Molecular Mechanisms of Fibroblast Growth Factor Signaling ...

Review
Beyond VEGF: Inhibition of the Fibroblast Growth FactorPathway and Antiangiogenesis
Christopher Lieu1, John Heymach2, Michael Overman1, Hai Tran2, and Scott Kopetz1
AbstractFibroblast growth factor (FGF) signaling regulates cell proliferation, differentiation, survival, angiogen-
esis, and wound healing. Compelling evidence for deregulated FGF signaling in tumorigenesis continues to
emerge, and a growing body of research suggests that FGF may also play an integral role in the resistance
to anti-VEGF therapy. Although agents targeting FGF signaling are early in development, the potential to
target both the VEGF and FGF pathways may translate into improvements in the clinical care of cancer
patients. Clin Cancer Res; 17(19); 6130–9. �2011 AACR.
Introduction
Fibroblast growth factors (FGF) belong to a structurallyrelated family of 22 molecules that interact with high-affinity tyrosine kinase FGF receptors (FGFR) to regulatemultiple fundamental pathways and cellular behaviors (1).FGF signaling regulates events in embryonal development,including mesenchymal–epithelial signaling and the de-velopment of multiple organ systems (2, 3). FGF signalingalso regulates cell proliferation, differentiation, and surviv-al, as well as angiogenesis and wound healing (4). In somesituations, FGFs can act as a negative regulator of prolifer-ation and positive regulator of differentiation (5). Giventhe role of FGF in multiple cellular processes, compellingevidence for deregulated FGF signaling in tumorigenesiscontinues to emerge (6). Studies with animal models havesuggested that aberrant FGF signaling can promote tumordevelopment through increased cell proliferation and sur-vival, as well as increased tumor angiogenesis (7, 8). Thisbody of research indicates that FGF signaling is an impor-tant pathway in tumorigenesis and tumor angiogenesis andthat appropriate targeting of the FGFR tyrosine kinases maybe an effective therapeutic intervention for cancer.
This review describes the FGF family of growth factorsand their associated receptors, as well as their associationwith tumor development, growth, and metastasis. We alsodescribe the effect of FGFs on tumor angiogenesis, includ-ing key preclinical and clinical evidence about the role of
FGFs in the development of resistance to anti-VEGF ther-apy. Finally, FGF as a potential therapeutic target isreviewed, including the current state of drug developmentin this field.
Fibroblast Growth Factor Family
FGFs were first isolated as mitogens from pituitaryextracts and bovine brain tissue in the 1970s (9, 10). Sinceinitial discovery, 22 members of the FGF family have beenidentified, all of which are structurally related signalingmolecules ranging from 17 to 34 kDa in size (11). SomeFGFs seem to be expressed exclusively during embryonicdevelopment (FGF-3, 4, 8, 15, 17, and 19), and others areexpressed in both embryonic and adult tissues (FGF-1, 2,5–7, 9–14, 16, 18, and 20–23; ref. 11).
FGFs are structurally similar to one another, with 28highly conserved and 6 identical amino acid residues (12).Most FGFs are secreted glycoproteins (FGF-3–8, 10, 15, 17–19, and 21–23), but FGF-1 and FGF-2 are exported fromcells by mechanisms that remain unclear. FGF-1 and FGF-2may be released from damaged cells or by exocytosis that isindependent of the endoplasmic reticulum–Golgi pathway(13). FGFs have strong affinities for the glycosaminoglycanside chains of cell surface proteoglycans, which help tosequester FGFs on the surface of the secreting cell or onnearby cells, and in the binding of FGF to the FGFR.
FGFRs are transmembrane tyrosine kinases that contain2 or 3 extracellular immunoglobulin-like domains and anextracellular heparin-binding sequence (14–16). The 2proximal immunoglobulin-like extracellular domains bindthe FGF ligand, whereas the heparin-binding sequencebinds a glycosaminoglycan moiety, resulting in the forma-tion of a complex containing 2 FGFs, 2 FGFRs, and theglycosaminoglycan moiety (17). Only 4 FGFRs are knownto exist, designated FGFR-1 through FGFR-4 (Table 1).Their specificity for various ligands is altered by processesthat create multiple isoforms. Alternative mRNA splicing of
Authors' Affiliations: Departments of 1Gastrointestinal Medical Oncologyand 2Thoracic/Head and Neck Medical Oncology, The University of TexasMD Anderson Cancer Center, Houston, Texas
Corresponding Author: Scott Kopetz, Department of GastrointestinalMedical Oncology, The University of Texas MD Anderson Cancer Center,1515 Holcombe Boulevard, Unit 0426, Houston, TX 77030. Phone: 713-792-2828; Fax: 713-563-6764; E-mail: [email protected]
doi: 10.1158/1078-0432.CCR-11-0659
�2011 American Association for Cancer Research.
ClinicalCancer
Research
Clin Cancer Res; 17(19) October 1, 20116130
on June 8, 2020. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 27, 2011; DOI: 10.1158/1078-0432.CCR-11-0659

the FGFR gene significantly alters the ligand specificity bychanging the sequence of the carboxy-terminal half ofimmunoglobulin-domain III. This sequence change resultsin 2 isoforms termed IIIb and IIIc (18, 19). In general, IIIbisoforms are expressed on epithelial cells, and IIIc isoformsare expressed on mesenchymal cells, where they mediatetissue interactions in normal development and woundhealing (20–22).FGF signaling can also be modulated by several mem-
brane proteins, including cell adhesion molecules of thecadherin and immunoglobulin superfamilies (23). Thebest characterized of these is neural cell adhesion molecule(NCAM). NCAMhas been shown to be amajor regulator ofFGF-FGFR interaction in several cell types, including non-neural tissues (24). NCAM has been shown to act as anonconventional ligand that can induce a specific FGFR1-mediated cellular migration that is different from theresponse elicited by FGF-2 (25). Furthermore, NCAM ex-pression has been shown to reduce FGF-stimulated extra-cellular signal regulated kinase (ERK)1/2 activation, cellproliferation, and cell-matrix adhesion in fibroblast celllines, suggesting that NCAM acts as a novel control mech-anism for FGFR signaling (26).
Fibroblast Growth Factor and Tumor Growth
Aberrant FGF and/or FGFR signaling has a wide range ofeffects and can involve both tumor cells and the surround-ing stroma. These effects include cellular proliferation;resistance to cell death; increasedmotility and invasiveness;increased angiogenesis; enhanced metastasis; and resis-tance to chemotherapy (27). Deregulation of FGF signalingin tumorigenesis can result from activating mutations,FGFR gene amplifications, and chromosomal transloca-tions, which lead to increased autocrine and paracrinesignaling (28–30). Because aberrant signaling can promotetumorigenesis by affecting major downstream biologicprocesses, FGFs have been implicated in multiple tumortypes, including prostate, astrocytoma, breast, lung, blad-der, hepatocellular, and colon cancers (31–41).
Alternative splicing of the FGFR gene has also beenimplicated in carcinogenesis. Carcinomas have been ob-served to switch expression of FGFR to the mesenchymalisoforms, enabling cells to receive signals usually restrictedto the connective tissue, such as ectopic expression oftypically stroma-localized FGFR1-IIIc (42, 43). The IIIcsplice variant has been detected in colon carcinoma butnot in adenoma-derived cell lines, suggesting that it isupregulated during tumor progression (44). During pros-tate cancer progression, alternative splicing of FGFR2 canoccur in epithelial cells, leading to isoform changes fromFGFR2-IIIb into the more ligand-promiscuous FGFR2-IIIc(Fig. 1; refs. 8, 43). Thus, this aberrant alternative splicingof FGFR potentially destroys the balanced interdependencebetween stroma and epithelium (8, 43, 45).
