5. Spleen, Liver and Pancreas, Biliary ducts and Gallbladder (75).pptx

Best of UEG week 2017
(Pancreas-biliary)
Marianna Arvanitakis
Erasme University Hospital, ULB, Brussels, Belgium
10th Nottingham Endoscopy Masterclass

SPEAKER DECLARATIONS
This presenter has the following
declarations of relationship with industry
• NONE
[28/10/17]

3

OP103: COVERED VS UNCOVERED SEMS FOR
PALLIATION IN MALIGNANT CBD STRICTURES: A RCT
4Mangiavillano et al, UEG journal 5S, A44
Clin Gastrol Hepatol 2013
Latest meta-analysis of 9 RCTs (1061 patients)
No difference in stent patency, AP, cholecystitis, cholangitis, perforation, LoS
Covered SEMS: More stent migration (OR 7.1)
More tumor overgrowth (OR 1.9)
Less tumor ingrowth (OR 0.2)
ESGE guidelines 2012

OP103: COVERED VS UNCOVERED SEMS FOR
PALLIATION IN MALIGNANT CBD STRICTURES: A RCT
5Mangiavillano et al, UEG journal 5S, A44
FC SEMS
NitiS Biliary
N=78
Uncovered SEMS
NitiS Biliary
N=78
RCT: Primary end-point Stent patency
Secondary end-point AE
148/156 analysed
Technical success 98.7% 100% NS
Decrease in bili -70% -68% NS
Normalisation in bili 28.2% 28.9% NS
AE 25.4% 13.1% 0.09
Migration 7% 0% 0.024
Stent patency 9.5 mo 18 mo 0.046

OP107: DIGITAL SOC FOR TREATMENT OF DIFFICULT
STONES
6
International, multicenter, retrospective study
407 patients with difficult bile stones (2/15-2/16)
D-SOC with laser lithotripsy or electro-hydraulic lithotripsy
Difficult stones: large (15mm), multiple, impacted,
cystic/IH duct, Mirizzi syndrome, biliary stricture
Failed ERCP before treatment: 85.8%
End points:
Technical success
Safety
Brewer-Guttierez et al, UEG journal 5S, A45

OP107: DIGITAL SOC FOR TREATMENT OF DIFFICULT
STONES
7Brewer-Guttierez et al, UEG journal 5S, A45
Total
(n=407)
EHL
(n=306)
LL
(n=101)
P
Technical success 396 (97.3%) 296 (96.7%) 100 (99%) NS
Number of
sessions (med)
1(1-4) 1 (1-4) 1 (1-4) NS
Need for ESWL or
surgery
1 1 0 NS
Duration of
procedure (min)
67 73 49 <0.001

OP105: SHORT TYPE DBE FOR ERCP: A LARGE CASE SERIES
8Shimatani et al, UEG journal 5S, A44
Usefulness of new short DBE for ERCP on post-
operative patients
Retrospective study with 222 post-operative
patients (280 procedures)
End points:
Success rate and time for reaching the blind end
Diagnostic success rate
Therapeutic success rate
Overall success rate
Mean time to complete DB-ERCP
Adverse effects

OP105: SHORT TYPE DBE FOR ERCP: A LARGE CASE SERIES
9Shimatani et al, UEG journal 5S, A44
RnY HJ WhippleRnY total gastrectomy
91
pt
42
pt
85
pt
RnY HJ RnY total Whipple Total
Success blind end 95.6% 100% 100% 98.6%
Time blind end (min) 20.9 13.4 8.4/20 14.4
Success diagnostic rate 100% 95.2% 98% 97.4%
Overall success rate DB-
ERCP
95.6% 95.2% 98% 96.1%
Time for DB-ERCP (min) 71.7 78.5 42 61
AE 1.1%

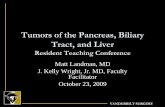
OP106: EUS GUIDED GASTRO-GASTROSTOMY ASSISTED
ERCP VS ENTEROSCOPY ASSISTED ERCP IN RNYGB
10Bukhari et al, UEG journal 5S, A45
Multicenter, comparative trial
Kedia et al, GIE 2015

OP106: EUS GUIDED GASTRO-GASTROSTOMY ASSISTED
ERCP VS ENTEROSCOPY ASSISTED ERCP IN RNYGB
11Bukhari et al, UEG journal 5S, A45
160 patients, 5 centers

12
OP359:INTRADUCTAL ABLATION DURING ENDOSCOPIC
AMPULLECTOMY
Perez-Cuadrado et al, UEG journal 5S, A152
Retrospective analysis of patients undergoing endoscopic
ampullectomy
Rustagi et al, GIE 2016

13
OP359:INTRADUCTAL ABLATION DURING ENDOSCOPIC
AMPULLECTOMY
Perez-Cuadrado et al, UEG journal 5S, A152
Retrospective analysis of patients undergoing endoscopic
ampullectomy
If necessary, intraductal ablation was performed with wire-guided
RF or wire-guided cystotome
Retrospective analysis 2010-2016 73 patients (58 years)
EUS detected intraductal involvement in 16 (21.9%)
Intraducactal ablation with cystotome (n=14) and RFA (n=2),
followed with biliary and/or pancreatic stenting
Complications 19.2% (AP, bleeding, perforation, ductal stricture)
HGD (n=27, 37%) and adenocarcinoma (n=6, 8.2%)
FU 23 months: Recurrence (16.4%) and surgery (3 pt)
Multivariate analysis: only repeated endoscopic sessions >2
were associated with recurrence

