Bile duct Reconstruction in Liver Transplant Surgery · Web viewComplications from bile duct...
23
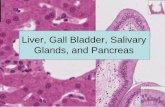
Bile Duct Reconstruction in Liver Transplant Surgery Adeel S Khan MD, Jeffrey Campsen MD, Goran B Klintmalm MD. Introduction Complications from bile duct reconstruction are a major source of morbidity, graft loss and even death in the liver transplant patient. 2-5 The integrity of the anastomosis is highly dependent on surgical technique. However, there are variations in bile duct anatomy and the vascular supply that make this a particularly challenging aspect of liver transplant surgery. Surgeons have therefore developed several techniques of biliary reconstruction. To date, there is still considerable debate on which technique is best suited to a particular anatomic bile duct variant. The purpose of this review is to outline the basic knowledge and controversial topics that influence which type of reconstruction is used during liver transplant surgery. We will review the anatomy of the biliary system and the common techniques of reconstruction. The pros and cons of each technique are reviewed. Bile Duct Anatomy The common hepatic duct (CHD) is formed by the union of the right and left hepatic ducts in most patients. In most adults, the CHD duct is 6-8 cm long and approximately 6 mm in diameter. The hepatic artery lies medial to and the portal vein posterior- medial to the bile duct as it exits the liver. Together these three structures form the portal triad. There are common variations in this anatomical pattern including absence of the right or left hepatic duct. In addition there can also be
Transcript of Bile duct Reconstruction in Liver Transplant Surgery · Web viewComplications from bile duct...
Bile Duct Reconstruction in Liver Transplant Surgery
Adeel S Khan MD, Jeffrey Campsen MD, Goran B Klintmalm MD.
Introduction
Complications from bile duct reconstruction are a major source of morbidity, graft loss and even
death in the liver transplant patient.2-5 The integrity of the anastomosis is highly dependent on
surgical technique. However, there are variations in bile duct anatomy and the vascular supply
that make this a particularly challenging aspect of liver transplant surgery. Surgeons have
therefore developed several techniques of biliary reconstruction. To date, there is still
considerable debate on which technique is best suited to a particular anatomic bile duct variant.
The purpose of this review is to outline the basic knowledge and controversial topics that
influence which type of reconstruction is used during liver transplant surgery. We will review
the anatomy of the biliary system and the common techniques of reconstruction. The pros and
cons of each technique are reviewed.
Bile Duct Anatomy
The common hepatic duct (CHD) is formed by the union of the right and left hepatic ducts in
most patients. In most adults, the CHD duct is 6-8 cm long and approximately 6 mm in
diameter. The hepatic artery lies medial to and the portal vein posterior-medial to the bile duct
as it exits the liver. Together these three structures form the portal triad. There are common
variations in this anatomical pattern including absence of the right or left hepatic duct. In
addition there can also be multiple sectoral or accessory ducts entering the right and/or left
hepatic ducts at different levels as they exit the liver. 1,2
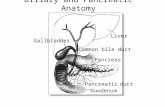
The cystic duct drains the gallbladder and then joins the CHD in a highly variable position to
form the common bile duct (CBD). The duct travels through the head of the pancreas before it
empties into the duodenum (Image 1). The blood supply to the bile ducts comes from vessels
running laterally at 3’o clock and 9’o clock position and is mainly derived from the
gastroduodenal artery (GDA) and right hepatic artery (RHA).1 However, there is considerable
variation in the blood supply and it is not uncommon to find vessels from the cystic and gastric
arteries or the celiac axis that supply the biliary tree. During liver transplant surgery the bile
duct is transected and reconstructed at the level of the CHD. Consequently the blood supply to
the divided donor duct is far more tenuous than the recipient’s.
