Benign Prostatic Hyperplasia.doc(2)
85
1 CONTENTS Page Benign Prostatic Hyperplasia (BPH) ........................................................... 4 Classification of the Prostate ...................................................................... 4 Incidence ...................................................................................................... 6 Etiology .......................................................................................................... 7 Endocrinology & Pathogenesis .................................................................. 8 I. Androgen Factor ................................................................................... 9 The 5-alpha-dihydrotestosterone hypothesis .................................... 9 II. Factor Related to Ageing ..................................................................... 10 1. Oestrogen-Testosteron Imbalance ................................................. 10 2. Stem Cell Theory ................................................................................ 11 3. Reduced Cell Death Theory ............................................................ 12 4. Stromal-Epithelial Interaction Theory .............................................. 13 Pathology ...................................................................................................... 14 Pathogenesis ................................................................................................ 16 Diagnostic Tests ............................................................................................ 18 I. Mandatory tests ....................................................................................... 19 a. History or Symptoms ............................................................................ 19 Medical Complication of BPH ............................................................... 21 Quantification of Symptoms .................................................................. 23 Impact BPH on Daily Life ......................................................................... 25 b.Physical Examination ........................................................................... 26 Sign .......................................................................................................... 26 Digital Rectal Examination .................................................................. 27 c. Urinalysis and Renal Functions Assessment ...................................... 29 II. Recommended tests ............................................................................... 29
-
Upload
wahyunita-ilham -
Category
Documents
-
view
31 -
download
3
description
cfjhnmb
Transcript of Benign Prostatic Hyperplasia.doc(2)
-
1
CONTENTS
Page
Benign Prostatic Hyperplasia (BPH) ........................................................... 4
Classification of the Prostate ...................................................................... 4
Incidence ...................................................................................................... 6
Etiology .......................................................................................................... 7
Endocrinology & Pathogenesis .................................................................. 8
I. Androgen Factor ................................................................................... 9
The 5-alpha-dihydrotestosterone hypothesis .................................... 9
II. Factor Related to Ageing ..................................................................... 10
1. Oestrogen-Testosteron Imbalance ................................................. 10
2. Stem Cell Theory ................................................................................ 11
3. Reduced Cell Death Theory ............................................................ 12
4. Stromal-Epithelial Interaction Theory .............................................. 13
Pathology ...................................................................................................... 14
Pathogenesis ................................................................................................ 16
Diagnostic Tests ............................................................................................ 18
I. Mandatory tests ....................................................................................... 19
a. History or Symptoms ............................................................................ 19
Medical Complication of BPH ............................................................... 21
Quantification of Symptoms .................................................................. 23
Impact BPH on Daily Life ......................................................................... 25
b.Physical Examination ........................................................................... 26
Sign .......................................................................................................... 26
Digital Rectal Examination .................................................................. 27
c. Urinalysis and Renal Functions Assessment ...................................... 29
II. Recommended tests ............................................................................... 29
-
2
Uroflowmetry ............................................................................................. 29
Residual Urine ........................................................................................... 30
III. Optional tests ........................................................................................... 32
Serum Prostatic Specific Antigen ......................................................... 32
Ultrasonography Examination (USG) ................................................... 33
Imaging of the upper urinary tract ...................................................... 34
Endoscopy of lower urinary tract ......................................................... 35
CT Sacanning & magnetic Resonance Imaging (MRI) .................... 35
Treatment ...................................................................................................... 36
I. Conservative Therapy .............................................................................. 36
a. Watchful Waiting ................................................................................. 36
b. Medical Treatment ............................................................................. 37
1. Endocrine Therapy .......................................................................... 38
a. 5 Alpha Reductase Inhibitor (5R) Therapy ............................ 38
b. Anti Androgen = Androgen Deprivation Therapy ................. 39
c. LHRH Analogue / LHRH Agonist ................................................. 39
d. Aromatase Inhibition and Anti Oestrogens ............................ 40
2. Alpha Adrenergic Antagonist Therapy ........................................ 41
Alpha Blocker (-Blocker) ................................................................ 42
Classification of the alpha blocker in the treatment of BPH ..... 43
3. Phytotherapy ..................................................................................... 45
Phytotherapy component .............................................................. 46
Active Ingredient .............................................................................. 47
Working Mechanism ......................................................................... 48
4. Combination Therapy ...................................................................... 49
II. Conventional Surgical Therapy .............................................................. 51
Indications ................................................................................................ 51
1. Open Prostatectomy ....................................................................... 52
-
3
a. Supra Pubic Transvesical Prostatectomy .................................. 53
b. Supra Pubic-Retro Pubic Prostatectomy .................................. 55
c. Perineal Prostatectomy .............................................................. 60
2. Endoscopic Prostatectomy ............................................................ 62
a. Trans Urethral Resection of the prostate (TURP) = Trans
Urethral Prostatectomy ............................................................. 62
b. Trans Urethral Incision of the Prostate (TUIP) ......................... 65
III. Interventional Treatment = Minimal Invasive ...................................... 66
1. Ballon Dilatation ....................................................................... 66
2. Intra Prostatic Stent ................................................................. 68
3. Cryo Therapy ............................................................................ 71
a. Trans Urethral ...................................................................... 71
b. Transperineal ...................................................................... 72
4. Hyperthermia = Thermotherapy ............................................ 73
a. Microwave Thermo Therapy ........................................... 73
b. Laser .................................................................................... 75
c. Radiofrequency Energy ................................................... 77
d. High-Intensity Focused Ultrasound Therapy (HIFU) ...... 78
e. Vaporation of the prostate ............................................. 79
Catheterization ............................................................................................ 80
Prognosis ........................................................................................................ 81
References .................................................................................................... 82
-
4
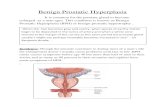
BENIGN PROSTATIC HYPERPLASIA (BPH)
BPH is the non cancerous growth of nodule in the region of the
prostate gland surrounding the urethra
Prostate gland is accessory male sex gland surrounds the prostatic
urethra and lies between the bladder outlet and the external sphincter
Prostate gland consist of three main types of tissues:
Epithelial element (20-30%) : 1.) Epithelial tissue, consisting of
prostatic acini glandular organ
Stromal element (70-80%): a fibromuscular tissue, consist of :
2.) Smooth muscle tissue (20-40%)
3.) Connective tissue (60-80%)
Its weight about 20 gr and length 2,5 cm
CLASSIFICATION OF THE PROSTATE (LOWSLEY)
Consists of :
1. The anterior lobe, lies in front of the urethra
2. The median lobe, project upwards beneath surround the two
lateral lobes which project into the urethra
3. The right lateral lobe
4. The left lateral lobe
5. The posterior lobe, lies behind the lateral lobes and distal to the
median lobe
The anterior lobe is dominated fibromuscular tissue
Prostatic adenoma (BPH) develops from periurethral gland of the site
of median and / or lateral lobes
The posterior lobe is prone to cancerous degeneration
adisastraHighlight
adisastraHighlight
-
5
Fig.1. Anatomy of the prostate gland (Adapted from Lowsley, 1930) (Ref.
Scott p.26
ZONAL ANATOMY OF THE PROSTATE
Mc Neal (1968) has popularized the concept of zonal anatomy of the
prostate : (Fig.2)
1. Peripheral zones (PZ : 70% of the volume)
2. Central zone (CZ: 25%)
3. Transition zone (TZ : 5%)
The concept of zonal anatomy is more important in differentially
afflicted with neoplastic processes : (Mc Neal et al,1988)
1. 60-70% of ca. P originated in the peripheral zone
2. 10-20%in the transition zone
3. 5-10% in the central zone
4. BPH uniformly originates in transition zone
adisastraHighlight
-
6
Fig.2. Zonal anatomy of the prostate gland (Mc.Neal. A : Schematic lateral
view of the prostate. B : Cut section of the same, C : transverse View
of area show in B (Ref.Tanagho 15th Ed. p.400)
INCIDENCE
BPH is the most common benign tumor in men
Its incidence is age-related
BPH is ageing male disease
Life expectancy increase BPH increase
50% of all elderly men, at age approximately 75 years have complain of
decrease in the force and caliber of the urinary stream and 20-50% of
them undergo surgery
BPH in autopsy studies found : (Berry et al, 1984)
20% in men aged 41-50 years
To 50% in men aged 51-60 years
To over 90% in men older than 80 years
adisastraHighlight
-
7
Approximately 50% of men under the age of 60 who undergo surgery for
BPH may have heritable form of the disease. This form is most likely an
autosomal dominant trait
First degree male relative of such patients carry an increased relative risk
of approximately 4-fold (Sonda et al, 1994)
Incidence of BPH is lower in black males than white males but in Orleans,
USA, higher incidence in blacks than whites
The prevalence of BPH seems considerably lower in far Eastern country,
especially in Japan and China than in the West
South-East Asian migrating to the USA acquire a higher rate of BPH than
their counterparts remaining in South-East Asia
BPH is higher in man who consume milk than vegetable
ETIOLOGY
Unknown exactly
It seems to multi factorial and endocrine controlled
Each element of the prostate glands either alone or in combination can
give rise to hyperplastic noduls
Laboratory and clinical studies have identified two factors necessary for
the development of BPH :
1. Androgen factor : The presence of 5-alpha-dihydrotestosteron
(DHT)
2. Factor related to ageing
Other proposed risk factors for development of BPH :
1. Western diet
2. Industrialized environment
3. Hypertension
4. Diabetes mellitus
adisastraHighlight
-
8
ENDOCRINOLOGY & PATHOGENESIS
The prostate in man requires the presence of adequate levels of
circulating testosteron in order to develop and grow (Fig.3)
The decopeptide Luteinizing Hormone Releasing Hormone (LHRH) in
released from Hypothalamus
LHRH stimulates the pituitary to secrete Luteinizing Hormone (LH)
LH then in turn acts directly on the Leydig cells within the testis stimulating
them to secrete 90-95% of testosteron. The remaining 5-10% of daily
testosteron production is either directly by the adrenal gland or
peripheral metabolism
Adrenal gland required stimulating ACTH from pituitary to produce
adrenal-androgen
Fig.3. Control of androgen production and utilization. (ACTH,
adrenocorticotrophic hormone; LH, luteinizing hormone; LHRH,
luteinizing hormone releasing hormone) (Ref. Kirby p.15)
adisastraHighlight
-
9
TESTOSTERON
(in the Cytoplasma)
5 - Reductase
(in nucleus membrane)
Androgen
Receptor
+ Cell
Replication
Growth Factor
(In the Cytoplasma) mRNA
DHT
(in the nucleus)
+
I. ANDROGEN FACTOR :
THE 5-ALPHA-DIHYDROTESTOSTERONE HYPOTHESIS (Fig.4 & 5)
In the blood stream 98% of circulating testosterone is bound to human
serum albumin and Sex Hormone Binding Globulin (SHBG)
The remaining 2% as a free testosteron (T).
