
Beyond the SCM - caduceushandouts.comcaduceushandouts.com/csm/2016/handouts/pedAPTA-2232193.pdf ·...
29
Reprints not permitted 1 Beyond the SCM: Anatomy of the Neck and Its Clinical Implications Jean Anne Zollars, PT, DPT, MA www.jazollarspt.com www.barralinstitute.com Anjali Gupta, PT, MS Disclosure The presenters declare no conflict of interest or bias in the content of this presentation. Objectives 1. Identify anatomical structures of the neck and thoracic inlet: muscles, fascia, organs, nerves, arteries, and bones 2. Identify physiological, functional and symptomatic issues associated with tightness in the above structures in infants and children. 3. Identify clinical implications in regards to treatment of infants and children, focusing on stretching, positioning, AROM, and developmental treatment.
-
Upload
truonghuong -
Category
Documents
-
view
221 -
download
3
Transcript of Beyond the SCM - caduceushandouts.comcaduceushandouts.com/csm/2016/handouts/pedAPTA-2232193.pdf ·...

Reprints not permitted 1
Beyond the SCM: Anatomy of the Neck and Its
Clinical Implications
Jean Anne Zollars, PT, DPT, MA
www.jazollarspt.com www.barralinstitute.com
Anjali Gupta, PT, MS
Disclosure
The presenters declare no conflict of interest or bias in
the content of this presentation.
Objectives
1. Identify anatomical structures of the neck and
thoracic inlet: muscles, fascia, organs, nerves,
arteries, and bones
2. Identify physiological, functional and symptomatic
issues associated with tightness in the above
structures in infants and children.
3. Identify clinical implications in regards to treatment
of infants and children, focusing on stretching,
positioning, AROM, and developmental treatment.

Reprints not permitted 2
Outline
• Anatomical review with self-palpation of
neck/supraclavicular structures
• Discussion of symptomology to be aware of
with overstretching/compression of
neurovascular structures
• Clinical implications, evaluative procedures,
treatment suggestions
• Case studies
• Summary & Questions
• Anatomy of neck: muscle and fascial layers
• Neurovascular anatomy through layers
-accessory n
-cervical nerves
-ant neck & trachea/vagus
-subclavian a
-brachial plexus
• Signs of overstretching nerves: phrenic,
brachial plexus, vagus, cervical plexus
Anatomy of neck
• Muscle and fascial layers
• Neurovascular anatomy through layers
-accessory n
-cervical nerves
-ant neck & trachea/vagus
-subclavian a
-brachial plexus

Reprints not permitted 3
Cervical Fascia
• Tubes within tubes
• Anteriorly: visceral sheath (trachea, esophagus, thyroid)
• Posteriorly: vertebrae
• Laterally: blood vessels
• Muscles and fascia
Illustration by Frank Lowen
Sternocleidomastoid
Superficial cervical fascia
Trapezius
Platysma
Superficial cervical fascia: Loose, disorganized connective
tissue. Surrounds external jugular vein.
(13)
Illustration by Frank Lowen
Self-palpation
Sternocleidomastoid: Manubrium of sternum & medial clavicle
to mastoid process of temporal bone & via aponeurosis to lateral
½ of superior nuchal line of occiput. (Palpate sup to inf)
Trapezius: Med 1/3 superior nuchal line of occiput, SP C1-C7,
T1-T12 to acromium to lat 1/3 clavicle, acromium, scapular spine

Reprints not permitted 4
(Punctum nervosum)
Punctum Nervosum: sensory branches of cervical
plexus nerves emerge at posterior border of SCM (at
C3 level)
Self-palpation: From angle of mandible, go posterior to SCM &
Inferior 1 vertebral level to feel for punctum nervosum
(C2)
(C2,C3)
Cervical Plexus: sensory
innervation to…
• Lesser occipital nerve: scalp posterior to
ear
• Greater auricular nerve: scalp/skin of
mastoid process & parotid gland, outer ear
• Deep transverse cervical nerve: skin of
ant/lat neck
• Supraclaviclavicular nerves: skin above &
below the clavicle
Spinal Accessory Nerve
• Cranial root: origin medulla
• Spinal root: origin - lat aspect of ventral horn in spinal cord from 6th cervical segment to junction of spinal cord with medulla. The fibers go sup through foramen magnum
• Spinal root joins with cranial root, exiting thru jugular foramen
• Gray’s Anatomy, 40th Edition, p.459 (Standring 2008)
*Manual Therapy of the Cranial Nerves by
Barral and Croibier.Barral Productions.
Illustration © Elsevier Masson and Éléonore Lamoglia.*

