Bilateral multiple spindle cell lipomas of the tongue
6
Bilateral multiple spindle cell lipomas of the tongue Tomoaki Imai, DDS, PhD, a Masahiro Michizawa, DDS, PhD, b Hidetaka Shimizu, DDS, PhD, c Takumi Imai, DDS, PhD, d Naonori Yamamoto, DDS, e and Yoshiaki Yura, DDS, PhD, f Osaka and Nara, Japan SAISEIKAI SENRI HOSPITAL, OSAKA UNIVERSITY GRADUATE SCHOOL OF DENTISTRY, AND TENRI HOSPITAL Spindle cell lipoma (SCL) typically occurs in elderly men as a solitary lesion in the posterior neck and back, but less commonly also involves the oral cavity. Here, we describe a rare case of bilateral multiple SCLs of the tongue. The patient was a 72-year-old Japanese man with multiple painless soft nodules in the bilateral margins of the tongue. The patient was not obese, and had used alcohol moderately for more than 40 years. A clinical diagnosis of multiple tongue lipomas was made. The tumors were resected surgically, and they exhibited the histopathological features of SCL, composed of mature fat cells, collagen-forming CD34-positive spindle cells, and sparse mast cells. This suggests that differential diagnosis of intraoral multiple lipomatous nodules should include not only lipomatosis but also multiple SCLs, notwithstanding the rare incidence of the latter. (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;106:264-9) Lipomas are the most frequent benign soft tissue tu- mors, occurring as a slowly enlarging, painless mass formation. They commonly affect the upper back and shoulder, but also occur in the oral cavity in lower rates, predominantly the buccal mucosa, followed by the lip and the tongue. 1,2 Multiple involvement is known as benign symmetrical lipomatosis (BSL; Madelung’s dis- ease), and characterized by the diffuse growth of non- encapsulated lipomas. 3,4 Multiple tongue lipomas, 5 particularly symmetric tumor formation, is called sym- metric lipomatosis of the tongue (SLT). 6-10 Histologically, lipomas are classified into various subtypes, including simple lipoma, fibrolipoma, angio- lipoma, myxoid lipoma, pleomorphic lipoma, and spin- dle cell lipoma. Spindle cell lipoma (SCL), an uncom- mon variant first reported by Enzinger and Harvey in 1975, 11 is composed of mature fat cells, collagen-form- ing spindle cells, and sparse mast cells. SCL typically occurs in elderly men as a solitary lesion in the poste- rior neck and back, 11,12 but may less commonly also involve the oral cavity. 13,14 Because the occurrence of multiple intraoral SCLs is extremely rare 15 and their clinical appearance is similar to that of conventional lipoma, multiple lipomatous nodules of the tongue would be clinically diagnosed as multiple tongue lipo- mas or SLT. Here we describe a case of bilateral multiple SCLs of the tongue. A CASE REPORT A 72-year-old Japanese man attended Saiseikai Senri Hospital complaining of painless soft nodules in the left margin of the tongue, first noticed 2 weeks previously. Clinical examination revealed 2 tumors with maximal diameters of 12 mm and 15 mm in the left margin of the tongue. The covering mucosa appeared normal (Fig. 1). Further examination showed 3 smaller submucosal nod- ules ranging from 3 mm to 5 mm in the right margin. Palpation revealed elastic soft nodules of the tongue and no lymphatic node enlargement in the neck. No tumor masses were identified on the trunk, head and neck, or extremities. There was no family history of similar tu- mors. The patient had a history of angina pectoris, was not obese, had no allergies to foods or medications, did not smoke, and had used alcohol moderately for more than 40 years. Laboratory data were within normal limits. Com- puted tomography (CT) and magnetic resonance imaging (MRI) failed to delineate the tumor masses because of metal artifacts from full-cast crowns on neighboring teeth, but detected no enlarged lymphatic nodes in the neck. On the basis of these findings, a clinical diagnosis of multiple tongue lipomas was made. The 2 large lesions in the left side were resected under general anesthesia, followed 3 months later by those on the right under local anesthesia. Macroscopi- a Clinical Fellow, Department of Oral and Maxillofacial