The free testosteron enter to prostatic cells (cyto plasma) by simple
diffusion
DHT produced from testosteron (T) by the enzym 5-alpha-Reductase (5-
R) in nuclear membrane
The binding of DHT to androgen receptor (AR) produces a
conformational change in the chromatine which facilitates transcription
of specific sequences of DNA into messenger RNA (mRNA) producing
growth factors that stimulate prostate growth (cell replication)
5 ALPHA-DIHYDROTESTOSTERON (5 - DHT)
l
Fig. 4. Testosterone is converted in to DHT by a nicothinamide adenosine dinucleotide
phosphate (NADP) a dependent enzyme in the nuclear membrane and name 5 alpha reductase
BPH developes if : 1. Increased intraseluler DHT
2. Increased 5 reductase activity 3. Increased androgen receptor level
adisastraHighlight
adisastraHighlight
-
10
Fig. 5. Development of BPH : The 5 DHT hypothesis (Ref. Kirby p.16)
II. FACTORS RELATED TO AGEING
1. OESTROGEN-TESTOSTERON IMBALANCE
In ageing male, there is decreased responsiveness of the testis to
bioactive LH, while plasma LH within normal limit
The consequence of this change is an age related decrease in free
testosteron
In ageing male, there is increased plasma level of oestrogen /
extradiol
Oestrogen in BPH :
Produced in man largely by aromatization of androgen
Induce stromal cell hyperplasia
Increase androgen receptor population in prostatic cell nuclei
Increased stromal cell longevity and inhibit the rate of prostate
death
adisastraHighlight
adisastraHighlight
-
11
2. STEM CELL THEORY
Stem cell is a cell which have extensive proliferative potential to
maintain balanced cell numbers, in growth and death rates of the
organ, allowing a steady state to exist (Fig.6)
Stem cell produce amplifying cells and finally transit cell
Amplifying cell is a cell have limited proliferative potential
Transit cell is a cell have very limited proliferative potential and it is
determined by the level of androgen stimulation
Transit cell death it self, normally stimulates stem cell to produce new-
cells
Apoptosis occurred after androgen withdrawal. Epithelial cells are
more susceptible than stromal cells to the withdrawal of androgen
stimulus. Stem cells survive, however, that are capable of
regeneration if the androgen stimulus is restored
BPH is postulated to be the result of inappropriate activity of stem cell
with resultant overproduction of both stroma and epithelial cells
abnormal proliferation of stem cell
Fig.6. Stem cell theory for the development of BPH (Ref. Kirby p.22)
adisastraHighlight
-
12
3. REDUCED CELL DEATH THEORY
Barrack and Barry (1987) demonstrated rather elegantly that
oestrogen, when given in the presence of androgen, inhibit the rate
of cell death in the canine prostate (Fig.7)
This result clearly raise the possibility that BPH in man might not be due
to an increased in cell replication but rather be caused by a
decreased in cell death
Increasing oestrogen levels in later life may also play a role either by
inducing androgen receptors or decreasing the rate of either
epithelial or stromal cell death
Fig. 7. Reduced cell death resulting in BPH (Ref. Kirby p.22)
adisastraHighlight
-
13
4. STROMAL EPITHELIAL INTERACTION THEORY
This theory is based on significant of epithelial interaction the growth
and maintenance of the prostate gland
Reischeuer (1925) concluded that the initial lesion in BPH might be a
stromal node that would lead to a subsequent migration of epithelial
cells resulting in a new gland component (acinus)
Mc.Neal (1978) found that the initial (acinus) in BPH was not the
formation of stromal nodes but a glandular budding and branching,
mechanism which could create new alveoli on the pre prostatic
area.It suggest the occurrence of a potential embryonic
reawakening of the prostatic stroma during the adult phase as a
result of the similarities observed between epithelial budding and
glandular morphogenesis on the embryonal tissue. For that reason,
this theory is also called as embryonic reawakening theory
Cunha et al (1980) suggested that the potential presence of an
embryonal stroma induce on the epithelial prostatic cells of adult.
Stromal autocrine or paracrine growth factors may stimulate
epithelial reawakening, growth factors implicated, include,
epidermal growth factor (EGF) transforming growth factor beta (TGF-
), Fibroblast growth factor (FGF), etc
Other hypothesis (Lawson) is based on Basic Fibroblast growth factor
(b FGF). This factor is released by microinjury of distal prostatic duct
from voiding, ejaculation or infection and causes induction of
primitive mesenchym in the periurethral tissues BPH. The b FGF may
be released directly from epithelial cells with a resulting paracrine
action on adjacent stromal cells or released from injured stromal cell
with an autocrine effect on adjacent stromal cells. The 3rd alternative
is that b FGF released from the injured denuded basement
adisastraHighlight
-
14
membrane or extra cellular matrix by the action of the enzyme
heparitinase with stimulation of adjacent stromal cells.(Fig.8)
PATHOLOGY
The basic change of BPH is :
Epithelial hyperplasia of the prostatic gland
Muscle hypertrophy
Connective tissue hyperplasia
BPH be aims to appear from :
The 2nd to 3rd decades, microscopic pathological BPH
The end of the 4th decades, macroscopic pathological BPH
The 5th decade on there occurrence of clinical BPH
The hyperplasia originates in the transition zone and an adenoma is
formed, it compress the outer zone of the prostate, which forms a false
capsule as a called, surgical capsule
Fig. 8. Hypothesis for the role of growth factor in the genesis of
BPH. Paracrine and/or autocrine effects of growth factors may
play an important role in hyperplastic prostate growth. (Ref.
Herbert Lepor p.451)
adisastraHighlight
-
15
The gland may become extremely large if there much of the epithelial
but can remain quite small if the fibrous stroma chiefly affected
fibrotic prostate
Fibrous stroma hyperplasia of median lobe median bar
All lobes of the prostate may be affected and commonly may assume
any combination of these type : (Fig.9)
Isolated median lobe enlargement (30%)
Lateral lobes (Right & left) (15%) intrusion into the urethral
lumen they make a kissing lobes
Lateral and median lobes Trilobar (23%)
Posterior commissure (posterior vesical lip. or elevated bladder
neck) hyperplasia, sub cervical median lobe hyperplasia (15%)
Lateral and posterior commissure hyperplasia (17%)
Fig. 9. Commonly the hypertrophy may assume any combination of these
types (Ref. Scott p.221)
-
16
PATHOGENESIS
The enlarged gland produces its harmful effect obstructing the
bladder neck and by upsetting the mechanisms which force open
and funnel the vesical orifice
I. Changes in the bladder
1. Early: As the degree of obstruction increase, the vesical detrussor
undergoes compensatory hypertrophy in order to overcome the
increasing urethral resistance. The muscle wall may become
more than 2 cm thick. This power of compensation varies :
One patient may have a few symptoms with a markedly
obstructive gland
Another may have great difficulty to void with a milder
obstruction
Thus, no relationship between the size of the gland and the
severity of symptoms.
As compensatory hypertrophy develops the following take place.(Fig.10)
a. Trabeculation of bladder wall intertwined muscle bundle lift up
the mucosa
b. Hypertrophy of the trigone and inter ureteric ridge
c. Cellules : The increasing intravesical pressure tends to push mucosa
between the superficial muscle bundles causing the formation of
small pockets or cellules
d. Diverticula: If cellules force their way entirely through the
musculature of the bladder wall, they become balloons or
diverticula in the perivesical fat. Diverticulum, sometimes grows to
large size and has no muscular wall. It can not emptying itself. The
urine, its contains, easily becomes infected.
adisastraHighlight
adisastraHighlight
-
17
2. Late : If muscle of vesical compensation becomes exhausted,
when the muscle can no larger hypertrophy and
decompensation occurs resulting in the presence of residual
urine. Thereafter, infection may occurs, mucosa become
reddened and oedematous and may be stone formation.