Type of Anastomosis
Bile duct reconstruction during liver transplantation is usually performed by an end to end
anastomosis (choledocho-choledochostomy [DD]) between the donor and recipient common
bile ducts. The next most common technique is an end to side Roux-en-Y hepaticojejunostomy
(RYHJ).4-7, 12-14 In the latter procedure, the end of the hepatic duct is anastomosed to the side of
the jejunum. Direct insertion of the common bile duct into the duodenum known as
choledocho-duodenostomy (CD) is a third but less common option for biliary reconstruction.9
Duct-to-Duct Anastomosis (DD) (Choledochocholedochostomy): The common bile ducts of the
donor and recipient can be anastomosed as an end-to-end choledocho-choledochostomy. This is
the technique of choice for biliary anastomosis in deceased donor liver transplantation (DDLT).
It is a technically easier and faster procedure than a RYHJ. The DD also avoids intestinal
manipulation, maintains anti-reflux mechanism of sphincter of Oddi and provides easy access for
endoscopic intervention in case of future anastomotic strictures.7,8,10,17 The anastomosis itself
can be performed using interrupted or running mono-filament (absorbable or non absorbable)
suture. It can be technically challenging if the ducts are very small or if there is a large size
discrepancy between donor and recipient bile ducts. The latter issue is particularly important in
pediatric liver transplantation.
The most expeditious way to address the donor and recipient duct size discrepancy is to make a
side-cut on the side of the smaller duct (usually donor side). With very large ducts a
choledochoplasty of the oversized duct can be performed. Neuhaus et al from Germany
described a technique of side-to-side anastomosis between the donor and recipient common
bile ducts (choledocho-choledochostomy) instead of the more common end to end method.
Studies have shown that this is as safe option for performing bile duct anastomosis and has a
low complication rate.14
Roux-en-Y hepaticojejunostomy (RYHJ): In this technique, a loop of small bowel 10-20 cm distal
to the ligament of Treitz is divided and brought up to the donor bile duct. An end to side
anastomosis is then completed between the two (Image 2). The RYHJ is a preferred technique
when the donor bile duct diameter is small (pediatric, split liver and living donor transplants)
and in patients with extrahepatic biliary disease (eg. primary sclerosing cholangitis, Caroli’s
disease and cholangio-carcinoma).
There are unique complications associated with type of biliary reconstruction that are related to
the surgical enteric anastomosis. This approach adds to the operative time because it involves
small bowel resection and anastomosis. In addition, there is an increase the risk of peritonitis
due to enteric leaks and bleeding complications. These complications are exacerbated by the
high venous pressure associated with portal hypertension in some patients. There is also an
increase the risk of developing ascending cholangitis from contamination with gut flora. Further,
subsequent endoscopic intervention to treat bile duct narrowing is difficult if not
impossible.7,8,10,12,17,22
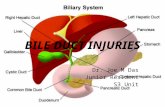
Choledochoduodenostomy (CD): This technique involves direct anastomosis between the end
of the bile duct and the side of the duodenum. The CD has been shown in a several studies to
be a safe alternative to a Roux-en-Y when a duct-to-duct anastomosis cannot be performed.9
Advantages include the ease of postoperative access to the biliary system. However this type of
anastomosis may expose the biliary system to enteric contents raising the risk of ascending
cholangitis. (Image 3)
Role of T-tube/stenting
Insertion of biliary drainage catheters or T-tubes has been a topic of controversy in the
transplant community. The rationale for using T-tubes includes the ease of access to the biliary
system and protecting the anastomosis against narrowing by the insertion of an internal stent.
In addition, the T-tubes allow physicians to monitor the quality of the bile and thus the function
of the liver graft which can provide critical information in cases of primary non-function. It also
allows endoscopic access to bile ducts to diagnose or repair a stenosis or leak. Some
investigators think that T-tubes may protect the anastomosis from developing leaks by lowering
the intra-ductal pressure.7
However initial randomized trials that examined the safety of T-tubes in liver transplant
recipients showed that biliary complications occurred in up to 50% of patients.11-15 These
complications included narrowing of the bile duct lumen, cholangitis, spontaneous dislodgement
of the T-tube, and bile leaks following T-tube removal. These complications seem to be caused
by impaired healing due to immunosuppression. Spasm of sphincter of Oddi is also thought to
occur more frequently in patients with T-tubes. These findings discouraged transplant surgeons
from using T-tubes and a recent meta-analysis confirmed this observation by demonstrating that
most of the larger transplant centers now avoid the use of T-tubes in cadaveric liver
transplants.15
Bile duct reconstruction in living donor liver transplantation
Living donor liver transplantation (LDLT) is an accepted option to increase the donor organ pool 16,17,19,20. The long term outcomes are comparable to deceased donor liver transplants. 23. Both
the right and left hemi-liver are used in adult to adult living donation surgery. In contrast, the
left lateral section (segments 2 and 3) is commonly used when an adult donates to a pediatric
patient.