Surgery, Saiseikai Senri Hospital, Suita, Osaka, Japan. b Head, Department of Oral and Maxillofacial Surgery, Saiseikai Senri Hospital, Suita, Osaka, Japan. c Assistant Professor, Department of Oral and Maxillofacial Surgery II, Osaka University Graduate School of Dentistry, Suita, Osaka, Japan. d Clinical Fellow, Department of Oral and Maxillofacial Surgery, Tenri Hospital, Tennri, Nara, Japan. e Graduate Fellow, Department of Oral and Maxillofacial Surgery II, Osaka University Graduate School of Dentistry, Suita, Osaka, Japan. f Professor, Department of Oral and Maxillofacial Surgery II, Osaka University Graduate School of Dentistry, Suita, Osaka, Japan. Received for publication Dec 18, 2007; returned for revision Feb 18, 2008; accepted for publication Feb 18, 2008. 1079-2104/$ - see front matter © 2008 Mosby, Inc. All rights reserved. doi:10.1016/j.tripleo.2008.02.026 264
-
Upload
tomoaki-imai -
Category
Documents
-
view
217 -
download
1
Transcript of Bilateral multiple spindle cell lipomas of the tongue

Bilateral multiple spindle cell lipomas of the tongueTomoaki Imai, DDS, PhD,a Masahiro Michizawa, DDS, PhD,b Hidetaka Shimizu, DDS, PhD,c
Takumi Imai, DDS, PhD,d Naonori Yamamoto, DDS,e and Yoshiaki Yura, DDS, PhD,f Osakaand Nara, JapanSAISEIKAI SENRI HOSPITAL, OSAKA UNIVERSITY GRADUATE SCHOOL OF DENTISTRY, AND TENRIHOSPITAL
Spindle cell lipoma (SCL) typically occurs in elderly men as a solitary lesion in the posterior neck and back, butless commonly also involves the oral cavity. Here, we describe a rare case of bilateral multiple SCLs of the tongue. Thepatient was a 72-year-old Japanese man with multiple painless soft nodules in the bilateral margins of the tongue. Thepatient was not obese, and had used alcohol moderately for more than 40 years. A clinical diagnosis of multiple tonguelipomas was made. The tumors were resected surgically, and they exhibited the histopathological features of SCL,composed of mature fat cells, collagen-forming CD34-positive spindle cells, and sparse mast cells. This suggests thatdifferential diagnosis of intraoral multiple lipomatous nodules should include not only lipomatosis but also multiple SCLs,
notwithstanding the rare incidence of the latter. (Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2008;106:264-9)Lipomas are the most frequent benign soft tissue tu-mors, occurring as a slowly enlarging, painless massformation. They commonly affect the upper back andshoulder, but also occur in the oral cavity in lower rates,predominantly the buccal mucosa, followed by the lipand the tongue.1,2 Multiple involvement is known asbenign symmetrical lipomatosis (BSL; Madelung’s dis-ease), and characterized by the diffuse growth of non-encapsulated lipomas.3,4 Multiple tongue lipomas,5
particularly symmetric tumor formation, is called sym-metric lipomatosis of the tongue (SLT).6-10
Histologically, lipomas are classified into varioussubtypes, including simple lipoma, fibrolipoma, angio-lipoma, myxoid lipoma, pleomorphic lipoma, and spin-dle cell lipoma. Spindle cell lipoma (SCL), an uncom-mon variant first reported by Enzinger and Harvey in1975,11 is composed of mature fat cells, collagen-form-ing spindle cells, and sparse mast cells. SCL typicallyoccurs in elderly men as a solitary lesion in the poste-
aClinical Fellow, Department of Oral and Maxillofacial Surgery,Saiseikai Senri Hospital, Suita, Osaka, Japan.bHead, Department of Oral and Maxillofacial Surgery, SaiseikaiSenri Hospital, Suita, Osaka, Japan.cAssistant Professor, Department of Oral and Maxillofacial Surgery II,Osaka University Graduate School of Dentistry, Suita, Osaka, Japan.dClinical Fellow, Department of Oral and Maxillofacial Surgery,Tenri Hospital, Tennri, Nara, Japan.eGraduate Fellow, Department of Oral and Maxillofacial Surgery II,Osaka University Graduate School of Dentistry, Suita, Osaka, Japan.fProfessor, Department of Oral and Maxillofacial Surgery II, OsakaUniversity Graduate School of Dentistry, Suita, Osaka, Japan.Received for publication Dec 18, 2007; returned for revision Feb 18,2008; accepted for publication Feb 18, 2008.1079-2104/$ - see front matter© 2008 Mosby, Inc. All rights reserved.
