BIHAR A RAPID PRIVATE HEALTH SECTOR...
32
BIHAR A RAPID PRIVATE HEALTH SECTOR ASSESSMENT A Discussion Document The World Bank South Asia Region May 2005 Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized Public Disclosure Authorized
Transcript of BIHAR A RAPID PRIVATE HEALTH SECTOR...

BIHARA RAPID PRIVATE HEALTH SECTOR ASSESSMENT
A Discussion Document
The World BankSouth Asia Region
May 2005
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
Pub
lic D
iscl
osur
e A
utho
rized
wb350881
Typewritten Text
56169


Table of Contents
I Health Status................................................................................................................... 1
II Delivery System and Health Seeking Behavior ........................................................... 4
Delivery System .............................................................................................................. 4Government Health Facilities ...................................................................................... 4Private Health Facilities .............................................................................................. 6
Health Seeking Behavior ............................................................................................... 6Factors That Influence Health Seeking Behavior ........................................................ 6Demand For Private Providers .................................................................................... 8Affordability, Accessibility and Quality of Care .......................................................... 9Initial Observations on Health-seeking Behaviors ...................................................... 9
III Health Care Financing and Insurance ....................................................................... 12
Health Care Financing................................................................................................. 12Government Spending on Health Care ...................................................................... 12Out of Pocket Expenditures ........................................................................................ 12Community-based General Savings Funds ................................................................ 13Costs of Health Care by Type of Provider .................................................................. 14
Health Insurance .......................................................................................................... 16Private Health Insurance ........................................................................................... 16Universal Health Insurance Scheme .......................................................................... 17
IV Key Private Sector Issues ............................................................................................ 18
Introduction .................................................................................................................. 18Public Private Partnerships ........................................................................................ 18
Partnering with a not-for-profit – the The Kurji Holy Family Hospital .................... 18Bihar Volunteer Health Association (BVHA) ............................................................. 19Partnering with a For-Profit Hospital ....................................................................... 19The Pros and Cons of Subsidized Services................................................................. 20
V Options for Maximizing the Potential of the Private Sector .........................................21
Key Health Care Challenges for Bihar ...................................................................... 21Improving the Primary Health Care System ............................................................ 21Engaging the Private Sector ........................................................................................ 22Improving the Performance of Informal Providers.................................................. 23Private Sector Financing Options............................................................................... 24
Selected Bibliography .......................................................................................................... 26


ACKNOWLEDGEMENTS
This policy note is based on the findings of World Bank mission that visited Bihar in January2004. The team consisted of Ismail Radwan and Jet Riparip (consultant). The team was supportedin Delhi by Nina Anand, Ritika Rodrigues and H. Bhawani. The authors would also like toacknowledge the work of Chiaki Yamamoto on social franchising issues and the Janani casestudy.
During a two-week period, the mission team visited public and private health facilities in andaround Patna. The team also undertook announced and unannounced visits to several publicand private hospitals. Field visits also included a sub-centre, a primary health centre, and threecommunity health centers. The team also spent considerable time visiting the Janani facilitiesboth at the head office and some examples in the field of Titli centers and Surya Clinics.
During the mission, the team met with a broad range of health sector stakeholders includinggovernment officials, public and private health providers, members of the private sector, NGOsactive in the field and various research institutes. This report would not have been possiblewere it not for their remarkable combined support.
The mission team would like to take this opportunity to thank the following government officialsof the Department of Health and Family Welfare; Sri Ashok Kumar Chowdhury, (Secretary ofHealth), Dr. A. K. Tiwari (State Program Officer IDT), and Dr. Vishwa Ratan (retired officer)who kindly accompanied the team on several field visits. The team enjoyed extensive discussionswith the private sector including; Dr Satyajit Singh (Dr. Ruban Memorial Hospital), Dr. AhmadHai (MD Hai Medicare & Research Institute), Sisters Sophie and Julie (Kurji Holy FamilyHospital), Mr. Abhay Singh (CII), Ms. Viji Srinivasan (ADITHI), and Mr. Chandrashekar (IPAS).The team would also like to thank Dr. Moses Vijayakumar (Project Officer UNICEF) and Mr.Keshri (Director Amrapali Foods Ltd).
We would like to thank all the staff of Janani for their warm welcome and the time they spentwith us especially; Dr. Gopi Gopalakrishnan (Program Director), Ms. Vimla Menezes (GM –Finance and Administration) and Mr. A. K. Sharma (Assistant Manager).
The team would like to convey our gratitude to everyone that we met for their hospitality andthe tremendous spirit of partnership encountered during our visit to Bihar. The warm welcomeand the time that all stakeholders devoted to meetings with the team were greatly appreciated.


I Health Status
1. Bihar is the poorest state in India and has some of the worst health indicators.1 Thetable below presents data by state on the major health indicators targeted for improvementby the Millennium Development Goals (MDGs). Despite its low per capita income andhigh rates of poverty, the state still boasts an IMR and MMR that are close to all-Indiaaverages.
2. Female socio-economic development indicators are particularly poor. Bihar has theworst performance of any Indian state in terms of female literacy (33.0 percent), and thepercentage of female household population aged 6-17 years attending school (54 percent).More than 63 percent of women suffer from Anemia. The sex ratio is 921 females per 1,000males compared to the Indian average of 933.2
3. Poor female health and education results in poor reproductive and child healthoutcomes. Bihar has the lowest contraceptive prevalence rate (24.5 percent) and knowledgeabout HIV/Aids among ever married women (12 percent). Moreover, 58 percent of womenare married before they reach 18 years, compared to the Indian average of 37 percent. Only6.4 percent of women received a full package of ante-natal care and only 14.6 percent ofbirths are institutional.
1 Although this report has been prepared for Bihar, many of the statistics included in the report pre-date the state’s division into thestates of Bihar and Jharkand which took place in 2000. As Jharkand was home to several industries and on balance wealthier than therest of Bihar, the combined averages would tend to understate the current health challenges in Bihar.
2 2001 Population Census, provisional results.
Table 1.1 : Key Health Indicators, Bihar and Selected States
Income Poverty IMR MMR Immunized Malnutrition(Rs per capita Headcount (per (per (% fully (weight forcurrent Ratio- 1,000) 100,000) immunized) age)2001/02) (1999/00)
All India 20,198 26.1 67.6 453 53.3 45.5
Bihar* 6,006 42.6 72.9 452 11.18 54.3
Orissa 11,093 47.2 90 367 44.0 54.1
Uttar Pradesh 12,038 33.0 82 707 44.0 51.7
Punjab 29,973 6.2 57.1 369 72.1 39.2
Marahastra 29,873 25.0 43.78 336 78.4 39.9
Kerala 26,603 12.7 16.3 87 79.7 21.9
Tamil Nadu 23,414 21.1 48.2 376 88.8 29.4
Karnataka 22.816 20.0 51.5 450 60.0 36.6
West Bengal 20,039 27.0 48.7 389 43.8 41.5
Andhra Pradesh 20,112 15.8 65.8 436 59.0 38.6
Source: State GNP and poverty count: Punjab Economic Report; IMR, U5M, % children stunted: NFHS-2, 1998/99;MMR, The progress of Indian states, UNICEF, 1995.
* Includes Jharkhand.
1

Bihar: A Rapid Private Health Sector Assessment
4. Bihar’s primary health care system is dysfunctional and poorly utilized. Figure 1.1illustrates that Bihar lags every other state in India on crucial RCH indicators that trackhealth system utilization; the percentage of children that are fully immunized andthe percentage of institutional deliveries. It is disappointing to note that the currentrate of children who are fully immunized has dropped from a high of 90 percent in 1990to just 11 percent.
Figure 1.1 : Selected Indian States, Immunizations and Institutional Births
Source: NFHS-2 1998/9
5. Communicable diseases are also a major public health issue. Although accurate burdenof disease information is not available, it is clear that given Bihar’s level of developmenttackling communicable diseases is an immediate priority for government. The table belowindicates some of the major diseases detected recently.
6. Particularly worrying is the high rate of HIV infection detected from a sample12,262 pregnantwomen tested between March 2002 and April 2003. Bihar accounted for 203 of 213 reporteddeaths nation-wide from Kala-Azar in 2001. Bihar is also home to almost one-third of all
Table 1.2 : Bihar, Status of Health Programs, 2002-2003
Disease Number of Cases
Filaria 411,076
T.B. 53,804
Kala-Azar (Leishmaniasis) 101,129
Malaria 3,683
Leprosy 38,588
HIV/ Aids 11.5%
Source: Bihar State Health Profile at a Glance, 2003. Dr. Vishwa Ratan
2