Clinical studies of FGF have suggested a critical role ofFGF signaling in clinical tumor progression. In 1 study ofadvanced serous ovarian adenocarcinomas, FGF-1 mRNAcopy number was found to be significantly correlated withDNA copy number and protein expression levels (46). BothFGF-1 mRNA and protein levels were associated with worseoverall survival, possibly secondary to an increase in tumorangiogenesis and autocrine stimulation of cancer cells. Inanother study of 100 resected colorectal cancer surgicalspecimens, high FGF-2 expression was associated withincreased grade, stage, lymphovascular invasion, and intra-tumoral microvessel density (47). Significantly elevatedlevels of FGF-2 in circulation were found in a small cohortof patients with metastatic colorectal cancer, relative tomedian levels in control subjects (48). In other studies,although increased levels of FGF-2 were found in plasmafrom patients with different types of cancer, it was unclearwhether the higher levels resulted from tumor invasion anddegradation of the extracellular matrix (ECM), liberatingFGF to function as a paracrine growth factor, or whethertumor cells induced FGF2 release from stromal inflamma-tory infiltrate (49, 50).
Loss of expression of NCAM has also been implicated inthe progression of tumor metastasis. NCAM has beenshown tomodulate neurite outgrowth andmatrix adhesionof b cells from the Rip1-Tag2 transgenic mouse model ofpancreatic neuroendocrine tumors by assembling a FGFR-4
Translational Relevance
Angiogenic inhibitors have shown promise in thetreatment of multiple tumor types and have improvedoutcomes in patients with metastatic disease. However,many patients will not respond to antiangiogenic ther-apy, and for those that do, resistance develops quickly.Fibroblast growth factor (FGF) seems to play an integralrole in the resistance to antiangiogenic therapy, andagents that specifically target the FGF pathway are beingdeveloped and tested in clinical trials. It is critical thatinvestigators review the existing literature on FGF andtumor angiogenesis to understand the importance ofthis target in various malignancies, as well as to designrational clinical trials that can expedite a potentiallymeaningful therapy in patients previously treated withantiangiogenic agents.
Table 1. Receptors for the FGFR family
Receptor Specific For
FGFR-1b FGF-1, 2, 3, and 10FGFR-1c FGF-1, 2, 4, 5, and 6FGFR-2b FGF-1, 3, 7, and 10FGFR-2c FGF-1, 2, 4, 6, and 9FGFR-3b FGF-1 and 9FGFR-3c FGF-1, 2, 4, 8, and 9FGFR-4 FGF-1, 2, 4, 6, 8, and 9
Adapted from Itoh and Ornitz (1).
Inhibition of the FGF Pathway and Antiangiogenic Therapy
www.aacrjournals.org Clin Cancer Res; 17(19) October 1, 2011 6131
on June 8, 2020. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 27, 2011; DOI: 10.1158/1078-0432.CCR-11-0659

signaling complex that leads to the modulation of b1-integrin–mediated cell-matrix adhesion (51). Ablation ofthe expression of NCAM in this mouse model resulted inthe disruption of the tumor tissue architecture, tumor-associated lymphangiogenesis, and lymph node metastasis(51, 52).
Though a full review of FGF signaling and tumor growthis beyond the scope of this article, please see the compre-hensive review from Turner and Grose for additionalinformation (41).
Fibroblast Growth Factors and Angiogenesis
Angiogenesis, the formation of new blood vessels fromthe endothelium of the existing vasculature, plays a pivotalrole in tumor growth, progression, and metastasis (53, 54).Along with embryogenesis, angiogenesis was one of thefirst areas where FGF signaling was shown to be important(55, 56). In particular, FGF-1 and FGF-2 were found to beimportant for new blood vessel growth at the site of anexcision wound and have been shown to stimulate angio-genesis in various assays (57–59). FGF-2 is a very potentinducer of angiogenesis. In a preclinical model of micro-vascular endothelial cells grown on a 3-dimensional col-
lagen gel, VEGF and FGF-2 were able to induce cells toinvade the underlying matrix to form capillary-like tubules(60). Interestingly, FGF-2 was found to be twice as potentas VEGF in this model. The critical role of FGF in tumorangiogenesis was shown through the interference of FGFfunction with a recombinant adenovirus expressing solubleFGFR (AdsFGFR). AdsFGFR seemed to impair the mainte-nance of tumor angiogenesis, in contrast to inhibition ofthe VEGF pathway that predominantly affected the initia-tion of tumor angiogenesis (61). Injection of AdsFGFR inthe Rip1-Tag2murine model of pancreatic neuroendocrinetumor resulted in repression of tumor growth, with asignificant decrease in tumor vessel density. FGFs exerttheir effects by modulating proliferation and migrationof endothelial cells, production of proteases, and promo-tion of integrin and cadherin receptor expression (62).In particular, FGF-1 and FGF-2 directly affect tumorangiogenesis by promoting the cellular proliferation ofendothelial cells. FGF-2 has been shown to induce revas-cularization in various experimental models in severalspecies, including rabbit, chicken, and mouse (63–65).In a murine model, FGF-1 knockout mice and FGF-1/FGF-2 double-knockout mice had poor wound healingcompared with normal control mice (58). FGFR-1 is most
© 2011 American Association for Cancer Research
FGF
FGF
FGFR lllcBloodvessel
lllc
FGFRlllb
EpitheliumStroma
ECM
Normal
FGFFGF-BP
FGF
PDGF
VEGFAng2
FGFR lllc NRP1 PDGFRBloodvessel
FGFRlllc
FGFRlllc
EpitheliumStroma
ECM
Cancer
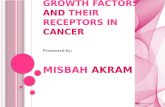
Figure 1.Changes in FGF and FGFR in the microenvironment and epithelium in normal tissue and cancer. Compared with normal tissue, alternative splicing ofthe FGFR gene can switch expression of FGFR from the IIIb isoform to the ligand promiscuous IIIc isoforms. Furthermore, release of FGF from thetumor and stroma may initiate tumor angiogenesis. FGF-BP–mediated reduction of the affinity of FGF-2 to heparin can induce its release from the ECM.FGF-BP, FGF binding protein; PDGF, platelet-derived growth factor; PDGFR, platelet-derived growth factor receptor.
Lieu et al.
Clin Cancer Res; 17(19) October 1, 2011 Clinical Cancer Research6132
on June 8, 2020. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 27, 2011; DOI: 10.1158/1078-0432.CCR-11-0659

commonly expressed on endothelial cells, although FGFR-2 has been shown to be present under certain circum-stances (50, 66). The presence of FGFR-3 and FGFR-4has not been reported in the endothelium.FGFs can exert their angiogenic mechanism of action via
paracrine signaling through their release by tumor andstromal cells, or through their mobilization from theECM (50). FGF-1, in particular, may stimulate endothelialcell growth and the motility of endothelial cells throughparacrine signaling, which results in increased prolifera-tion, survival, and motility of endothelial cells (46). FGF-2has been studied in xenograft models in which liposome-mediated gene transfer was used to deliver episomal vectorscontaining antisense FGF-2 or FGFR-1 cDNAs into humanmelanomas grown in nude mice. In contrast to the stim-ulation seen during deregulated FGF signaling, tumorsinjected with these antisense constructs showed arrestedtumor growth or reduced tumor density because of blockedintratumoral angiogenesis (67). There is also evidence thatFGF-2 increases the expression of angiopoietin-2, a potentregulator of vascular branching and angiogenesis, as well asVEGF in cultured human and endothelial cells (68).FGFs may also exert their effects through autocrine
signaling in endothelial cells, stimulating the proliferationof new capillary endothelial cells (66). This induces aproangiogenic state that creates an environment favorablefor vascular growth. Evidence for this growth is seen in aparticular subtype of Kaposi sarcoma (KS) in which FGF-2,produced by the KS cells, has been found to synergize withhuman immunodeficiency virus type 1 Tat protein toenhance endothelial cell growth and type IV collagenaseexpression (66, 69). These tumors were found to haveincreased aggressiveness and frequency compared withother forms of KS.Preclinical models of tumor angiogenesis have suggested
that FGF–binding protein (FGF-BP) serves as an angiogenicswitch molecule and can be rate limiting for tumor growth(70). FGF-2 is present in most tissues under normal phys-iologic conditions but is inactivated by being tightly boundto the ECM. FGF-BP binds to FGF-2 in a dose-dependentmanner, which results in a marked reduction of the affinityof FGF-2 to heparin and release from the ECM (Fig. 1; refs.71, 72). Exogenously administered FGF-BP has been shownto stimulate FGF-2–dependent growth of both adrenalcarcinoma and prostate carcinoma cells. In addition, down-regulation of FGF-BP expression has been shown to inhibitangiogenesis in squamous cell carcinoma xenografts (73).