Reprints not permitted 5
Spinal Accessory Nerve
• Pierces SCM 3 cm from mastoid process (@ level of C3, behind angle of mandible)
• Within SCM, SAN receives branches of C2-C3, creating Ansa of Maubrac
• Exits SCM at posterior border at level of hyoid/C4
(Kierner A et al 2000, Dailiana et al, 2001)
Self-palpation: from C3 (punctum
nervosum, palpate within belly of SCM
*https://upload.wikimedia.org/wikipedia/common
s/4/4b/Gray793.png
Suboccipital nerve: (C1 posterior
branch) innervates rectus
capitus posterior minor between
occiput/C1 (connected to
spinal duramater)& vertebral
artery
Greater occipital nerve: innervates posterior
cranial dura, scalp & pierces trapezius
*Manual Therapy of the Cranial Nerves by
Barral and Croibier.Barral Productions.
Illustration © Elsevier Masson and Éléonore Lamoglia.*
Self-palpation: Find Greater
Occipital N & C2 Posterior N
• From sup nuchal line (midine @ EOP), go 1 finger lat, 2 fingers inf
• (If feel pulse of > occ artery, just go medially)
• Find C2 nerve: from C2 spinous process, go laterally & cephalad into laminar groove to feel nerve & bud
*Manual Therapy of the Cranial Nerves by
Barral and Croibier.Barral Productions.
Illustration © Elsevier Masson and Éléonore Lamoglia.*

Reprints not permitted 6
Mid-cervical fascia
Fascia of infrahyoid muscles and pretracheal fascia
Attachments:
-Sup: hyoid
-Inf: upper border of scapula near the scapular notch (origin of omohyoid), post edge of clavicle, scalene tubercle and cartilage of rib 1, medial clavicle and post sternum.
Functions:
-Orients the hyoid muscles
-Surrounds all veins (brachiocephalic, thyroid, subclavian), thus maintains the patency of veins
*The Thorax. Barral JP 1991. Eastland Press. p 27
Thieme Lat view hyoid

Reprints not permitted 7
Middle cervical fascia
Omohyoid
Sternohyoid
Sternothyroid
Self-palpation: Superficial & Middle Cervical Fascia
Superficial
cervical fascia
Illustration by Frank Lowen
Visceral Sheath: Contains trachea, esophagus
& thyroid gland
Visceral sheath:
Vascular sheath:
• Thyroid gland
• Trachea
• Esophagus
Carotid artery
Jugular vein
Vagus nerve
Self-palpation: With back of your fingers, gently feel trachea. Swallow, that
movement is esophagus. Just lateral & posterior, feel pulse of carotid artery
Within the vascular sheath with jugular vein & vagus nerve
Illustration by Frank Lowen

Reprints not permitted 8
Jugular vein
Carotid artery
Vagus nerve
Vascular Sheath
Vagus Nerve
Deep Cervical/Prevertebral Fascia (32 &
handout)• Covers longus colli,
longus capitus and scalenes
• Deepest part goes from occiput to T3, where if fuses with ant long lig
• Anterior scalene attaches to tubercle of 1st rib
• Finding anterior scalene or subclavian artery can guide us to brachial plexus, pleural dome
Anterior scalene
Middle scalene Longus colli

Reprints not permitted 9
Deep cervical fascia
Longus colli
Anterior scalene
Medial and
(Prevertebral fascia)
posterior scalene
Levator scapula
Illustration by Frank Lowen
Self palpation of anterior scalene
Sit slouched. Backs of fingers 2-4 between 2 heads of a
of SCM. Feel TPs. Follow sternal head to sternum. Post
is ant scalene.
*Clemente (1997) Anatomy p.448
• Mostly C4, some C3, C5• Mixed motor (diaphragm) & sensory• Sensory: pericardium, pleura,
diaphragm, upper peritoneum.
• Connects to: subclavian n, stellate ganglion, vagus, hypoglossal, and sympathetic nerves of the neck.
Phrenic Nerve
*Manual Therapy of the Peripheral Nerves by
Barral and Croibier.Barral Productions.
Illustration © Elsevier Masson and Éléonore Lamoglia.*

Reprints not permitted 10
Subclavian
artery & brachial
plexus descend
posterior to
clavicle, between
clavicle &1st rib
Consider implications
of compression
on clavicle when
stretching
Subclavian
artery & brachial
plexus pass under
pectoralis minor
Consider tension
of pectoralis minor
Muscle Spindle Physiology• Intrafusal Muscle Fibers:
fibers of muscle responsible
for sensing the muscle
length and, the rate of
change of muscle length.
Sensory organ within
intrafusal fiber = muscle
spindles
• Extrafusal Muscle Fibers:
responsible for muscle
contraction
*Positional Release Therapy: D’Ambrogio & Roth. Mosby 1997