The biliary reconstruction in LDLT patients tends to be more challenging than in cadaveric liver
transplants because the ducts are smaller and can have multiple or irregular branching
depending on the plane of transection. 17 Roux-en-Y hepaticojejunostomy (RYHJ) was considered
the standard approach for LDLT biliary reconstruction until 1998 when Wachs et al reported the
first case of duct-to-duct reconstruction for right hemi liver transplant. 16 Since then several
studies have reported good outcomes using duct-to-duct biliary anastomosis for LDLT. 17,19,20
A single hepatic duct is favored for a DD anastomosis. If two ducts are present, a DD
anastomosis can still be used if the openings are less than 3 mm apart. In this case, the duct is
modified to create a single orifice. If the distance is greater than 3 mm then two separate
hepaticojejunostomies are performed using a Roux-en-Y loop. 5 In 2005 Asonuma et al.
described using the recipient cystic duct for biliary reconstruction in right liver donor
transplantation when two bile duct orifices were present. 24
The advantages and disadvantages of using the different biliary reconstruction techniques are
similar to those for deceased donor liver transplant as described above however, the outcomes
in LDLT recipients are not as good due to higher rates of biliary complications seen with LDLT
(see complications). The use of biliary drainage catheter or T-tube in LDLT is as controversial as
their use in DDTL. Overall, T-tubes are rarely used in LDLT. 5,12,13,14,17
Complications of bile duct reconstruction
Calne in 1976 described the biliary anastomosis as the “Achilles heel” of liver transplantation3.
This observation still stands true today. Biliary complications after liver transplant occur in 9-
34% of all liver transplant recipients. They are more common in LDLT due to smaller sized and
often multiple ducts. 3,5,8,17,20 The most common complications seen are bile leaks and
anastomotic strictures, Two thirds of these complications present in the first three months. 18
Bile leaks complicate up to 20% of liver transplant surgeries. Early bile leaks (<4 weeks) are
generally considered a technical complication and usually occur at the site of anastomosis. 10
Causes can include loose or widely placed sutures, ischemic necrosis of the bile duct edges often
from small and tightly placed sutures or from hepatic artery stenosis or thrombosis. 5, 10, 17
Because the biliary anastomosis relies on blood flow from the right hepatic artery, a reduction in
blood supply can manifest as a bile leak. Late bile leaks are rare and are usually seen in patients
with T-tubes after their intentional or inadvertent removal. 4,10,14,15 Bile leaks can present with
altered liver function test and/or peritonitis from bilious ascites. If left untreated, this can
progress to sepsis from an infected biloma. 6,18,22
Bile Duct strictures are seen in as many as 27% of liver transplants 7.Similar to bile leaks, early
anastomotic strictures (<4 weeks) are commonly due to a technical problem such as tight
sutures, purse-stringing of anastomosis or “back-walling” of posterior wall. Bile duct ischemia
from hepatic artery stenosis, thrombosis or devascularized duct edges can also predispose to
strictures. However, these generally present in a more indolent fashion. 4,6,10,17 Other factors
that increase the risk of late anastomotic strictures include chronic ductopenic rejection,
prolonged cold ischemia time (>12 hrs), ABO incompatibility, cytomegalovirus (CMV) infection
and recurrent primary sclerosing cholangitis (PSC). 6,10 Patients present with a number of signs
and symptoms of biliary obstruction including jaundice, itching, fever, and pain from cholangitis.