doi:10.1016/j.tripleo.2008.02.026264
rior neck and back,11,12 but may less commonly alsoinvolve the oral cavity.13,14 Because the occurrence ofmultiple intraoral SCLs is extremely rare15 and theirclinical appearance is similar to that of conventionallipoma, multiple lipomatous nodules of the tonguewould be clinically diagnosed as multiple tongue lipo-mas or SLT. Here we describe a case of bilateralmultiple SCLs of the tongue.
A CASE REPORTA 72-year-old Japanese man attended Saiseikai Senri
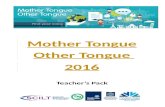
Hospital complaining of painless soft nodules in the leftmargin of the tongue, first noticed 2 weeks previously.Clinical examination revealed 2 tumors with maximaldiameters of 12 mm and 15 mm in the left margin of thetongue. The covering mucosa appeared normal (Fig. 1).Further examination showed 3 smaller submucosal nod-ules ranging from 3 mm to 5 mm in the right margin.Palpation revealed elastic soft nodules of the tongue andno lymphatic node enlargement in the neck. No tumormasses were identified on the trunk, head and neck, orextremities. There was no family history of similar tu-mors. The patient had a history of angina pectoris, was notobese, had no allergies to foods or medications, did notsmoke, and had used alcohol moderately for more than 40years. Laboratory data were within normal limits. Com-puted tomography (CT) and magnetic resonance imaging(MRI) failed to delineate the tumor masses because ofmetal artifacts from full-cast crowns on neighboring teeth,but detected no enlarged lymphatic nodes in the neck. Onthe basis of these findings, a clinical diagnosis of multipletongue lipomas was made.
The 2 large lesions in the left side were resectedunder general anesthesia, followed 3 months later by
those on the right under local anesthesia. Macroscopi-
OOOOEVolume 106, Number 2 Imai et al. 265
cally, the lesions consisted of encapsulated, easily enu-cleated whitish-yellow nodules (Fig. 2). Histopatho-logic examination revealed that all lesions werecomposed of mature adipocytes with a clear cytoplasm,well-aligned fibroblastic spindle cells, and wiry colla-gen bundles (Fig. 3), with no evidence of cellular atypiaor pleomorphism. A histopathological diagnosis ofSCL was made. The relative proportions of adipocytesand spindle cells varied markedly in different areaswithin the large lesions of the left tongue (Fig. 3, A),particularly with the appearance of the spindle cellcomponent (Fig. 3, B). Furthermore, fat cells dominatedthe area neighboring this component in the same lesion(Fig. 3, C). In contrast, this intratumor variation wasalmost completely absent in all small lesions of theright tongue(Fig. 3, D), which were essentially devoidof a large spindle cell component and showed a largelyhomogeneous appearance with approximately equalproportions of adipocytes and spindle cells. The myx-oid area was localized in the spindle cell componentand homogeneously positive-stained with alcian blue,
Fig. 1. Clinical appearance. Submucosal lipomatous nodulesare seen in the left (A) and right (B) side of the tongue(arrows).