Reprints not permitted 11
Muscle Spindle Physiology• When muscle stretched,
impulses go to spinal cord
(via Ia & II neurons)
• Synapse in ventral horn of
spinal cord
• Gamma motor neurons
send impulses to muscle
spindle to contract spindle
as a protective mechanism
so muscle does not get
overstretched or torn
• Alpha motor neurons send
impulses to extrafusal
fibers to contract
*Positional Release Therapy: D’Ambrogio & Roth.
Mosby 1997
Gamma Gain• In resting conditions, gamma motor
neurons maintain a level of
discharge into the intrafusal muscle
fibers, such that there is always
some muscle tone (not flaccid).
• Gamma motor neurons are like a
volume control, creating more or
less background tension in the
muscle.
• Gamma motor neurons are under
control of the bulboreticular
formation of the brainstem
• So, if too much gamma gain, person
has high resting tension in muscle,
or in CNS lesion, spasticity
• If someone has more activated
ANS, normal resting muscle tone is
higher
*Positional Release Therapy: D’Ambrogio &
Roth. Mosby 1997
What happens with muscle spasm?• If the muscle is quickly stretched or
overstretched, impulses are sent back via Ia
afferents to spinal cord at that level, above
& below, & to brain.
• Gamma motor neurons send impulses back
to intrafusal muscle fibers to further
contract muscle to protect it from injury
• If gamma activation continues or is higher
than usual, muscle spasm continues
*Positional Release Therapy: D’Ambrogio &
Roth. Mosby 1997

Reprints not permitted 12
Nocioceptors: Pain receptors• Found in body’s connective
tissues including muscles
ligaments, tendons, joint
capsules, the outer wall of all
larger blood vessels, visceral
fascia (peritoneum) and in the
neural fascia (epineurium/dura).
(Schleip, R 2003)
• Nocioceptive reflex is spinal
reflex, such that if you touch a
hot burner, you quickly take
your hand off.
Peripheral Nerve Innervation
Nervi nervorum – nerve of nerve
2 types:
Sympathetic fibers: -Around arteries, regulating
vascularization due to diameter
change
Multinodal fibers:-Innervates CT of peripheral n’s,
n roots, & ANS/visceral NS
-Nerve monitors its own
sensitivity & nocioception
-Neuropathic pain
Peripheral Nerve
*Manual Therapy of the Peripheral Nerves by Barral and
Croibier.Barral Productions. Illustration © Elsevier and Hardlines.*
Nocifensive Reflexes
• Nocifensive reflexes: muscle contracts in response to
nociceptor activation (pain) in the involved tissues. (How
the body protects inflamed or damaged tissues).
• Nociautonomic reflexes are neural connections to the
autonomic nervous system that can result in autonomic
responses such as vasodilation, bronchodilation, or
gastrointestinal stasis. Skeletal muscle, for example, (due
to the presence of beta adrenoreceptors) will “engorge” or
swell under the influence of these reflexes due to the
release of chemicals such as histamine and bradykinin.
(Van Buskirk RL 1990)

Reprints not permitted 13
Noxious Stimulus
Nocioceptor Vasodilation & Tissue
EdemaSpinal Cord
Nocifensive Reflexes
Skeletal Muscle Shortened
Maintain Shortening
Connective Tissue Reorganized
In Shortened Form
Sympathetic
Activation
Model of Nociceptive Origin & Maintenance of
Somatic Dysfunction
(Modified from Van Buskirk RL 1990)
Inappropriate Stretching
• Gamma gain is high
causing increased muscle
spasm
• Nociceptive reflex
activated: pain &
increased muscle spasm
• Nociautonomic reflex
activated
*The American College of Sports Medicine recommends that for maximal effect, stretching should NOT exceed the point of discomfort.(Garber et al 2011)
(Punctum nervosum)
Revisiting nerves and muscles…what are we
stretching?