There have been many studies and randomized trials comparing the outcomes of patients with
DD and RYHJ reconstruction. The risk of bile leak in DDLT is not strongly associated with the
method of biliary reconstruction. 18,21 Even though bile duct strictures can be seen with either
approach, at least two large studies report higher stricture rates with RYHJ compared to DD. 2,21
A review of LDLT literature suggests that there are overall higher rates of bile leaks and biliary
strictures compared with DDLT. 5,717,20 DD reconstruction appears to have a lower incidence of
bile leaks but a higher incidence of biliary strictures when compared to RYHJ. 8
We have focused upon bile duct complications. However, there are other significant biliary
complications after liver transplant. These include non-anastomotic strictures, ampullary
dysfunction, hemobilia, choledocholithiasis and mucocele of cystic duct stump. 3,4,6,10 (Table 2)
Diagnosis:
All evaluations for biliary anastomotic leaks and strictures should include a full assessment for
the presence of hepatic artery blood flow. Hepatic artery stenosis or thrombosis can be
identified by duplex sonography or angiography. The diagnosis of both anastomotic strictures
and leaks can be made with imaging techniques such as percutaneous transhepatic
cholangiography (PTC) and endoscopic retrograde cholangiography (ERC). Ultrasonography is
rarely helpful in diagnosing post transplant biliary strictures. Undrained extrahepatic bile
collections can be diagnosed by computed tomography (CT) scan or ultrasound. 2,4,6,10,17,18
Magnetic resonance cholangio pancreatography (MRCP) is gaining popularity as a selective
screening tool in patients with biliary complications. 6
Management of biliary complications
Treatment strategies for biliary complications after liver transplant vary with the experience of
each transplant center. 3,22 However, a few generalizations can be made. The first step in the
management of biliary strictures or leaks aims to ensure hepatic arterial patency. Any inflow
compromise must be definitively treated before a biliary intervention is attempted.
Anastomotic bile leaks after liver transplants (both DD and RYHJ) are almost always managed
surgically. Treatment may include the surgical revision of an anastomosis or the conversion of a
DD to a RYHJ. Some centers have described success managing small anastomotic leaks after liver
transplants with endoscopic stenting (DD) and PTC stenting with an internal-to-external drain
(RYHJ). 3,6,12,21,22 but surgery remains the main stay of treatment.
Endoscopic balloon dilation and stenting is generally the first step in treating biliary strictures
after liver transplant. In patients with RYHJ where endoscopic intervention may not be possible,
PTC dilation with an internal-external drain may be used. Long term results with management
of early strictures are good but delayed strictures tend to be more resistant to therapy. Thus,
patients may require multiple sessions over a 2-3 month period. Refractory strictures and
strictures involving a long segment of bile duct usually require a surgical intervention in the form
of conversion of DD to RYHJ or revision of RYHJ. 3,6,12,21,22 Some centers are more aggressive with
management of biliary strictures and prefer early surgical intervention as opposed to multiple
endoscopic dilations.
Non anastomotic strictures are more refractory to balloon dilation and often require surgical
intervention or re-transplant. Bleeding into the biliary tree can be managed with endoscopic
retrieval of clot and embolization of involved vessel. Sludge and stone formation can be
diagnosed and treated with ERC and PTC approached. The use of ursodeoxcholic acid may
further delay new stone formation. Mucoceles of the cystic duct stump usually need surgical
decompression because they recur if only drained . 6,21,22
Summary
Bile duct complications are common in liver transplant recipients. They occur more frequently in LDLT recipients compared to DDLT. This is probably related to the smaller size of the bile ducts and more variation in the anatomic divisions of the hepatic duct. Surgeons have identified three common techniques for bile duct reconstruction: duct to duct, Roux-en Y hepaticojejunostomy and insertion of the bile duct into the duodenum. To date there is no consensus guiding the selection of one technique over another. The only exception is that most surgeons agree that RYHJ is preferential for patients with extrahepatic biliary disease. Complications of bile duct reconstruction occur with all surgical techniques. However, some complications are more commonly associated with one type of reconstruction compared to another. Important factors that are considered when choosing a technique for bile duct reconstruction includes LDLT vs. DDLT, bile duct anatomy, size discrepancy and access to the biliary tree to treat postoperative complications.