Filaria diseased persons in India. Malaria is particularly endemic to tribal areas, althoughthe tribes account for less than 8 percent of the total, they contribute 82 percent of malariain the state. Preliminary data for 2003 indicates that with 15,634 new cases of leprosydetected in 2003, Bihar accounts for more new cases of leprosy than another state in Indiaand almost a quarter of all newly detected infections.3
7. Bihar’s health outcomes are also challenged by inadequate infrastructure. Only 18.2percent of households have access to electricity, less than 17 percent have access to adequatesanitation and more than one quarter of households do not have access to clean water. Suchdesperate living conditions, accompanied by a breakdown in governance and high levels ofviolence and banditry have forced most International Financial Institutions and bi-lateraldonors out of the state which has in turn compounded Bihar’s problems.
8. Improvement in Bihar’s health performance is a key to improved Indian and worldaverages. Despite its problems and the continued failure of governance, Bihar remainshome to approximately 1 in 12 Indians. After the bifurcation of the state, Bihar has gonefrom being the most populous state to number three following Uttar Pradesh and Maharasthra.Given the huge population and the extent of poverty and disease, improvement in healthoutcomes in the state is vital to achieving the MDGs.
3 Ministry of Health and Family Welfare, Government of India 1999.
3

Bihar: A Rapid Private Health Sector Assessment
II Delivery System and Health Seeking Behavior
Delivery System
Government Health Facilities
9. The number of Government health facilities in Bihar falls far short of national norms.Publicly provided primary and secondary level care in Bihar as in other Indian states relieson a network of primary health centers (PHCs) and community health centers (CHCs).Bihar has 396 PHCs and 101 CHCs which means that each PHC caters for more than 200,000patients while each CHC caters for more than 800,000. These figures should be comparedto national targets to have one PHC cater for a population of 30,000 and one CHC to caterfor a population of 100,000. It is reported that there are 15,426 beds in Bihar in both thepublic and private sectors less than one bed per 5,000 population. Table 2.1 below presentscurrent data on public health facilities in Bihar.
10. The number of health workers falls far short of national norms. There are 2,992 registereddoctors in Bihar or about 1 per 28,000 of the population compared to the national average ofone per 2,100. These disparities are repeated for all other types of health worker. In theoryeach PHC in Bihar is staffed with between two and four doctors. In practice, doctors rarelyshow up, especially in the rural areas. The government salary, although described as“reasonable” by government officials is only a third of what doctors could earn in the privatesector. It is clear that the PHC could be managed with a single dedicated doctor rather thanfour absentee doctors. It would also make it easier to hold them accountable.
11. The quality of government health infrastructure is shocking. Our site visits to variousPHCs and sub-centers in Bihar revealed that they are nothing more than dilapidated oldbuildings devoid of even the most basic medical equipment. PHCs are in theory meant to besix bedded facilities. Even our announced site visits revealed that not only do many of thePHCs not have any beds they are completely dysfunctional. Most PHCs do not even havepaper on which to write a prescription let alone any medical supplies, equipment, beds andother facilities (see table 2.2).
Table 2.1 : Bihar, Government Health Infrastructure 2002.
Facility Bihar No. of Facilities Bihar Population Covered Indian average
Sub Center 10,332 8,033 5,401
Additional PHC 1,247 66,560
PHC 396 209,596 32,169
CHC 101 821,782 243,729
Hospitals & Med. Col1 53
Other2 140
Source: Department of Health, Government of Bihar.1 Includes sub-division and district hospitals.2 Includes TB centers, blood banks, filarial and leprosy centers and other facilities.
4

12. Primary health care centers are ill-equipped and poorly utilized. The National FamilyHealth Survey confirmed the unacceptable state of Bihar’s primary health facilities. Lessthan a third of PHCs have electricity and more than a third have no running water. Only 1percent have an operating theatre and only 15 percent have a labor room, while more thanhalf of these had no normal delivery kit. Each PHC is supposed to have a female worker butonly 6 percent do so. Given these statistics it is not surprising that primary health care isunder utilized and outcomes are among the worst in the country with less than 11 percent ofchildren fully immunized and government facilities accounting for less than 3 percent oftotal deliveries.
13. A 1999 study, showed that on average, only 27 patients attended a PHC per day. This lowutilization could explain why few of the respondents knew the causes of common diseases,such as diarrhea and TB, something that would have been provided by the PHC staff ifmore contact was made with the people4.
14. Reproductive and child health outcomes have suffered. Bihar’s dismal health indicatorsreflect the meager utilization of public health facilities by the majority of the population forboth preventive and curative care. It also highlights the need for the government to seriouslyconsider alternative means of delivering primary health care goods and services to satisfydemand, such as the estimated 40% unmet needs for family planning commodities andservices.6
4 Dr. Mahabir Das. Status of Health in Bihar, May 1999.5 Most of the listed equipment are basic for ANC and safe delivery.6 Janani Social Marketing Project
Table 2.2 : Staff and Facilities Survey5
No. of Bihar PHCs surveyed (339) Number Percent
With Female staff (All HA) 20 6%
With BP instruments 136 40%
With water 210 62%
With electricity 105 31%
With labor room 51 15%
With labor room equipment 102 30%
With normal delivery kit 27 8%
With auto clave/sterilizer 146 43%
With working vehicle 92 27%
With operation theater 2 1%
With mounted lamp 3 1%
With generator 1 0.3%
Supplies
With oral pills 41 12%
With IUD insertion kit 14 4%
With measles vaccines 41 12%Source: National Family Health Survey II, 1998-99
5