Reprints not permitted 14
*Manual Therapy of the Cranial Nerves by Barral and Croibier.Barral Productions.
Illustration © Elsevier Masson and Éléonore Lamoglia.*
Phrenic Nerve
Manual Therapy of the Peripheral Nerves by Barral and Croibier. Barral
Productions. Illustration © Elsevier and Hardlines.*
Brachial
plexus
Subclavian
artery
Consider implications
of compression
on clavicle when
stretching

Reprints not permitted 15
Signs of Possible Irritation/Compression
of Nerves in Neck/Supraclavicular Area
• Punctum nervosum: increased sensitivity to
skin in and around lateral neck, scalp, head
• Greater occipital (posterior branch of C2):
increased tension in posterior trap, sensitivity in
back of scalp
• Phrenic: hiccupping, diaphragmatic spasm
• Accessory: increased tightness in SCM, trap
• Brachial plexus: Tension around shoulder, may
contribute to difficulty weight bearing in prone
Appropriate Stretch: Clinical
Practice Guidelines (Kaplan et al 2013)
• Stretch without stimulating the nocioceptors and
nervi nervorum (stretch without causing pain)
(Van Buskirk RL 1990, van Vlimmerman 2006,
Taylor 1997)
• Low-intensity, sustained , pain-free stretches to
avoid microtrauma (van Vlimmerman 2006)
• If the baby is crying, neck ROM does not increase,
muscle tightness still present, your stretching is
not helping.
Physiology of Stretching
• Muscle afferents responsible for cardiovascular changes:
• Group III – mechanoreceptors – sensitive to mechanical forces.
• Group IV – metaboreceptors – sensitive to metabolic changes.
• Elicit cardiovascular changes through parasympathetic withdrawal (tachycardia) and sympathetic activation (HR).
• (Drew 2008, Fisher 2005, Gladwell 2002, Farinatti 2011)
• Valsalva maneuver (VM) reduces the venous return, cardiac output (induces a baroreflex responses) and increases BP.
(Farinatti 2011, Lima 2011)

Reprints not permitted 16
The nucleus of the tractus solitaries receives afferents from the carotid baroreceptors via the glossopharyngeal nerve and from the aortic baroreceptors from the vagus nerve (Klingler
2014) .
www.studyhttpsblue.com/notes/note/n/1-
vascularphysiology-4/deck/12427959
Vagus Nerve
• Sensory from ear, pharynx, larynx, palate, face, epiglottis, esophagus, lungs, abdominal viscera
• Motor to pharynx, larynx, palate, thoracic & abdominal viscera
Esophagus
Gastroesophageal
junction
Stomach
Vagus Nerve
Illustration by Frank Lowen
Vagus Nerve
• Important part of the ANS
• Often involved with dysregulation of the ANS
• Viewed as a modulator of the nervous system in the field of neuropsychology (Polyvagal theory, Porges,1999, 2001, 2007, 2009 )
48

Reprints not permitted 17
Signs of ANS dysregulation/vagal nerve
• Digestion issues: reflux, bloating, gas, constipation• Baby with irritability• Baby who is easily overwhelmed• Baby who is not sleeping well• Baby who does not want to make eye contact, or with
vacant eyes, dissociating.• Baby who is tacitely defensive (pulling away, muscles
tightening).• Baby with breathing difficulties, or noisy breathing.
49
Reprinted with permission from John W. Kimball
Nerve Reflexes to consider
• Laryngeal Cough Reflex: Yim et al (2010) demonstrated that irritation of the internal branch of the superior laryngeal nerve (branch of vagus nerve) causes a cough and a color change.
Reprints not permitted 18
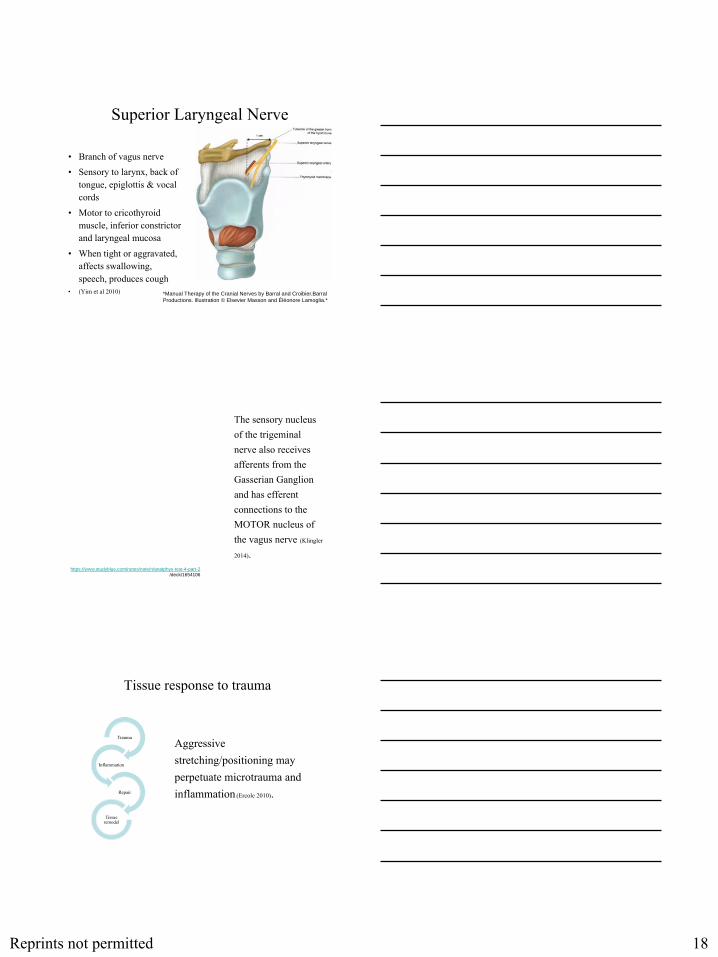
Superior Laryngeal Nerve
• Branch of vagus nerve
• Sensory to larynx, back of tongue, epiglottis & vocal cords
• Motor to cricothyroid muscle, inferior constrictor and laryngeal mucosa
• When tight or aggravated, affects swallowing, speech, produces cough
• (Yim et al 2010) *Manual Therapy of the Cranial Nerves by Barral and Croibier.Barral
Productions. Illustration © Elsevier Masson and Éléonore Lamoglia.*
https://www.studyblue.com/notes/note/n/anatphys-test-4-part-2
/deck/1654106
The sensory nucleus of the trigeminal nerve also receives afferents from the Gasserian Ganglion and has efferent connections to the MOTOR nucleus of the vagus nerve (Klingler
2014).
Tissue response to trauma
Aggressive stretching/positioning may perpetuate microtrauma and inflammation (Ercole 2010).
Trauma
Inflammation
Repair
Tissue remodel

