Benign Epilepsy of Children with Centro-Temporal EEG …900147/FULLTEXT01.pdf · Benign Epilepsy of...
34
Benign Epilepsy of Children with Centro-Temporal EEG Foci Clinical, Genetic and Neurophysiological Studies AKADEMISK AVHANDLING SOM MED VEDERBÖRLIGT TILLSTÅND AV REKTORSÄMBETET VID UMEÅ UNIVERSITET FÖR AVLÄGGANDE AV MEDICINE DOKTORSEXAMEN KOMMER ATT OFFENTLIGEN FÖRSVARAS I SAMHÄLLSVETARHUSET, SAL D, LÖRDAGEN DEN 8 MAJ 1976 KL.9.15 AV JAN HEIJBEL med. lic. UMEÂ 1976
Transcript of Benign Epilepsy of Children with Centro-Temporal EEG …900147/FULLTEXT01.pdf · Benign Epilepsy of...

Benign Epilepsy of Children with Centro-Temporal EEG Foci
Clinical, Genetic and Neurophysiological Studies
A K A D E M I S K A V H A N D L I N G
SOM MED VEDERBÖRLIGT TILLSTÅND
AV REKTORSÄMBETET VID UMEÅ UNIVERSITET
FÖR AVLÄGGANDE AV MEDICINE DOKTORSEXAMEN
KOMMER ATT OFFENTLIGEN FÖRSVARAS
I SAMHÄLLSVETARHUSET, SAL D,
LÖRDAGEN DEN 8 MAJ 1976 KL.9.15
AV
JAN HEIJBELm ed. lic .
UMEÂ 1976


UMEÀ UNIVERSITY MEDICAL DISSERTATIONSNew Series No. 17 1976
From the Departments of Clinical Neurophysiology and Pediatrics, University of Umeå, Umeå, Sweden
Benign Epilepsy of Children with Centro-Temporal EEG Foci
Clinical, Genetic and Neurophysiological Studies
BY
JAN HEIJBEL
UMEA 1976


3
Contents
1 Definitions Page 4
2 Introduction 5
3 Present investigations 6
3.1. Aims 6
3.2. Materials and methods 6
3.2.1. Materials 7
3.2.2. Methods 10
3.2.3. Classification of epileptic seizures 12
4 Summary of previous and present investigations 13
4.1. Age 13
4.2. Sex 14
4.3. Incidence and prevalence 14
4.4. EEG findings 14
4.5. Symptomatology of seizures 16
4.6. Relation to cerebral lesions 17
4.7. Genetic factors 17
4.8. Intelligence, behavior and school adjustment 18
4.9. Therapy 19
4.10. Prognosis 19
5 General conclusions 20
6 Summary 24
7 Acknowledgements 25
8 References 27

4
1 Definitions
Rolandic: Referring to Rolandic fissure = sulcus centralis. The Rolandic area corresponds roughly to areas 4 and 6, and to areas 3, 1 and 2 in Brodman's classification of the cerebral cortex (12).(Luigo Rolando, Italian anatomist, 1773-1831).
Rolandic discharges: Spikes or sharp waves recorded with their maximal amplitudes in the centro-temporal region and often, but with lower amplitudes, in the posterior-frontal and parietal region and with a normal background activity.
Discharge rate: Mean number of Rolandic discharges per minute.
Epileptic seizures: Symptoms of cerebral origin appearing suddenly and ceasing spontaneously usually with disturbances of consiousness and/or motor, sensory, psychical and autonomous manifestations.
Epilepsy: The state of having repeated epileptic seizures during the last three years.
Febrile convulsions: Short generalized seizures before the age of 5, appearing in connection with fever, seldom with a duration of more than a few minutes and without symptoms or signs of cerebral infection or poisoning.
Incidence rate: The number of new cases occuring during one year, the incidence year, and expressed as cases per 100 000 of the population at risk.
Prevalence of epilepsy: All patients who have had epileptic seizures during the last three years before a given day expressed as cases per 1000 of the population at risk.
Sharp wave: A wave, distinguished from background activity, with a duration of more than 1/12 and less than 1/5 s (21).
Spike: A wave, distinguished from background activity and having a duration of 1/12 s or less (21).

5
2 Introduction
In 1952 Mme Y Gastaut described in her study "Un élément déroutant de la séméiologie électroencéphalographique: les pointes prérolandiques sans signification focale" (22) the EEG changes, which have been calledRolandic spikes, Rolandic paroxysms and Rolandic discharges. These EEGchanges, which occur during a limited period of childhood only, and the clinical symptoms coupled to them have been studied to some extent by clinical neurophysiologists and neuropediatricians, especially in France.
The purpose of this summary is to survey our present knowledge about benign epilepsy of children with centro-temporal (Rolandic) EEG foci. First a short description of our own investigations, their aims, materials and methods is given, followed by a report on this kind of epilepsy from different points of view, based on the results of investigations both our own and others.
The observations are based on the following five papers. In the textthey are designated by Roman numerals.
I Heijbel, J, Blom, S and Bergfors, PG. Benign Epilepsy of Childrenwith Centro-Temporal EEG Foci. A Study of Incidence Rate in Outpatient Care. Epilepsia in press.
II Heijbel, J, Blom S and Rasmuson, M. Benign Epilepsy of Childhood with Centrotemporal EEG Foci. A Genetic Study.Epilepsia, 16: 285-293, 1975.
III Blom, S and Heijbel, J. Benign Epilepsy of Children with Centro- Temporal EEG Foci. Discharge Rate During Sleep.Epilepsia, 16: 133-140, 1975.
IV Heijbel, J and Bohman, M. Benign Epilepsy of Children with Centro-Temporal EEG Foci. Intelligence, Behavior and School Adjustment.Epilepsia in press.
V Blom, S, Heijbel, J and Bergfors, PG. Benign Epilepsy of Children with Centro-Temporal EEG Foci. Prevalence and follow-up study of 40 patients. Epilepsia, 13: 609-619, 1972.

