejski TR, Safadi BY, Nakanuma Y, Milkes DE, Soetikno RM: Bileduct cysts in a patient with autosomal dominant polycystic kidney dis-ease. Gastrointest Endosc 59: 140–142, 2004
16. Dofferhoff AS, Sluiter HE, Geerlings W, de Jong PE: Complications ofliver cysts in patients with adult polycystic kidney disease.Nephrol Dial
Transplant 5: 882–885, 199017. Garber S, Mathieson J, Cooperberg PL: Percutaneous sclerosis of he-
patic cysts to treat obstructive jaundice in a patient with polycystic liverdisease. Am J Roentgenol 161: 77–78, 1993
18. Hollingsworth AB: The gallbladder in polycystic liver disease. JAMA
247: 462, 198219. Woodring JH, Fried AM, Lieber A: The gallbladder in polycystic liver
disease. JAMA 246: 864–866, 198120. Wittig JH, Burns R, Longmire WP Jr.: Jaundice associated with poly-
cystic liver disease. Am J Surg 136: 383–386, 197821. Howard RJ, Hanson RF, Delaney JP: Jaundice associated with poly-
cystic liver disease. Relief by surgical decompression of the cysts. ArchSurg 111: 816–817, 1976
22. Dmitrewski J, Olliff S, Buckels JA: Obstructive jaundice associated withpolycystic liver disease. HPB Surg 10: 117–120, 1996
23. Hogan MC, Abebe K, Torres VE, Chapman AB, Bae KT, Tao C, Sun H,Perrone RD, Steinman TI, Braun W, Winklhofer FT, Miskulin DC,Rahbari-Oskoui F, Brosnahan G, Masoumi A, Karpov IO, Spillane S,
J Am Soc Nephrol 28: 2738–2748, 2017 ADPKD and Biliary/Liver Disease 2747
www.jasn.org CLINICAL EPIDEMIOLOGY

FlessnerM,Moore CG, Schrier RW: Liver involvement in early autosomal-dominant polycystic kidney disease. Clin Gastroenterol Hepatol 13:155–164.e6, 2015
24. Sherstha R, McKinley C, Russ P, Scherzinger A, Bronner T, Showalter R,Everson GT: Postmenopausal estrogen therapy selectively stimulateshepatic enlargement in women with autosomal dominant polycystickidney disease. Hepatology 26: 1282–1286, 1997
25. Alvaro D, Mancino MG, Onori P, Franchitto A, Alpini G, Francis H,Glaser S, Gaudio E: Estrogens and the pathophysiology of the biliarytree. World J Gastroenterol 12: 3537–3545, 2006
26. Yoder BK: Role of primary cilia in the pathogenesis of polycystic kidneydisease. J Am Soc Nephrol 18: 1381–1388, 2007
27. Harris PC, Torres VE: Polycystic kidney disease.Annu RevMed 60: 321–337, 2009
28. Larusso NF, Masyuk TV: The role of cilia in the regulation of bile flow.Dig Dis 29: 6–12, 2011
29. Strazzabosco M, Fabris L: Development of the bile ducts: Essentials forthe clinical hepatologist. J Hepatol 56: 1159–1170, 2012
30. Hasegawa E, Sawa N, Hoshino J, Suwabe T, Hayami N, Yamanouchi M,Sekine A, Hiramatsu R, Imafuku A, Kawada M, Ubara Y, Imamura T,Takaichi K: Recurrent cholangitis in a patient with Autosomal DominantPolycystic Kidney Disease (ADPKD) and Caroli’s disease. Intern Med55: 3009–3012, 2016
31. Bergmann C: ARPKD and early manifestations of ADPKD: The originalpolycystic kidney disease and phenocopies. Pediatr Nephrol 30: 15–30, 2015