Bihar: A Rapid Private Health Sector Assessment
Private Health Facilities
15. There is little current information available on private health facilities in Bihar.Government has little to do with the private sector and no recent attempts have beenmade to survey the private formal or informal sectors. However, we know that theprivate sector is the dominant force in health care provision both for outpatient and in-patient services (see following section).
16. During site visits to Patna and the neighboring districts, we saw a number of privatehealth clinics clustered by main roads in secondary towns, most of which cater tomaternal and child health. Patna is home to a number of impressive private for profitand voluntary facilities. Such facilities have moved in to the fill the vacuum left by anon-performing public sector (see below).
17. As in other states informal providers both registered and unregistered and both qualifiedand unqualified are the predominant source of health care for those in both urban andrural areas. In many rural areas, these “quacks” represent the only source of healthcare. As one stakeholder puts it, “Where health is not provided by doctors, villagersthemselves must take control”. Many of them practice alternative systems of medicine.Bihar has the highest number of non-allopathic providers in the country, a total of160,0007 as of January 2000.
18. More and more NGOs engaged in rural or community development or micro enterprisesare integrating health in their portfolio of services. Some do it through health promotion,others through organizing community based health funds from which villagers couldtake a loan for hospitalization. One NGO, the ADITHI, works with 600 Self Help Groups(SHG) that have successfully delivered integrated health and education programs.
19. In conclusion, the gap between demand and supply has been filled by various privateproviders, who are seen to be either better or in many cases the only alternative to thepublic health facilities. They include a range of providers such as informal unqualifiedproviders, Traditional Birth Attendants (TBAs), faith healers, pharmacists or pharmacyassistants in medicine shops (for self-medication), qualified physicians8, NGO clinicsand for-profit nursing homes and hospitals. It is important to understand that the privatesector does not represent a homogenous group.
Health Seeking Behavior
Factors That Influence Health Seeking Behavior
20. The health-seeking behavior of the people of Bihar is largely determined by many
7 This figure from the MOH Annual Report of 2001-2002 was prior to the creation of the new province of Jharkand.
8 In Bihar, doctors who are employed by the government are allowed to hold private practice after office hours.
Table 2.3 : Bihar, Selected Primary Health Care Indicators
% of % Institutional % Safe % Full % FP % FPMothers Delivery Delivery Immunization Sterilization SpacingReceived ANC methods
India 65.3 33.6 42.3 58.7 36.0 8.3
Bihar 36.0 14.6 23.3 11.0 57.0 1.8
Source: National Family Health Survey II, 1998-99
6
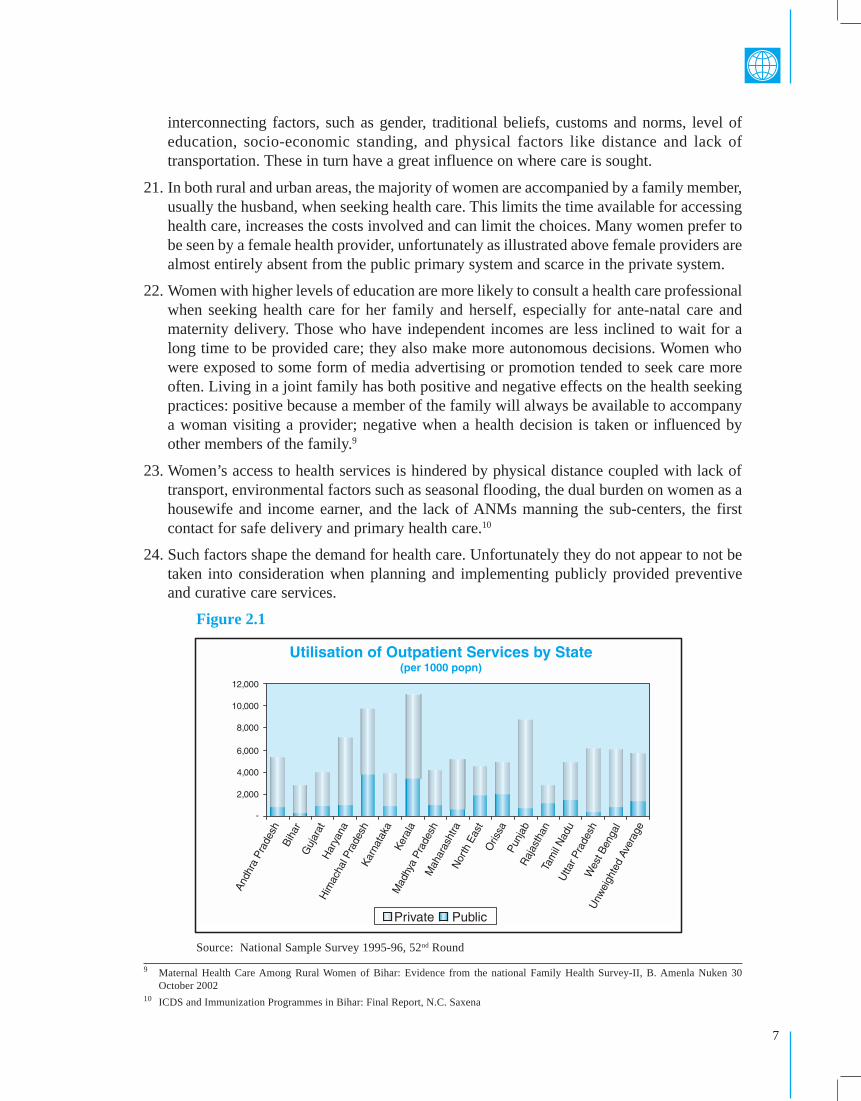
interconnecting factors, such as gender, traditional beliefs, customs and norms, level ofeducation, socio-economic standing, and physical factors like distance and lack oftransportation. These in turn have a great influence on where care is sought.
21. In both rural and urban areas, the majority of women are accompanied by a family member,usually the husband, when seeking health care. This limits the time available for accessinghealth care, increases the costs involved and can limit the choices. Many women prefer tobe seen by a female health provider, unfortunately as illustrated above female providers arealmost entirely absent from the public primary system and scarce in the private system.
22. Women with higher levels of education are more likely to consult a health care professionalwhen seeking health care for her family and herself, especially for ante-natal care andmaternity delivery. Those who have independent incomes are less inclined to wait for along time to be provided care; they also make more autonomous decisions. Women whowere exposed to some form of media advertising or promotion tended to seek care moreoften. Living in a joint family has both positive and negative effects on the health seekingpractices: positive because a member of the family will always be available to accompanya woman visiting a provider; negative when a health decision is taken or influenced byother members of the family.9
23. Women’s access to health services is hindered by physical distance coupled with lack oftransport, environmental factors such as seasonal flooding, the dual burden on women as ahousewife and income earner, and the lack of ANMs manning the sub-centers, the firstcontact for safe delivery and primary health care.10
24. Such factors shape the demand for health care. Unfortunately they do not appear to not betaken into consideration when planning and implementing publicly provided preventiveand curative care services.
Figure 2.1
Source: National Sample Survey 1995-96, 52nd Round
9 Maternal Health Care Among Rural Women of Bihar: Evidence from the national Family Health Survey-II, B. Amenla Nuken 30October 2002
10 ICDS and Immunization Programmes in Bihar: Final Report, N.C. Saxena
7

Bihar: A Rapid Private Health Sector Assessment
Demand For Private Providers
25. The private sector provides the vast majority of health care services in Bihar. NSS datafrom 1995/6 shows that residents of Bihar depend on the private sector almost entirely forin-patient and outpatient services (see Figure 2.1).
26. The poor use the private sector despite its cost. Although Bihar has a BPL population of42.6 percent11, the poor depend on private providers for their medical needs. When the poorare hospitalized, three-quarters of them go to private hospitals (see Figure 2.2). The reasonscited by the respondents to the NFHS II for this choice were as follows:
� Non-availability of doctors or no staff in time of need;
� Indifferent and bad behavior of staff;
� Inaccessibility due to distance;
� Belief that drugs provided were substandard and ineffective;
� Experienced charging of illegal fees for services that were supposed to be for free;
� Not aware of the range of services provided by the PHC.
27. High private health care costs can push the poor into poverty. As a result of inadequatepublic health facilities, Bihar leads the nation in terms of private health care delivery forboth inpatient and outpatient services. This is despite the fact that most of these patients donot have the means to make out-of-pocket payments for private health services except at thecost of other essential items such as basic nutrition. Studies at the national level haveillustrated that hospitalizations often result in patients and their families dropping belowthe poverty line.
Figure 2.2
Source: National Sample Survey 52nd Round
11 National Health Policy 2002
8

Affordability, Accessibility and Quality of Care
28. When it comes to health care in Bihar, affordability is not a major issue. Anecdotesrecount that Biharis care about three things in life; marriage, health, and education.Several surveys have confirmed that, despite high levels of poverty, Biharis are willingto pay for access.
29. Access refers not only to proximity to facilities, but also access to a female provider,flexible hours, availability of doctors, service on demand and availability of good qualitymedicines. Bihar scores poorly on all these aspects.
30. Given the well-known asymmetry of information involved in healthcare provision, theconcept of quality health care is difficult for patients to gauge. There is clear evidencehowever, that patients are deterred from visiting public facilities by the unwelcomingattitude of government staff.
Initial Observations on Delivery Systems and Health-seeking Behaviors
(i) Improving management and stewardship: Bihar’s health infrastructure is inadequateto meet current health care challenges. However, simply building more facilities willnot improve outcomes unless management reforms are also introduced (see Box 2.2).In a state in which more than 90 percent of outpatient care takes place in the privatesector, government can not expect to improve outcomes without improving stewardshipover the whole sector i.e. including the public and private spheres.
(ii) Strengthening the sub-centers: The sub-centers, are the first contact point forpreventive and curative care in a village. In the absence of effective management,supervision, infrastructure and equipment, sub-centers are not delivering the carethat is required of them. There are claims that sub-centers are either unmanned orthat ANMs are absent for long periods. This leaves many villagers with little optionbut to go to “quacks” or untrained providers that could contribute to the worsening ofan illness.
Box 2.1: Making a Choice: Paying for Private Health Care
Mr. Naseem works as a migrant laborer in Patna. His wife and child used to live with hismother in a village 35 km away from the city. In early January, he brought his family tolive with him in Patna. On January 21, 2004, he and his wife came to the Kurji HolyFamily Hospital Community Health Center to have his son immunized. Although he hadto pay a small fee for the shots, Naseem said that he did not mind that because he hadbeen told by his neighbors that Kurji Hospital staff would give his child proper attentionand good service. When asked if he knew of a nearby PHC where he could get freeimmunization, he answered in the affirmative, but claimed that the government healthstaff would not be able to give his child better care.
Source: Authors’ site visit.
9