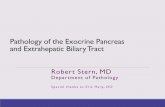
OP362: MISER RCT: MINIMALLY INVASIVE SURGERY VS
ENDOSCOPY FOR NECROTIZING PANCREATITIS
14Bang et al, UEG journal 5S, A153
Patients with necrotizing pancreatitis Walled-off necrosis
Minimally invasive
surgery
Laparoscopic KG with
internal debridement
or
VARD
Endoscopy
Initial transmural
drainage (single, multi
gate or dual)
And
Debridement if
necessary
Primary end-points: Composite of major complications (MOF, bleeding or fistula)/DeathSecondary end points: Treatment success (early/mid/late)

© UEG. 2016
APPROACHES TO WON: TENSION
Endoscopic step-up
approachETD ETN if needed
n = 51
Surgical step-up
approachPCD VARD if needed
n = 49
Major complications or
death during 6 m FU20% 28% NS
Mortality 18% 13% NS
No need for necrosectomy 41% 49% NS
Pancreatic fistula 5% 32% p=0.001
LOS 36 d 69 d p=0.03
Dutch Pancreaittis Study Group, Abstract UEGW 2016
TENSION trial: Multicenter RCT: 98 patients with infected WON

OP362: MISER RCT: MINIMALLY INVASIVE SURGERY VS
ENDOSCOPY FOR NECROTIZING PANCREATITIS
16Bang et al, UEG journal 5S, A153
Minimally invasive
surgery (n=32)
Endoscopy
(n=34)
40% required
debridement
MIS Endoscopy p
Primary end point 34.4% 5.9% 0.004
Treatment success
Early
Mid
Late
53.1%
81.3%
84%
97.1%
100%
96.2%
<0.001
0.01
0.19
Adverse effects 53.1% 41.2% 0.33
Mortality 6.3% 2.9% 0.61
LoS (days) 18.5 14 0.057

OP363:LAMS VS PLASTIC DPT….ACT 1
17Brewer-Guttierez et al, UEG journal 5S, A153
- Cost-effective analysis for patients receiving LAMS vs DPT for WON- Simulation based on a pre-determined decision tree based on
probabilities obtained from systematic review of the literature- Efficiency: Successful drainage without need for percutaneous or
surgical intervention
LAMS improves the effectiveness of endoscopic management of patients with WON

P0252:LAMS VS PLASTIC DPT….ACT 2
18Bang et al, UEG journal 5S, A248

Bang et al, Gut 2016
Interim analysis of ongoing RCT:EUS-guided drainage WON: Plastic vs LAMS
- Bleeding (n=3)- Buried stents (n=2)- After 3 weeks!!
LAMS
(12)
Plastic
(9)
AE
(6):50%
AE
(0):0%
Trial still ongoing but extraction
before 4 weeks
Endoscopic management
of WON (>20% necrosis)
Leeds et al, Gut 2016

P0252:LAMS VS PLASTIC DPT….ACT 2
20Bang et al, UEG journal 5S, A248
LAMS Plastic DPT p
Procedure duration (min) 15 42.5 <0.001
Resolution of pre-
intervention of SIRS
44.4% 69.2% 0.38
Treatment success 96.3% 88% 0.34
Adverse effects
Overall
Stent related
41.9
32.3
20.7
6.9
0.10
0.02
Number of re-interventions 1 1 0.78
Readmissions 29% 34.5% 0.78
LAMS (n=31) Plastic (n=29)
Extraction before 4 weeksAfter amendement, no
differences were found (6.5% vs
6.9%)

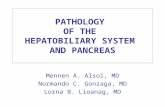
OP315: EUS GUIDED RFA FOR PREMALIGNANT PANCREATIC
TUMORS
21Barthet et al, UEG journal 5S, A248
Prospective multicenter French study (9/15-2/17)
Patients with premalignant lesions who are unfit
or refuse surgery:
Side branch IPMNs with worrisome features
Pancreatic NETs (<2cm)
MCA
EUS-guided RFA
End points:
Safety
Efficacy at 1 year FU

RFAHeat
injury
Immunomodulation
Cytokine
s

23
OP315: EUS GUIDED RFA FOR PREMALIGNANT PANCREATIC
TUMORS
Barthet et al, UEG journal 5S, A248
Complications 3/30 (10%)
AP
Delayed perforation
Pancreatic duct stricture
12
18
PATIENTS N=30
PNET CYSTIC T.
3
6
3
PNET:13.4 mm (8-20mm)
HEAD BODY TAIL
14
3
1
CYSTIC T. 29.1 mm (9-60 mm)
HEAD BODY TAIL
NSAIDS Antibiotics Aspirating cystic liquid before

24
OP315: EUS GUIDED RFA FOR PREMALIGNANT PANCREATIC
TUMORS
Barthet et al, UEG journal 5S, A248
NETs:
At 6 months: Significant response 82%
7 had complete necrosis or disappearance
2 a diameter decrease >50 %,
2 had a diameter decrease <50%
1 a complete failure Cystic lesions:
At 6 months: Significant response 69%
7 complete resolutions , 2 PR diameter decrease >50%
1 partial response <50%
3 no response
Mural nodes disappeared in 10 /12 cases

25

26