6
3 Present investigations
3.1. Aims
The aims of the investigations were
- to determine the incidence rate of epileptic seizures with Rolandic discharges in a well-defined population of children and to relate this kind of seizure to other forms of epileptic fits (I).
- to test the hypothesis that an autosomal, dominant gene with age- dependent penetrance is responsible for the EEG trait (II).
- to study the discharge rate during sleep, both quantitatively and during different stages of sleep (III).
- to investigate whether school children with this epilepsy differ from children of the same age without epileptic seizures as ragards intelligence, behavior and adjustment to school. (IV).
- to determine the prevalence rate (V).
- to investigate the long-term prognosis (V).
3.2. Materials and Methods
A short summary is given of the materials studied, and the methods used. For details, see the respective papers.
The Table 1. on pages 8-9, shows 32 of the 121 children who took partin investigations I-IV. It can be seen from the table which investigations they took part in. Cases 30, 31 and 32 were added during the investigation of the incidence rate (I). 5 out of the 94 children whotook part in study V took also part in studies II, III, and IV ascases 1, 5, 13, 19 and 28.

7
3.2.1. Materials
3.2.1.1. The Incidence Study (I)
The incidence rate of epileptic seizures (including febrile convulsions) was determined in a population of 52,252 children in the age-group 0 -15 years in the County of Västerbotten in the northern part of Sweden.The investigation was carried out over a period of 12 months, starting on February 1, 1973 and ending on January 31, 1974. This period was called the incidence year. From this material the incidence rate of epileptic seizures with Rolandic discharges was determined.
3.2.1.2. The Genetic Study (II)
In the genetic study 19 children, 10 boys and 9 girls, with at least onesibling between 3 and 13 years of age were selected as probands. Theywere taken from a material of 29 children 4 - 1 7 years old, withoutneurological symptoms other than the seizures. 34 siblings and 36 parents were included in the investigation.
3.2.1.3. Discharge Rate during Sleep (III)
24 out of 29 children, studied in paper II, took part in the investigation. The results obtained from 17 children, 8 boys and 9 girls were analyzed.7 children were excluded. (One child did not fall asleep and six children had no Rolandic discharges either during wakefulness or while asleep at the time of the investigation).
3.2.1.4. Intelligence, Behavior and School Adjustment (IV).
16 out of the 29 children, studied in paper II, 7 boys and 9 girls, between 7 and 12 years old, were selected for this study. They were attending ordinary primary schools where the teachers knew the pupils in the class well. They also lived within a distance of 40 km from Umeå, where the investigation was carried out. A class-control of the same sex and age was randomly chosen for every proband.

Table
1. The
children
with
Rolandic
discharges
arranged
according
to sex
and
age
at onset
of se
izur
es.
8
30 (HGS)

9
o CM
O om vD
co o
CO 00Csl CM CM CO
partial
seizures
only.
G: generalized
seizures
only.
SG: secondarily
generalized
seiz
ures.
Rolandic
discharges.
(+):
febrile
conv
ulsi
on.

10
3.2.1.5. Prevalence and Prognosis (V)
94 children, 54 (57%) boys and 40 (43%) girls, with Rolandic discharges and epileptic seizures took part in this investigation. The calculation of the prevalence rate was based on these 94 children.In the study of the prognosis, those 40 children (26 boys and 14 girls) who were older than 15 years were selected.
3.2.2. Methods
3.2.2.1. Clinical Examinations (I, II, III, IV, V)
The histories and the hospital records were studied with special reference to heredity, perinatal complications, psychomotor development, previous cerebral disorders and epileptic seizures, earlier examinations, especially neuroradiological investigations, therapy and the descriptions of the seizures. During the follow-up work the patients were also interviewed about their school records, occupations, military service and possession of a driver’s license.
Somatic and neurological examinations were performed and one or more EEGs were recorded on every child. Most of them also underwent skull X-rays and laboratory screening, the latter to show or to exclude disorders of calcium, carbohydrate and protein metabolism and infections of the central nervous system.
In the study of the incidence rate (I) all physicians and district nurses involved in the care of acutely sick children were informed about the project and its purposes. They were requested to refer every child who had its first epileptic seizure during the year in question.