indicating the existence of abundant acid mucopolysac-
charides (Fig. 4). Immunohistochemical staining forCD34 demonstrated intracytoplasmic reactivity in spin-dle cells but not adipocytes, which had immunoreac-tivity for S-100 antibody (Fig. 5). Further, mast cellsimmunoreactive for tryptase, a mast cell marker, werepredominantly scattered among the spindle cells andcollagen bundles (Fig. 6).
No sign of recurrence has been observed at 1 yearafter the second operation.
DISCUSSIONSCL is a relatively uncommon benign tumor that
accounts for approximately 1.5% of all adipocytic neo-plasms.16 Although usually occurring as a solitary le-sion, about 0.5% to 3.0% of cases are of multipletumors.17 Previous reports of oral lipomas also de-scribed a low occurrence of 1.36% (2 SCL cases of 146oral lipomas)13 or 2.2% (1 case of 46 lipomas).1 Fur-long et al.,2 however, recently reported 59 SCL cases(47%) of 125 lipomas in the oral and maxillofacialregion, indicating that oral SCL may be more common
Fig. 2. Excised tumors. A, Encapsulated whitish-yellow tu-mor on the left side. B, Smaller tumor nodules on the rightside.
than previously estimated. Although review of the lit-

sion w
OOOOE266 Imai et al. August 2008
erature reveals more than 50 cases of intraoral SCL,2,14
SCL of the tongue is relatively uncommon,18-20 andonly one of these was of multiple SCLs,15 in that case
Fig. 3. Micrographic appearance. The tumors consist of a m(hematoxylin and eosin stain). A, A low-magnification photointerface between the adipocytic component and collagenousSpindle cell–rich area of the anterior lipoma of the left tonguof the same tumor nodule (�100). D, The central lipoma of tof fat cell and spindle cell areas, compared with the large le
Fig. 4. Alcian blue-staining for myxoid matrix. High-magnifi-cation photomicrograph of the myxoid area in the spindle cellcomponent of the anterior lipoma of the left tongue (�200). Theintracellular matrix varies from collagenous to myxoid. A typicalmyxoid matrix stained homogeneously is shown (arrows).
occurring bilaterally in the margin of the tongue.
Histologically, SCL displays an admixture of maturefat cells and well-aligned uniform spindle cells withstrong immunoreactivity for CD34 in a fibrocollag-enous and myxoid background.11 CD34 was originallyidentified on the surface of hematopoietic progenitorcells of the lymphoid and myeloid lineage,21 and is alsoexpressed in nonhematopoietic tissues and their neo-plasms, including dermal dendritic cells, endoneurialcells, solitary fibrous tumors, and interstitial dendriticspindle cell components of lipomatous neoplasms.22,23
Spindle cells are believed to be nonlipoblastic stellatemesenchymal cells of the primitive fat lobules that havelost their ability to differentiate to lipocytes but arenevertheless capable of collagen synthesis.24
With regard to the clinical and histological differen-tial diagnosis of solitary SCL, consideration should begiven to the possibility of well-differentiated liposar-coma, which requires more radical treatment.12 SCLcan be differentiated from the liposarcoma by its well-circumscribed form, superficial location, slow growth,few or no lipoblasts, the uniformity and association ofthe spindle cells with collagen bundles, sparse vascu-larity, and the absence of atypical cells.12,25-27 How-ever, well-differentiated liposarcoma can also arise inthe tongue as a slow-growing and circumscribed sub-
of mature lipocytes and spindle cells in varying proportionsgraph of the anterior lipoma of the left tongue, showing the
cell component. The tumor is thinly encapsulated (�40). B,the thick wiry collagen bundles (�100). C, Adipocytic areat. This small mass lesion displays homogeneous distributionith intratumor variation (�100).