Reprints not permitted 19
Habitual posture/chronic
tissue deformation
Localized tissue ischemia or edema
Scarring of soft tissue leading to
trigger point/nodule
Connective Tissue Tightness Mechanism
WHOLE BODY ASSESSMENT
Beyond the SCM: What else do you notice?
• Elevated shoulder• Flared ribs• Internally rotated shoulder• Trunk flexion• Elevated pelvis• Increased hip external rotation and
abduction• Tibial internal rotation• Tightness through metatarsals/metacarpals

Reprints not permitted 20
SURROUNDING THE NECK
Fascial tightness Upper trap
is prominent while SCM is being stretched
Fascia has contractile ability
• Straubesand et al (1996) verified the ability of human fascia to actively contract and identified the presence of myofibroblasts or smooth muscle cells embedded within the fascia itself (Yahia LH, et. al (1993), Straubesand J, et. al, 1996).
• Subsequent experiments performed by Schleip in 2006 verified the presence of Type III and IV sensory endings, autonomic nerve fibers and contractile cells in fascia
Alternatives to Manual Stretching
• Myofascial release
• Joint Blocking
• Elastic Taping
• Positional release
• Neural manipulation

Reprints not permitted 21
MYOFASCIAL RELEASE
FASCIA BASICS
• Fascia is comprised of:• connective tissue that surrounds and links bones, muscle, vessels and
nerves • smooth muscle cells, giving it the ability to contract
• Fascia also glides on itself; this allows for glide/shear between the structures it surrounds
• (Klingler 2014, Stecco 2013)
http://thewellnessdigest.com/fascia-the-unknown-factor-in-muscle-movement-and-soft-tissue-pain/
FASCIA BASICS
• Studies now show that fascia has a mechanical role in movement and force generation
• Additional myofascial units may be recruited over time if the original injury is not treated immediately (fibrosis)
• Tension causes the fascia to shorten and solidify anywhere along the line of pull
• Fascia will begin tightening down before changes are noticed in the muscle itself
(Klingler 2014, Stecco 2013)

Reprints not permitted 22
WHAT IS MYOFASCIAL RELEASE?
• A gentle sustained pressure to treat soft tissue dysfunction causing increased tissue heat to increase viscoelasticity (Stecco 2013, Mattein 2009, Stern
2006).
• Soft tissue dysfunction can include (Stecco 2013): – limited AROM/PROM, – soft tissue adhesions, soft tissue tightness, and/or postural or
alignment dysfunction.
• Does not add tension to the neurovascular bundle under or within the tissue being stretched.
MYOFASCIAL ASSESSMENT/TREATMENT
• Maintain body mechanics
• Use the flat of your hands, not your fingertips
• Lightly traction the skin in all directions (like a compass) to determine area of restriction
• Approximate maximally restricted tissues to allow realignment
ELASTIC TAPING