11
3.2.2.2. EEG Recordings (I, II, III, IV, V)
The EEG recordings of the children (in the genetic study (II) of the siblings and parents too) were made on a 16-channel (in some cases on an 8-channel) EEG-Mingograph. In the retrospective prognostic study (V) most of the recordings were made on an 8-channel or a 16-channel Grass electroencephalograph. In all cases the electrodes were placed according to the 10-20-system (28) with both longitudinal and transverse montages covering the central and temporal regions simultaneously. The EEGs also included if possible photic stimulation and hyperventilation. Sleep was induced with mebumal sodium 50-200 mg or chlorpormazine 25-50 mg by mouth, the dosage depending on age and body weight.
In the study of the discharge rate during sleep (III) Rolandic discharges were counted and the frequency expressed as mean number per minute for each stage of sleep (18,47,53). Stages of sleep were classified according to Loomis et al (41): Stage A, drowsiness; stage B, falling asleep; stage C, light sleep; stage D, middle-deep sleep; stage E, deep sleep.
3.2.2.3. Psychological Methods (IV)
Terman-Merrill1s intelligence test, Form L (52), standardized according to Swedish conditions (27) was used to test intelligence and memory function and Benderfs visual motor gestalt test (7) to test visuomotor co-ordination. The results of Benderfs test were scored according to Pascal and Suttell (46).
3.2.2.4. Interviews with Teachers (IV)
Teachers were interviewed on the telephone by a social worker, trained to carry out interviews (11, 42). In these the probands were compared as a group with all their classmates of the same sex and individually with randomly selected class-controls of the same age and sex according to various behavioral and other characteristics of importance for the school adjustment.

12
3.2.2.5. Statistical Methods (III, IV)
Wilcoxon's test for paired observations was used to evaluate the difference between discharge rates in the various stages of sleep (III).The same test was also used when the probands were compared individually, and the chi square test when they were compared as a groups with their class-controls as regards different behavioral and other characteristics (IV). Studentfs t-test was used to evaluate the difference between the mean IQ values of the probands and their class-controls and the F-test to evaluate the difference between the variances (IV) (49).
3.2.2.6. Test of the Genetic Hypothesis (II)
The observed number of affected and non-affected children (oüt of 19 sib- ships) was tested against that expected from the dominant or recessive mode of inheritance with the so-called a priori method (51).
3.2.3. Classification of Epileptic Seizures (I)
The classification of the epileptic seizures was made according to that recommended by The International League Against Epilepsy (20). However, in the classification of epileptic seizures with Rolandic discharges only the EEG findings were used regardless of the nature of clinical seizures.

13
4 Summary of previous and present investigations
4.1. Age (I, V)
Rolandic discharges have not been observed before 2 years of age.They begin to appear between 2 and 6 years of age (38, 48) and disappear spontaneously after a duration of from 6 months to 13 years or at puberty (1,4,9,16,32,38). Occasional cases of Rolandic discharges have been discribed in adults (3,25).
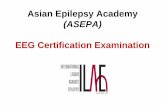
The epileptic seizures start between 1 and 14 years of age with a maximum between the ages of 4 and 10 (1,2,4,9,19,30,37,43,44,45).The column diagram in figure 1. shows the age of the children in studies I-1V at their first seizure. These disappear a couple of years after their first appearance or at puberty (1,9,16,29,30,32,37,43,50).
5
5 10Age, years
Fig.l. Histogram of the age of the children with Rolandic discharges at their first seizure.

14
4.2. Sex (I, II, V)
In many materials there is a certain predominance of boys (4,8,9,32,37,43) but a definite sex difference has not been verified (1,24,25).
4.3. Incidence and Prevalence (I, V)
No earlier investigations of incidence and prevalence rates seem to have been performed for benign epilepsy of children with Rolandic discharges. Sorel and Rucquoy-Ponsar (50) however found that 7.4% of 2303 children with epilepsy had Rolandic discharges and Lerman and Kivity that (32)14,4% of 360 children with epilepsy had them.
In the Swedish County of Västerbotten the incidence rate for epileptic seizures with Rolandic discharges is 21/100 000 (24) and the prevalence rate for this kind of epilepsy is 1.1/1000 (9). 15,7% of the children with their first epileptic seizure during the incidence year had Rolandic discharges (24).
4.4. EEG Findings (II, III, V)
The EEG findings (Rolandic discharges) consist of diphasic, monophasic or polyphasic spikes or sharp waves with an amplitude of 100-300 microvolt. They are often followed by a slow wave of lower amplitude and have a total duration of about 300 ms (1,2,19,22,35,38). They appear solitarily with a frequency of 1 per 20 min to 3/min or in clusters, often with a pseudorhythm of 1,5-4 Hz and seldom with a longer duration than 3 s (1,6,9,16,19 22,32,35,38,43,45). They are located in the prerolandic or Rolandic area (1,2,6,9,12,19,22,35,37,43,45). Lombroso (40) studied the area of maximal amplitude and found that it is situated in the central or centro-temporal regions. Rolandic discharges can spread to adjacent regions, especially to the middle and posterior temporal regions, however the amplitudes are there lower. The extension seems to be dependent on the height of the maximal amplitude (1,6,19,35,38,40,43). The forward migration of an occipital focus to the middle temporal region described by Gibbs and Gibbs (23) has not been observed by other authors in this type of epilepsy (19,40).