ixturemicro
spindlee. Notehe righ
mucosal mass.26 Pleomorphic lipoma exhibits features

OOOOEVolume 106, Number 2 Imai et al. 267
similar to SCL, but can be differentiated by the pres-ence of floret-type giant cells.24
With regard to the histological features of myxoidinterstitial material in SCL, some cases contain anabundant myxoid matrix,28 while others display collag-enous interstitium with small amount of myxoid.20 Thepresent case might be considered a combination ofthese types. The highly myxoid pattern with few spin-dle cells simulates myxoma or myxolipoma. Further-more, SCL is occasionally indistinguishable from den-dritic fibromyxolipoma,29 which is characterized byspindle or stellate fibroblastic cells admixed with adi-pose tissue in an abundant myxoid and collagenizedstroma. Although a vascular pattern is usually incon-spicuous in SCL, prominent vascularization in certainsegments might lead to a misdiagnosis of angiolipoma
Fig. 5. Immunohistochemistry of CD34 and S-100. A, Spin-dle cells are strongly immunopositive for CD34 (�200). B,Mature lipocytes stain positive for S-100 protein, while thespindle cell area is negative for S-100 protein (�200).
or angiomyxolipoma.30
The proportion of spindle cells in SCL varies in differ-ent areas within the same lesion.11,31 In multiple SCLs ofthe trunk and extremities, the lesions became increasinglymore cellular as they develop over time.17 The previousreport of intraoral multiple SCLs15 presented 2 uniformtumors of 30 mm and 24 mm, but did not describe thedistribution of spindle cell areas. The finding in ourpresent case that collagen-forming spindle cell areas werepredominant in the large but not small lesions indicatesthat the increasing cellularity with development occursindependently of tumorigenesis region. This characteristicmay be associated with mast cell infiltration, on the basisthat mast cells have biological effects on mesenchymalcell proliferation and collagen production.32,33 On his-topathological diagnosis, the predominant collagen andspindle cell area in SCL may cause the tumor to berecognized as a nonlipomatous lesion,31 such as a solitaryfibrous tumor, but in contrast as a conventional lipoma ifthe localized spindle cells are overlooked. The possibilityof misdiagnosis on incisional biopsy of a large lesion isthus increased.
In the present case, the clinical presentation of multipleinvolvement suggested little potential for malignant lipo-matous neoplasm. A clinical diagnosis of multiple tonguelipomas that might develop to SLT was thus made, buthistopathological examination confirmed a diagnosis ofmultiple SCLs. Moreover, a review of tongue liposarco-mas in 32 cases described 2 cases of submucosal multi-nodular lesions.27 These findings suggest that differentialdiagnosis of intraoral multiple lipomatous nodules, partic-
Fig. 6. Immunohistochemistry of tryptase, a mast cellmarker. Mast cells are predominantly sparse among spindlecells and collagen bundles in the spindle cell-rich area (bar)(�200).
ularly of the tongue, should include not only lipomatosis

the ton
OOOOE268 Imai et al. August 2008
but also multiple lesions of SCL or liposarcoma, notwith-standing the rare incidence of the latter.
The term SLT has been clinically used to describelipomatosis involving only the tongue (Table I).6-10 Incontrast, BSL initially appears predominantly on theposterior neck and spreads sequentially in a caudaldirection,3,4,17 with only rare involvement of thetongue.34-36 Although SLT and BSL share the samehistopathological features, recent reports have sug-gested different etiologies. SLT has a different ethnicbackground to BSL, and is less relevant than BSL tomedical conditions such as alcoholism and obesity.6-10
A recent study suggested that BSL was associated withbrown fat mitochondrial dysfunction,37 but the etiologyof SLT has not be clearly elucidated.