Bihar: A Rapid Private Health Sector Assessment
ANMs are relatively well-paid for the level of their training and experience. Otherstate governments have shown that it is possible to recruit and deploy contract ANMsfor far lower rates than they are currently paid by government. The main reasons thatANMs are not available is a lack of supervision. Often the Medical Officerresponsible for overseeing their work is also unavailable. Many ANMs complainthat there is not enough equipment and supplies or transport to allow them to dotheir jobs effectively.
(iii) Informal providers: Although untrained, the informal providers are trusted by manynot for necessarily for their healing skills but because they are there when neededand offer an affordable and courteous service. An informal provider who lives at hisplace of practice, as many do, is available 24 hours a day, seven days a week. Theyaccept cash or in kind payment for services rendered and often offer credit for thosewho cannot afford to pay on delivery of service. It is not common for villagers tochoose to continue going to the informal providers even if an ANM is around.
Government can consider methods to co-opt these informal providers, primarily forthe trust that they have with villagers. They could be utilized for health promotionand even the provision of simple services. The Janani model has shown that this canbe achieved relatively quickly and with impressive results. What remains morechallenging is how to stop such informal providers from practicing “quackery”. Themost promising method is probably a combination of carrot and stick, providing thosethat are willing and able with additional training and skills (similar to barefoot doctorsin China) and shutting down those that continue to ply their harmful trades. Asimultaneous effort to educate the public as to their potentially harmful effects couldalso pay dividends.
(iv) SHGs: Since almost 90 percent of the population resides in the rural areas, SHGscould be a suitable vehicle for selected health services, including the distribution offamily planning commodities like pills and condoms, and mobilization forimmunization, with the ANM providing the services. Members of the communitywho can read and write could be trained as volunteer health workers, so simpleactivities like measuring blood pressure, weighing and first aid could be made availablequickly and safely to the community. SHGs can also play a role in establishingsimplified community based health funds or pre-paid services patterned after amanaged care model.
(v) Contracting out primary health care: In general, community participation remainsa key, yet elusive, factor to sustain health efforts. Governments have tended to ignorethe power of community mobilization and are happy to let NGOs take a lead in thisarea. Contracting out primary health care services to NGOs and for-profit providersis one potential way of encouraging an integrated system of community-based primaryhealth care. If government can devise an appropriate system of payment for contractedservices that focused on outcomes rather than inputs, the private sector could developappropriate health delivery systems tailored to local needs.
10

Box 2.2 : Death of a Hospital
The Bihar Karpoor Thakur Referral Hospital (KTRH) began construction in August 1991.By January 1994, the hospital was inaugurated at an estimated cost of Rs50 million. The30-bed hospital included several specialist departments and catered to a population of70,000, many of whom were rural poor.
Within two months the hospital ceased operations. No one knows all the reasons why thehospital was shut down but observers suggest it was due to poor management and lack ofresponsibility and accountability that led to a situation in which the newly constructedhospital was not provided with an adequate budget and the state never sanctioned separateposts for the hospital. Government officials blame doctor apathy claiming that doctorswere not induced to stay at the block. Several attempts were made in the late 1990s toreopen the facility. All were in vain. It appeared as one politician put it, that the hospitalwas “an orphan or illegitimate child” – there was no one to protect or nurture it.
The buildings fell into disrepair and are now being used to store animal fodder and rearcattle. All the windows, gates, electrical wiring, basins and other moveable equipmenthave long since been looted from the site which now resembles a ghost town.
Spending more money on facilities in such a context is unlikely to improve healthoutcomes.
Source: Hindustan Times January 24, 2004
11

Bihar: A Rapid Private Health Sector Assessment
III Health Care Financing and Insurance
Health Care Financing
Government Spending on Health Care
31. Bihar’s spending on health care is inadequate in the face of significant public healthchallenges. Bihar’s state budget for health for 2003/4 is Rs7.3 billion or approximately 3.5percent of total state spending. This amounts to about Rs88 (US$2) per person per year. Inaddition to the state budget, Bihar receives money from the central government for thecentrally sponsored programs and funding from the Employees State Insurance Scheme.
32. Donor agencies are not funding health care interventions through the state budget.Despite the size of the health care challenge, the state government has not attracted anydonor funding for the sector. Total donor funding channeled through the Bihar state budgetaccounts for just 0.02 percent of total spending. However, donor organizations and donor-funded NGOs are active in the state, an indication that external agencies perceive that theirresources would be better spent outside the government sector.
Out of Pocket Expenditures
33. As indicated above, most health care is provided by the private sector and funded byout-of-pocket expenditures. In India 83 percent of out-of-pocket expenditures are spenton private services. In Bihar this ratio is over 90 percent, indicating Bihar’s heavy dependenceon the private sector. Out of pocket expenditures (OOP) pay for almost all privately providedhealth care as private insurance has yet to take off throughout India and especially in Bihar.OOP is also used to access care from government secondary and tertiary facilities, andfinance supplemental purchases when using PHCs.
Figure 3.1 : Sources of Health Care Financing
Source: NSS 1995/6 and Department of Finance Bihar.
12

34. The majority of out-of-pocket expenditures are spent in the private sector. However, alook at where out-of-pocket expenditures are going can be misleading as public facilitiescharge much lower fees than private facilities and provide a number of services free ofcharge. Therefore including state expenditures gives a fairer picture of the sources of healthcare spending (see figure 3.1).12 Even those below the poverty line spend a high proportionof their out of pocket expenditures on private health care (77 percent) and a higher proportionof their income on private sector services than non-poor households.13
35. In the rural areas, people who go to alternative private providers (APP), such as TBAs orquacks, pay either in cash or in kind or a combination of both. Many of the so called quacksalso extend credit to their patients. A TBA is usually paid a mixture of cash and kind. It istraditional in Bihar to present a TBA with a sari and sometimes a small payment for a homedelivery. However, many poor families resort to selling their assets or use them as collateralfor loans to pay for hospitalization. This can often result in long term indebtedness andplaces BPL families under tremendous financial pressure.14
36. For the rural poor, this financing method automatically limits their choices for care. Withhard-to-come by cash and limited goods that could be bartered in exchange for care, theonly available option to them is the informal provider, whose credentials may be suspectand who engages in the most part in dubious curative care. In the absence of a regularlyfunctioning sub-center, and a PHC with very limited services, many cannot take advantageof primary health care. Thus, the rural poor have the double burden of paying for their owncare that they can hardly afford and lacking access to life saving and more cost-effectivepreventive health services that could help avert the need for curative care.
Community-based General Savings Funds
37. General savings funds are only available to members of self help groups (SHG). A SHG isa community group, numbering between 10-20, residing in a single village that have bandedtogether for economic or developmental reasons, for example to create a pool of resourcesfor credit, developing skills for production, and marketing its produce.15 SHGs are oftentargeted to empowering the most marginalized members of the community such as womenand BPL households. SHGs often create a mandatory general savings fund to which memberscontribute an agreed upon sum of money that is usually paid daily or weekly. Members canborrow from the fund for various purposes, including payment for hospitalization, which isthe most common health-related loan. The general savings fund is providing SHG memberswith possibly the only inexpensive source of credit to pay for health care expenses. Theloan is repaid in equal installments within a specified period of time and at a specifiedinterest rate. Repayment is often at 99 percent or more due to the pressure exerted on theborrower by the other members.
38. Although many NGOs have organized SHGs, the number remains very small in relation tothe total population. ADITHI, a Bihar-based NGO, estimated that less than 2% of thepopulation are members of SHGs. Given the time and effort involved in establishing SHGsit is not clear whether this is a viable model for scaling up across the state. For instance, the
12 Note that this does not represent total health care spending as it omits the centrally sponsored schemes, ESI spending and health carefunded by private insurance, although the later is negligible.
13 NSS 1995/6.14 Financing Primary Health Care, Sujatha Rao, et al, September 1997.15 ADITHI: 15 Years in the Field of Women Empowerment
13