15
As a rule Rolandic discharges appear unilaterally but they may also occur bilaterally, synchronously or side-shifting from two foci .apparently independent of each other, of which the one with higher amplitudes dominates the other (1,2,3,4,6,9,22,35,38,43). Rolandic discharges can shift sides in two successive recordings (9,44) or may disappear in one or more recordings, which are entirely normal, to reappear in the subsequent ones (1,9,43). The background activity is normal(1,4,6,19,40).
The frequency of Rolandic discharges increases significantly during drowsiness and light sleep. Some children have Rolandic discharges during sleep only (10,19,35,38,43,45). Sometimes the frequency of Rolandic discharges increases when the eyes are opened and decreases during muscular effort. As a rule they are uninfluenced by hyperventilation and photic stimulation (2,4,6,19,22,35,38,43). Mu rhythms sometimes exist together with Rolandic discharges (3,22). Bilaterally synchronous 3 Hz spike-and-wave activity and Rolandic discharges may appear in the same EEG with or without corresponding clinical manifestations. In connection with hyperventilation and/or photic stimulation short bursts of generalized bilaterally synchronous spike-and- wave activity can occur. (1,3,4,9). Rolandic discharges can appear in normal children without neurological symptoms and without epileptic seizures (2,4,18,25,45).
Recently, an EEG has been recorded in one patient during a seizure (17). At the onset of this seizure focal low voltage fast activity was recorded over the centro-temporal region in one hemisphere, spreading to the whole ipsilateral hemisphere and finally to the contralateral. In connection with the cessation of the seizure the activity ended abruptly without postictal flowing.

16
4.5. Symptomatology of Seizures (I, V)
Most seizures (55-75%) appear on falling asleep, during sleep or«at awakening. Three types of seizures exist: Partial and secondarily and primarily generalized seizures. The last may of course in many cases in reality be secondarily generalized, especially when they occur during nocturnal sleep and their onsets have not been observed. The manifestations of the seizures can be motor (tonic contractions or clonic twitchings), sensory (paraesthesias of various kinds and pain) and autonomous (hypersalivation). These manifestations occur fairly often during one and the same seizure (1,2,4,9,16,19,24,29,30,34,35,36,37,39, 40,43,44,45,50).
During the partial and at the beginning of the secondarily generalized seizures the symptoms often occur simultaneously in the facial, mouth and throat regions. These are the so-called oropharyngeal seizures which are typical but not crucial for this form of epilepsy. The oropharyngeal symptoms, which occur in over half of the fits, consist of: increased salivation, which can sometimes be very pronounced; guttural sounds which occur especially during nocturnal seizures and consist of various sounds from the mouth and throat; twitchings of lips and tongue; paraesthesias in the mouth cavity with sensations of dryness or pricking in throat, tongue or inner cheeks; contraction of jaws with inability to open the mouth; tonic contraction of tongue with deviation or difficulties in moving it; inhability to swallow and feelings of suffocation (1,9,24,34, 37,40,43).
The partial seizures can also occur on one side of the face only with contractions, twitchings or paraesthesias around the eye, in the cheek or at the corner of the mouth. They may also appear in the upper or lower extremities unilaterally or bilaterally. Jacksonian march has been described but is seldom found (40). The generalized seizures include both tonic and clonic convulsions.

17
Consciousness may be completely preserved during the whole partial seizure (in 58% of seizures according to Loiseau and Beaussart) (34) but can also be affected to various degrees down to complete unconsciousness. During the generalized seizure the patients are as a rule completely unconscious (9,24,34,37,43).
Inability to speak exists in a great number of seizures with consciousness entirely maintained. During these seizures the patients hear and see everything but they cannot talk to people around them. Yet, some patients can communicate by gestures, others emit inarticulated sounds. The parents often consider the children more or less unconscious(1.34).
Epigastric pain, vomiting, blindness and flashing lights rarely occur(1.34).
4.6. Relation to Cerebral Lesions (I, V)
The medical history before the beginning of the seizures is usually scanty. As a rule these children were healthy before their first convulsion. In general perinatal complications are few. Symptoms of cerebral lesions may be found but no connection is believed to exist between the cortical lesions and the Rolandic discharges (1,2,6,8,9,22,32,35,38,43, 45,48).
4.7. Genetic Factors (II, V)
In parents, siblings and other relatives of children with benign epilepsy of childhood, this type as well as other types of epilepsy have been observed (1,4,5,9,25,38).
Bray and Wiser (13) found a much higher incidence of temporo-central spike discharges in near relatives of children with focal "temporal lobe-epilepsy" than in a matched control group. They observed in their material two types of epilepsy: temporo-central spikes in combination with focal or generalized seizures in children, and anterior temporal spike foci in combination with