Reprints not permitted 23
ELASTIC/FLEXIBLE TAPING
• Principles of elastic taping make it a suitable modality for relaxing tight muscles/fascia.
• Depending on the degree of tightness and the patient’s tolerance, use relaxation techniques specific to the manufacturer
• Consider taping larger muscles due to skin sensitivity at the neck
ELASTIC TAPING
• Trim to fit patient’s size
• For muscle techniques: “Insertion to Origin in a lengthen position”
• Consider relaxing: cervical extensors if have a capital extension moment, traps, pectorals, latissimus, arm, trunk extensors, trunk fascia, leg
• Educate parents on cues of adverse reaction: stress cues, changes in eating/sleeping patterns, inconsolable
JOINT BLOCKING
• Uses positioning and body weight for a slow, low load “joint mobilization”
• Use to treat pelvic misalignment
• By correcting pelvic misalignment, you create normalized tissue length lower in the chain allowing for increased slack in the soft tissues higher in the chain.
• EXAMPLE: to correct an upslip, place a small towel roll under the upslip ischial tuberosity with the baby in supine. Can repeat as needed until neutral alignment is reached

Reprints not permitted 24
“Pseudotumors”: Tender
Points/Fascial tightness
• With fibrosis, there are vascular changes, often
edema, then ischemia, so these areas need
special consideration.
• In order to release these areas, often the
muscle/fascial/neural/vascular structure needs
to be shortened to decrease gamma bias, and
inhibit the nocioceptors, the nocifensive &
nociautonomic reflexes
Positional Release TechniquesThese techniques are the opposite of direct stretch, such that the
muscle or joint is moved towards comfort to allow muscle
spindles to rest & reduce nocioceptive activity. They all use
tender points (TPs) and position of comfort or ease. Differences:
• Strain-counterstrain: uses TPs and reports of decreased pain to
assess efficacy of treatment (Jones 1997)
• Functional positional release: uses TPs, but relies on decreased
muscle hypertonicity, not pain
• Facilitated positional release: indirect MFR, uses TPs, position
of ease, then distraction, shear, etc to further decrease tension
• Total motion release for tots: indirect treatment in position of
ease
Total Motion Release for Torticollis

Reprints not permitted 25
Positional Release Techniques
Research
Strain/counterstrain
• Systematic Review/meta-analysis: reduction of
pain TPs, no harm, only adults (Wong 2014)
• Decreased Hoffman reflex in patients with
Achilles tendonitis (Howell 2006) & plantar
fasciitis (Wynne 2006)
Neural Manipulation
• Neural Manipulation (NM)
is a gentle hands-on therapy
which helps to free up the
nerves and the connective
tissue around the nerves
(dura mater), the bones
around the brain (cranium)
so that the nervous system
functions better.
(Barral & Croibier 2007)
74
NM & UE Nerves
• NM can release compressed brachial plexus’ & UE nerves, thus allowing greater shoulder girdle mobility & UE to develop strength
• Gibson quotes Hilton, British anatomist and surgeon of the early 1800’s,“The same trunk of nerves whose branches supply a joint also supply muscles that move the joint and their articular insertions, as well as the skin covering the joint” (Gibson, 1955). 75

Reprints not permitted 26
NM/VM Neck & Thorax
By releasing:• Left vagus nerve: help
with protective muscle
spasm L lateral neck
• T1/T2, ribs 1 & 2: help
with retraction of L ribs,
scapula
76
By releasing C2 (greater occipital nerve, help to
release trapezius, C1, C2 and posterior cranial
duramater
77
*Manual Therapy of the Cranial Nerves by Barral and Croibier.Barral
Productions. Illustration © Elsevier Masson and Éléonore Lamoglia.*
By releasing:
• L Accessory N: help to
release and lengthen L
SCM, trapezius
• L Phrenic N: help to
release C3-C5, anterior
ribs and diaphragm
• L brachial plexus: help
to free clavicle, 1st rib,
anterior shoulder
tension78