References:
1. Adkins RB Jr, Chapman WC, Reddy VS. Embryology, anatomy and surgical applications of the extrahepatic biliary system. Surg Clin North Am. 2000 Feb;80(1):363-79
2. Colonna JO: Technical problems: biliary. In Transplantation of the liver, end 1. Edited by Busuttil R, Klintmalm G. Philadelphia: WB Saunders Co;1996:617-625
3. Perrakis A, Fortsch T, Schellerer V, Hohenberger W, Muller V. Biliary tract complications after orthotopic liver transplantation: still the “Achilles heel”? Transplantation proceedings 2010;42:4154-57
4. Pascher A, Neuhaus P. Biliary complications after deceased-donor orthotopic liver transplantation. J Hepatobiliary Pancreat Surg 2006;13:487-96
5. Chan SC, Fan ST. Biliary complications after liver transplantation. Hepatol Int 2008;2:399-404
6. Jagannath S, Kalloo AN. Biliary complications after liver transplantation. Curr treatment options in gastroenterology 2002;5:101-12
7. Feng XN, Ding CF, Xing MY, Cai MX, Zheng SS. Technical aspects of biliary reconstruction in adult living donor liver transplantation. Hepatobiliary Pancreat Dis Int. 2011;10(2):136-42
8. Yazumi S, Chiba T. Biliary complications after a right-lobe living donor liver transplantation. J Gastroenterol 2005;40:861-65
9. Bennet W, Zimmerman MA, Campsen J, Mandell MS. Bak T, Wachs M, Kam I. Choledochoduodenostomy is a safe alternative to Roux-en-Y choledochojejunostomy for biliary reconstruction in liver transplantation. World J Surg 2009;33:1022-25
10. Franco J. Biliary complications in liver transplant recipients. Current gastroenterology reports 2005;7:160-4
11. Weiss S, Schmidt S, Ulrich F, Pascher A, Schumacher G, Stockmann M, Puhl G, Guckelberger O, Neumann U, Pratschke J, Neuhaus P. Biliary reconstruction using side to side choledochocholedochostomy with or witout T-tube in deceased donor liver transplantation: A prospective randomized trial. Ann Surg. 2009;250(5):766-71
12. Vougas V, Rela M, Gane E, et al. A prospective randomized trial of bile duct reconstruction at liver transplantation: T tube or no T tube? Transpl Int. 1996;9:392–395
13. Scatton O, Meunier B, Cherqui D, et al. Randomized trial of choledochocholedochostomy with or without a T-tube in orthotopic liver transplantation. Ann Surg. 2001;233:432–437
14. Neuhaus P, Blumhardt G, Bechstein WO, Steffen R, Platz KP, Kech H. Technique and results of biliary reconstruction using side-to-side choledochocholedochostomy in 300 orthotopic liver transplants. Ann Surg. 1994;219(4):426-34