Fibroblast Growth Factor–2 Cross-Talk withAngiogenic Factors
VEGF plays an integral role in the development of newblood vessels in tumor formation, and angiogenesis inhi-bitors targeting the VEGF pathway have proved to be effi-cacious inpreclinical cancermodels and in clinical trials (74,75). A significant amount of cross-talk is thought to existbetween members of the VEGF family and FGF-2 duringangiogenesis, with VEGF appearing earlier during angiogen-
esis than does FGF (50). In 1 study, the angiogenic responseoccurred more quickly when VEGF and FGF-2 were addedsimultaneously to microvascular endothelial cells on 3-dimensional collagen gels than the response to either cyto-kine alone, suggesting synergy between the 2 cytokines (60).It has also been shown that induction of FGF-2–inducedangiogenesis is partly dependent on the activation of VEGFand the presence of endogenous VEGF and VEGF-C (76).Evidence for synergybetweenVEGF andFGF-2has alsobeenshown in xenograft models expressing FGF-2 and VEGF intumor cell transfectants. Simultaneous expression of FGF-2and VEGF resulted in fast-growing lesions with high bloodvessel density and permeability (77). Interestingly, inhibi-tion of FGF-2 production caused a significant decrease intumor burden with a concomitant decrease in blood vesseldensity and size. This differed from the effects of VEGFinhibition,whichcausedadecrease inpericyteorganization,vessel patency, and permeability. This finding suggests thatFGF-2 and VEGF stimulate angiogenesis synergistically butwith different effects on vessel size and function.
FGF-2 may also have indirect effects on VEGF pathways.In a breast cancer cell line (T47D), FGF-2 was found toactivate hypoxia-induced VEGF release through augmenta-tion of the phosphoinositide 3-kinase pathway, as well ashypoxia-inducible factor-1a expression (78). FGF-2 hasalso been shown to indirectly enhance the effect of VEGFthrough upregulation of neurolipin-1 (NRP-1), a corecep-tor for VEGF. FGF-2 increased NRP-1 levels and enhancedthe migration of human vascular smooth muscle cells inresponse to VEGF.
There is also evidence of cross-talk between FGF-2 andplatelet-derived growth factor (PDGF)–BB. FGF-2 andPDGF-BB together have been shown to synergisticallypromote tumor angiogenesis and pulmonary metastasis,as well as formation of high-density primitive vascularplexuses coated with pericytes and vascular smooth musclecells (79). Pericyte recruitment to coat nascent vesselsduring angiogenesis is essential for the stabilization andfurther establishment of a tumor’s vascular network. FGF-2seems to upregulate PDGF receptor (PDGFR) expression,which causes increased responsiveness to PDGF-BB, andPDGF-BB–treated vascular smooth muscle cells becomeresponsive to FGF-2 signaling through upregulation ofFGFR-1. Interestingly, overexpression of PDGF-BB alonein tumor cells was shown to result in decreased recruitmentof pericytes and dissociation of vascular smooth musclecells. In tumor cells subjected to prior upregulation ofFGF-2 caused by VEGF receptor 2 (VEGFR2) inhibition,PDGFR-b inhibition also attenuated the expression ofFGF-2 (80). In a mouse model of cervical carcinogenesis,pharmacologic blockade of PDGFR signaling with imatinibslowed progression of premalignant cervical lesions andimpaired the growth of preexisting invasive carcinomasthrough suppression of the expression of FGF-2 andFGF-7, which resulted in decreased proliferation and an-giogenesis within the lesions (81). Treatment with an FGFtrap also impaired the angiogenic phenotype similar to theblockade of the PDGFR with imatinib.
Inhibition of the FGF Pathway and Antiangiogenic Therapy
www.aacrjournals.org Clin Cancer Res; 17(19) October 1, 2011 6133
on June 8, 2020. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 27, 2011; DOI: 10.1158/1078-0432.CCR-11-0659

Fibroblast Growth Factor Signaling andResistance to Anti-VEGF Therapy
Emerging evidence has suggested that upregulation ofFGF and FGFR may serve as a mechanism of resistance toanti-VEGF therapy. Preclinical trials of anti-VEGF therapyin a murine pancreatic neuroendocrine tumor model(PNET), Rip1-Tag2, showed that tumors with an initialresponse to VEGFR2 blockade expressed higher levels ofFGF-2 at the time of progression compared with stabletumors (82). When the tumors were first treated with aVEGFR inhibitor alone and subsequently treated at thepeak of response with an FGF trap, the combinationattenuated revascularization and slowed tumor growth(Fig. 2). The dual tyrosine kinase inhibitor (TKI) of VEGFRand FGFR, brivanib, has also been studied in this murinemodel and has proved to be efficacious following thefailure of 2 VEGFR inhibitors (83). It was even moreeffective when used in the frontline setting, suggesting thatdual inhibition of VEGFR and FGFR was able to delayinduction of evasive resistance. Further evidence for therole of alternative angiogenic factors in tumor escape fromangiogenesis inhibitors has been shown in tumors in whichgrowth was impaired by ectopic expression of the endog-enous angiogenesis inhibitors thrombospondin-1, tumsta-tin, and endostatin (84). In that study, renal carcinomacells transfected with thrombospondin-1 resisted angio-genesis inhibition by upregulating the proangiogenic fac-tors FGF-2, angiopoietin 2, and PDGF-A, despite high
baseline levels of VEGF. In 1 xenograft model of renal cellcarcinoma, tumors unresponsive to sunitinib treatmentwere sensitive to a dual inhibitor of the VEGF and FGFRs(85). This inhibitor seemed to reduce blood vessel densitythrough inhibition of FGF-2–induced angiogenesis.
Clinical evidence in colon cancer also supports the roleof FGF-2 in resistance to bevacizumab-containing regi-mens. To determine the dynamic changes in circulatingfactors during the emergence of therapeutic resistance,profiles of cytokines and angiogenic factors were assessedin 40 patients receiving a regimen of 5-fluorouracil (5-FU),leucovorin, and irinotecan (FOLFIRI) plus bevacizumab.Levels were assessed after a single dose of bevacizumab andFOLFIRI plus bevacizumab, at the time of progression, andat the nadir of radiographic response (86, 87). The inves-tigators showed that FGF-2 levels were elevated immedi-ately prior to progression compared with baseline levels.Strikingly, 30% of patients had an increase in FGF-2 to 10-fold the upper limit of normal, suggesting significantheterogeneity in the FGF-2 response. In 1 study of neoad-juvant bevacizumab with 5-FU and radiation in rectalcancer, the administration of a short regimen of bevacizu-mab in combination with chemotherapy had no significanteffect on plasma FGF-2 levels, suggesting that elevations inFGF-2 are instead a later event temporally associated withthe development of resistance to the bevacizumab combi-nation regimen (88).