18
psychomotor seizures in adults. From an analysis of "EEG Icindred diagrams" the same authors (14) drew the conclusion that focal "temporal lobe spike discharges", independent of the symptomatology of seizures, were transmitted by an autosomal, dominant gene with age-dependent penetrance. According to the definition of these authors epilepsies with epileptic discharges other than Rolandic discharges are included in their material too.
In the genetic study (II) it was shown that an autosomal, dominant gene with age-dependent penetrance is responsible for the EEG trait in benign epilepsy of children with centro-temporal EEG foci. Recessive and multifactorial inheritance were excluded.
4.8. Intelligence, Behavior and School Adjustment (IV)
Investigations using controls as regards the intelligence, behavior and school adjustment of children with benign epilepsy of childhood have not been carried out earlier. Yet, mental retardation, abnormalities of behavior and difficulties in adiusting to home and school have been observed in these children (1,6,19,37,43,48). Aicardi et al (1) did not get the impression that these problems were greater in children with benign epilepsy of childhood than in children with other types of epilepsy, if anything, they were more moderate. They were of the opinion, that the abnormalities observed were related to the psychic factors in the environment of the child with epilepsy, its family and the results of antiepileptic therapy.
From study IV it appears that there are no differences between children with benign epilepsy and Rolandic discharges (without symptoms other than the fits) and controls of the same sex and age regarding intelligence, behavior, school adjustment and memory. Their visuomotor co-ordination and perception were however poorer than their controls. The cause is yet unknown. Timely information given to the parents about the benign nature of this type of epilepsy and adequate medical treatment given to the children have probably reduced the risk of anguished reactions, over-protection and rejection on the part of the parents and in turn of emotional disturbances in the children.

19
4.9. Therapy (V)
As a rule the therapy is simple and successful with phénobarbital and diphenylhydantoin in low or moderate doses (1,4,6,9,19,37,40,44). The risk of relapse into seizures is considered to exist if the therapy is discontinued too early (35), or between 13 and 15 years of age, if the child has not been seizurefree for 2-3 years and the EEG is not normal (1). Carbamazepine has also been shown to have a good effect in adequate doses (31).
4.10. Prognosis (V)
Rolandic discharges and epileptic seizures cease either during therapy or spontaneously, usually at puberty (1,2,4,9,16,32,38). This is ascribed to the effect of cerebral maturation (2,16). Occasional cases of Rolandic discharges have been observed in adults (3,25).

20
5. General conclusions
From own studies of incidence and prevalence rates (9,24) it is evident that benign epilepsy of children with centro-temporal (Rolandic) EEG foci is one of the most common types of epilepsy in children in the Swedish County of Västerbotten. As no other similar investigations of the incidence and prevalence rates of benign epilepsy of childhood exist it is not known whether these rates are a regional phenomenon or if they are generally valid. Published papers from various sources indicate, however, that this epilepsy is widespread and frequent among children.
The diagnosis "Benign epilepsy of children with centro-temporal EEG foci" can only be made if both the clinical convulsive manifestations and the typical interictal EEG changes (cf. petit mal with bilaterally synchronous, regular 3 Hz spike-and-wave activity) are simultaneously present. The seizures cannot form the sole basis of the diagnosis. It is characteristic but not conclusive for benign epilepsy of children.The partial seizures with reduced consciousness, inability to speak, guttural sounds, increased salivation etc, can easily be mistaken for other types of epilepsy especially psychomotor epilepsy, which has a more unfavourable prognosis than benign epilepsy of children. Therefore, a name has been proposed for this type of epilepsy which includes both seizures and EEG findings.
Rolandic discharges are defined as spikes or sharp waves recorded simultaneously over posterior frontal, central, middle temporal and sometimes parietal regions. Their maximal amplitudes should be in the centro-temporal and not in the anterior temporal region. They stand out clearly from normal background activity. They often appear in small clusters in which the individual potentials have almost identical amplitudes and form. They appear unilaterally, bilaterally or sideshifting(9,40). To be able to identify the Rolandic discharges with certainty the EEG recordings ought to be performed on a 16-channel electroencephalograph. Electrodes should be placed according to the 10-20 system

21
(28) with both longitudinal and transversal montages covering central and temporal regions simultaneously. EEG recordings during sleep are indicated when children suspected of having this seizure type have a normal EEG when awake. Brief induced sleep is usually adequate (10).
The clinical and electroencephalographical classification of epileptic seizures recommended by the International League Against Epilepsy (20) is based upon such factors as clinical seizure type, electroencephalo- graphic seizure type, electroencephalographic interictal expression, anatomical substrate, etiology and age. Since, when this investigation started, no other author had described personal observations of the epileptic seizures of benign epilepsy of children, or any EEG recordings during such a fit, my own classification was based principally on the typical interictal EEG changes. In 1975, however, Dalla Bernadina and Tassinari (17) were the first authors to publish a report of an epileptic seizure in benign epilepsy of children with simultaneous EEG recording. This and other observations together with my own investigations now make it possible to introduce this type of epilepsy into the classification. It can be placed in a special subgroup in Group C with the following characteristics:
Clinical seizure type: Partial seizures, secondarily generalized. Electroencephalographic seizure type: Unilateral or bilateral discharges focal in centro~temporal region, secondarily and rapidly generalized. Electroencephalographic interictal expression: Unilateral or bilateral, mostly asynchronous, sometimes sideshifting discharges in the centro- temporal region.Anatomical substrate: Unknown.Etiology: Autosomal, dominant gene with age-dependent penetrance.Age : Childhood.
The patho-physiological mechanism behind Rolandic discharges are unknown. The hypothesis is that, in spite of their focal trait, there is a dys