Bihar: A Rapid Private Health Sector Assessment
Community Health Centers run by the Kurji Holy Family Hospital have successfullyorganized only 88 SHGs or about 1,500 individuals within an estimated target populationof 450,000 in its 2 sites.
Costs of Health Care by Type of Provider
39. There are two major costs of health care, direct and indirect. The direct costs of healthcare include; the fee charged by the provider for consultations, the cost of medicationand consumables, the charges for investigation and diagnostics, and the price of roomand board for a hospital stay. The indirect costs include transportation, the costsassociated with a traveling companion, lost income, costs of childcare or care for theaged. Both the direct and the indirect costs that can often influence the decision onwhether, from whom and when to seek health care. This section addresses focuses onthe direct costs.
40. It is important to note that government secondary and tertiary facilities charge fees forservices and hospitalization, although at a lower rate than private providers. Although PHCsare supposed to offer free services including; consultation, minor surgeries, deliveries, minorlab work, and medication, anecdotal reports suggest that patients are forced either to makeinformal payments for access or that more often than not, consumables and medicines,even basic laboratory agents are not available, thus, patients end up purchasing them usingtheir own funds or going to a private provider.
Box 3.1 Building a Savings Fund for Self Help Groups
The Kurji Holy Family Hospital is a missionary-run facility operating in Patna since 1939.This 300-bed secondary general hospital provides general and specialty services. As part ofits mission to help provide equal access to quality health care for all, it established two (2)community health centers (CHC). One is located within the hospital compound to give careto poor residents living in the surrounding slum communities within 10 km from Kurji; theother is located in Maner Block, a rural district. Immunization, ante-natal care, baby weighing,family planning counseling and commodities distribution, and health education classes areprovided for a Rs 10 initial registration fee. Consultations for minor illnesses are also availablefor Rs 10 for initial registration and Rs 5 for subsequent visits. Vaccines and commodities aresupplied by the government.
To complement its health services, each CHC organizes women-only self help groups (SHG).In the CHC in Patna, 8 SHGs have been organized in a slum area where about 150,000people reside. Each SHG created an all purpose savings fund from fixed contributions of itsmembers. Loans can be made from the fund for various purposes, such as micro-credit forsmall businesses and for health expenses.
The SHG in Batta B is called “Bajrang”. It has 10 members, which is typical for an SHG. Themembership agreed to contribute Rs 50.00 per month per member. From these contributions,it has loaned out a total of Rs. 10,500 to its members. It generates additional income frominterest on loans, bank interest, and fines imposed on members for infractions. As of January16, it has a total bank deposit of Rs. 9,835.
14
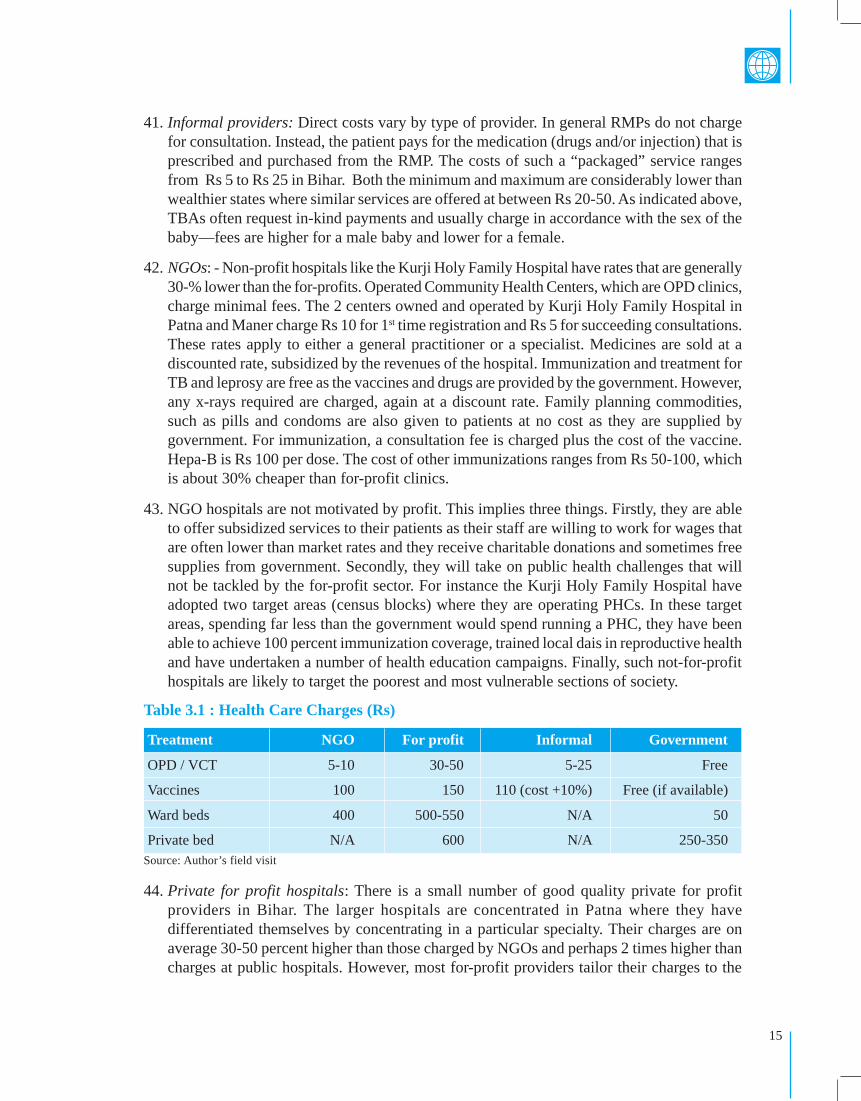
41. Informal providers: Direct costs vary by type of provider. In general RMPs do not chargefor consultation. Instead, the patient pays for the medication (drugs and/or injection) that isprescribed and purchased from the RMP. The costs of such a “packaged” service rangesfrom Rs 5 to Rs 25 in Bihar. Both the minimum and maximum are considerably lower thanwealthier states where similar services are offered at between Rs 20-50. As indicated above,TBAs often request in-kind payments and usually charge in accordance with the sex of thebaby—fees are higher for a male baby and lower for a female.
42. NGOs: - Non-profit hospitals like the Kurji Holy Family Hospital have rates that are generally30-% lower than the for-profits. Operated Community Health Centers, which are OPD clinics,charge minimal fees. The 2 centers owned and operated by Kurji Holy Family Hospital inPatna and Maner charge Rs 10 for 1st time registration and Rs 5 for succeeding consultations.These rates apply to either a general practitioner or a specialist. Medicines are sold at adiscounted rate, subsidized by the revenues of the hospital. Immunization and treatment forTB and leprosy are free as the vaccines and drugs are provided by the government. However,any x-rays required are charged, again at a discount rate. Family planning commodities,such as pills and condoms are also given to patients at no cost as they are supplied bygovernment. For immunization, a consultation fee is charged plus the cost of the vaccine.Hepa-B is Rs 100 per dose. The cost of other immunizations ranges from Rs 50-100, whichis about 30% cheaper than for-profit clinics.
43. NGO hospitals are not motivated by profit. This implies three things. Firstly, they are ableto offer subsidized services to their patients as their staff are willing to work for wages thatare often lower than market rates and they receive charitable donations and sometimes freesupplies from government. Secondly, they will take on public health challenges that willnot be tackled by the for-profit sector. For instance the Kurji Holy Family Hospital haveadopted two target areas (census blocks) where they are operating PHCs. In these targetareas, spending far less than the government would spend running a PHC, they have beenable to achieve 100 percent immunization coverage, trained local dais in reproductive healthand have undertaken a number of health education campaigns. Finally, such not-for-profithospitals are likely to target the poorest and most vulnerable sections of society.
44. Private for profit hospitals: There is a small number of good quality private for profitproviders in Bihar. The larger hospitals are concentrated in Patna where they havedifferentiated themselves by concentrating in a particular specialty. Their charges are onaverage 30-50 percent higher than those charged by NGOs and perhaps 2 times higher thancharges at public hospitals. However, most for-profit providers tailor their charges to the
Table 3.1 : Health Care Charges (Rs)
Treatment NGO For profit Informal Government
OPD / VCT 5-10 30-50 5-25 Free
Vaccines 100 150 110 (cost +10%) Free (if available)
Ward beds 400 500-550 N/A 50
Private bed N/A 600 N/A 250-350Source: Author’s field visit
15