In terms of the most common initial site and direc-tion of progress, multiple SCLs resemble BSL (TableI).17 In contrast to this similarity in clinical appearance,multiple SCL patients share no common medical con-dition or environmental exposure.17 However, the factthat the present patient had used alcohol moderatelysuggests that an etiological mechanism involving alco-hol remains a possibility, as occurs with lipomatosis.The small number of cases means that the etiologicaldifferences between the conventional widespread pat-tern of multiple SCLs in Caucasian men and the local-ized lingual pattern in Japanese men cannot yet beclarified. Further differentiation awaits the accumula-tion of additional cases.
With regard to treatment, the gold standard for symp-tomatic SCL is complete surgical resection, but this can
Table I. Clinical features of lipomatosis and multiple
Lipomatosis
BSL
Predominant locations Posterior neck and uppertrunk; �rareinvolvement of thetongue
Tongue on
Number of cases Over 200 7Sex (male:female) M:F � 15:1 All M
Average age, y 52 68Predominant ethnic
backgroundMediterranean descent Asian men
Associated medicalconditions
Alcoholism (60%-90%),liver disease, obesity
Weaker as1 alcoho5 nondr
References 3, 4, �34-36 6-10
BSL, benign symmetric lipomatosis; SLT, symmetric lipomatosis of
lead to postexcisional cosmetic or functional disorders in
the case of multiple SCLs or a large solitary lesion. For-tunately, our present patient did not develop a postopera-tive feeding disorder or disturbance of pronunciation. Be-chara et al.38 recently reported the use of injectionlipolysis with phosphatidylcholine to reduce tumor vol-umes, and this will likely become an effective therapeuticoption for patients with multiple conventional lipomas.Injection lipolysis may also be valuable as preoperativetherapy in progressive multiple SCLs.
No clear case of malignant transformation of SCLhas been reported to date. However, Harvell39 recentlydescribed a 48-year-old man with multiple SCLs of theneck who suffered a fibrosarcomatous transformationof the chest into dermatofibrosarcoma protuberans(DFSP), a CD34-positive neoplasm of intermediate ma-lignancy derived from interstitial dendritic cells. Thesemesenchymal cells are considered to have the ability todifferentiate into CD34-positive spindle cells.23 Thiscase may suggest the potential for malignant neoplasticconversion of spindle cells in patients with multipleSCLs.
Generally, solitary SCL shows no features of localrecurrence after total excision,17 with only 1 case reportedto date.16 In the case of multiple involvement, consider-ation should be given to the possibility of sequential andmulticentric development of lesions over several years,and the postoperative area should be carefully monitored.
The authors thank Dr. Aki Kakutani, Department of Pathol-ogy and Laboratory Medicine, Saisekai Senri Hospital, foradvice and for confirmation of the histopathological diagno-
mSCLs
mSCLs
mSCLs of thetongue (previous
and present cases)
Posterior neck and uppertrunk
Tongue only
19 2Familial: both sexes
(male predominant)Non-familial: all M
all M
55.2 73.5Caucasian men Japanese men
n than BSL;ild drinker,
No particular Previous case: NDPresent case:moderatedrinker
17, 39 15
gue; mSCLs, multiple spindle cell lipomas; ND, not described
SCLs
SLT
ly
sociatiolic, 1 m
inker
sis.

OOOOEVolume 106, Number 2 Imai et al. 269
REFERENCES1. Fregnani ER, Pires FR, Falzoni R, Lopos MA, Vargas PA.
Lipomas of the oral cavity: clinical findings, histological classi-fication and proliferative activity of 46 cases. Int J Oral Maxil-lofac Surg 2003;32:49-53.
2. Furlong MA, Fanburg-Smith JC, Childers EL. Lipoma of the oraland maxillofacial region: site and subclassification of 125 cases.Oral Surg Oral Med Oral Pathol Oral Radiol Endod2004;98:441-50.