If urine becomes infected, urine might be entered to ejaculatory
duct and then through vas deferens to epididymis and testicle
and at last epididymitis and orchitis occur.
Fig. 10. Changes the bladder developing from obstruction: a. normal
bladder and prostate, b. trabecula, cellules formation and
hypertrophy of the inter ureteric ridge. c. market trabeculetion and
diverticulum ( Ref. Tanagho 15th Ed. p.209)
II. Changes In The Upper Urinary Tract (Ureter and Kidney)
With secondary hypertrophy of the trigonal-ureteral complex, there is
increased downward traction on the intra mural ureteral segment,
a b
c
adisastraHighlight
-
18
thus increasing resistence to urine flow. This leads to progressive
proximal dilatation and is the common cause of hydrouretero
nephrosis
In the decompensated phase, significant residual urine leading to
chronic vesical distention may cause a vesico ureteral reflux which is
reflected in diminution in renal urinary secretion which is caused by
making largely hydrouretero nephrosis
If the vesico ureteral junction gives way, the infected urine may
ascend to the kidney, ureteristis and pyelonephritis develop
DIAGNOSTIC TESTS
Recommendation of the International Consensus Committee WHO
(1993) guidelines three classification of diagnostic tests and studies :
I. Mandatory tests : these should be performed on every patient
presenting to doctor with complaints of bladder outflow
obstruction :
a. History or symptoms and quantification of symptoms
b. Physical examination and digital rectal examination
(DRE)
c. Urinalysis and renal function assessment
II. Recommended tests of proven value in the evaluation of
most patients. Their use strongly encouraged during initial
evaluation :
a. Uroflowmetri
b. Residual urine
III. Optional tests of proven value in the evaluation of selected
patients only :
a. Pressure / flow studies
adisastraHighlight
-
19
b. Serum prostate specific antigen (PSA)
c. Transrectal ultrasound (TRUS)
d. Imaging of the upper urinary tract
e. Endoscopy of lower urinary tract
f. CT Scanning/ MRI
I. MANDATORY TESTS
a. HISTORY OR SYMPTOMS
Obtain an adequate history by enquiring about the urinary tract
especially the complaints of the patients why they present to their
doctors
All symptoms of BPH are known as a prostatismus but much bladder
neck obstruction or urethral obstruction can occur without BPH such
as urinary tract infection, bladder or urethral stone, neurogenic
bladder, urethral stricture, median bar or bladder neck contracture.
So, that term now about prostatismus is known as Lower Urinary Tract
Symptoms (LUTS)
CLINICAL FINDING
A. SYMPTOMS
The individual symptoms in a logical sequence of micturation
consist of :
1. Pre micturation symptoms
Frequency
Nocturia
Urgency and urge incontinence
Incontinence
2. Micturation symptoms
Hesitancy
-
20
Intermittency
Straining to void
Dysuria
Reduction in the force and the caliber of stream
Terminal dribble
3. Post micturation symptoms
Feeling of incomplete emptying
Post micturation dribble
The symptoms of bladder outflow obstruction resulting from BPH have
been divided in two groups.
Obstructive or voiding symptoms :
1. Hesitancy
2. Straining to void
3. Weak stream (poor flow rate)
4. Terminal dribble/post micturation dribble
5. Prolonged micturation
6. Urinary retention
7. Incontinence
8. Incomplete emptying
9. Intermittent stream
Irritative or filling symptoms = storage symptoms
1. Frequency
2. Urgency of micturation
3. Urge incontinence
4. nocturia
-
21
Obstructive component which produce obstructive symptoms can
be sub divided
a. Mechanical obstruction may result from intrusion into the
urethral lumen or bladder neck leading to a higher bladder
outlet resistance = BPO : Benign Prostate Obstruction
b. Dynamic obstruction may result from the contraction of the
smooth muscle compound of fibro muscular stroma caused by
stimulus of adrenergic nerve = BOO : Bladder Outlet
Obstruction
c. Decreased detrussor contractility produce reduction in the
force of urinary stream
Irritative voiding complaints of BPH may result from the secondary
response of the bladder to the increased outlet resistance.
Urodynamic evaluation in patients with BPH has demonstrated a loss
of compliance and unstable detrussor contractions during filling in up
to 70% patients. Muscle enlargement of the bladder with occurs and
this heightens the irritability of trigone the most sensitive part of the
bladder, which is located just inside the bladder neck
The presence of urinary tract infection or / and bladder stones may
result in progressive severity of symptoms of BPH
MEDICAL COMPLICATION OF BPH
1. Prolonged obstruction may bring further complication, such as
hydronephrosis with accompanying compromised renal function
2. Incomplete bladder emptying causes urinary stasis which predisposes
to infection and secondary inflammatory changes in the bladder and
urinary tract. Urinary stasis also predisposes to calculus formation
-
22
3. Straining to void urine can congest superficial veins of prostatic
urethra and trigonum, leading to rupture and subsequent hematuria
4. Prolonged urinary retention may result in progressive renal failure and
azotemia
5. Infected urine that ascend to the ureter can be ureteritis and
pyelonephritis
6. Straining to void infected urine may press urine entered to ejaculatory
duct vas deferens epididymis and testis, resulting epididymitis
and orchitis
7. Acute urinary retention: A medical emergency that requires prompt
attention via the passage of a catheter into the bladder to drain off
urine. Less than 10% of patients will present initially with acute urinary
retention.
Bladder neck obstruction can occur in the absence of BPH which product
symptoms like a Prostatismus
1. Median bar = posterior vesical lip. Connective tissue stroma
hyperplasia of median lobe
2. Bladder neck contracture: occurrence hypertrophy of
connective tissue surround internal urethral orifice caused :
Congenital
Acquired infection cystitis
3. Chronic congestive prostatitis
This is a morbid condition in which there is distention of
the gland with a excessive amount of prostatic fluid
Etiology: Usually result from continued or repeated
unphysiological sexual practice. Sexual excitement
without ejaculation in the most common cause. This
occurs frequently in a married man who is accustomed
-
23
to regular coitus, and whose wife becomes ill or
pregnant, also often occurs in a man whose wife dies or
who is away from home for several months. Sometimes it
is also found in unmarried men who do a lot of petting
but do not have coitus.
Therapy is prostate massage for 4-7 days
QUANTIFICATION OF SYMPTOMS
Symptoms should be quantified by using the International Prostate
Symptoms Score (I-PSS) and Quality of Life (QOL) assessment. This
scoring system was adopted from the American Urological
Association (AUA, 1991) (Fig.11)
This symptoms assessment in clinical studies, firstly was published by
Boyarsky et al in 1977, then followed by Madsen & Iversen (1983),
Fowler et al (1988) and Hald et al (1991 a group of Danish Urologists)
Division of urology, Department of Surgery, Faculty of Medicine of
University Indonesia, Jakarta has often used the Madsen & Iversen
system
Madsen & Iversen score :
Score consist of 9 symptoms. This score introduces the concept of
weighting symptoms. The scaling of each symptom is very variable:
frequency (0-3), nocturia (0-3), hesitancy (0 or 3), intermittency (0-3),
urgency (0-3), weak stream (0-4), feeling of incomplete emptying (0-
4), straining (0 or 2), incontinence (2)
adisastraHighlight
-
24
Fig. 11. International Prostate Symptom Score (I-PSS) consist 0f 7
symptoms/questions each symptom is scored as 0 5. Total score is 35 and divided in 3 categories 0 7: Mildly symptomatic, 8 19: Moderately, 20 35: Severely. In addition, a single question assesses the patients quality of Life (QOL) (Ref. Kirby p.28)
-
25
IMPACT BPH ON DAILY LIFE
A Recent European study (1993) found that :
More than 50% of men with BPH are significantly restricted in an
aspect of daily life :
Limit fluid before travel and bedtime
Can not drive for two hours
Not enough sleep at night
Limit going to place without toilets
Limit playing outdoor sports
Limit going to cinema, theatre, church, etc
Despite like these, the study found that few of patients with BPH
consult their doctors with at least one of a number of restricted in their
participation of social life
Other reason, a small group of BPH patients, less than 10%, will present
to their doctor with acute urinary retention
Reasons why BPH patients do not present to their doctor :
Assumption that symptoms are part of ageing
Stigma associated with dribbling and urgency
Fear of surgery
Fear of diagnosis of ca.prostate
Reductance to submit to digital rectal examination
Symply do not want to bother the doctor
Many men regard the prostate as a genital, they may be
unwilling to admit any defect in its functioning
-
26
b. Physical Examination
SIGNS
A physical examination, Digital Rectal Examination (DRE) and
focused neurologic examination are performed on all patients
Physical examination in BPH often provides less information than the
history
Physical examination should asses
General examination may reveal :
Loss of weight
Oedema
Pallor from anemi secondary to renal impainmant
Costo vetebral angle : pain or mass on palpable
Supra pubic area to rule out significant bladder tone and
mass of enlarged bladder
External genitalia to detect : Hernia, orchitis, epididimitis.