Bihar: A Rapid Private Health Sector Assessment
patient’s ability to pay and most state that they are often willing to write-off charges altogetherfor BPL households.
45. Many of the large for-profit hospitals have been established by returning non-resident Indians(NRIs). All such NRIs could enjoy a higher standard of living overseas and have returned toestablish hospitals to provide services that otherwise would not be available in the state.Although they are established as for-profit entities, health care providers have a very differentrelationship with their clients than other economic sectors and have objectives other thansimply making money. All for-profit hospitals are interested in making a percentage of theirbeds and facilities available to the very poor at no charge and would look to cross subsidizethese services from profits made from richer patients. At the moment, with little competitionin the local market they are able to operate profitably on this model.
46. Government hospitals: The Indira Gandhi Institute of Medical Science, a tertiary referralhospital, charges fees for all services at a graduated scale. For instance, for the same surgery,poorer are charged Rs 2,000, while a private room patient is charged Rs 3,500. The poorestof the poor are reportedly not charged at all. The institute has 600 beds of which 62 aresingle rooms with attached baths. The best equipped rooms also have A/C and are providedat about half the rates offered by the private sector. However, private room patients are alsocharged double for all other services, including diagnostics, related to the procedure. Thehospital also runs a rest house where accompanying family members can stay from Rs25per night. Hospital management plans to attract a mixture of clients composed approximatelyof 50 percent of poor, 35 percent middle income and 15 percent high income.
47. Social franchising: Janani Franchisees16 have set fees for its franchised services andcommodities. At a Surya Clinic, the price of a pregnancy test is Rs. 50 and for naturaldelivery, Rs 699. The Surya Clinics have recruited doctors that were already practicing inthe private sector. After joining Janani, they have lowered their fees by 10-20 percent forthe majority of services offered. However, the doctors report that the franchise fee thatcovers the cost of marketing (through radio, roadside billboards etc.) brings an increasedvolume that more than makes up for the shortfall in per patient charges (see later for moredetails).
Health Insurance17
48. There are several types of health insurance institutions operating in the state. The two largestare the Employee State Insurance or ESI, the mandatory insurance for employees and workersin the business sector with at least 10 employees and earning less that Rs 6,500 a month andgovernment employees, and the Central Government Health System (CGHS), which coversonly central government employees assigned to the state. There is also a number of privateinsurance schemes offered by government and private insurance companies and, the recentlylaunched government Universal Health Insurance Scheme.
Private Health Insurance
49. Private health insurance in Bihar has been outsourced to about 10 Third Party Administrators(TPAs) who act as both back room administrators under contract with an insurance companyand brokers. The health plans they market and administer are mostly those developed andissued by the four government-owned insurance corporations. The rest are private plans
16 Janani’s franchising scheme is a variation, as it franchises only a set of services or some commodities. This is not the commonpractice in a franchise.
17 Detailed description of health insurance schemes can be found in the
16

from private insurance joint ventures. All the schemes cover general hospitalization, with afew for critical illnesses only. Many are bundled with accidental death and/or dismembermentcover. In almost all instances, the plans are co-branded by the TPA and the insurer, with theTPA issuing its own ID card to enrolled members. Since TPAs are generally located in theurban centers, it can be assumed that almost all of the policies are sold to wealthier clients.
50. Interviews with private doctors, hospital owners and business associations, indicate thatthis type of health insurance has not taken off due to a high number of fraudulent claims. Italso appears that such health insurance is being marketed to those that easily afford to payfor private hospitalization should they need it and therefore there remains little demand forsuch products.
51. However, some private hospitals have signed up with TPAs. One example Dr. Ruben SinghMemorial Hospital whose director reports that about 5 percent of all in-patients treated athis hospital are covered by health insurance. He also estimates that the average reimbursementfor treatment takes about three weeks.
52. Other hospitals are wary of entering into agreement with TPAs. The Hai Medical and ResearchInstitute allege that reimbursement for hospital services rendered is fraught with delays anduncertainty. All private hospital owners and operators realize that once the market developsmore and more patients will be covered by a health insurance policy. However, at the moment,many are taking a wait and see attitude.
Universal Health Insurance Scheme
53. In August 2003, the Government of India launched a Universal Health Insurance Scheme(UHIS). The plan costs just Rs 1 per day and was developed essentially as a hospitalizationplan with added benefits related to accidental death and disability. It is being marketednationwide by the government-owned insurance corporations, focusing on the low incomegroup, either individuals or families. For families living below the poverty line, thegovernment pays a subsidy of Rs 100 towards the premium.
54. In Bihar, take up of the scheme has been slow for a number of reasons.
(i) Government insurance corporations realize that the scheme is not financially viableand are not eager to market the scheme.
(ii) Although even poor families can reportedly afford Rs1 per day, they are not ableto raise the required Rs365 in one installment.
(iii) The costs of marketing the scheme individually are extremely high and thereforethe insurance corporations have adopted a strategy of marketing the plan throughNGOs and selling a minimum of 100 individual policies in a group format. Thisstrategy has not yet taken off (see below).
55. The tie-up calls for Janani to act as a broker, marketing the UHIS to the rural areas where ithas a presence. Ten Super Titli Centers will coordinate its marketing through the network ofTitli Centers under each. The commission paid by Oriental Insurance will be split betweenthe Titli Center and the Super Titli Center. Janani is also about to finalize a plan to becomea TPA, using its new Surya Clinics as first-line providers for UHIS policy holders by offeringa “guaranteed cashless transaction” to them.
17

Bihar: A Rapid Private Health Sector Assessment
IV Key Private Sector Issues
Introduction
56. Given the situation analysis outlined in the preceding chapters, the government of Biharfaces a challenge in addressing and improving primary health care services. There are threepossible ways of achieving this desired result that need not be mutually exclusive;
� Improve public sector delivery� Contract for primary health care with the private sector� Establish public private partnerships
57. The first option is beyond the scope of this paper. Contracting for health care services iscovered elsewhere and therefore this section focuses only on the pros and cons of existingand potential public private partnerships in Bihar.
58. Given the lack of public health care services and the large number of NGOs and for profitproviders active in Bihar, the Department of Health has made successfully co-opted a numberof private sector organizations to expand access to vital primary health care. Some examplesare discussed below while the Janani model is presented in a separate chapter.
Public Private Partnerships
Partnering with a not-for-profit – the The Kurji Holy Family Hospital
59. The Kurji Holy Family Hospital is a missionary-run facility operating in Patna since 1939.This 300-bed secondary general hospital provides general and specialty services. Its feesfor both out-patient and in-patient care are generally lower than similar for-profit hospitals.As part of its mission to help provide equal access to quality health care for all, it hasembarked on the following activities:
� Partnering with government to; host and manage an HIV/AIDs Voluntary Counselingand Training Center (VCTC), a TB DOTS Center, a Leprosy detection and treatmentcenter. In each case, drugs and laboratory reagents are provided by the government.The VCTC also benefits from having two government-employed counselors.
� To complement its health services, the CHC also organized 88 women-only, self-help groups (SHG). Each SHG created an all purpose savings fund from fixedcontributions of its members. Loans can be made from the fund for various purposes,such as micro-credit for small businesses and for health expenses.
� Established two community health centers (CHC). One is located within the hospitalcompound to give care to poor residents living in the surrounding communities.Immunization, ante-natal care, baby weighing, family planning counseling andcommodities distribution, and health education classes are provided for a Rs 10initial registration fee. Consultations for minor illnesses are also available for Rs10 for initial registration and Rs 5 for subsequent visits. Vaccines and commoditiesare supplied by the government. It is interesting to note that the Kurji-run CHCs areable to achieve 100 percent immunization coverage and provide a full-set of ANC topregnant women in the target catchment area while operating on a budget that is smallerthan that of a government-run PHC (see Table 4.1 below).
18