Elevated FGF-2 levels have also been shown in glioblas-toma patients treated with a VEGFR small molecule
0
20
Control
t = 0 10 days 4 weeks
Control Anti-R2 Anti-R2 Anti-R2FGF-trap
40
60
80
100
120
140
160
Tum
or
bur
den
(mm
3 )
*
Figure 2. VEGFR2 blockadetransiently stops tumor growthand decreases vascularity,followed by tumor progression,reinduction of angiogenesis, andreestablishment of the tumorvasculature. Quantification ofoverall tumor burden plotted asaverage and SD per animal at thetime of initiation of treatment(t ¼ 0; purple bar), after treatmentfor 10 days (orange bars), and at4 weeks of age (teal and greenbars) for the different treatmentarms. Averages from cohorts of 8to 10 mice per group are plottedwith their respective SD bars.(Adapted from Cancer Cell, withpermission from Elsevier; ref. 82.)
Lieu et al.
Clin Cancer Res; 17(19) October 1, 2011 Clinical Cancer Research6134
on June 8, 2020. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 27, 2011; DOI: 10.1158/1078-0432.CCR-11-0659

inhibitor (89). In patients who experienced tumor progres-sion while receiving treatment, increased tumor enhance-ment volume was associated with significant increases inplasma levels of FGF-2 and stromal cell–derived factor-1. Astatistically significant positive correlation was observedbetween FGF-2 levels and tumor vessel size measured byMRI. This work provided further clinical evidence that FGF-2 may play a role in tumor relapse in patients treated withanti-VEGF agents (89).Unlike preclinical models, clinical studies investigating
levels of FGF can only show an association of elevatedFGF and/or FGFR with the resistance to anti-VEGF ther-apy; they cannot show causation or an actual resistancemechanism. Furthermore, because most studies are con-ducted in combination with cytotoxic chemotherapy, it isdifficult to discern whether the patient and tumor havebecome resistant to the chemotherapy, the antiangiogenictherapy, or both. Therefore, high-quality preclinical mod-els will be essential for further investigation to provide asound preclinical rationale for future clinical studies.
Targeting Fibroblast Growth Factor
Because FGFs have a clearly defined role in tumorangiogenesis, as well as a possible role in resistance tocurrent VEGF inhibitors, several FGF pathway inhibitorsare currently under development. The inhibitors enteringthe clinic are either TKIs or soluble antibody fragmentsthat block ligand binding and receptor dimerization(Table 2). Most of the TKIs have dual specificity for FGFRand VEGFR, both as a matter of design and because of thestructural similarities in their kinase domains. However,the inhibitors vary in their relative potency for VEGFR andFGFR, with many inhibitors having higher potency forVEGFR than FGFR (90, 91). Targeting both kinases mayalso increase the toxicity associated with these com-pounds, although biologically active doses have beenshown with most of the compounds (41). The other classof compound in development, FGF ligand trap, has thepotential to block the interaction of multiple FGF ligandswith the soluble FGFR fragments. In 1 study, such anFGFR-1 antagonist was shown to prevent FGFR-1 ligands
from binding, and it had in vitro activity against lung andrenal cell carcinoma (92).
The safety of FGFR inhibitors currently under develop-ment seems acceptable. Preclinical toxicity studies withthese agents have not shown a reproducible class effect,aside from hypertension, which is difficult to attribute tothe VEGFR or FGFR inhibitory effects of many of the agents(93, 94). Monoclonal antibodies directed against FGFR1-IIIc resulted in anorexia in mice and monkeys, which wascaused by an FGF signaling blockade in the hypothalamus,and a similar toxicity was seen in 1 phase I study (95, 96).Encouragingly, the concerns based on preclinical studiesabout phosphate and vitamin Dmetabolism have not beenreflected in the reported toxicities in the early-phase studies(97).
Although a separate development strategy is being pur-sued based on somatic mutation or amplification of FGFR(reviewed in ref. 98), antiangiogenesis strategies targetingthe tumor microenvironment pose additional drug devel-opment strategies. Prior studies of anti-VEGF antibodieshave shown clinical utility when the agents are used incombination with cytotoxic therapy and minimal activityas single agents with rare exceptions (75, 99). Similarly,FGF inhibition alone is unlikely to show a significantbenefit in various tumor types. Combination strategiesof FGF/FGFR inhibition with traditional cytotoxic therapyin tumor types in which proliferation and angiogenesis isFGF/FGFR–dependent will have the highest likelihood ofachieving a clinical benefit.
The timing of FGF/FGFR–directed therapy is also an areaof emerging interest given the evolving evidence that theFGF axis may serve as an adaptive resistance mechanism toanti-VEGF therapy. Histopathologic evidence from a mu-rine PNET model suggests that the switch to an FGFRinhibitor during treatment with a VEGFR inhibitor maybe more effective at the time of early revascularization priorto detectable tumor growth (83). Future clinical trials willhelp determine whether dual inhibition of VEGFR andFGFR will be more effective in the front-line setting orwhether FGFR inhibition will be better instituted at thetime prior to or at progression after treatment with VEGF/VEGFR inhibitors. However, determination of biologic
Table 2. Current FGF and FGFR-targeting agents
Drug Manufacturer Target(s) Clinical development stage
TKI258 (dovitinib; ref. 96) Novartis FGFR, PDGFR, VEGFR Phase IIBIBF 1120 (Vargatef; ref. 104) Boehringer Ingelheim FGFR, PDGFR, VEGFR Phase IIIBMS-582664 (brivanib; ref. 105) Bristol-Myers Squibb FGFR and VEGFR Phase II and IIIE7080 (106) Eisai FGFR, PDGFR, VEGFR Phase ITSU-68 (SU6668; ref. 107) Taiho Pharmaceutical FGFR, PDGFR, VEGFR Phase I and IIAZD4547 (108) AstraZeneca FGFR Phase IFP-1039 (109) Five Prime Therapeutics FGF ligand trap (multiple FGFs) Phase IBGJ398 (110) Novartis FGFR Phase IAstex FGFR inhibitor (111) Janssen Oncology FGFR Preclinical
Inhibition of the FGF Pathway and Antiangiogenic Therapy
www.aacrjournals.org Clin Cancer Res; 17(19) October 1, 2011 6135
on June 8, 2020. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 27, 2011; DOI: 10.1158/1078-0432.CCR-11-0659

resistance to VEGF/VEGFR inhibitors is difficult in theclinic, as resistance to the cytotoxic component of thetreatment may be sufficient to induce tumor growth inthe absence of single-agent anti-VEGF activity. Determiningresistance to these inhibitors is a high hurdle for develop-ment of such alternate antiangiogenic therapies, and sev-eral strategies are being considered in the early clinicaldevelopment, including randomized discontinuation stud-ies and enrichment designs.
Biomarkers under consideration for FGF inhibitors in-clude plasma levels of FGF family members and increasedFGF-axis expression in the stroma; however, their use assurrogates for FGF/FGFR–dependent tumors remains un-clear. Integration of imaging or biomarkers of antiangio-genesis therapy likewise has hurdles of cost reproducibilityand lack of correlation with clinical efficacy, and theseapproaches are not routinely integrated into most clinicaldevelopment strategies of these agents (100, 101). Basedon the VEGF inhibitor experiences, radiographic endpointswith antiangiogenesis strategies will be difficult, and ulti-mately, the benefits of these agents will be measured bytheir ability to improve overall survival (102, 103).