Anal and bulbo cavernous reflex plus brif assessment of
motor and sensory function in lower body. Include
external urethral spincther
A full examination of the respiratory and cardiovascular
system
Where the posibility of operation is raised the following investigation
are mandatory :
a. Electro cardiography to asses myocardial state
b. Chest X-Ray
c. Pulmonary function test
-
27
DIGITAL RECTAL EXAMINATION (DRE)
Urinary bladder is emptied and bimanual DRE the 2nd finger of the
right hand in the rectum and left hand on supra pubis
The well lubricated finger should asses the prostate attention being
paid to :
Size and protrusion of the prostate gland into the rectal lumen
Consistency, like the tip of the nose or rubbery
Irregularities or hard nodules/induration (CaP)
Tenderness, smooth
Presence of fixation to the pelvic wall (CaP)
Symetry
Fibrotic prostate : small, hard DD : CaP
Degree of mobility of the rectal mucosa
Any rectal pathology
The median lobe is impalpable by DRE
BPH and CaP are two distinct disease, although they may be CaP
exist in the same patient
Patients should be reassured that if BPH is diagnosa, CaP is more likely
to be detected at an earlier stage
How to assess the length of protrusion of the prostate gland into the rectal
lumen
1
2
3
Make an imaginary line
from the left point of the
prostate and rectal wall
angle to right angle (1)
Make an imaginary line at
the top of protrusion of the
prostate to be parallel with
the first line (2)
Its range of two lines is the
length of protrusion (3)
Fig.12. The assessment of the length of the prostate protrusion in to the rectal lumen.
-
28
CLASSIFICATION OF THE PROSTATE GRADING
1. Rectal grading : Based on the length of protrusion of enlargement
prostate gland into the rectal lumen. (Fig. 12)
Grade 1 : 1 2 cm : Prostate superior margin easy to reach
Grade 2 : 2 3 cm : Prostate superior margin can be reached
Grade 3 : 3 4 cm : Prostate superior margin can be reached which
bladder is pressed on supra pubic by left hand
Grade 4 : > 4 cm : Prostate superior margin can not be reached
despite it is maneuvered like third grade.
2. Clinical grading : based on residual urine which can be measured by
admitting catheter post voiding. Also can be measured by USG or IVU
post voiding
Grade 1 : residual urine approximately 50 cc
Grade 2 : residual urine approximately 100 cc
Grade 3 : residual urine approximately 150 cc
Grade 4 : residual urine approximately >1 50 cc or urinary retention
3. Radiological grading : based on Protrusion of enlargement prostate
gland into bladder cavity (caudal indentation) on IVU
Grade 1 : Protrusion below the half of range inter ureteric ridge and OUI
Grade 2 : Upper the half of range inter ureteric ridge and OUI
Grade 3 : Protrusion on inter ureteric ridge
Grade 4 : Protrusion upper the inter ureteric ridge
4. Endoscopic grading/intra urethral grading based on the length of kissing
lobes
Grade 1 : < 1 cm
Grade 2 : < 2 cm
Grade 3 : < 3 cm
Grade 4 : > 3 cm
-
29
Grades Of
Sizes
Bergman, Turner Barnes, Hadley Turner, Belt
Weight Of Tissue Removed Weight Of Tissue Removed
1
2
3
4
About 20 gm
About 40 gm
About 70 gm
More than 120 gm
10 25 gm
26 50 gm
51 100 gm
More than 100 gm
Fig.13. Reported Grades Of Sizes On Dre And Their Corresponding Weights
Of Removed Prostatic Tissues (Ref. Tan p71)
c. URINALYSIS AND RENAL FUNCTION ASSESSMENT
Urinalysis to exclude infection or hematuria. If bacteriuria or leucocyt
sediment should be assessed urine culture and sensitivity test. May be
possible to give the antibiotic pre operative
Renal function assessment are required. Renal insufficiency may be
observed in 10% of patient with prostatism. Patients with renal
insufficiency are at an increased risk of developing post operative
complication following surgical intervention for BPH
II. RECOMMENDED TESTS
UROFLOWMETRY
Urine flow studies are the simplest of the range of urodynamic tests
which can be used to investigate patients with lower urinary tract
symptoms
Maximal urinary flow rate (Q max) is the best single measure, but a
low Q max does not distinguish between obstruction and decreased
bladder contractility
-
30
Because of great individual variability of flow rate and the volume of
dependency of the peak urinary flow rate, at least two uroflow
measurement should be obtained, with a resulting volume ideally
more than 150 ml
Urine flow decreases in the overall population with age. A normal
man of 60 years of age will not have the same flow as a normal man
of 20
In children under 10 the Q max should reach a minimum 10 ml/sec
and by 15 years a minimum of 15 ml/sec
In women the Q max before the menopause are generally in exess of
18 ml/sec and after the menopause in exsess of 15 ml/sec
In men before the age of 45 Q max are usually in excess if 18 ml/s, up
to the age of 55, 15 ml/sec and over 65, 13 ml/sec
Assessement an average volume of Q max :
> 15 ml/sec non obstruction
10 15 ml/sec border line
< 10 ml/sec obstructive
RESIDUAL URINE
In general, the quantity of residual urine is an indication of the severity
of the obstruction
But the presence of residual urine does not confirm the diagnosis of
prostatic hypertrophy for it is also associated with other condition,
however does aid in making a diagnosis and also helps guide the
clinician in this choice of treatment
The amount of residual urine is estimated :
-
31
The patient voids all he can, then a small catheter is gently
passed and the urine found to have been retained in the
bladder is meassured
In an excreatory urogram, take a post voiding film at the end of
the series of exposure, after the patients voids all he can and X-
ray at the bladder is taken immediately. Retained urine is
shown by the opaque fluid remaining in the bladder. The
opacity is approximately 1 cm, an average diameter for every
15 ml
The determination of residual urine can also be performed by non
invasive trans abdominal ultra sonography. This will simultaneously
provide information about bladder wall change, bladder stones,
diverticula and median lobe. An ultra sound estimate of residual urine
is perform after each void. Patients lying supine the bladder is
scanned in the transverse and coronal plans. The bladder diameter
Anterior-Posterior (D1), Cranial-Caudal (D2) and Lateral-lateral (D3)
are measured Post Voiding Residual urine is D1 x D2 x D3 x 0,7 (index
value)
The cystogram is a value in making diagnosis. When urinary
obstruction has persisted over a period of several months, the shape
of the bladder becomes pyramidal and its cystographic outline
irregular due to trabeculation and multiple cellules. This appearance
is called a christmas tree
-
32
III. OPTIONAL TESTS
SERUM PROSTATIC SPECIFIC ANTIGEN (PSA)
The clinical distinction between BPH and CaP can not be
accomplished with certainly by DRE and physical examination
PSA determination and DRE in combination provide the best means
to determine the pre treatment probability for CaP and
consequently, the need for TRUS and a prostate biopsy
PSA is not specific for CaP but specific for organ (prostate gland).
Other factors such as BPH, urethral instrumentation, infection, biopsy,
DRE can cause elevation of serum PSA
Normal values PSA depend on age of the patients. Age adjusted
reference ranges for PSA :
40 49 years of age : PSA 0 2,5 ng/ml
50 59 PSA 0 3,5 ng/ml
60 69 PSA 0 4,5 ng/ml
70 79 PSA 0 6,5 ng/ml
Normal value PSA average < 4 ng/ml
Free PSA: 10-40% of total PSA
Patients with PSA 4 10 ng/ml who may need a repeat biopsy
Free / Total PSA ratio: < 15% suggestive of cancer
> 25% suggestive of BPH
15 25% unknown
PSA level are elevated approximately 0,12 ng/ml per gram of BPH
tissue (other literature : 0,33 ng/ml). Thus, patients with enlarged
glands due to BPH may have elevated PSA levels more than 10
ng/ml. The ratio of PSA to gland volume is term the PSA density. Some
investigators advocated prostate biopsy if the PSA density exceeds
0,1 or 0,15
-
33
Patients whose serum PSA increase by 0,75 ng/ml/year, appear to be
at an increased risk of harboring cancer. Increasing PSA level/year is
term the PSA velocity
PSA level-adjusted reference ranges for elevated volume of prostate
gland
Level PSA :
0,2 1,3 ng/ml : volume of prostate gland 0,7 ml/y
1,4 3,2 ng/ml : volume of prostate gland 2,1 ml/y
3,3 9,9 ng/ml : volume of prostate gland 3,3 ml/y
In one study, the sensitivity and specificity of PSA velocity were 72%
and 90% respectively
ULTRASONOGRAPHY EXAMINATION (USG)
USG can be made by Trans abdominal ultrasonography, trans
urethral ultrasonography and transrectal ultra sonography
Trans abdominal USG of the bladder also provides relevant in
formation about bladder wall thickness, the presence of diverticula or
calculi and the post void residual urine (PVR). May also be visualized
the bladder tumor. Prostatic volume can be roughly estimated but
TRUS is more accurate for this, median lobe enlargement visualized.