3. Kohan D, Miller PJ, Rothstein SG, Kaufman D. Madelung’sdisease: case reports and literature review. Otolaryngol HeadNeck Surg 1993:108:156-9.
4. Meningaud JP, Pitak-Arnnop P, Bertrand JC. Multiple symmet-ric lipomatosis: case report and review of the literature. J OralMaxillofac Surg 2007;65:1365-9.
5. Pisanty S. Bilateral lipomas of the tongue. Oral Surg1976;42:451-3.
6. Ogawa A, Nakamura H, Takahashi H. Benign symmetric lipo-matosis of the tongue: report of a case. J Oral Maxillofac Surg1988;46:502-4.
7. Katou F, Shirai N, Motegi K, Satoh R, Satoh S. Symmetricallipomatosis of the tongue presenting as macroglossia. Report oftwo cases. J Craniomaxillofac Surg 1993;21:298-301.
8. Calvo-Garcia N, Prieto-Prado M, Alonso-Orcajo N, Junquera-Gutierrez LM. Symmetric lipomatosis of the tongue: report of acase and review of the literature. Oral Surg Oral Med Oral PatholOral Radiol Endod 1999;87:610-2.
9. Jinbu Y, Otawa K, Obi Y, Tsukahara T, Kusama M, NakagawaH. Symmetric lipomatosis of the tongue: report of a case. OralMed Pathol 2004;9:123-6.
10. Ishikawa Y, Katada Y, Enomoto M, Kawada K, Okamoto Y,Ozawa M. A case of symmetrical lipomatosis of the tonguepresenting as macroglossia. Oral Science International 2006;3:90-3.
11. Enzinger FM, Harvey DA. Spindle cell lipoma. Cancer1975;36:1852-9.
12. Enzinger FM, Weiss SW. Spindle cell lipoma. In: Enzinger FM,editor. Soft tissue tumors. 3rd ed. St Louis (MO): Mosby; 1995.p. 395-9.
13. Said-Al-Naief N, Zahurullah FR, Sciubba JJ. Oral spindle celllipoma. Ann Diagn Pathol 2001;5:207–5.
14. Billings SD, Henley JD, Summerlin DJ, Vakili S, Tomich CE.Spindle cell lipoma of the oral cavity. Am J Dermatopathol2006;28:28-31.
15. Kaku N, Kashima K, Daa T, Nakayama I, Kerakawauchi H,Hashimoto H, et al: Multiple spindle cell lipomas of the tongue:report of a case. APMIS 2003;111:581-5.
16. Fletcher CD, Martin-Bates E. Spindle cell lipoma: a clinicopath-ological study with some original observations. Histopathology1987;11:803-17.
17. Fanburg-Smith JC, Devaney KO, Miettinen M, Weiss SW. Mul-tiple spindle cell lipomas: a report of 7 familial and 11 nonfa-milial cases. Am J Surg Pathol 1998;22:40-8.
18. McDaniel RK, Newland JR, Chiles DG. Intraoral spindle celllipoma: case report with correlated light and electron micros-copy. Oral Surg Oral Med Oral Pathol 1984;57:52-7.
19. Lombardi T, Odell EW. Spindle cell lipoma of the oral cavity:report of a case. J Oral Pathol Med 1994;23:237-9.
20. Dutt SN, East DM, Saleem Y, Jones EL. Spindle-cell variant ofintralingual lipoma—report of a case with literature review. JLaryngol Otol 1999;113:587-9.
21. Andrews RG, Singer JW, Bernstein ID. Monoclonal antibody12-8 recognizes a 115-kd molecule present on both unipotent andmultipotent hematopoietic colony-forming cells and their precur-
sors. Blood 1986;67:842-5.22. van de Rijn M, Rouse RV. CD34: a review. App Immunohisto-chem 1994;2:71-80.
23. Suster S, Fisher C. Immunoreactivity for the human hematopoi-etic progenitor cell antigen (CD34) in lipomatous tumors. Am JSurg Pathol 1997;21:195-200.