22
function of reticulo-thalamo-cortical mechanisms of the same tÿpe as in petit mal but limited to a sector of this system. It has been shown that an autosomal, dominant gene with age-dependent penetrance is involved in producing the EEG changes. It remains to be proved whether, besides this dysfunction, any kind of trigger-mechanism also exists. However it is obvious that, irrespective of what the trigger- mechanism may be, reductions of wakefulness increase the amount of epileptic activity and that seizures in most cases appear during sleep. Rolandic discharges can also be discovered for example in children with cerebral palsy but without seizures. Yet it is not known if hereditary mechanisms operate in this group, too.
No changes of the brain have been demonstrated at carotid arteriograms and pneumoencephalograms performed on children with benign epilepsy of childhood without neurological symptoms of cerebral lesion (4,9,32).At follow-up investigations of such children no new neurological symptoms have been noted and no tumors have been discovered or suspected. Therefore it has been concluded that neuroradiological examinations are unnecessary in these children unless there are other reasons for performing such investigations.
Genetic factors as a cause of benign epilepsy in children have been discussed by various authors (13,14,33). Bray and Wiser (13,14) claim that hereditary focal "temporal-lobe" epilepsy is transmitted by a simple, autosomal, dominant gene with age-dependent penetrance. The basis for their assumption is that when two types of focal "temporal- lobe” epilepsy exist in the same family it is the same disorder, mani- festating itself with different types of seizures and EEG foci dependent on age: The child has temporo-central spike-and-wave acitivty in combination with focal or generalized seizures (presumably corresponding to benign epilepsy of children), the adult anterior temporal EEG foci and psychomotor fits. Evidence to support this statement does not exist, in my opinion in the published material. It is impossible to decide whether Rolandic discharges exist in all the children in Bray and Wiser!s material, since the published EEG recordings in many cases lack montages involving central electrodes.

23
Loiseau and Beaussart (33) are of the opinion, that "familial epilepsy in childhood with interictal EEG evidence of Rolandic paroxysms should not be regarded as true focal epilepsy: it is because it occurs at a certain age that these seizures produce focal symptoms (focal paroxysms in the EEG occurs because the brain has reached a certain stage of matu- rition)". They base their opinion on observations that even other types of epileptic seizures can exist at different ages in the same family. Their conclusion is that hereditary partial epilepsy does not exist. This conclusion is right if one presumes that partial seizures are always caused by cortical lesions. Yet, in my opinion the term partial seizure should be used on clinical basis only, i.e. it should be based on focal features in the apperance of the seizure. Then benign epilepsy of children with centro-temporal EEG foci is a hereditary partial epilepsy. It has not yet been proved if other types of epilepsy, which can exist in the same family (13,14,33), bear any genetic relation to benign epilepsy of children but it seems unlikely. Here other factors, probably other genetic factors too, are crucial.
From a practical point of view it is important to emphasize the benign character of this type of epilepsy. The investigations of these children’s behavior and adjustment (26) have shown that early, careful and repeated information to the parents as well as to the patients can most probably prevent the appaearance of or reduce psychic symptoms. This investigation has also shown that the epileptic seizures did not influence the children’s intelligence. Moreover, medical treatment and regular, checks of the patients ought to be able to be discontinued in most cases at the age of about 20, frequently even earlier. The prospect of the young people obtaining a driver’s license should not be restricted and their choice of a profession should not be influenced by their seizure disorder.

24
6. Summary
Benign epilepsy of children with centro-temporal (Rolandic) EEG foci is characterized by the following:
1. It is one of the most frequent types of epilepsy in children.
2. It is transmitted by an autosomal, dominant gene with age-dependentpenetrance.
3. It is found just as frequently in boys as in girls.
4. In most cases it starts between 4 and 10 years of age.
5. There are 3 types of epileptic seizures: Partial and primarily and secondarily generalized convulsions. During the partial seizures motor, sensory and autonomous manifestations appear in the face, mouth and throat, usually without but often with varying degrees of disturbance of consciousness.
6. Most seizures appear on falling asleep, during sleep and on awakening.
7. The EEG findings consist of spikes or sharp waves and are recorded with their maximal amplitudes in the centro-temporal region with normal background acitivity. This trait is often designated Rolandic spikes.
8. The epileptic discharges increase in frequency during sleep and sometimes appear only during sleep.
9. The prognosis is good. Both seizures and EEG changes disappear as a rule before 20 years of age.
10. The seizures are in general easy to treat with antiepileptic drugs, for example diphenylhydantoin.

25
7 Acknowledgements.
In the scientific work, which led up to my thesis, I had great deal of help from many collaborators. The colleague I want to thank above all is my supervisor, Associate Professor Sigfrid Blom, the head of the Department of Clinical Neurophysiology, University Hospital, Umeå. He interested me in investigating children with epileptic seizures and Rolandic discharges. The main part of this research was also carried out in his department. A clever teacher he taught me the elements of clinical neurophysiology and guided me through the pitfalls of science with constructive criticism, stimulation and never-failing friendship. This dissertation would never have been written without his enthusiasm and valuable support.
Professor Michael Bohman, Department of Child Psychiatry, University Hospital, Umeå taught me the methods of investigation and gave me valuable advice and criticsm in the study of intelligence, behavior and school adjustment for which I thank him very much.
I am very grateful to Professor Jan Winberg, the previous head and Professor Karl-Henrik Gustavson, the present head of the Department of Pediatrics, University Hospital, Umeå for their valuable advice and support.
I would also like to express my gratitude to the following people:
Dr PG Bergfors, the head of the Department of Pediatrics, Skellefteå for his help in collecting the patients from the northern part of the County of Västerbotten.
Associate Professor Marianne Rasmuson, Department of Genetics, University of Umeå for her aid in the genetic study.
Professor Gösta Tibblin, Associate Professor Jan Ekstedt and Dr Jan Beskow for valuable advice.
Ann-Marie Frisendahl and Svante Âberg for performing the psychological tests.