32. Caroli A, Perico N, Perna A, Antiga L, Brambilla P, Pisani A, Visciano B,Imbriaco M, Messa P, Cerutti R, Dugo M, Cancian L, Buongiorno E, DePascalis A, Gaspari F, Carrara F, RubisN, Prandini S, Remuzzi A, RemuzziG, Ruggenenti P; ALADIN study group: Effect of longacting somato-statin analogue on kidney and cyst growth in autosomal dominantpolycystic kidney disease (ALADIN): A randomised, placebo-controlled,multicentre trial. Lancet 382: 1485–1495, 2013
33. Pisani A, SabbatiniM, ImbriacoM, Riccio E, RubisN, Prinster A, PernaA,Liuzzi R, Spinelli L, Santangelo M, Remuzzi G, Ruggenenti P; ALADINStudy Group: Long-term effects of Octreotide on liver volume in pa-tients with polycystic kidney and liver disease. Clin GastroenterolHepatol 14: 1022–1030.e4, 2016
34. Bigg-Wither GW, Ho KK, Grunstein RR, Sullivan CE, Doust BD: Effectsof long term octreotide on gall stone formation and gall bladderfunction. BMJ 304: 1611–1612, 1992
35. Torres VE, Chapman AB, Devuyst O, Gansevoort RT, Grantham JJ,Higashihara E, Perrone RD, Krasa HB, Ouyang J, Czerwiec FS; TEMPO3:4 Trial Investigators: Tolvaptan in patients with autosomal dominantpolycystic kidney disease. N Engl J Med 367: 2407–2418, 2012
36. Chapman AB, Devuyst O, Eckardt KU, Gansevoort RT, Harris T, Horie S,Kasiske BL, Odland D, Pei Y, Perrone RD, Pirson Y, Schrier RW, Torra R,Torres VE, Watnick T, Wheeler DC; Conference Participants: Autosomal-dominant polycystic kidney disease (ADPKD): Executive summaryfrom a kidney disease: Improving Global Outcomes (KDIGO) Contro-versies Conference. Kidney Int 88: 17–27, 2015
37. Hossack KF, Leddy CL, Johnson AM, Schrier RW, Gabow PA: Echo-cardiographic findings in autosomal dominant polycystic kidney dis-ease. N Engl J Med 319: 907–912, 1988
38. 3C Study Collaborative Group; Haynes R, Harden P, Judge P, BlackwellL, Emberson J, Landray MJ, Baigent C, Friend PJ: Alemtuzumab-basedinduction treatment versus basiliximab-based induction treatment inkidney transplantation (the 3C Study): A randomised trial. Lancet 384:1684–1690, 2014
39. The 3C study. Registry Linkage in the 3C Study. Available at: http://www.3cstudy.org/Registrylinkagevalidation_2017_01_12.pdf. AccessedJanuary 16, 2017
40. Ong E, Goldacre R, Hoang U, Sinclair R, Goldacre M: Associationsbetween bullous pemphigoid and primary malignant cancers: AnEnglish national record linkage study, 1999-2011. Arch Dermatol Res306: 75–80, 2014
41. World Health Organization. International Statistical Classification ofDiseases and Related Health Problems version 10 (ICD-10). Availableat: http://apps.who.int/classifications/icd10/browse/2010/en. AccessedJanuary 26, 2016
42. Yu TM, Chuang YW, Yu MC, Chen CH, Yang CK, Huang ST, Lin CL,Shu KH, Kao CH: Risk of cancer in patients with polycystic kidney dis-ease: A propensity-score matched analysis of a nationwide, population-based cohort study. Lancet Oncol 17: 1419–1425, 2016
43. Department of Communities and Local Government, English Indices ofDeprivation. Available at: https://www.gov.uk/government/statistics/english-indices-of-deprivation-2015. Accessed November 9, 2016
This article contains supplemental material online at http://jasn.asnjournals.org/lookup/suppl/doi:10.1681/ASN.2017010084/-/DCSupplemental.
2748 Journal of the American Society of Nephrology J Am Soc Nephrol 28: 2738–2748, 2017
CLINICAL EPIDEMIOLOGY www.jasn.org