Summary
FGFs are a family of growth factors that are involved inmany pathways that can contribute to carcinogenesis andaffect cellular proliferation, migration, and survival. They
also play a large role in angiogenesis, which is a funda-mental step in the transition from a dormant to a malig-nant state, and FGF acts synergistically with VEGF toincrease tumor blood vessel growth and maturation. Evi-dence is also increasing that FGF may be part of themechanism of resistance to anti-VEGF agents.
Although agents targeting FGF signaling are still earlyin development, the potential to target both the VEGFand FGF pathways is near, and the combination orsequential inhibition of these 2 critical angiogenic path-ways may translate into improvements in the clinical careof cancer patients. Successful strategies will depend onappropriate selection of tumors and patients in whomFGF inhibition is mostly likely to inhibit angiogenesisand proliferation.
Disclosure of Potential Conflicts of Interest
S. Kopetz: commercial research grant, AstraZeneca. The other authorsdisclosed no potential conflicts of interest.
Grant Support
NIH T32 CA-009666 (C. Lieu); National Research Service Award (NRSA)Research Training Grant; Conquer Cancer Foundation Young InvestigatorsAward (C. Lieu); NIH CA-136980 (S. Kopetz); NIH/National Cancer Institute(NCI) Cancer Center Support Grant (CCSG) Core Grant CA-106672.
Received March 18, 2011; revised July 20, 2011; accepted July 25, 2011;published OnlineFirst September 27, 2011.
References1. Itoh N, Ornitz DM. Evolution of the Fgf and Fgfr gene families. Trends
Genet 2004;20:563–9.2. De Moerlooze L, Spencer-Dene B, Revest JM, Hajihosseini M,
Rosewell I, Dickson C. An important role for the IIIb isoform offibroblast growth factor receptor 2 (FGFR2) in mesenchymal-epithe-lial signalling during mouse organogenesis. Development 2000;127:483–92.
3. Yamaguchi TP, Harpal K, Henkemeyer M, Rossant J. fgfr-1 isrequired for embryonic growth and mesodermal patterning duringmouse gastrulation. Genes Dev 1994;8:3032–44.
4. Baird A, Esch F, Morm�ede P, Ueno N, Ling N, B€ohlen P, et al.Molecular characterization of fibroblast growth factor: distributionand biological activities in various tissues. Recent Prog Horm Res1986;42:143–205.
5. Colvin JS, Bohne BA, Harding GW, McEwen DG, Ornitz DM. Skeletalovergrowth and deafness in mice lacking fibroblast growth factorreceptor 3. Nat Genet 1996;12:390–7.
6. Grose R, Dickson C. Fibroblast growth factor signaling in tumori-genesis. Cytokine Growth Factor Rev 2005;16:179–86.
7. Dickson C, Spencer-Dene B, Dillon C, Fantl V. Tyrosine kinasesignalling in breast cancer: fibroblast growth factors and theirreceptors. Breast Cancer Res 2000;2:191–6.
8. Feng S, Wang F, Matsubara A, Kan M, McKeehan WL. Fibroblastgrowth factor receptor 2 limits and receptor 1 accelerates tumori-genicity of prostate epithelial cells. Cancer Res 1997;57:5369–78.
9. Armelin HA. Pituitary extracts and steroid hormones in the control of3T3 cell growth. Proc Natl Acad Sci U S A 1973;70:2702–6.
10. Gospodarowicz D. Localisation of a fibroblast growth factor and itseffect alone and with hydrocortisone on 3T3 cell growth. Nature1974;249:123–7.
11. Ornitz DM, Itoh N. Fibroblast growth factors. Genome Biol 2001;2:reviews3005.1–3005.12.
12. Ornitz DM. FGFs, heparan sulfate and FGFRs: complex interactionsessential for development. Bioessays 2000;22:108–12.
13. Mignatti P, Morimoto T, Rifkin DB. Basic fibroblast growth factor, aprotein devoid of secretory signal sequence, is released by cells via apathway independent of the endoplasmic reticulum-Golgi complex.J Cell Physiol 1992;151:81–93.
14. Lee PL, Johnson DE, Cousens LS, Fried VA, Williams LT. Purificationand complementary DNA cloning of a receptor for basic fibroblastgrowth factor. Science 1989;245:57–60.
15. Johnson DE, Williams LT. Structural and functional diversity in theFGF receptor multigene family. Adv Cancer Res 1993;60:1–41.
16. McKeehan WL, Wang F, Kan M. The heparan sulfate-fibroblastgrowth factor family: diversity of structure and function. Prog NucleicAcid Res Mol Biol 1998;59:135–76.
17. Naski MC, Ornitz DM. FGF signaling in skeletal development. FrontBiosci 1998;3:d781–94.
18. Miki T, Bottaro DP, Fleming TP, Smith CL, Burgess WH, Chan AM,et al. Determination of ligand-binding specificity by alternative splic-ing: two distinct growth factor receptors encoded by a single gene.Proc Natl Acad Sci U S A 1992;89:246–50.
19. Chellaiah AT, McEwen DG, Werner S, Xu J, Ornitz DM. Fibroblastgrowth factor receptor (FGFR) 3. Alternative splicing in immunoglob-ulin-like domain III creates a receptor highly specific for acidic FGF/FGF-1. J Biol Chem 1994;269:11620–7.
20. Orr-Urtreger A, Bedford MT, Burakova T, Arman E, Zimmer Y, YayonA, et al. Developmental localization of the splicing alternativesof fibroblast growth factor receptor-2 (FGFR2). Dev Biol 1993;158:475–86.
21. Murgue B, Tsunekawa S, Rosenberg I, deBeaumont M, PodolskyDK. Identification of a novel variant form of fibroblast growth factorreceptor 3 (FGFR3 IIIb) in human colonic epithelium. Cancer Res1994;54:5206–11.
Lieu et al.
Clin Cancer Res; 17(19) October 1, 2011 Clinical Cancer Research6136
on June 8, 2020. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 27, 2011; DOI: 10.1158/1078-0432.CCR-11-0659

22. Scotet E, Houssaint E. The choice between alternative IIIb and IIIcexons of the FGFR-3 gene is not strictly tissue-specific. BiochimBiophys Acta 1995;1264:238–42.
23. Cavallaro U, Christofori G. Cell adhesion and signalling by cadherinsand Ig-CAMs in cancer. Nat Rev Cancer 2004;4:118–32.
24. Hinsby AM, Berezin V, Bock E. Molecular mechanisms of NCAMfunction. Front Biosci 2004;9:2227–44.
25. Francavilla C, Cattaneo P, Berezin V, Bock E, Ami D, de Marco A,et al. The binding of NCAM to FGFR1 induces a specific cellularresponse mediated by receptor trafficking. J Cell Biol 2009;187:1101–16.
26. Francavilla C, Loeffler S, Piccini D, Kren A, Christofori G, Cavallaro U.Neural cell adhesion molecule regulates the cellular response tofibroblast growth factor. J Cell Sci 2007;120:4388–94.
27. Kwabi-Addo B, Ozen M, Ittmann M. The role of fibroblast growthfactors and their receptors in prostate cancer. Endocr Relat Cancer2004;11:709–24.
28. Greenman C, Stephens P, Smith R, Dalgliesh GL, Hunter C, BignellG, et al. Patterns of somatic mutation in human cancer genomes.Nature 2007;446:153–8.
29. Kunii K, Davis L, Gorenstein J, Hatch H, Yashiro M, Di Bacco A, et al.FGFR2-amplified gastric cancer cell lines require FGFR2 and Erbb3signaling for growth and survival. Cancer Res 2008;68:2340–8.