Reprints not permitted 27
Neural Manipulation Research
• Most studies have been performed with “neural mobilization”, which is stretching the nerve through active movement along the nerve’s pathway. (This might be what we are doing with direct manual stretching of the neck).
• With Barral & Croibier’s neural manipulation, the neural restriction is first released gently in the “direction of ease”, where the tissues want to go, and only when the nerve is ready to lengthen, do you lengthen the nerve. One never fights with a nerve or tight tissue, otherwise the nerve tightens to protect itself.
79
Neural Mobilization/Stretching
Research in Adults• Much clinical research has been done by Barral, Croibier
(2007, 2009) and therapists trained in this technique; however, EBP is lacking both with adults and children.
• Chhabra’s study of 37 subjects with cervico-brachial pain concluded that neural tissue mobilization was a more effective treatment approach than cervical lateral glide (Chhabra et al., 2008).
• By using high-resolution ultrasound, Coppitiers and colleagues (2009) confirmed that the median nerve was longitudinally lengthened with six different neural stretching exercises.
• In a systematic review of 10 articles pertaining to neural mobilization, Ellis and Hing (2008) found current research to be lacking in the quantity and quality needed to support the use of neural mobilization.
80
WITH YOUR NEW RANGE
• Strengthen cervical flexors depending on age and tightness:
– Find the pacifier in either SL or supine depending on strength
– Visually attend to a toy at eye level then bring toy slowly down to chest area
– In sitting maintain a neutral pelvis while playing with toys at or below waist level

Reprints not permitted 28
Video
References• Barral J-P, Croibier A. Manual Therapy for the Peripheral Nerves. New York, NY: Churchill
Livingstone/Elsevier; 2007.
• Barral J-P, Croibier A. Manual Therapy for the Cranial Nerves. New York, NY: Churchill Livingstone/Elsevier; 2009.
• Chhabra D, Raja K, Ganesh B, Prabhu N. Effectiveness of neural tissue mobilization over cervical lateral glide in cervico-brachial pain syndrome - a randomized clinical trial. Indian J Physio OccTherapy. 2008;2(4)47-52.
• Coppitiers MW, Hough AD, Dilley A. Different nerve-gliding exercises induce different magnitudes of median nerve longitudnal excursion: an in vivo study using dynamic ultrasound imaging. J Orthop Sports Phys Ther. 2009;39(3);164-71.
• Dailiana ZH, Mehdian H, Gilbert A. Surgical anatomy of spinal accessory nerve: is trapezius functional deficit inevitable after division of the nerve? J Hand Surg. 2001;26:137–41.
• Drew RC, Bell MP, White MJ. Modulation of spontaneous baroreflex control of heart rate and indexes of vagal tone by passie calf muscle stretch during graded metaboreflex activation in humans. J Appl Physiol. 2008; 104:716-723.
• Ellis RF, Hing WA. Neural mobilization: a systematic review of randomized controlled trials with an analysis of therapeutic efficacy. J Man Manip Ther. 2008;16(1)8-22.
• Ercole B, Stecco A, Day JA, Stecco C. How much time is required to modify a fascial fibrosis? J of Bodyworks and Movement Therapies. 2010(14);318-325.
• Farinatti PTV, Brandao C, Soares PSP, Duarte AFA. Acute effects of stretching exercise on the heart rate variability in subjects with low flexibility levels. J of Strength and Conditioning Research. 2011;25(6): 1579-1585.
• Farinatti PTV, Soares PS, Monteiro WD, Duarte AFA, Viveiros de Castro LA. Cardiovascular responses to passive static flexibility exercises are influenced by the stretched muscle mass and the Valsalva maneuver. Clinics. 2011;66(3): 459-464.
• Fisher JP, Bell M, White MJ. Cardiovascular responses to human calf muscle stretch during varying levels of muscle metaboreflex activation. Exp Physiol. 2005;90:773-81.
• Garber CE, Blissmer B, Deschenes MR, et al; American College of Sports Medicine. American College of Sports Medicine position stand. Quantity and quality of exercise for developing and maintaining cardiorespiratory, musculoskeletal, and neuromotor fitness in apparently healtyadults: guidance for prescribing exercise. Med Sci Sports Exerc. 2011 Jul;43(7):1334-59. doi: 10.1249/MSS.0b013e318213fefb.
• Gibson A. John Hilton: “Rest and Pain”. Can Med Assoc J. 1955;73(7):569-72.
• Gladwell VF, Coote JH. Heart rate at the onset of muscle contraction and during passive muscle stretch in humans: a role for mechanoreceptors. J of Physiology. 2002.540(3): 1095-1102.
• Iba´n˜ez-Garcı´a J, Alburquerque-Sendı´n F, Rodrı´guez-Blanco C, et al. Changes in masseter muscle trigger points following strain-counterstrain or neuro-muscular technique. J Bodyw MovTher. 2010;13(1).
• Howell JN et al. Stretch reflex and Hoffmann reflex responses to osteopathic manipulative treatment in subjects with Achilles tendinitis. J Am Osteopath Assoc. 2006;106(9): 537-545.
• Jones L. Jones Strain-Counterstrain. Boise, ID: Jones Strain-Counterstrain;1995.