15. Riediger C, Muller MW, Michalski CW, Huser N, Schuster T, Kleeff J, et al. T-tube or no T-tube in the reconstruction of the biliary tract during orthotopic liver transplantation: systematic review and meta-analysis. Liver Transpl 2010;16:705-17
16. Wachs ME, Bak TE, Karrer FM, Everson GT, Shrestha R, Trouillot TE, et al. Adult living donor liver transplantation using a right hepatic lobe. Transplantation 1998;66:1313-1316
17. Liu CL, Lo CM, Fan ST. What is the best technique for right hemiliver living donor liver transplantation? With or without the middle hepatic vein? Duct-to-duct biliary anastomosis or Roux-en-Y hepaticojejunostomy? Journ Hepatol 2005;43:13-17
18. Scanga AE, Kowdley KV. Management of biliary complications following orthotopic liver transplantation. Current gastroenterology reports 2007;9:31-8
19. Grewal HP, Shokouh-Amiri MH, Vera S, Stratta R, Bargous W, Gaber AO. Surgical technique for right lobe adult living donor liver transplantation without venovenous bypass or portocaval shunting and with duct-to-duct biliary reconstruction. Ann Surg 2001;233:502-508
20. Malago M, Testa G, Hertl M, Lang H, Paul A, Frilling A, et al. Biliary reconstruction following right adult living donor liver transplantation end-to-end or end-to-side duct-to-duct anastomosis. Langenbecks Arch Surg 2002;387:37-44
21. Greif F, Bronsther OL, Van Thiel DH et al,: the incidence, timing, and management of biliary tract complications after orthotopic liver transplantation. Ann Surg 1994;219:40-45
22. Kuo OC, Lewis WD, Stokes K, et al: A comparison of operation, endoscopic retrograde cholangiography, and percutaneous transhepatic cholangiography in biliary complications after hepatic transplantation. J Am Coll Surg 1994 179:177
23. Olthoff KM, Merior RM, Ghobrial RM, Abecassis MM, Fair JH, Fisher RA, et al. Outcomes of 385 adult-to-adult living donor liver transplant recipients: a report from the A2ALL consortium. Ann Sugg 2005;243(3):314-23
24. Asonuma K, Okajima H, Ueno M, Takeichi T et al. Feasibility of using the cystic duct for biliary reconstruction in right lobe living donor liver transplantation. Liver Transpl. 2005 Nov;11(11):1431-4
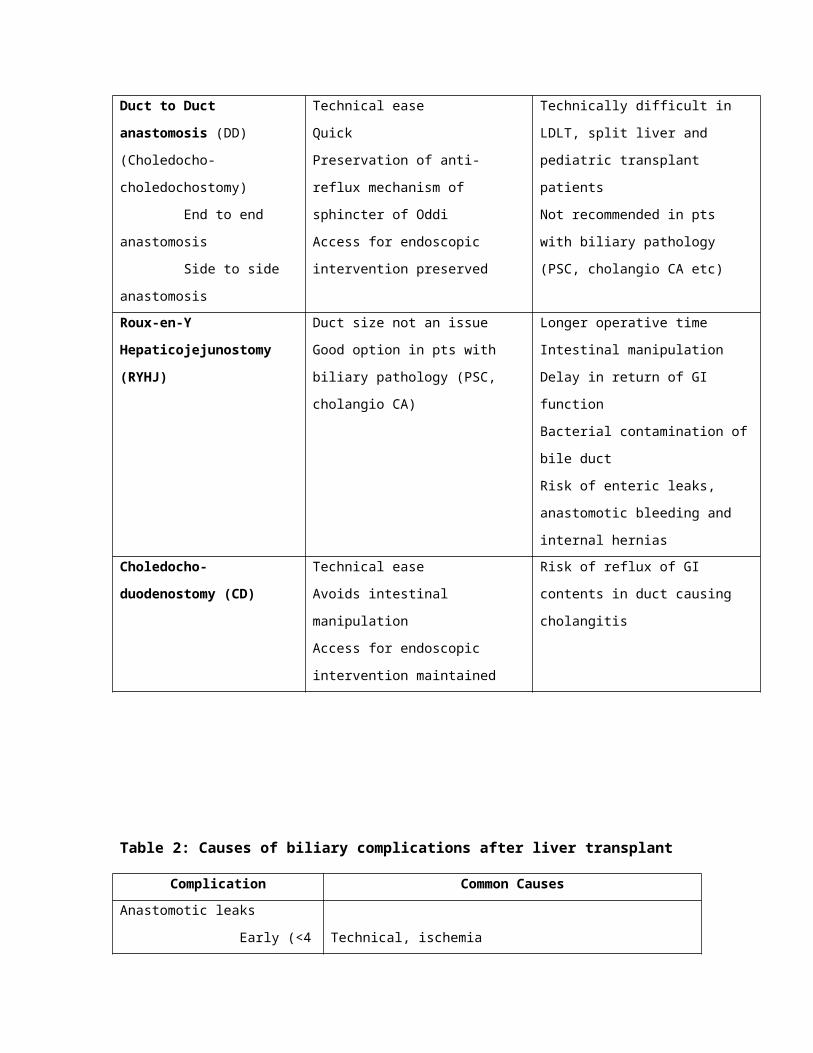
Table 1: Comparison of techniques of bile duct reconstruction during liver transplant.