More over renal USG can also be performed at the some sitting to
identify secondary upper tract dilatation or coincidented renal
pathology
Trans urethral ultrasonography approach during cystoscopy has been
recommended for tumor detection and staging
Trans rectal ultrasonography (TRUS) provides more accurate local
staging then does DRE. The sonographic feature homogenously. CaP
-
34
tends to appear as a hypoechoic lesion in peripheral zone. Biopsies
are usually obtained under TRUS guidence
TRUS also enable measurement of the prostate volume which is
needed in the calculation of PSA density. Typically a prolate ellipsoid
formula is used : (/6)x(anterior posterior diameter=D1)x(transverse
diameter=D2)x(sagittal diameter=D3) or : 0,52 x D1 x D2 x D3, TRUS is
also used the performance of cryosurgery and brachytherapy
IMAGING OF THE UPPER URINARY TRACT
Upper urinary tract imaging (intravenous pyelography) is
recomended only in the presence of concomitant urinary tract
disease or complication from BPH, hematuria, urinary tract infection,
pyelocaliectasis appearance on renal ultra sonography and history
of stone disease.
The straight X-ray may reveal the presence of urinary tract calculi or
soft tissue shadows such as an enlarged kidney or bladder
Attention should be paid to the skeleton for the presence of possible
osteoblastic metastasis from prostatic neoplasma
IVU is carried out and the feature which can be seen in the presence
of obstructive prostatic disease, include :
a. Complete suppression of renal function, usually bilateral
b. Hydronephrosis and hydroureter
c. Fish hooking of the lower ends of the ureters caused by
lateral lobe enlargement
d. Trabeculation of the bladder
e. Bladder diverticular formation
f. Filling defect in the bladder, usually basal, caused by the
enlarging prostate (caudal indentation) of the contrast
-
35
g. Residual contrast left in the bladder after micturation. The
experience eyes can usually estimate how much residual urine
is left
h. The voiding X-ray may reveal the presence of vesico ureteralis
reflux in the decompensated phase of detrussor muscle
i. The cystogram of the BPH which chronic urinary obstruction
the shape of the bladder becames pyramidal and outline
irregular due to trabeculation and multiple cellules. This
appearance it is called a Christmas tree bladder
ENDOSCOPY OF LOWER URINARY TRACT
It is not recommended except in indication :
Hematuria : to detect cause of hematuri such as bladder tumor
or stones
BPH is small on DRE while the symptoms are severity. There are
discrepancies between BPH measure and the symptoms
Urethro cystoscopy to see directly situation of the urethra, zise of
lumen, kissing lobes of BPH, contracture bladder neck, trabeculation
& cellular and diverticula
Before doing uretrocystoscopy may measure PVR
Endoscopy may also assist in choosing the surgical approach in
patients : TURP, TUIP or open prostatectomy
CT-SCANNING & MAGNETIC RESONANCE IMAGING (MRI)
For prostate disease. CT is used for detection of lymphadenopathy
and to evaluate prostatic abscess
In imaging the prostate gland, MRI stirred much interest because
multiplanar imaging and very good tissue contrast allow an excellent
-
36
display of anatomy and intra prostatic pathology. MRI is used in the
evaluation of congenital anomalies and in the staging of prostate
carcinoma
CT scanning and MRI is not recommended for BPH only
TREATMENT
After patients have been evaluated, they should be informed of the
various therapeutic options for BPH. It is important, therefore, when
considering treatment options, that the patient be actively involved
in the choice of therapy; this shared decision-making allows patients
to evaluate the benefits and risks of the various therapeutic options
for themselves
Three main options are currently available for the management of
BPH :
I. Conservative therapy
a. Watchful waiting
b. Medical therapy
II. Conventional surgical therapy
III. Minimally invasive therapy
I. CONSERVATIVE THERAPY
Ad.1a. WATCHFUL WAITING
Although watchful waiting has no direct effect on BPH, it is still a
management option. Any patients, however, complaining of overt
symptoms of BPH must by definition have overcome any inhibition to
present and merits the consideration of active treatment. The
International Consensus Committee (ICC-WHO 1993) recommended
-
37
that patients should be informed of all treatment options before
watchful waiting is chosen and then reevaluated yearly to determine
whether a change to active therapy is needed.
The patients with mild symptoms (IPSS: 0-7)
Watchful waiting is not an option for patients with severe BPH or for
patients with acute retention of urine and/or bothersome symptoms
During in watchful waiting time, all patients will not be suggest to
consume all foods that can increase the symptoms of BPH such as
alcohol, coffee, congestant drugs, etc
Ad.1b. MEDICAL TREATMENT
The idea of pill for the prostate has long been an allowing one for
patient, although the concept has been viewed with skepticism by
surgical oriented urologist for many years
However, data are accumulating to suggest that a number of
pharmacological agent may have reasonable safety and efficacy in
the longer term treatment of obstructive BPH
The treatment of BPH is according to its etiology by giving medical
treatment which blockades pathogenesis and pathophysiology of
BPH to decrease the volume of the prostate gland and relaxes the
contracted smooth muscles of the bladder neck, prostate, prostates
capsule and prostatic urethra.
Medical treatment is only given to BPH which has no indication for
operation, patients awaiting or unwilling to undergo surgery and
patients in whom surgery is contra indication
-
38
Three main options are currently available for medical treatment of
BPH and combination therapy :
1. Endocrine therapy (Hormonal therapy)
2. Alpha adrenergic antagonist therapy
3. Phytotherapy
4. Combination therapy
Ad.1. ENDOCRINE THERAPY
A number of different hormonal preparations have been used to improve
the symptom of BPH. These include:
a. Five alpha reductase (5-R) inhibitors,
b. Anti androgen (androgen deprivation therapy)
c. Luteinizing hormone releasing hormone (LHRH) agonist
d. Aromatase inhibitors and anti oestrogen
Ad. a. 5 Alpha Reductase Inhibitor (5R) Therapy
According to 5-DHT hypothesis, BPH develop as result of the
binding of DHT which product from testosterone by the enzyme
5 Reductase
Finasteride is a 5 reductase inhibitor that blocks conversion of
testosterone to DHT. This drug affects the epithelial component
of the prostate; resulting in a reduction in the size of the gland
and improvement in symptoms.
Six month of therapy are required to see the maximum effect of
prostate size (20-30%) reduction and symptomatic
improvement
Dozes of Finasteride 5 mg once daily
-
39
A number of Finasteride in Indonesia are :Proscar, (MSD), Finpro
(Interbat), Finered (Sunti Seduri), Prosh (Dexa Medica),
Prostakom (Combiphar), etc
Ad. b. Anti Androgen = Androgen Deprivation Therapy
Two type of anti androgen
1. Steroidal with intrinsic hormonal activity:
Cyproterone acetat 50 mg daily
Bromocriptine 2,5 mg / daily
2. Non steroidal that bind directly onto androgen receptor, but with no
intrinsic hormonal actvity :
Flutamide 100 mg 3 times a day
Bicalutamide (Casodex) 150 & 50 mg daily
Anti androgen drugs resulting in a reduction in the size of the gland
23%-30% in 6 month
Side effect of this drugs : gynecomastia & nipple pain 54%,
gastrointestinal disorders (diarrhea) 49%, decrease of libido and
impotence, cardiac side effect, oedem and thromboemboli
This is not acceptable in the elective management of BPH
At this time, significant side effects still seem to be prohibitive for routine
clinical use
Ad. c. LHRH Analogue / LHRH agonist
LHRH analogue therapy like an orchidectomy is a medical androgen
ablation. They inhibit LH & FSH and decrease testosterone. The use of
LHRH analogue agonists has been well deplored in numerous studies in
the treatment of advance Ca.P
-
40
Naferelin inj. s.c. 0,4 mg for 6 month. Prostate size decrease average
25%. After cessation of treatment, the prostate regrewth to original size
by 6 month
Some patients which was given Buserelin, Produce the reduction
prostate volume + 29%
After discontinuation, regrewth of the prostate occurred which
amounted to 97% of the original volume after 24 weeks
The side effect: loss of libido, impotence. To prevent it regrewth again, all
patient should be given continuous treatment, as well as the side effect
of medical castration and they did not believe that this form of therapy
would likely be of significant use in the general population of men with
prostatism
Ad. d. Aromatase Inhibitor and Anti Oestrogens
Aromatase is an enzyme complex responsible for converting androgen
to oestrogen. Aromatase is widely distributed in the reproductive tissue
of both sexes. Androgen extra testicular oestrogen E1 and androgen
testicular oestrogen E2
Oestrogens have long been implicated in the pathogenesis of BPH. BPH
can be induced by the administration of oestradiol.
Aromatase inhibitor leads to a lowering of plasma E1 and E2 in intact
males
The best known and most widely used aromatase inhibitor are :
Aminoglutethimide
Ketoconazole
However, ketoconazole is much more widely used as an anti fungal
agent and Aminoglutethimide has been used as a treatment for Ca.P.