30. Yagasaki F, Wakao D, Yokoyama Y, Uchida Y, Murohashi I, KayanoH, et al. Fusion of ETV6 to fibroblast growth factor receptor 3 inperipheral T-cell lymphoma with a t(4;12)(p16;p13) chromosomaltranslocation. Cancer Res 2001;61:8371–4.
31. Linder C, Bystr€omP, Engel G, Auer G, AspenbladU, Strander H, et al.Correlation between basic fibroblast growth factor immunostainingof stromal cells and stromelysin-3 mRNA expression in humanbreast carcinoma. Br J Cancer 1998;77:941–5.
32. Halaban R. Growth factors and melanomas. Semin Oncol 1996;23:673–81.
33. Bian XW, Du LL, Shi JQ, Cheng YS, Liu FX. Correlation of bFGF,FGFR-1 and VEGF expression with vascularity and malignancy ofhuman astrocytomas. Anal Quant Cytol Histol 2000;22:267–74.
34. Relf M, LeJeune S, Scott PA, Fox S, Smith K, Leek R, et al.Expression of the angiogenic factors vascular endothelial cell growthfactor, acidic and basic fibroblast growth factor, tumor growth factorbeta-1, platelet-derived endothelial cell growth factor, placentagrowth factor, and pleiotrophin in human primary breast cancerand its relation to angiogenesis. Cancer Res 1997;57:963–9.
35. Yamanaka Y, Friess H, Buchler M, Beger HG, Uchida E, Onda M,et al. Overexpression of acidic and basic fibroblast growth factors inhuman pancreatic cancer correlates with advanced tumor stage.Cancer Res 1993;53:5289–96.
36. Berger W, Setinek U, Mohr T, Kindas-M€ugge I, Vetterlein M, DekanG, et al. Evidence for a role of FGF-2 and FGF receptors in theproliferation of non-small cell lung cancer cells. Int J Cancer1999;83:415–23.
37. Gazzaniga P, Gandini O, Gradilone A, Silvestri I, Giuliani L, MagnantiM, et al. Detection of basic fibroblast growth factor mRNA in urinarybladder cancer: correlation with local relapses. Int J Oncol 1999;14:1123–7.
38. Dellacono FR, Spiro J, Eisma R, Kreutzer D. Expression of basicfibroblast growth factor and its receptors by head and neck squa-mous carcinoma tumor and vascular endothelial cells. Am J Surg1997;174:540–4.
39. Huang X, Yu C, Jin C, Yang C, Xie R, Cao D, et al. Forced expressionof hepatocyte-specific fibroblast growth factor 21 delays initiation ofchemically induced hepatocarcinogenesis. Mol Carcinog 2006;45:934–42.
40. Galdemard C, Brison O, Lavialle C. The proto-oncogene FGF-3 isconstitutively expressed in tumorigenic, but not in non-tumorigenic,clones of a human colon carcinoma cell line. Oncogene 1995;10:2331–42.
41. Turner N, Grose R. Fibroblast growth factor signalling: from devel-opment to cancer. Nat Rev Cancer 2010;10:116–29.
42. Yan G, Fukabori Y, McBride G, Nikolaropolous S, McKeehan WL.Exon switching and activation of stromal and embryonic fibroblast
growth factor (FGF)-FGF receptor genes in prostate epithelial cellsaccompany stromal independence and malignancy. Mol Cell Biol1993;13:4513–22.
43. Carstens RP, Eaton JV, Krigman HR, Walther PJ, Garcia-Blanco MA.Alternative splicing of fibroblast growth factor receptor 2 (FGF-R2) inhuman prostate cancer. Oncogene 1997;15:3059–65.
44. Sonvilla G, Allerstorfer S, Heinzle C, St€attner S, Karner J, KlimpfingerM, et al. Fibroblast growth factor receptor 3-IIIc mediates colorectalcancer growth and migration. Br J Cancer 2010;102:1145–56.
45. Acevedo VD, Gangula RD, Freeman KW, Li R, Zhang Y,Wang F, et al.Inducible FGFR-1 activation leads to irreversible prostate adenocar-cinoma and an epithelial-to-mesenchymal transition. Cancer Cell2007;12:559–71.
46. Birrer MJ, Johnson ME, Hao K, Wong K-K, Park D-C, Bell A, et al.Whole genome oligonucleotide-based array comparative genomichybridization analysis identified fibroblast growth factor 1 as aprognostic marker for advanced-stage serous ovarian adenocarci-nomas. J Clin Oncol 2007;25:2281–7.
47. Elagoz S, Egilmez R, Koyuncu A, Muslehiddinoglu A, Arici S. Theintratumoral microvessel density and expression of bFGF and nm23-H1 in colorectal cancer. Pathol Oncol Res 2006;12:21–7.
48. George ML, Tutton MG, Abulafi AM, Eccles SA, Swift RI. Plasmabasic fibroblast growth factor levels in colorectal cancer: a clinicallyuseful assay? Clin Exp Metastasis 2002;19:735–8.
49. Poon RT-P, Fan S-T, Wong J. Clinical implications of circulatingangiogenic factors in cancer patients. J Clin Oncol 2001;19:1207–25.
50. Presta M, Dell’Era P, Mitola S, Moroni E, Ronca R, Rusnati M.Fibroblast growth factor/fibroblast growth factor receptor systemin angiogenesis. Cytokine Growth Factor Rev 2005;16:159–78.
51. Cavallaro U, Niedermeyer J, Fuxa M, Christofori G. N-CAM mod-ulates tumour-cell adhesion to matrix by inducing FGF-receptorsignalling. Nat Cell Biol 2001;3:650–7.
52. Perl AK, Dahl U, Wilgenbus P, Cremer H, Semb H, Christofori G.Reduced expression of neural cell adhesion molecule induces met-astatic dissemination of pancreatic beta tumor cells. Nat Med1999;5:286–91.
53. Folkman J, Klagsbrun M, Sasse J, Wadzinski M, Ingber D, VlodavskyI. A heparin-binding angiogenic protein—basic fibroblast growthfactor—is stored within basement membrane. Am J Pathol 1988;130:393–400.
54. Ingber DE, Folkman J. Mechanochemical switching between growthand differentiation during fibroblast growth factor-stimulated angio-genesis in vitro: role of extracellular matrix. J Cell Biol 1989;109:317–30.
55. Werner S, Grose R. Regulation of wound healing by growth factorsand cytokines. Physiol Rev 2003;83:835–70.
56. Abraham JA, Whang JL, Tumolo A, Mergia A, Friedman J, Gospo-darowicz D, et al. Human basic fibroblast growth factor: nucleotidesequence and genomic organization. EMBO J 1986;5:2523–8.
57. Greenhalgh DG, Sprugel KH, Murray MJ, Ross R. PDGF and FGFstimulate wound healing in the genetically diabetic mouse. Am JPathol 1990;136:1235–46.
58. Broadley KN, Aquino AM, Woodward SC, Buckley-Sturrock A, SatoY, Rifkin DB, et al. Monospecific antibodies implicate basic fibroblastgrowth factor in normal wound repair. Lab Invest 1989;61:571–5.
59. Risau W. Angiogenic growth factors. Prog Growth Factor Res1990;2:71–9.
60. Pepper MS, Ferrara N, Orci L, Montesano R. Potent synergismbetween vascular endothelial growth factor and basic fibroblastgrowth factor in the induction of angiogenesis in vitro. BiochemBiophys Res Commun 1992;189:824–31.
61. Compagni A, Wilgenbus P, Impagnatiello M-A, Cotten M, ChristoforiG. Fibroblast growth factors are required for efficient tumor angio-genesis. Cancer Res 2000;60:7163–9.
62. Javerzat S, Auguste P, Bikfalvi A. The role of fibroblast growth factorsin vascular development. Trends Mol Med 2002;8:483–9.