Bihar Volunteer Health Association (BVHA)
60. The BVHA was established in1970 to bring together all the not-for-profit and missionary hospitalsinto a secular organization to coordinate the work of the voluntary health sector and collaboratewith government to avoid duplication and make use of government facilities and supplies.
61. In the 1970s, before the central government vaccination programs were operating, the BVHAcollected and stockpiled vaccines for use at 240 voluntary clinics and hospitals. They alsocoordinated their activities with 100 NGOs that were not members of the organization.
62. BVHA also undertook training programs for the voluntary sector bringing in internationalexpertise and funding. They brought together the 7 major not-for-profit hospitals who wouldeach take it in turn to host training events and thus learn from each others facilities and procedures.Like some of its members, BVHA received funding from religiously motivated donors.
63. BVHA’s current activities include support to Community-based Organizations, and supportto government programs including; Malaria, MCH, TB and HIV/AIDs. The IEC programincluding an anti-tobacco program is undertaken in partnership with Patna Medical Collegeand supported by WHO. BVHA also take part in flood relief work recognizing that naturaldisasters can exacerbate existing health issues and lead to epidemics.
Partnering with a for profit hospital
64. The Dr. Ruban Singh Memorial Hospital (RSMH) is a 28 bed tertiary facility that wasestablished in 1996 by returning non-resident Indians. This private hospital specializes inhi-tech kidney and urology treatments. However, hospital management report that about 80percent of patients come from the rural areas of Bihar. In general, they are attracted bythe doctor’s name and reputation rather than the facilities or equipment. This presents adifficulty for private sector managers wishing to invest in appropriate facilities andequipment. Like many private hospitals throughout India, RSMH has enough demandto make a profit and continue in operation but they still have a lot of additional unusedcapacity. Hospital management state that to attract rich patients, most private hospitalsoffer incentives to well-known doctors of the rich.
65. Although the hospital itself specializes in tertiary care, the hospital owner-managersare interested in furthering public health issues. In particular the hospital managementis concerned that there are few health care facilities available in the rural areas,neonatology and trauma continue to be especially weak. To further such aims, theyclaim that no patient is turned away because they cannot pay for treatment.
19
Table 4.1 : Selected Health Center Budgets (Rs)Kurji-run Facilities
Budget Items CHC Rural CHC Maner Public PHC
Staff Salaries 404,211 262,661 1548000
Doctors’ salary 72,000 45,200 960000
Drugs and Pharmacy 72,325 79,068 75000
Other supplies 25,295 54,714 74,185
Aids program 61,850 - -
TB/HIV 97,981 18,268 -
Health and Family welfare 137,700 271,353 -
Total 871,362 731,264 2,657,185Source: Kurji Holy-Family Hospital and Government of Bihar

Bihar: A Rapid Private Health Sector Assessment
66. The hospital management have also adopted an outreach project in 6 panchayats wherethey are taking on the immunization program and ensuring that all children in the targetgroup are fully immunized. Although this effort represents the limit of their financialability to cater for the poor, hospital management state that they are very interested inpartnering with government to run PHCs and other government facilities. Given theiroverseas exposure they also have a number of ideas on partnering that they havewitnessed in operation in the UK, US and elsewhere in India.
The Pros and Cons of Subsidized Services
67. Although all of these examples have been successful, they rely on the generosity of theprivate sector and are therefore limited in outreach and the potential for scale up. There isas yet no broad framework for incorporating the private sector into health care delivery.However, government officials are open to considering possible ideas and models forincreased participation for the private sector including public funding for private provision.
68. Subsidized preventive and primary health care services and commodities are oftenprovided by NGOs, Trusts or other institutions. As illustrated above, even for-profithealth care institutions acknowledge their public service functions and often providehealth care services on a charitable basis for BPL and other vulnerable groups. Althoughthe communities that enjoy such services certainly benefit from them, subsidized serviceshave their pros and cons.
69. Pros: Services and commodities may not always be available on demand in localcommunities. For example, in many rural areas, family planning commodities are notalways obtainable at the sub-center or the PHC. The ANMs who staff the sub-centersare reportedly not always present, have no supplies or transport. As seen above, mostPHCs in Bihar are not well equipped. Thus, NGOs who offer medical services and sellmedical supplies such as pills and condoms at a subsidized rate offer a unique benefitto the people. Institutions like hospitals that hold medical missions in poor communitiesprovide opportunities for people to access care that may not always be on hand at littleor no cost to the beneficiaries. In many instances, selected supplies, like vaccines, areprovided to such organizations by the government. Given that many of theseorganizations work in the most remote and vulnerable areas precisely where governmentservices are most lacking they fill a much needed niche.
70. Cons: The downsides of subsidized services and commodities are their sustainabilityand the potential for scale-up. NGOs that rely on donors or the government for theirfunding and supplies are subject to changes in government and donor policies. Areduction in funding and supplies would have a tremendously negative impact on thecontinuous flow of supplies to the poor or to rural residents, who could have becomedependent on those supplies. None of the not-for-profit institutions we met with had anannual budgeted program for medical services but were forced into ad hoc operations.
71. Subsidized services and commodities are generally palliative measures. Though theyserve a purpose, most are short-term and temporary in nature. This implies that theycannot play a useful role in government programs that require a constant surveillanceand delivery capability such as immunization and disease surveillance. Co-opting suchproven NGOs and charitable institutions and providing them with a government budgetbased on a performance contract seems to be a sensible way to expand governmentcapabilities and build on existing services.
20

V Options for Maximizing the Potential of the Private Sector
Key Health Care Challenges for Bihar
72. The preceding sections have highlighted the tremendous health care challenges thatBihar faces. Bihar is the poorest state in India and spends only US$2 per capita annuallyon health care. Low levels of spending in a system which is not focused on resultshave resulted in poor health outcomes especially for women and children. Morethan half the state’s children suffer from malnutrition, only 11 percent are fullyimmunized, while more than half receive no immunizations at all. Women marryvery young, on average before the age of 18. They are among the most poorly educatedin India with more than two-thirds illiterate and half the female population of schoolgoing age do not attend school.
73. Within such a context the first priority for government must be to improve primary healthcare outcomes with a specific focus on reproductive and child health. Given the poor situationof the primary health system, government should consider alternative methods of servicedelivery including involving the private sector.
74. This section presents some initial ideas for potential health reforms that involve the privatesector including;
� Improving the primary health care system,
� Engaging the private sector,
� Improving the performance of informal providers, and
� Private sector financing options
Improving the Primary Health Care System
75. The primary health care system, in Bihar, is almost entirely funded and provided by thepublic sector. The not-for-profit sector are involved but only at the margins of the healthcare system on an ad hoc basis. The for-profit private sector are interested in gettinginvolved but their activities are currently limited to small-scale charitable services.
76. Earlier sections have highlighted the weakness of the public primary health care deliverysystem including;
� Lack of adequate facilities especially PHC buildings
� Lack of equipment and supplies, especially reliable drugs.
� Lack of operations and maintenance budgets
� Absentee doctors at most public facilities
77. Although the state’s health budget is small in relation to the magnitude of the challenges itfaces, the real reason behind poor health outcomes in Bihar is poor management of publicsector services and poor stewardship of the whole health sector. Spending more moneywithin the current system, without introducing any reforms, is likely to be counterproductive.
21

Bihar: A Rapid Private Health Sector Assessment
What is needed, in such an environment, is improved management and oversight of thewhole system, the introduction of a performance culture and the measurement andaccountability for inputs, outputs and outcomes.
78. A few other states have been successful in introducing such reforms. A good example arethe secondary health care reforms introduced in Punjab with the support of the World Bank.Unfortunately, there are many other states that have unsuccessfully attempted to introducehealth care reforms. Bihar faces a number of difficulties in introducing reforms to improvethe performance of the public sector. Firstly, government capacity in Bihar is extremelyweak and will take a long time to improve. It is not possible to improve the health systemwithout increased government capacity. Secondly, donor organizations are unwilling toprovide support to the system through the Bihar government as there is a widespread lackof confidence in the state’s governance.
79. Given this situation, Government should consider the potential of the private sector.Government officials have shown themselves open to consider various options availableand have indicated an interest in understanding successful, regional and international PPPmodels. Government is currently focused on its role as health care provider. If it wereprepared to move gradually towards taking a greater role in stewardship over the wholesector and strengthened its supervision and monitoring role while allowing other actors toprovide services, donor organizations might be more willing to support the health caresector in Bihar. The following section introduces some ideas for engaging the private sector.
Engaging the Private Sector
80. Improving primary health outcomes in Bihar requires among other things; (i) building fromscratch or rehabilitating a large number of PHCs and sub-centers, (ii) providing the PHCswith adequate staff and equipment, (iii) maintaining the centers, (iv) supervising theiroperations to ensure that renovated facilities function to their fullest capacity.
81. Given its limited capacity, government would be hard stretched to meet these requirements.However, there are lots of private sector stakeholders that are willing to provide theirmanagement and health care expertise to run such facilities. Many have already startedwith their own funds to take on some of these challenges. As explained above, relying onthe generosity of the private sector is not sustainable and cannot be scaled up. Thereforegovernment should consider supporting and tapping into these initiatives through publiclyfunded but privately provided health care. In essence government would be changing itsrole away from direct provider of health care towards purchasing, regulating and monitoringservice provision.
82. For instance, government could recruit the private sector to provide health care services toselected areas on the basis of performance contracts. The contracting model and internationalexperience is explained at length in another bank document that has been drafted as part ofthis study. Other states have experimented with contracting models for the operation andmaintenance of primary health care facilities. In Bihar this model could be extended tocover the construction of facilities and provision of equipment. An alternative model thathas worked well in Punjab and Andhra Pradesh is for government to seek donor support to
22