26
Christina Agert for the well conducted interviews with teaòhers.
Margit Leonardsson, Anna-Greta Krüger and Rose-Marie Johansson for making all the EEG recordings with competence and great interest.
Karin Hellgren for her skilful typing of my manuscripts.
Yvonne Andersson for drawing the pictures.
Anders Nylén for statistical advice.
Pat Shrimpton for checking the English in my manuscripts,
all those colleagues who gave me their stimulating support
and all those children and parents who so willingly took part in the investigations.
The studies were supported by grants from the Margaretha Home Foundation and Karl Oskar Hansson*s Found.

27
8 References
1. Aicardi J and Chevrie JJ. Epilepsie partielle avec foyer Rolandiquede la seconde enfance. Journ Paris Péd 4_: 125-142, 1969.
2. Bancaud J, Colomb D and Dell MB. Les pointes rolandiques. Un syndrome EEG propre lfenfant. Rev Neurol 99: 206-209, 1958.
3. Beaumanoir A, Ballis T, Varfis G and Ansari K. Benign epilepsy ofchildhood with Rolandic spikes. A clinical, electroencephalographic and telencephalographic study. Epilepsia 15: 301-315, 1974.
4. Beaussart M. Benign epilepsy of children with Rolandic (centro-temporal) paroxysmal foci. A clinical entity. Study of 221 cases. Epilepsia 13: 795-811, 1972.
5. Beaussart M and Loiseau P. Hereditary factors in a random populationof 5200 epileptics. Epilepsia 10: 55-63, 1969.
6. Beaussart M, Beaussart-Boulenge L and Mahieu N. L*épilepsie avecparoxysmes EEG rolandiques. Une nouvelle forme d Tépilepsie à ne plus ignorer. Concours méd 10: 2195-2212, 1970.
7. Bender L. A visual motor gestalt test and its clinical use. Researchmonographs no 3. The American Orthopsychiatric Association, New York, 1938, 176 pp.
8. Blom S and Brorson LO. Central spikes or sharp waves (Rolandicspikes) in children*s EEG and their clinical significance. Acta Paediat Scand 55: 385-393, 1966.
9. Blom S,Heijbel J and Bergfors PG. Benign epilepsy of children withcentro-temporal EEG foci. Prevalence and follow-up study of 40 patients. Epilepsia 13: 609-619, 1972.
10. Blom S and Heijbel J. Benign epilepsy of children with centro- temporal EEG foci. Discharge rate during sleep. Epilepsia 16 : 133-140, 1975.

28
11. Bohman M. Adopted children and their families. Proprius, Stockholm, 1970, 239 pp.
12. von Bonin G. Architecture of the precentral motor cortex and someadjacent areas. In: PC Bucy (Ed) The precentral motor cortex.The University of Illinois Press, Urbana, Illinois, 1949, 615 pp.
13. Bray PF and Wiser WC. Evidence for a genetic etiology of temporal-central abnormalities in focal epilepsy. N Engl J M 271:926-933, 1964.
14. Bray PF and Wiser WC. Hereditary characteristics of familialtemporo-central focal epilepsy. Pediatrics 36: 207-211, 1965.
15. Brorson LO. Epilepsi hos barn och ungdom. En klinisk, psykometriskoch social undersökning inom Uppsala län. I: Epileptikervården. Socialstyrelsen redovisar nr 12, bilaga 1. Nordiska Bokhandeln, Stockholm, 1970, 84 pp. (in Swedish).
16. Courjon J and Cotte MR. Les décharges pseudo-rythmiques localiséeschez l1enfant et leur évolution à la puberté. Congrès pédiatrie langue française, Montpellier, Oct, 1959.
17. Dalla Bernardina B and Tassinari CA. EEG of a nocturnal seizurein a patient with "Benign epilepsy of childhood with Rolandic spikes". Epilepsia 16: 497-501, 1975.
18. Eeg-Olofsson 0, Petersén I and Selldén U. The development of theelectroencephalogram in normal children from the age of 1 through 15 years. Paroxysmal activity. Neuropädiatrie 4: 375-404, 1971.
19. Faure J and Loiseau P. Une corrélation clinique particulière despointes-ondes rolandiques sans signification focale. Rev Neurol 102: 399-406, 1960.
20. Gastaut H. Clinical and electroencephalographical classificationof epileptic seizures. Suppl Epilepsia 10: S2-S13, 1969.