Some report said that araomatase was not an effective treatment for
-
41
BPH because of pituitary feedback mechanism of the lowering of
plasma E1 and E2
A more logical approach would be to block the effect of oestrogen at
target cell by means of anti oestrogen therapy (i.e. an oestrogen
receptor antagonist)
Tamoxifen, as an oestrogen receptor blocker, at a dose of 80 mg daily
for 4 weeks, demonstrated no useful effect
Ad. 2. Alpha Adrenergic Antagonist Therapy
Infravesical obstruction in men with symptomatic BPH is comprise of
static and dynamic components
The dynamic component of obstruction is determined primarily by the
tone of the prostate smooth muscle, bladder neck and prostatic
urethra, while static obstruction by the prostate gland
The development of histochemical methods of identification of
cholinergic and adrenergic nerve ending and receptors demonstrated
the presence of adrenergic receptors in the prostate smooth muscle
bladder neck and prostatic urethra
Most of the treatments for BPH are essentially designed to correct the
obstructive factors. Static factor of prostate gland by surgical treatment
(TUR-P) and various of hormonal manipulation
However, alpha blockers are active on dynamic aspect of obstruction
The prostate smooth muscle, bladder neck & urethra are innervated by
the sympathetic nervous system. This nerve release nor-adrenaline or nor
epinephrine from the nerve ending of the post gangliomic fibre. Nor-
epinephrine acts on the adrenergic receptor of the smooth muscle fibre.
The adrenergic receptors are divided into two groups :
-
42
Alpha receptor and beta receptor
Stimulation of the alpha receptor produces contraction of the
bladder neck and prostate muscle and beta receptors produces
relaxation
There are two groups of alpha receptors
1. The -1 receptors are only present on the target cell and mediate
effect exerted on it
2. The -2 receptors are mainly present on the post-gangliomic nerve
terminals and locally control the uptake of excess norepinephrine
The bladder neck and prostate principally contain -receptor, while the
detrussor contain muscarinic receptor and adrenergic receptors and
-adrenergic receptors are present in only small amount
ALPHA BLOCKER (-BLOCKER)
At present at least six different types of alpha adrenergic receptor have
been identified and classified into two main groups : -1 receptors and
-2 receptors
Consequently, certain drugs are almost exclusively -1 antagonist, -2
antagonist and mixed antagonist
Alpha adrenergic receptor of the bladder neck, urethra and prostate
are essentially -1 receptor an alpha-1 blocking effect have therefore
been more frequently proposed in the treatment of BPH
Many of the -blockers were initially prescribed for their hypotensive
action which could constitute an adverse effect in the context of BPH
So, therefore indication and contra indication to -blocker treatment in
BPH
-
43
INDICATION TO -BLOCKERS TREATMENT
1. Symptomatic relief of BPH in patient without an absolute indication for
surgery
2. Patients in whom surgery is contraindicated
3. Patients unwilling to undergo surgery
4. Patients awaiting surgery
5. Prophylaxis of acute retention in patients undergoing intercurrent surgery
CONTRA INDICATION TO -BLOCKERS TREATMENT
a. Absolute Contra Indication
1. Renal failure secondary to obstructive BPH
2. Gross bladder over distension due to obstructive BPH
3. Postural hypotension
4. Repeated acute retention due to BPH
5. Repeated UTIs associated with BPH
b. Relative contra indication
1. Recent cerebrovascular disease
2. Strong positive history of syncope
3. Bladder stones associated with BPH
4. Gross hematuria
CLASSIFICATION OF THE ALPHA BLOCKER IN THE TREATMENT OF BPH
There are three sub groups of -blockers
a. Non selective -blockers (mixed -1 and -2 blocker):
Phenoxibenzamine
Pentolamin
Nicergoline
Thymoxamine
-
44
b. Short acting selective - blockers:
Prazosine
Alfuzosine
Indoramine
c. Long acting selective -1 blockers:
Terazosine
Doxazosine
Tamsulosine
Phenoxibenzamin is non selective -blocker is presently approved in
the USA for the treatment of pheochromocytoma. The dose may be
titrated up to 40 mg 3 times a day. In BPH phenoxibenzamin at a dose
0f 10 ml twice a day. Incidence and severity adverse reaction are
tiredness, dizziness, impaired ejaculation, nasal stuffiness, difficultly
with visual accommodation and sometimes gastric carcinoma after
prolonged high dose treatment. Because of this possibility its use is no
longer recommended
Prazosin for the treatment of BPH at a dose of 2 mg twice a day, the
peak urinary flow rate improved 59%. This drugs was initially introduce
as an anti hypertensive agent. Prazosin has been shown to inhibit
noradrenalin induced contraction of strips of both prostatic
adenoma and capsule in vitro experiment. The action of prazosin in
BPH demonstrated a significant improvement in symptom, a
significant increase of both the mean and maximum flow rate and
significant reduction in the post micturition residual volume
A variety of -adreno receptor blockers with distinct properties have
been develop as a possible treatment of BPH, the one most used is a
selective long acting -1 blockers group :
Terazosin (Abbot : Hytrin ) : 1 mg. 2 mg. 5 mg)
-
45
Doxazosin (Pfizer : Cardura ) : 1 mg 2 mg
Tamsulosin (Yamanouchi : Harnal ) : 0,2 mg
Terazosin and doxazosin has given dose titration : 1 mg. 2 mg. 5 mg.
20 mg and 1 mg. 2 mg. 4 mg. 8 mg. 12 mg. once daily
Side effect of Terazosin is tiredness , headache, palpitation, nasal
congestion, chest pain, nausea, dyspneu and decrease of libido
Side effect of doxazosin is : dizziness, fatigue, and headache
Doxazosin can be given the BPH patients whose in hypertensive or
unhypertensive condition
The most recommended is tamsulosin which is an -1A blockers, has
around a 30 fold selectivity, as compared with other -1 blockers to
smooth muscle of the prostate, its capsule and urethra. There are
negligible effects on the muscle of the blood vessels. The reasonable
efficacy and very low incidence of cardio vascular side effects,
makes tamsulosin when given once daily in a dosage of 0,2 mg or 0,4
mg without titration procedure as other -1 blockers.
Ad.3. PHYTOTHERAPY
The use of plants or plant extract for the treatment of symptoms
associated with BPH has been done since ancient times. It was
written on Egyptian Papyrus in the 15th century B.C.
It is also widely used in the Western hemisphere especially in Europe
In Germany and Austria, phytotherapy is the first line of drugs
treatment for LUTS caused by BPH, from mild to moderate symptoms
and represent more than 90% of all drugs used in treating BPH
In Italy 49% drugs used in treating BPH are plant extract where else
5-R inhibitor and 1-blockers are only used 5% each
-
46
Also, in Indonesia especially the use of Serenoa repens, pumpkin
seeds and those used in traditional mixtures
Compared with other medicamentous therapy, several researches
obtained result which displayed resemblance to Finasteride but for
more less efficacious compare with 1-blockers (Alfusozin or
Tamsulozin)
The working mechanism and active ingredients of phytoterapeutic
agents have not been identified and conformed because there is a
lot of controversy among researches depending on their experience
and clinical trial
PHYTOTHERAPY COMPONENT
This component can be divided into 4 groups :
Phytoterapeutic agents
Cholesterol lowering agent phytosterol with active
component, sitosterol and beta sitosterol
Amino acid complexes
Organ extract
These 4 groups overlap one another, so they are considered as one
group: Phytotherapeutic agents
Among the many plants commonly use, which extract is taken from :
the leaves, flower, fruit, seeds, bark, branch, root or the whole plant
as phytoterapy are :
Pygeum Africanum (African plum tree)
Populus Tremula (Aspen)
Serenoa Repens (Dwarf palm tree)
Echinacea Purpurea (Purple Cone Flower)
Cucurbita Pepo (Pumpkin Seeds)
-
47
Secale Cereola (Rye Pollen)
Hypoxis Rooperi (South Africans Star Grass)
Urtica Dioica (Stinging Nettle)
Aletrius Farinosa (Unicorn Root)
Sabal Cerula (Sago Palm)
For Example, the part of the plant extracted:
Taken from:
Root : Hypoxis Rooperi and Echinacea Purpurea
Fruit : Serenoa Repens
Bark : Pygeum Africanum
Seeds : Cucurbita Pepo
Leaves : Trembling Poplar
Flower/Pollen: Extract Protaflor
ACTIVE INGREDIENT
Plant extracts are a combination of several chemical components
There are water soluble and fat soluble
The active ingredients in lipids are composed of 85% - 95% fatty acid
and sterol
The fatty acid :
Free Fatty Acids (FFAs)
Fatty Acid ethyl-Esthers (FAEs)
Fatty alcohol
Phytosterol
Triterpenes
The sterol fraction :
Beta-sitosterol
-
48
Stigmasterol
Cycloartenol
Lupeol
Lupenone
Methyl-cycloartenol
Further studies of these extracts, its known that the ingredients that
inhibit 5-reductase are :
Lauric acid
Linoleic acid
Linolenic acid
WORKING MECHANISM
The actual working mechanism of the active ingredients is still not
clear, but a few hypotheses have been brought forth:
1. Anti inflammatory effects through interference with
prostaglandin metabolism
2. Alteration of cholesterol metabolism
3. Inhibiting prostate growth
4. Anti androgenic effect
5. Anti oestrogenic effect
6. Action within the liver reducing the production of Sex hormone
binding globulin (SHBG)
7. Inhibiting the production of Growth Hormones (bFGF & EGF)
8. Reducing smooth muscle tone around bladder neck, prostate,
prostate capsule and urethra prostatica
9. Inhibiting 5-reductase
10. Cytotoxic effect towards hyperplastic cells
11. Inhibiting the growth of prostate cancer cells
-
49
SEVERAL TYPE OF MEDICINAL PHYTOTHERAPY
Permixon (fruit serenoa repens), 320 mg / day for 1 month
Curbicin (cucurbita pepo & sabal serulata), 80 mg in dose 3x2 tab /
day for 3 month
IDS 89 (strogen) (serenoa repens), 3x2 caps (160 mg) / day for 12
week
Tadenan (Pygeum Africanum) with doses 2x1 capsule (50 mg) which
prevent contractil disfunction bladder neck given for 2 month
showed improved urinating symptom
Other researches that compared serenoa repens with finasteride and
1-blocker showed that finasteride was almost as effective as
serenoa repens (permixon 2 x 160 mg) but less effective than 1-
blocker (Alfusozin 3x2,5 mg)
SEVERAL DRUGS CIRCULATING IN INDONESIA
1. Lanaprost (Landson) Serenoa Repens extract 1-2 tab. (80-160 mg) /
day
2. Prostakur (Medikon) serenoa repens extract 2x1 caps. (160 mg)
3. Tadenan (Fourniers) Pygeum Africanum 2x1 caps. (50 mg)
4. Soprost (Soho) combination of Serenoa repens 80 mg with Cucurbita
pepo 80 mg + Zinc picalinate 15 mg / capsule. Dosage is 1-2 cap/day.