24. Beham A, Schmid C, Hodl S, Fletcher CD. Spindle cell andpleomorphic lipoma: an immunohistochemical study and histo-genetic analysis. J Pathol 1989;158:219-22.
25. Piattelli A, Fioroni M, Rubini C. Spindle cell lipoma of the oralcavity: report of a case. J Oral Maxillofac Surg 1999;57:624-5.
26. Nascimento AF, McMenamin ME, Fletcher CD. Liposarcomas/atypical lipomatous tumors of the oral cavity: a clinicopathologicstudy of 23 cases. Ann Diagn Pathol 2002;6:83-93.
27. Allon I, Vered M, Dayan D. Liposarcoma of the tongue: clinico-pathologic correlations of a possible underdiagnosed entity. OralOncol 2005;41:657-65.
28. Tosios K, Papanicolaou SI, Kapranos N, Papadogeorgakis N.Spindle cell lipoma of the oral cavity. Int J Oral Maxillofac Surg1995;24:363-4.
29. Suster S, Fisher C, Moran CA. Dendritic fibromyxolipoma: clini-copathologic study of a distinctive benign soft tissue lesion that maybe mistaken for a sarcoma. Ann Diagn Pathol 1998;2:111-20.
30. Tardío JC, Martín-Fragueiro LM. Angiomyxolipoma (vascularmyxolipoma) of subcutaneous tissue. Am J Dermatopathol2004;26:222-4.
31. Billings SD, Folpe AL. Diagnostically challenging spindle celllipomas: a report of 34 ”low-fat” and ”fat-free” variants. Am JDermatopathol 2007;29:437-42.
32. Gruber BL, Kew RR, Jelaska A, Marchese MJ, Garlick J, Ren S, etal. Human mast cells activate fibroblasts: tryptase is a fibrogenicfactor stimulating collagen messenger ribonucleic acid synthesis andfibroblast chemotaxis. J Immunol 1997;158:2310-7.
33. Sakai H, Kuroda K, Hara D, Tajima S. Coexistence of spindlecell lipoma and ordinary lipoma. J Dermatol 2004;31:831-4.
34. Ghislain PD, Garzitto A, Legout L, Alcaraz I, Creusy C, Modi-ano P. Symmetrical benign lipomatosis of the tongue and Lau-nois-Bensaude lipomatosis. Ann Dermatol Venereol 1999;126:147-9. French.
35. Vargas-Díez E, Daudén E, Jones-Caballero M, García-Díez A.Madelung’s disease involving the tongue. J Am Acad Dermatol2000;42:511-3.
36. Lopez-Ceres A, Aguilar-Lizarralde Y, Villalobos Sánchez A,Prieto Sánchez E, Valiente Alvarez A. Benign symmetric lipo-matosis of the tongue in Madelung’s disease. J CraniomaxillofacSurg 2006;34:489-93.
37. Klopstock T, Naumann M, Seibel P, Shalke B, Reiners K,Reichmann H. Mitochondrial DNA mutations in multiple sym-metric lipomatosis. Mol Cell Biochem 1997;174:271-5.
38. Bechara FG, Sand M, Sand D, Rotterdam S, Stücker M, Altm-eyer P, et al. Lipolysis of lipomas in patients with familialmultiple lipomatosis: An ultrasonography-controlled trial. J Cu-tan Med Surg 2006;10:155-9.
39. Harvell JD. Multiple spindle cell lipomas and dermatofibrosar-coma protuberans within a single patient: evidence for a commonneoplastic process of interstitial dendritic cells? J Am AcadDermatol 2003;48:82-5.
Reprint requests:
Tomoaki Imai, DDS, PhDDepartment of Oral and Maxillofacial SurgerySaiseikai Senri Hospital1-1-6 Tsukumodai, SuitaOsaka 565-0862, Japan
[email protected]