63. Gualandris A, Urbinati C, Rusnati M, ZicheM, PrestaM. Interaction ofhigh-molecular-weight basic fibroblast growth factor with endothe-lium: biological activity and intracellular fate of human recombinantM(r) 24,000 bFGF. J Cell Physiol 1994;161:149–59.
Inhibition of the FGF Pathway and Antiangiogenic Therapy
www.aacrjournals.org Clin Cancer Res; 17(19) October 1, 2011 6137
on June 8, 2020. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 27, 2011; DOI: 10.1158/1078-0432.CCR-11-0659

64. Ribatti D, Urbinati C, Nico B, Rusnati M, Roncali L, Presta M.Endogenous basic fibroblast growth factor is implicated in thevascularization of the chick embryo chorioallantoic membrane.Dev Biol 1995;170:39–49.
65. Passaniti A, Taylor RM, Pili R, Guo Y, Long PV, Haney JA, et al. Asimple, quantitative method for assessing angiogenesis and anti-angiogenic agents using reconstituted basement membrane, hep-arin, and fibroblast growth factor. Lab Invest 1992;67:519–28.
66. Ensoli B, Gendelman R, Markham P, Fiorelli V, Colombini S, RaffeldM, et al. Synergy between basic fibroblast growth factor and HIV-1Tat protein in induction of Kaposi's sarcoma. Nature 1994;371:674–80.
67. Wang Y, Becker D. Antisense targeting of basic fibroblast growthfactor and fibroblast growth factor receptor-1 in human melanomasblocks intratumoral angiogenesis and tumor growth. Nat Med1997;3:887–93.
68. Fujii T, Kuwano H. Regulation of the expression balance of angio-poietin-1 and angiopoietin-2 by Shh and FGF-2. In Vitro Cell Dev BiolAnim 2010;46:487–91.
69. Ensoli B, Nakamura S, Salahuddin SZ, Biberfeld P, Larsson L, BeaverB, et al. AIDS-Kaposi's sarcoma-derived cells express cytokineswith autocrine and paracrine growth effects. Science 1989;243:223–6.
70. Abuharbeid S, Czubayko F, Aigner A. The fibroblast growth factor-binding protein FGF-BP. Int J Biochem Cell Biol 2006;38:1463–8.
71. Tassi E, Al-Attar A, Aigner A, Swift MR, McDonnell K, Karavanov A,et al. Enhancement of fibroblast growth factor (FGF) activity by anFGF-binding protein. J Biol Chem 2001;276:40247–53.
72. Aigner A, Butscheid M, Kunkel P, Krause E, Lamszus K, WellsteinA, et al. An FGF-binding protein (FGF-BP) exerts its biologicalfunction by parallel paracrine stimulation of tumor cell and endo-thelial cell proliferation through FGF-2 release. Int J Cancer 2001;92:510–7.
73. Czubayko F, Liaudet-Coopman EDE, Aigner A, Tuveson AT,Berchem GJ, Wellstein A. A secreted FGF-binding protein can serveas the angiogenic switch in human cancer. Nat Med 1997;3:1137–40.
74. P�aez-Ribes M, Allen E, Hudock J, Takeda T, Okuyama H, Viñals F,et al. Antiangiogenic therapy elicits malignant progression of tumorsto increased local invasion and distant metastasis. Cancer Cell2009;15:220–31.
75. Hurwitz H, Fehrenbacher L, Novotny W, Cartwright T, Hainsworth J,Heim W, et al. Bevacizumab plus irinotecan, fluorouracil, and leu-covorin for metastatic colorectal cancer. N Engl J Med 2004;350:2335–42.
76. Tille JC, Wood J, Mandriota SJ, Schnell C, Ferrari S, Mestan J, et al.Vascular endothelial growth factor (VEGF) receptor-2 antagonistsinhibit VEGF- and basic fibroblast growth factor-induced angiogen-esis in vivo and in vitro. J Pharmacol Exp Ther 2001;299:1073–85.
77. Giavazzi R, Sennino B, Coltrini D, Garofalo A, Dossi R, Ronca R, et al.Distinct role of fibroblast growth factor-2 and vascular endothelialgrowth factor on tumor growth and angiogenesis. Am J Pathol2003;162:1913–26.
78. Shi YH, Bingle L, Gong LH, Wang YX, Corke KP, Fang WG. BasicFGF augments hypoxia induced HIF-1-alpha expression and VEGFrelease in T47D breast cancer cells. Pathology 2007;39:396–400.
79. Nissen LJ, Cao R, Hedlund E-M, Wang Z, Zhao X, Wetterskog D,et al. Angiogenic factors FGF2 and PDGF-BB synergistically pro-mote murine tumor neovascularization and metastasis. J Clin Invest2007;117:2766–77.
80. Shen J, Vil MD, Prewett M, Damoci C, Zhang H, Li H, et al. Devel-opment of a fully human anti-PDGFRbeta antibody that suppressesgrowth of human tumor xenografts and enhances antitumor activityof an anti-VEGFR2 antibody. Neoplasia 2009;11:594–604.
81. Pietras K, Pahler J, Bergers G, Hanahan D. Functions of paracrinePDGF signaling in the proangiogenic tumor stroma revealed bypharmacological targeting. PLoS Med 2008;5:e19.
82. Casanovas O, Hicklin DJ, Bergers G, Hanahan D. Drug resistance byevasion of antiangiogenic targeting of VEGF signaling in late-stagepancreatic islet tumors. Cancer Cell 2005;8:299–309.
83. Allen E, Walters I, Hanahan D. Brivanib, a dual FGF/VEGF Inhibitor, isactive both first and second line against mouse pancreatic neuro-endocrine tumors developing adaptive/evasive resistance to VEGFinhibition. Clin Cancer Res 2011;17:5299–5310.
84. Fernando NT, Koch M, Rothrock C, Gollogly LK, D’Amore PA,Ryeom S, et al. Tumor escape from endogenous, extracellularmatrix-associated angiogenesis inhibitors by up-regulation of mul-tiple proangiogenic factors. Clin Cancer Res 2008;14:1529–39.
85. Bello E, Colella G, Scarlato V, Oliva P, Berndt A, Valbusa G, et al. E-3810 is a potent dual inhibitor of VEGFR and FGFR that exertsantitumor activity in multiple preclinical models. Cancer Res2011;71:1396–405.
86. Kopetz S, Hoff M, Eng C, Overman M, Glover K, Chang Z, et al.Levels of angiogenic cytokines prior to disease progression inmetastatic colorectal cancer patients treated with bevacizumab.Gastrointestinal Cancers Symposium; 2009 Jan 15–17; San Fran-cisco, CA; 2009.
87. Kopetz S, Hoff PM, Morris JS, Wolff RA, Eng C, Glover KY, et al.Phase II trial of infusional fluorouracil, irinotecan, and bevacizumabfor metastatic colorectal cancer: efficacy and circulating angiogenicbiomarkers associated with therapeutic resistance. J Clin Oncol2009;24:8252.
88. Willett CG, Duda DG, di Tomaso E, Boucher Y, Ancukiewicz M,Sahani DV, et al. Efficacy, safety, and biomarkers of neoadjuvantbevacizumab, radiation therapy, and fluorouracil in rectal cancer: amultidisciplinary phase II study. J Clin Oncol 2009;27:3020–6.
89. Batchelor TT, Sorensen AG, di Tomaso E, Zhang W-T, Duda DG,Cohen KS, et al. AZD2171, a pan-VEGF receptor tyrosine kinaseinhibitor, normalizes tumor vasculature and alleviates edema inglioblastoma patients. Cancer Cell 2007;11:83–95.