Similar to Curbicin but without Zinc and dosage of 3x2 tablets a day.
Ad.4.COMBINATION THERAPY
BPH can be treated with 1-adrenergic blockers drugs that relax
prostatic smooth muscle, bladder neck and prostatic urethra or with
drugs that inhibit 5-reductase and therefore reduce tissue androgen
-
50
concentration / prostate gland. However, the effects of the two types
of drugs have not been compared.
As compared 1-adrenergic blockers drugs with 5 reductase
inhibitor, finasteride, the onset of action of the 1-adrenergic blockers
is more rapid, they have no effect on serum concentration of PSA
and they can improve hypertension at the same time
As compared 5-reductase inhibitor, finasteride, with 1-blockers,
finasteride has minimal side effect, does not required titration at the
first of therapy and decrease prostatic size
Since this the different mechanism which these two type of
medications act, the next principal advance may come from using
them in combination
Lepor et.al. (1996). Compared the safety and efficacy of placebo
terazosin (10 mg daily), finasteride (5 mg daily) and combination of
both drugs in 1229 men with BPH. AUA symptom score and peak
urinary flow rates were determined at base line and periodically for
one year
This result from the base line in the symptoms score in the placebo,
finasteride, terazosin and combination therapy groups were
decrease of 2,6 , 3,2 , 6,1 , and 6,2 points, respectively (p < 0,001) for
the comparisons of both terazosin and combination therapy with
finasteride and with placebo.
In the peak urinary flow rate were increase of 1,4 , 1,6 , 2,7, 3,2 per
second, respectively (p < 0,001) for the comparisons of both terazosin
and combination therapy with finasteride and with placebo.
-
51
Conclusion :
In men with BPH terasozin was effective therapy whereas finasteride
was not, and the combination of terazosin and finasteride was no
more effective than terasozin alone
II. CONVENTIONAL SURGICAL THERAPY
The indication for prostatectomy may be divided into: Absolute and
Relative indication
Absolute indications :
1. Chronic obstruction and azotemia
2. Chronic obstruction and bladder neck stone
3. Recurrent retention of urine
4. Chronic obstruction with upper tract dilatations bladder
trabeculation and diverticulation
5. Recurrent urinary tract infection
6. Recurrent hemorrhage from prostatic vessel
7. IPSS severity
8. Urine flow: maximum flow rate of urine (Q-max): < 10 ml /sec.
Relative indications :
1. Total acute urinary retention for the first times
2. Chronic obstruction with mild changes of the upper urinary
tract
3. Recurrent prostatitis
4. Bladder stone
5. Clinical grading III (residual urine > 100 ml)
6. BPH associated with :
Asthmatic patient
Cardio-vascular disease
-
52
Diabetes mellitus
Hernia
7. IPSS moderately
8. Urine flow : Maximum flow rate of urine (Q-max) : 1015 ml/sec
Although most patients will now be considered able to tolerate the
regional/spinal or general anasthesia necessary for prostatic surgery
there are still some important contraindications :
1. Severe anesthetic risk due to pulmonary or cardiac disease
2. Anti coagulation or bleeding disorders
3. Neurological disease such as Alzheimers, Parkinsons, cerebral
hemorrhage
4. Striated spinchter weakness
There are two procedures of the conventional surgery therapy :
1. Open prostatectomy, consist of :
a. Supra pubic transvesical prostatectomy
b. Supra pubic retro pubic prostatectomy
c. Perineal prostatectomy
2. Endoscopy prostatectomy :
a. Trans urethral resection of the prostate (TUR-P)
b. Trans urethral incision of the prostate (TUI-P)
Method procedure of surgery depending upon the size of gland as
assessed by digital rectal examination and trans rectal ultra
sonography (TRUS)
A report focuses on a pilot study now underway dividing men with
significant signs and symptoms of BPH into three classes :
Class I : BPH is 20-50 grams in size : Randomization will be TURP,
balloon dilatation, medical therapy or watchful waiting
-
53
Class II : BPH is 51-80 gram in size : randomization is between TURP
and open prostatectomy
Class III : BPH is greater than 81 gram in size all patients undergo
open prostatectomy
In the Wahidin Sudirohusodo general hospital Makassar TURP for the
gland which less than 50 gram in size. While, BPH which more than 50
gram reserve to open prostatectomy for the trainee / resident of
Department of Surgery of Medical Faculty, Hasanuddin University
The choice of operation procedure is a personal matter the surgeon /
urologist and the patient what it is preferred
Ad. 1a. SUPRA PUBIC TRANSVESICAL PROSTATECTOMY
This approach to the removal of the very large prostate gland or
patients where there is co.existing bladder pathology e.q. large-stone
or diverticulum
TECHNIQUE:
This technique was popularized by Peter Freyer (1902)
1. The patient is positioned supine and in the little Trendelenburg
position
2. The supra pubic mid line incision or a transverse Phannenstiel incision
which is more preferred
Fig.14. This position to allow the intestine to fall away from the area of the
bladder (Ref. Scott p.235)
-
54
3. After the abdominal wall is opened, urinary bladder is filled water or
saline about 150-200 cc, to identify the bladder with aspiration the
water
4. A longitudinal incision in the bladder
5. After the bladder is opened, it is inspected for coexisting pathology,
prostate gland & internal urethral orifice and ureteric orifices
6. Circular incision is made in the bladder mucosa a round the bladder
neck/internal urethral meatus, with careful avoidance of injury to the
ureteric orifice and avulsion of the bladder mucosa, when the
adenoma is enucleated
7. The internal meatus is identified and the index finger passed into this
meatus to stretch it. This maneuver should break the anterior
commisura and allow separation of the lobes of the prostate (Fig.15a)
8. The plane between the false capsule and the prostatic adenoma is
found and the lateral lobes are enucleated. The enucleation usually
breaks the urethra at the apex of the prostate. This may be assisted
by the presence of the gloved index finger in the rectum. The apical
enucleation and breaks, the urethra should be done sharply to avoid
injury to the external urethral sphincter. (Fig.15 b)
9. A self retaining catheter-three ways 24 F is inserted to urethra
10. Under direct vision any obvious bleeding points in the prostatic-bed
are diathermied
11. Hemostatic suture are inserted through the junction of the prostatic
fossa and the bladder neck (Hryntschaks suture) (Fig.15c)
12. The bladder and wound are closed and a tube drain is left on the
retro pubic space (Fig.15d)
13. Catheter was put in traction and fixation at the medial part of the
right patella
-
55
14. The bladder is irrigated to wash out any blood clot
Fig. 15. Supra pubic transvesical prostatectomy technique. (Ref.Scott p.235-
236)
Ad. 1b. SUPRA PUBICRETRO PUBIC PROSTATECTOMY
Retro pubic prostatectomy (RPP) was developed and popularized by
Terrence Millin and is preferred by most urologists
It give a more direct approach to the prostate by virtue of the fact
that the bladder is not opened
Sometimes a preliminary cystoscopy is performed and the bladder is
inspected to eliminate any coincidental pathology
a b
c d
-
56
TECHNIQUE
1. The patients is positioned with head down to allow the intestine to fall
away from the area of the bladder and to open up the retro pubic
space (Fig.16a)
2. A transverse Phannenstiel incision is preferred
3. The bladder which should be empty is identified and retracted
posteriorly. This further open up the retro pubic space (Fig.16b)
4. Prostatic capsule is identified and a transverse incision in the anterior
prostatic capsule after ligation of the overlying venous plexus
(Fig.16c)
Fig.16 a,b,c. Supra pubic retropubic prostatectomy technique. (Ref.Scott
p.232)
5. The plane between the prostatic adenoma and the false capsule
and adenoma is enucleated with the index finger and using scissors
the urethra is divided proximal the external urethral sphincter with
care being taken to avoid injury to the sphincter (Fig.16 d,e,f)
a b c
-
57
6. Control hemorrhage with a swab is placed in the prostatic cavity and
any obvious bleeding points are diathermied (Fig.16 g)
7. Any small tags tissue are excised and a wedge of tissue is removed
from the posterior bladder neck
Fig. 16 d,e, f, g. Supra pubic retropubic prostatectomy technique. (Ref.Scott
p.233)
8. The bladder mucosa of the posterior lip of the bladder neck is then
suture down into the row cavity of the posterior urethra (Fig.16 h)
d e
f g
-
58
9. A simplastic self retaining three ways catheter no 24 F is passed up
the urethra into the bladder and the prostatic capsule is closed
(Fig.16i)
10. The wound is closed after a tube drain is inserted into the retro pubic