Technique Advantages Disadvantages
Duct to Duct anastomosis (DD)
(Choledocho-choledochostomy)
End to end anastomosis
Side to side anastomosis
Technical ease
Quick
Preservation of anti-reflux mechanism
of sphincter of Oddi
Access for endoscopic intervention
preserved
Technically difficult in LDLT, split liver
and pediatric transplant patients
Not recommended in pts with biliary
pathology (PSC, cholangio CA etc)
Roux-en-Y Hepaticojejunostomy
(RYHJ)
Duct size not an issue
Good option in pts with biliary
pathology (PSC, cholangio CA)
Longer operative time
Intestinal manipulation
Delay in return of GI function
Bacterial contamination of bile duct
Risk of enteric leaks, anastomotic
bleeding and internal hernias
Choledocho-duodenostomy
(CD)
Technical ease
Avoids intestinal manipulation
Access for endoscopic intervention
maintained
Risk of reflux of GI contents in duct
causing cholangitis
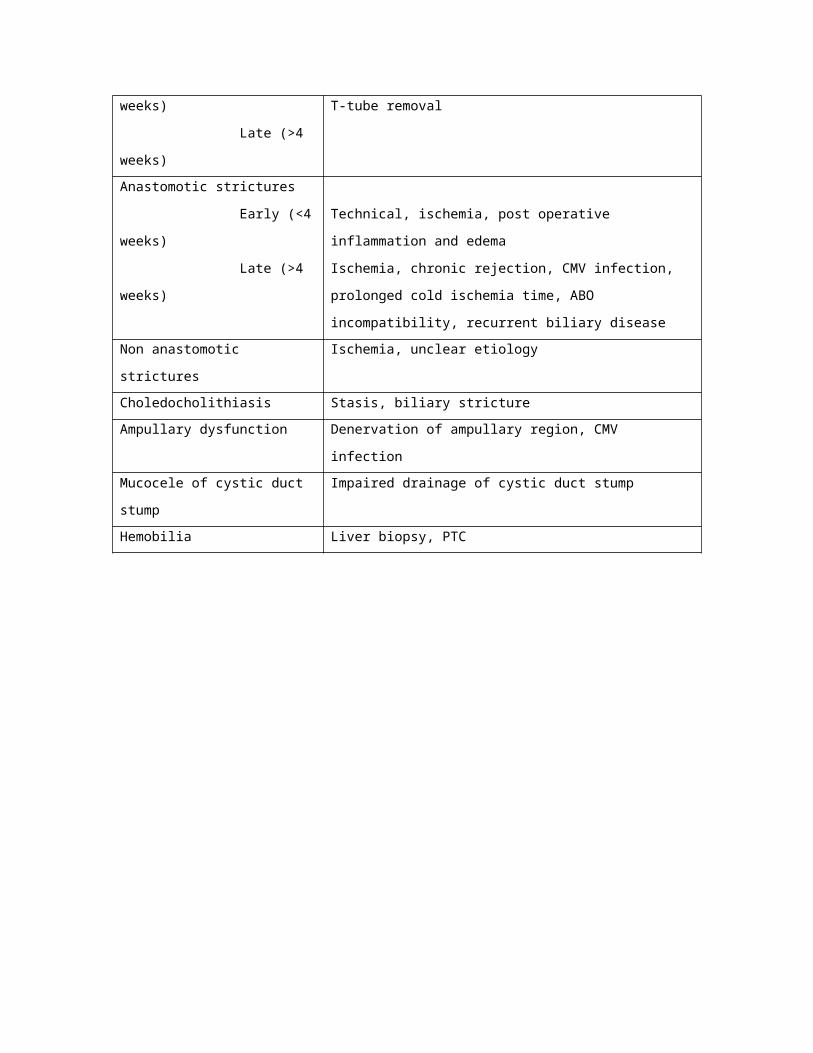
Table 2: Causes of biliary complications after liver transplant
Complication Common Causes
Anastomotic leaks
Early (<4 weeks)
Late (>4 weeks)
Technical, ischemia
T-tube removal
Anastomotic strictures
Early (<4 weeks) Technical, ischemia, post operative inflammation and edema
Late (>4 weeks) Ischemia, chronic rejection, CMV infection, prolonged cold
ischemia time, ABO incompatibility, recurrent biliary disease
Non anastomotic strictures Ischemia, unclear etiology
Choledocholithiasis Stasis, biliary stricture
Ampullary dysfunction Denervation of ampullary region, CMV infection
Mucocele of cystic duct stump Impaired drainage of cystic duct stump
Hemobilia Liver biopsy, PTC
Image 1: Anatomy of the biliary tree. Adapted with permission from Transplantation of the liver. Second edition. Edited by Busuttil R, Klintmalm G. Philadelphia: WB Saunders
Image 2: Roux-en-Y Hepaticojejunostomy (RYHJ)
Image 3: Cholecystoduodenostomy (CD) reconstruction of two right sided bile ducts during LDLT.
Questions:
1) Blood supply to the bile duct anastomosis after liver transplant is mainly derived from:
a. Gastroduodenal arteryb. Left hepatic arteryc. Right hepatic arteryd. Common hepatic arterye. Right gastric artery
Answer: C