90. Garrett CR, Siu LL, Giaccone G, El-Khoueiry A, Marshall J, LoRussoP, et al. A phase I study of BMS-582664 (brivanib alaninate), an oraldual inhibitor of VEGFR and FGFR tyrosine kinases, in combinationwith full-dose cetuximab in patients with advanced gastrointestinalmalignancies who failed prior therapy. J Clin Oncol 2007;25(18S):14018.
91. Matsui J, Yamamoto Y, Funahashi Y, Tsuruoka A, Watanabe T,Wakabayashi T, et al. E7080, a novel inhibitor that targets multiplekinases, has potent antitumor activities against stem cell factorproducing human small cell lung cancer H146, based on angiogen-esis inhibition. Int J Cancer 2008;122:664–71.
92. Zhang H, Masuoka L, Baker K, Sadra A, Bosch E, Brennan T, et al.FP-1039 (FGFR1:Fc), a soluble FGFR1 receptor antagonist, inhibitstumor growth and angiogenesis. AACR-NCI-EORTC InternationalConference; 2007 Oct 22–26; San Francisco, CA; 2007.
93. Jonker DJ, Rosen LS, Sawyer MB, de Braud F, Wilding G, SweeneyCJ, et al. A phase I study to determine the safety, pharmacokineticsand pharmacodynamics of a dual VEGFR and FGFR inhibitor, bri-vanib, in patients with advanced or metastatic solid tumors. AnnOncol 2011;22:1413–9.
94. Okamoto I, Kaneda H, Satoh T, Okamoto W, Miyazaki M, MorinagaR, et al. Phase I safety, pharmacokinetic, and biomarker study of bibf1120, an oral triple tyrosine kinase inhibitor in patients with advancedsolid tumors. Mol Cancer Ther 2010;9:2825–33.
95. Sun HD, Malabunga M, Tonra JR, DiRenzo R, Carrick FE, ZhengH, et al. Monoclonal antibody antagonists of hypothalamic FGFR1cause potent but reversible hypophagia and weight loss inrodents and monkeys. Am J Physiol Endocrinol Metab 2007;292:E964–76.
96. Sarker D, Molife R, Evans TR, Hardie M, Marriott C, Butzberger-Zimmerli P, et al. A phase I pharmacokinetic and pharmacodynamicstudy of TKI258, an oral, multitargeted receptor tyrosine kinaseinhibitor in patients with advanced solid tumors. Clin Cancer Res2008;14:2075–81.
97. Shimada T, Kakitani M, Yamazaki Y, Hasegawa H, Takeuchi Y, FujitaT, et al. Targeted ablation of Fgf23 demonstrates an essentialphysiological role of FGF23 in phosphate and vitamin D metabolism.J Clin Invest 2004;113:561–8.
98. Greulich H, Pollock PM. Targeting mutant fibroblast growth factorreceptors in cancer. Trends Mol Med 2011;17:283–92.
Lieu et al.
Clin Cancer Res; 17(19) October 1, 2011 Clinical Cancer Research6138
on June 8, 2020. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 27, 2011; DOI: 10.1158/1078-0432.CCR-11-0659

99. Saltz LB, Clarke S, Díaz-Rubio E, Scheithauer W, Figer A, Wong R,et al. Bevacizumab in combination with oxaliplatin-basedchemotherapy as first-line therapy in metastatic colorectal cancer:a randomized phase III study. J Clin Oncol 2008;26:2013–9.
100. Jain RK, Duda DG, Willett CG, Sahani DV, Zhu AX, Loeffler JS, et al.Biomarkers of response and resistance to antiangiogenic therapy.Nat Rev Clin Oncol 2009;6:327–38.
101. Murukesh N, Dive C, Jayson GC. Biomarkers of angiogenesis andtheir role in the development of VEGF inhibitors. Br J Cancer2010;102:8–18.
102. Chun YS, Vauthey JN, Boonsirikamchai P, Maru DM, Kopetz S,Palavecino M, et al. Association of computed tomography morpho-logic criteria with pathologic response and survival in patientstreated with bevacizumab for colorectal liver metastases. JAMA2009;302:2338–44.
103. Ocaña A, Amir E, Vera F, Eisenhauer EA, Tannock IF. Addition ofbevacizumab to chemotherapy for treatment of solid tumors:similar results but different conclusions. J Clin Oncol 2011;29:254–6.
104. Santos ES, Gomez JE, Raez LE. Targeting angiogenesis from mul-tiple pathways simultaneously: BIBF 1120, an investigational noveltriple angiokinase inhibitor. Invest New Drugs 2011. [Epub ahead ofprint] 25 Feb 2011.
105. Dempke WCM, Zippel R. Brivanib, a novel dual VEGF-R2/bFGF-Rinhibitor. Anticancer Res 2010;30:4477–83.
106. Yamada K, Yamamoto N, Yamada Y, Nokihara H, Fujiwara Y, HirataT, et al. Phase I dose-escalation study and biomarker analysis ofE7080 in patients with advanced solid tumors. Clin Cancer Res2011;17:2528–37.
107. Ueda Y, Shimoyama T, Murakami H, Yamamoto N, Yamada Y,Arioka H, et al. Phase I and pharmacokinetic study of TSU-68, anovel multiple receptor tyrosine kinase inhibitor, by twice daily oraladministration between meals in patients with advanced solidtumors. Cancer Chemother Pharmacol 2011;67:1101–9.
108. Gavine P, Mooney L, Kilgour E, Thomas A, Al-Kadhimi K, Beck S,et al. Characterization of AZD4547: An orally bioavailable, potent andselective inhibitor of FGFR tyrosine kinases 1, 2, and 3. 102nd AACRAnnual Meeting; 2011 Apr 2–6; Orlando, FL; 2011.
109. Harding T, Palencia S, Long L, Finer J, Keer H, Baker K, et al.Preclinical efficacy of FP-1039 (FGFR1:Fc) in endometrial carcinomamodels with activating mutations in FGFR2. American AACR AnnualMeeting; 2010 Apr 17–21; Washington, DC; 2010.
110. ClinicalTrials.gov. Bethesda (MD): NIH; 2011. Novartis. A doseescalation study in adult patients with advanced solid malignancies.NCT01004224. Available from: http://clinicaltrials.gov/ct2/show/NCT01004224.
111. Saxty G, Akkari R, Angibaud P, Arts J, Benderitter P, Berdini V, et al.Fragment based drug discovery of selective inhibitors of fibroblastgrowth factor receptor (FGFR). 102nd AACR Annual Meeting; 2011Apr 2–6; Orlando, FL; 2011.
Inhibition of the FGF Pathway and Antiangiogenic Therapy
www.aacrjournals.org Clin Cancer Res; 17(19) October 1, 2011 6139
on June 8, 2020. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 27, 2011; DOI: 10.1158/1078-0432.CCR-11-0659

2011;17:6130-6139. Published OnlineFirst September 27, 2011.Clin Cancer Res Christopher Lieu, John Heymach, Michael Overman, et al. and AntiangiogenesisBeyond VEGF: Inhibition of the Fibroblast Growth Factor Pathway
Updated version
10.1158/1078-0432.CCR-11-0659doi:
Access the most recent version of this article at:
Cited articles
http://clincancerres.aacrjournals.org/content/17/19/6130.full#ref-list-1
This article cites 103 articles, 33 of which you can access for free at:
Citing articles
http://clincancerres.aacrjournals.org/content/17/19/6130.full#related-urls
This article has been cited by 22 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://clincancerres.aacrjournals.org/content/17/19/6130To request permission to re-use all or part of this article, use this link
on June 8, 2020. © 2011 American Association for Cancer Research. clincancerres.aacrjournals.org Downloaded from
Published OnlineFirst September 27, 2011; DOI: 10.1158/1078-0432.CCR-11-0659