space (Fig.16 i)
Fig.16 h, i. Supra pubic retropubic prostatectomy technique. (Ref.Scott
p.234)
POST OPERATIVE MANAGEMENT OF TRANSVESICAL AND RETRO PUBIC
PROSTATECTOMY
Care must be paid to the efficient drainage of the catheter, irrigation
should be discourage as it may be infection
Sedation and analgetic, beside antibiotic, should be aimed at keeping
feels pain, there is tendency for him to strain. This will cause pelvic an
engorgement and promote venous hemorrhage and clot formation
catheter will be obstructed
Intra venous fluids will be required for the first 24 hours after operation or
until the patients is able to drinks freely without gastrointestinal upset
h i
-
59
Early mobilization is to be encourage and the patient should sit out of
bed the day after the operation
When the urine is relatively free from blood the urethra catheter is
removed 4-5 day after operation, if the fluid at the drain tube from retro
pubic space has eliminated
The patients is warned that initial his urinary control may be poor but is
encourage to perform perineal exercises to regain control quickly
(Kegels exercises)
POST OPERATIVE COMPLICATION OF TRANSVESICAL AND RETRO PUBIC
OPERATION
1. Hemorrhage :
Varying hemorrhage during operation
Profuse from all surface of the prostatic cavity
Arterial hemorrhage
Secondary hemorrhage :
It commonly arise about the 6th 8th post operative day
and can be quite perfuse
Secondary hemorrhage is not uncommon if there is any
degree bladder infection
2. Incontinence may be caused by sphincter injury or long term
catheterization
3. Infection are common after prostatectomy and may present in different
sites : wound, bladder, urethra, kidney, epididimitis/orchitis
4. Urinary fistula are usually due to deficient closure of the bladder of
prostatic cavity
-
60
5. Bladder neck stenosis can occur as a result of healing where excessive
fibrous tissue is laid down or where excessive Hryntschaks suture. This
may be promoted be bladder infection
6. Urethral stricture can develop in the posterior urethra
7. Impotence and retro grade ejaculation. The impotence is most likely to
be permanent and does not to administration of androgens
Ad. 1C. PERINEAL PROSTATECTOMY
This method of prostatectomy is not employed in this country (Indonesia)
but is more commonly used in USA. (Formerly about 1950-1965 Indonesia
had a expert in this method: dr. Rudi E. Tan : First chief of Department of
Surgery, Medical Faculty, Hasanuddin University).
TECHNIQUE
1. The patient is placed in the exaggerated lithotomy position (Fig.17a)
2. The incision is made the anterior to the subcutaneous anal sphincter.
Care is taken to avoid damage to the anterior rectal wall (Fig.1b)
3. The perineal muscle are separated to expose the prostatic capsule
4. The capsule is opened and the plans of cleavage between the
adenoma and the false capsule identified (Fig.17c)
a b c
Fig.17 a,b,c. Perineal prostatectomy technique (Ref.Scott 240)
-
61
5. The prostatic urethra is identified under vision and divided at the apex of
the prostate (Fig.17d)
6. The hypertrophy portion of the gland is removed and the bladder neck is
sutured to the membranous urethra after is inserted a self retaining three
ways catheter 24 F (Fig.17e)
7. The prostatic capsule then sutured and the perineal wound is closed
with adequate drainage
Fig. 17 d,e, Perineal prostatectomy technique (ref. Scott p.241)
COMPLICATION:
1. Impotence. It is a most complication of this method. For this reason this
method is little employed to do it, and it seem the main contra
indication especially the slightly younger patient
2. Hemorrhage
3. Damage to the rectal wall
4. Urinary fistula
5. Infection
d e
-
62
2A. TRANS URETHRAL RESECTION OF THE PROSTATE (TURP) = TRANS URETHRAL
PROSTATECTOMY
TURP is the most widely accepted method of treating prostatic
urethral obstruction in patients with BPH and is considered the Gold
standard against which other treatment should be compared
PROCEDURE
1. The patient is anesthetized (usually spinal) and lithotomy position.
Preliminary cystoscopy is perform to identify the ureteral orifices, bladder
neck and Verumontanum (Fig.18a)
2. A well lubricated resectoscope is passed
3. The irrigating fluid is a glycin is preferred to prevent hemolysis should
some be absorbed into the prostatic plexus. For this reason is not be
suggested to use water, since is always occurred hemolysis and other
post TURP syndrom e.q. hypervolemic, hyponatremic state due to
absorption of the hypotonic irrigating solution, likely water
(aquabidestilata). Clinical manifestation of the post TURP syndrome
include: nausea, vomiting, confusion, hypertension, Bradycardia and
visual disturbances. The risk of TURP syndrome increase with resection
time over 60 minutes
4. Resection is begun by excising the tissue in the bladder neck. This is
usually from a median bar or a formal median lobe to above the
verumontanum. Resection should not be carried out below the
landmark (verumontanum) to prevent damage at the external urethral
sphincter. The posterior urethra were regarded as a time piece this part
of resection would be from 5 oclock to 7 oclock (fig.18b & c)
5. The lateral lobes are then excised at position 10 oclock and 2 oclock.
The lateral lobes will fall towards the mid line making resection easier. The
-
63
prostate is excised fully till the cris-cros fibers of the fats capsule are
seem. Any obvious bleeding points are controlled under vision by
diathermy
6. The anterior lobes and the apex of the gland near the verumontanum
and external urethral sphincter are the resected (Fig.18d)
7. The resected pieces of chippings of prostate are evacuated with Elics
evacuator
8. A self retaining three ways catheter is inserted and urine is drained
continuously. Catheter is tracted and fixation in the medial part of the
right knee
Fig. 18a, b. (ref. Kirby p.48)
Trans urethral resection of the
prostate (TURP) is accomplished
using the cutting loop of a
resectoscope
a
b
Enlargement of the right
and left lobes prostate
gland and verumontanum under cystoscopic viewed
-
64
Fig. 18.c,d . Ref. Kirby p.49
HAZARD OF TURP
1. Hemorrhage :
Primary hemorrhage hemorrhage during operation or after post
operatively
Secondary hemorrhage 7-12 days post operatively, can develop if
there is bladder infection
2. Damage the ureter during the resection
3. Perforation of the bladder especially at the posterior of the bladder neck
The prostate is removed piecemeal and
the chippings are evacuated from the
bladder. Careful haemostasis is then
achieved using diathermy coagulation
c
d
-
65
4. Damage to the external urethral sphincter : such damage can lead to
dribbling incontinence
5. Damage to the urethra at operation may lead to urethral stricture. This
can be at the external meatus or in the posterior urethra
6. Epididymitis. This can occur especially if the urine is infected pre
operatively
7. Impotence can occur after transurethral resection of the prostate.
8. Post TUR-P Syndrome
This syndrome resulting from a hypervolemic, hyponatriemic state due to
absorption of the hypotonic irrigating solution. Clinical manifestation of
the TUR-P syndrome includes nausea, vomiting, confusion, hypertension,
dyspneu due to lung oedem, bradycardia and visual disturbances. The
risk of TUR syndrome increase with resection time over 60-90 minute. In
severe cases, treatments include diuresis and hypertonic saline (Sol NaCl
3%) administration, but the patient sometimes died.
Advantages of TURP:
Avoidance of an abdominal wound
Blood loss tend to be less than for operation
Period of catheter drainage is slightly shorter
Stay in hospital is shorter
2b. TRANS URETHRAL INCISION OF THE PROSTATE (TUIP)
TUIP is made with the Collins knife between the trigonum and the
verumontanum at seven oclock position
Incision line runs from the ureteric orifice to the verumontanum. This
procedure is associated with less retrograde ejaculation and a lower
complication rate than the standard TURP (Fig.19a)
-
66
Once the incision has been made, usually be electro cautery the
bladder neck and prostatic urethra should spring open resulting in an
improved flow rate and more complete bladder emptying (Fig.19b)
Fig.19a,b. Incision from the ureteric orifice to the verumontanum (ref.
Kirby p.50)
III. INTERVENTIONAL TREATMENT = MINIMAL INVASIVE
= INVASSIVE NON OPERATIVE TREATMENT
All patients for minimally therapy must really be BPH for that reason. It is prior
biopsy to eliminate Ca.P.
1. BALLOON DILATATION
There are two types of prostatic balloon dilatation system :
a b
-
67
a. A disposable endoscopic system allowing visualization to
ensure correct position of the balloon, so the distal sphincter
was not dilated (Fig.20)
b. Optilume prostatic balloon. This type used a l