build the facilities and then introduce performance based contracts (within the public sectorin Punjab and with the private sector in AP) to improve service delivery.
83. Experience in AP has shown that even NGOs that have little or no experience in health carecan be very effective in contracting with government, mobilizing resources to augmentgovernment funds, and delivering innovative and cost effective services that improve healthoutcomes. Bihar has an advantage that many NGOs are already operating and have showntheir ability to deliver good quality services in the most difficult circumstances. Governmentcan begin pilots using these groups and if successful move to integrate more for-profitproviders at a later stage.
Improving the Performance of Informal Providers
84. In the long term, RMPs will inevitably disappear as factors on the supply side (improvingavailability and functioning of public sector facilities along with increased harassment ofunregistered practitioners) as well as demand side (improved patient awareness andeducation) squeeze their practices. However, in the short to medium term there are a numberof options for dealing with them each has its pros and cons.
� Ignore: The current situation in which the supreme court has outlawed all RMPs butgovernment lacks the manpower and perhaps the will power to implement the decisionresults in the continued practice of RMPs. This has the advantage that it leaves in placea system of first call for many in rural areas. However, the down-side means that RMPscontinue to practice irrational medicine. RMPs endanger their patients health byunnecessary and often unsanitary injections, over-prescription of anti-biotics, (oftenprescribing an incomplete course for those that cannot afford a full course of treatment)and dangerous interventions such as intravenous drips for minor dehydrations. At bestthe public are simply wasting their time receiving a placebo and a comforting chat, atworst they are exposing themselves to serious diseases and contra-indicated medication.
� Involve: Some stakeholders have suggested that all quacks could be mainstreamed andtrained as general health workers. Each PHC covers around 50 villages and wouldtherefore be likely to include an area in which upto 100 informal providers are operating.They could be brought under the control and supervision of a qualified doctor at thePHC. Although this idea seems appealing at first, it might prove unworkable in practiceas quacks are well-paid making between Rs5-10,000 per month in consultations andsome observers contend that they make several times that amount in referral commissionsand will not be willing to be mainstreamed if that would result in a reduction in theirincomes. Moreover, qualified doctors at the PHC are often not present and therefore noteffectively supervising the PHC staff much less a large number of unqualifiedpractitioners in remote rural areas.
� Train: Informal providers can be trained to undertake new tasks or improve currentservices. A recent study among informal private practitioners in Bihar showed thatinformal private providers improved their history taking, examination and counselingpractices for ARI, diarrhea and fever following training based on verbal case reviewand INFECTOM methodologies.18
18 Chakraborty et. al. 2000.
23

Bihar: A Rapid Private Health Sector Assessment
� Educate: Informal providers are meeting a demand for health care in rural areas.Communities would like to have reliable care available. However, they are poorlyeducated and cannot tell whether they are receiving good service or not. A mass educationcampaign could be useful to both increase awareness of common illnesses andsimultaneously raise awareness of the dangers of quackery.
� Franchise: The Janani model has shown that involving RMPs in a franchise schemehas a number of advantages. It can train the RMPs to provide useful services such asfamily planning products and advice. It is usually tied with a mass marketing campaignthat can also raise awareness. However, such a program cannot reduce the irrationalactivities of RMPs.
85. Any successful course of action will have to address the realities of the political economyof rural villages. Following on from the Supreme Court’s various edicts concerning quackery,the High Court of Punjab passed a ruling to “weed out quacks from rural areas”. However,government is unwilling to implement this decision for the simple reason that RMPsconstitute an important vote bank and are closely connected to the Panchayati Raj in mostvillages. They outnumber qualified doctors by at least 10:1 and therefore wield considerablepolitical clout.
86. In some areas, quacks are so powerful and well entrenched in the local community that theyare able to drive out qualified public sector doctors that threaten them. In other communities,RMPs build lucrative symbiotic referral relationships with unscrupulous private sectordoctors. Informal providers are also careful to share a percentage of their profits with thelocal police and elected officials to ensure that these groups turn a blind eye to their practices.
87. In the medium term, government has set ambitious targets for institutional deliveries as it ishoped that this will reduce the IMR and MMR. Health seeking data indicates thatapproximately 60 percent of births are attended by a dais or trained birth attendant (TBA).Such individuals are usually completely untrained and have little or no equipment. Theyhave often inherited the trade from their mothers and have a low social status and concomitantpoor education and literacy rates. Providing all TBA with standard delivery kits and a shorttraining course in the basics of normal delivery could represent a viable option in the shortterm while government takes time to build its health care infrastructure.
Private Sector Financing Options
88. Earlier sections have shown that in the absence of a well-functioning public system, thepoor often utilize private health care services many of which are barely affordable. Themost vulnerable groups spend the largest proportion of their income on such care. Beloware some initial suggestions to ameliorate this situation in future.
� Financing Out-patient treatment: Although on a per visit basis, OPD is the least expensivetype of medical care, it accounts for 82 percent of out-of-pocket spending in Bihar.19
The poor are especially hard hit by such spending as they often live further from viablefacilities implying that they have less choice and have to spend more time and moneyaccessing health care.
19 NSS 1995/6
24

� Community-based health-specific funds or micro-insurance schemes providing smallloans have been successful in many communities. However, their success depends ongetting SHGs to be a distribution point for preventive and minor curative services andcommodities that do not require a medical practitioner. For example, in other developingcountries in Asia, village women are trained to dispense pills and condoms and ORS,while others are trained to take blood pressure, weight and height. More often than not,such services and commodities can be provided for a small fee to offset the cost oftransportation to get the commodities from the nearest government health center. Thefee paid will still be smaller than that of a private provider and the care given is likely tobe more rational.
� Health Insurance for the Poor: Establishing a comprehensive health insurance schemefor the poor would increase their uptake of health care services. Unfortunately the currentUHIS scheme is unlikely to provide a viable response to the health care needs of thepoor as it currently unsustainable due to questionable risk pooling and provideraccessibility particularly for those residing in the rural areas. It also has features thatcould be open to abuse, such as the disability payment due to hospitalization. Moreoverthe scheme does not address preventive care. Another World Bank team is reviewingthe potential of the Yashaswini Farmers’ Scheme as a promising alternative.
� Co-opting the Private Sector: There are efforts to co-opt the private sector to participatein certain government programs, such as immunization. In such cases, it is not clearwhether the private sector should be allowed to charge a fee for service. In general,unless the government reimburses or pays for the vaccine administration, it should allowthe private sector to charge a fee for the service. The costs of administering the vaccineare substantial (the personnel, the space, the utilities that are used up, the instrumentsand equipment, such as a sterilizer and other consumables) and paying for them willensure the widest involvement of the private sector. When a private sector entityparticipates in a preventive or primary health care program, government should sign anMOU to detail the rules of engagement. Such a document will help to provide clarityand protect all parties.
25

Bihar: A Rapid Private Health Sector Assessment
Selected Bibliography
Chakraborty, S., Ann D’Souza S., Northrup R, 2000. Improving Private Practitioner Careof Sick Children: testing new approaches in Bihar. Health Policy and PlanningVolume 15 (4).
Das, Dr. Mahibir 1999. Status Of Health in Bihar, India.
Nuken, B. Amenla 2002. “Maternal Health Care Among Rural Women of Bihar: Evidencefrom National Family Health Survey II”. Mumbai October 2002.
NFHS 1998/99. National Family Health Survey, National Report, Government of India NewDelhi 2002.
NSS 1995/95. National Sample Survey Organization, National Report 52nd Round. Governmentof India, New Delhi.
Ratan, Vishwa 2001. “Profile of an Additional Primary Health Care Center”, Bihar.
—————— 2003. “Bihar State Health Profile at a Glance”, Bihar.
Saxena, N. C. ICDS and Immunization Programmes in Bihar. January 2004.
UNICEF 1995. ‘The progress of Indian States”. New Delhi.
26