29
21. Gastaut H and Tassinari CA (Eds). Epilepsies. In: A Remond (Ed),Handbook of electroencephalography and clinical neurophysiology, voi 13, part A. Elsevier Scientific Publishing Company, Amsterdam, 1975, 104 pp.
22. Gastaut Y. Un element déroutant de la sëmëiologie ëlectroencéphalo-graphique: les pointes prérolandiques sans signification focale. Rev Neurol 87: 488-490, 1952.
23. Gibbs EL and Gibbs FA. Good prognosis of mid-temporal epilepsy.Epilepsia 1: 448-453, 1959/60.
24. Heijbel J, Blom S and Bergfors PG. Benign epilepsy of childrenwith centro-temporal EEG foci. A study of incidence rate in outpatient care. Epilepsia in press.
25. Heijbel J, Blom S and Rasmuson M. Benign epilepsy of childhoodwith centro-temporal EEG foci. A genetic study. Epilepsia 16 : 285-293, 1975.
26. Heijbel J and Bohman M. Benign epilepsy of children with centro-temporal EEG foci. Intelligence, behaviour and school adjustment. Epilepsia in press.
27. Hellström A. Intelligensmätning enligt Terman-Merrill. Svensköversättning och bearbetning. Föreningen Sävstaholmsskolorna, Stockholm, 4th edition, 1960, 504 pp. (in Swedish).
28. Jasper HH. Report of the committee on methods of clinical examination in electroencephalography. Electroencephalogr Clin Neurophysiol 10: 370-375, 1958.
29. Lerman P. Benign focal epilepsy in children. ElectroencephalogrClin Neurophysiol 28: 642, 1970.
30. Lerman P and Kivity S. Benign focal epilepsy in children associated with "centro-temporal spikes": a follow-up study of 100 cured patients. Electroencephalogr Clin Neurophysiol 34: 696, 1973.

30
31. Lerman P and Kivity-Ephraim S. Carbamazepine sole anticonvulsantfor focal epilepsy of childhood. Epilepsia 15: 229-234, 1974.
32. Lerman P and Kivity S. Benign focal epilepsy of childhood. Afollow-up study of 100 recovered patients. Arch Neurol 32:261-264, 1975.
33. Loiseau P and Beaussart M. Hereditary factors in partial epilepsy.Epilepsia 10: 23-31, 1969.
34. Loiseau P and Beaussart M. The seizures of benign childhood epilepsy with Rolandic paroxysmal discharges. Epilepsia 14:381-389, 1973.
35. Loiseau P and Faure J. Une forme particulière d fépilepsie de laseconde enfance. Journal de Médecine de Bordeaux 138: 381-389,1961.
36. Loiseau P, Cohadon F and Faure J. A propos des pointes rolandiquessans signification focale. Rev Neurol 105: 199-203, 1961.
37. Loiseau P, Cohadon F and Mortureux Y. A propos d !une forme singulièred ’epilepsie de l’enfant. Rev Neurol 116: 244-248, 1967.
38. Loiseau P, Geissmann P, Cohadon S, Vincent D and Faure J. Lesparoxysmes rolandiques en dehors de 1’épilepsie. Rev Neurol 111: 374-381, 1964.
39. Loiseau P, Guerin A and Cohadon S. Infantile sleep epilepsy. Theproblem of Rolandic spikes. Electroencephalogr Clin Neurophysiol 15: 710, 1963.
40. Lombrose CT. Sylvian seizures and mid-temporal spike foci inchildren. Arch Neurol 17: 52-59, 1967.
41. Loomis AL, Harvey EN and Hobart GA. Cerebral states during sleep, as studied by human brain potentials. J Exp Physiol 21: 127-144, 1937.

31
42. MacFarlane JW, Allen L and Honzik MP. A development study of thebehaviour problems of normal children between twenty-one months and fourteen years. University of California Press, 1954, 221 pp.
43. Mortureux Y. Etude électro-clinique de certains paroxysmesd 1expression rolandique chez l'enfant. Thèse de médecine, Bordeaux, 1966, 191 pp.
44. Mundier F. L fépilepsie à paroxysmes rolandiques. Médecine et hygiène31: 880-883, 1973.
45. Nayrac P and Beaussart M. Les pointes-ondes prérolandiques: expression EEG très particulière. Etude électro-clinique de 21 cas.Rev Neurol 99: 201-206, 1958.
46. Pascal GR and Suttell BJ. The Bender Gestalt Test. Quantificationand validity for adults. Grune and Stratton, New York, 1951, 274 pp.
47. Ross JJ, Johnson LC and Walter RD. Spike and wave discharges duringstages of sleep. Àrch Neurol 14: 399-407, 1966.
48. Smith JMB and Kellaway P. Central (Rolandic) foci in children: ananalysis of 200 cases. Electroencephalogr Clin Neurophysiol 17: 451-452, 1964.
49. Snedecor GW and Cochran WG. Statistical methods. The Iowa stateUniversity Press, Ames, Iowa, U.S.A.,1967, 593 pp.
50. Sorel L and Rucquoy-Ponsar M. L*épilepsie fonctionelle de maturi-tion. Apport des montages verticaux en EEG dans le diagnostic de cette forme d'épilepsie. Rev Neurol 121: 288-297, 1969.
51. Stern C. Principles of Human Genetics. Freeman, San Francisco, 1960,753 pp.
52. Terman LM and Merrill MA. Meassuring intelligence. Riverside Press,Cambridge, Massachusetts, 1937, 461 pp.
53. Trojaborg W. Focal spike discharges in children, a longitudinalstudy. Acta Paediat Scand Suppl. 168, 1966, 113 pp.

Centraltryckeriet, Umeå 1976, Offset