Reprints not permitted 29
• Kaplan SL, Coulter C, Fetters L. Physical therapy management of congenital muscular torticollis: An evidence-based clinical practice guideline. Pediatr Phys Ther. 2013; Winter;25(4)348-94.
• Kierner AC, Zelenka I, Heller S, Burian M. Surgical anatomy of the spinal accessory nerve and the trapezius branches of the cervical plexus. Arch Surg. 2000;135:1428–31.
• Klingler W, Velders M, Hoppe K, Pedro M. Clinical Relevance of Fascial Tissue and Dysfunction. Curr Pain Headache Rep. 2014(18): 439-446.
• Lima TP, Farinatti PT, Rubini EC, Silva EB, Monteiro WD. Hemodynamic responses during and after multiple sets of stretching exercises performed with and without the Valsalva maneuver. Clinics. 2015;70(5):333-338.
• Mattein P, Dei L, Carretti E, Volpi N, Goti A, Pini R. Structural behavior of highly concentrated hyaluronan. Biomacromoleucles. 2009; 10(6):1516-1522.
• Porges SW. The polyvagal perspective. Biol Psychol. 2007 Feb;74(2):116-43.• Porges SW. The polyvagal theory: phylogenetic substrates of a social nervous system. Int J Psychophysiol.
2001 Oct;42(2):123-46.• Porges, SW, et al. Sleep state and vagal regulation of heart period patterns in the human newborn: an
extension of the polyvagal theory. Psychophysiology. 1999 Jan;36(1):14-21.• Sakuma J, Kanehisa H, Yanai T, Fukunaga T, Kawakami Y. Fascicle-tendon behavior of the gastrocnemius
and soleus muscles during ankle bending exercises at different movement frequencies. Eur J Appl Physiol. 2011. 112(3):887-898.
• Schaller B, Cornelius JF, Prabkaker H, Koerbel A, Gnanaligham K, et al. The Trigemio-cardiac reflex: An update of the Current Knowledge. Neurosurg Anesthesiol. 2009; 21(3). 187-195.
• Schleip, R. Fascial Plasticity: A new Neurobiological Explanation. JBMT 2003; Jan.
• Schleip R. Fascia is able to contract in a smooth muscle-like manner and thereby influence musculoskeletal mechanics. Proceedings of the World Congress of Biomechanics, Munich, Germany 2006, ISBN 88-7587-270-8, pp. 51-54.
• Stecco A, Gesi M, Stecco C. Fascial Components of Myofascial Pain Syndrome. Current Pain Headache Rep. 2013:17;352-362.
• Stern R, Asari AA, Sugahara KN. Hyaluronan fragments: an information-rich system. Eur J Cell Biology. 2006; 85(5): 699-715.
• Straubesand J, et. al: Zum Feinbau der Fascia cruris mit besonderer Berucksichtigung epi-und intrafaszialer Nerven. Manuelle Medizin. 1996: 34: 196-200.
• Taylor JLNES. Developmental Muscular Torticollis: outcomes in young childrentreated by physical therapy. PediatPhys Ther. 1997;9:173-178.
• Van Buskirk RL: Nociceptive reflexes and the somatic dysfunction: A model. J Am Osteopath Assoc. 1990; 90:792-809.
• van Vlimmeren LA, Helders PJM, Van Adrinchem LNA & Engelbert RHH. Torticollis and plagiocephaly in infancy: therapeutic strategies. Pediatric Rehabilitation;2006;9, 40-46. doi: 10.1080/13638490500037904
• Wong, C. K., et al. Strain counterstrain technique to decrease tender point palpation pain compared to control conditions: a systematic review with meta-analysis. J Bodyw Mov Ther 2014;18(2): 165-173.
• Wynne, M. M., et al. "Effect of counterstrain on stretch reflexes, Hoffmann reflexes, and clinical outcomes in subjects with plantar fasciitis." J Am Osteopath Assoc; 2006. 106(9): 547-556.
• Yahia LH, et. al: “Viscoelastic properties of the human lumbodorsal fascia. J Biomed Eng; 1993 15: 425-429.
Resources
• To learn more about Neural Manipulation,
contact www.barralinstitute.com
• To learn more about TMR tots, contact
https://tmrseminars.com/


