2) The most common complication of bile duct reconstruction after liver transplant is:a. Anastomotic strictureb. Cholangitisc. Hemo-biliad. Bile leake. Choldocholithiasis
Answer: D
3) Most of the bile duct reconstructions after standard liver transplants are:a. Duct to duct choledocho-choledochostomyb. Roux-en-Y hepaticojejunostomyc. Choledochojejunostomyd. Side to side choledocho-choledochostomy
Answer: A
4) This method of bile duct reconstruction preserves the natural anti-reflux mechanism of the sphincter of Oddi
a. Duct to duct choledocho-choledochostomyb. Roux-en-Y hepaticojejunostomyc. Choledochoduodenostomy
Answer: A
5) A 40 year old male undergoes a successful deceased donor liver transplant. He is taken back to the operating room on post operative day 1 for bleeding. During the surgery small amount of bile is seen leaking from the anastomosis. The most likely cause of this bile leak is:
a. Bile duct ischemiab. Post operative bleedc. Acute cellular rejectiond. Technical error at time of initial bile duct anastomosis
e. CMV infection
Answer: D
6) A 30 year old woman undergoes liver transplant for primary sclerosing cholangitis. Bile duct is reconstructed using a Roux-en-Y hepaticojejunostomy. Post operatively an anastomotic stricture is suspected. What is the best way to reach the diagnosis in this patient?
a. Endoscopic retrograde cholangiography (ERC)b. Percutaneous transhepatic cholangiography (PTC)c. Computed tomography (CT) scan of the liverd. Duplex sonography of the transplanted liver
Answer: B
7) The best reconstruction option during right living donor liver transplant for two bile duct orifices 1 cm apart is:
a. Duct to duct choledocho-choledochostomyb. Side to side choledocho-choledochostomyc. Roux-en-Y hepaticojejunostomyd. Choledochoduodenostomy
Answer: C
8) Living donor liver transplants (LDLT) are associated with a higher rate of biliary complications than deceased donor liver transplants (DDLT)
a. Trueb. False
Answer: True
9) Duct-to-duct anastomosis should never be performed in living donor liver transplants
a. Trueb. False
Answer: False
10) Most of the transplant centers in the US routinely use T-tubes as part of bile duct reconstruction
a. Trueb. False
Answer: False