Beneficial Pre-ECT Ketamine Infusion in a Patient with Treatment-Resistant Depression
4
Case Reports Beneficial Pre-ECT Ketamine Infusion in a Patient with Treatment-Resistant Depression Ryan Sultan, M.D., Patricio Riva-Posse, M.D., Steven J. Garlow, M.D., Ph.D., Ann C. Schwartz, M.D. W e present a case of a 52-year-old white man with treatment-resistant depression, who received a single ketamine infusion before electro- convulsive therapy (ECT) and demonstrated marked and rapid improvement in his depressive symptoms. Case Report Mr. S, a 52-year-old white man, presented to a large academic center for inpatient psychiatric admission because of intolerable insomnia and anxiety. In the 2 weeks before hospital admission, his family had noted progressive slowing of his speech and motor activity, to the point of remaining motionless for prolonged periods. He was sleeping very little and had endorsed a plan to overdose on his medications. Mr. S was accompanied by his wife and daughter, who reported that he had not been at his baseline functioning for approximately 4 years. The index presentation was 6 months after a hospitalization in our Medical Psychiatry Unit when he presented with depressed mood, anhedonia, poor appetite with weight loss, and suicidal ideation. During this first admission, Mr. S received 12 ECT treatments, after which he and his wife reported subjective improve- ment in his symptoms. He was discharged home after a 1-month stay, and his medication regimen was 20 mg of escitalopram daily, 30 mg of mirtazapine nightly, 20 mg of olanzapine nightly, and 0.5 mg of clonaze- pam nightly as needed for insomnia. Following dis- charge, Mr. S continued his treatment with his outpatient psychiatrist. As per his wife, Mr. S had a sustained antidepressant effect from the ECT for approximately 1 month; however, his previous depres- sive symptoms returned after that period. Regarding his past psychiatric condition, Mr. S had a long history of depression dating back over 25 years. The current episode started 4 years ago, when he began experiencing depressive symptoms including low mood, psychomotor retardation, and anhedonia with no known precipitating event. A review of his records indicated that over the past 4 years, Mr. S had inadequate responses to therapeutic doses of multiple medications. Mr. S had no prior suicide attempts and had never had symptoms of mania. He did not use illegal substances or alcohol. Mr. S and his family reported no medical conditions other than hyperlipidemia treated with atorvastatin. Family history was significant for depression in his father and a completed suicide by shooting in his paternal grandfather. Because of the severity of his depressive symptoms and suicidal ideation, Mr. S was admitted to the inpatient unit with the plan of pursuing ECT as a treatment modality. On admission, a medical workup was completed. A baseline chemistry panel and complete blood count were essentially within normal limits. His total cholesterol level was 139 mg/dL, levels of triglycerides were 47 mg/dL, high-density lipopro- tein level was 47 mg/dL, and low-density lipoprotein Received November 1, 2013; revised November 27, 2013; accepted November 29, 2013. From Department of Psychiatry and Behavioral Sciences, Emory University School of Medicine, Atlanta, Georgia. Send correspondence and reprint requests to Ann Schwartz, 80 Jesse Hill Jr Dr, P.O. Box 26238, Atlanta, Georgia 30303; e-mail: aschwa2@ emory.edu & 2013 The Academy of Psychosomatic Medicine. Published by Elsevier Inc. All rights reserved. Psychosomatics 2013:]:]]]–]]] & 2013 The Academy of Psychosomatic Medicine. Published by Elsevier Inc. All rights reserved. Psychosomatics ]:], ] 2013 www.psychosomaticsjournal.org 1
Transcript of Beneficial Pre-ECT Ketamine Infusion in a Patient with Treatment-Resistant Depression

Psychosomatics 2013:]:]]]–]]] & 2013 The Academy of Psychosomatic Medicine. Published by Elsevier Inc. All rights reserved.
Case Reports
Beneficial Pre-ECT Ketamine Infusion in a Patient withTreatment-Resistant Depression
Ryan Sultan, M.D., Patricio Riva-Posse, M.D., Steven J. Garlow, M.D., Ph.D.,Ann C. Schwartz, M.D.
We present a case of a 52-year-old white manwith treatment-resistant depression, who
received a single ketamine infusion before electro-convulsive therapy (ECT) and demonstrated markedand rapid improvement in his depressive symptoms.
Received November 1, 2013; revised November 27, 2013; acceptedNovember 29, 2013. From Department of Psychiatry and BehavioralSciences, Emory University School of Medicine, Atlanta, Georgia.Send correspondence and reprint requests to Ann Schwartz, 80 Jesse HillJr Dr, P.O. Box 26238, Atlanta, Georgia 30303; e-mail: [email protected]
& 2013TheAcademy of PsychosomaticMedicine. Published byElsevier Inc. All rights reserved.
Case Report
Mr. S, a 52-year-old white man, presented to a largeacademic center for inpatient psychiatric admissionbecause of intolerable insomnia and anxiety. In the 2weeks before hospital admission, his family had notedprogressive slowing of his speech and motor activity,to the point of remaining motionless for prolongedperiods. He was sleeping very little and had endorsed aplan to overdose on his medications.
Mr. S was accompanied by his wife and daughter,who reported that he had not been at his baselinefunctioning for approximately 4 years. The indexpresentation was 6 months after a hospitalization inour Medical Psychiatry Unit when he presented withdepressed mood, anhedonia, poor appetite withweight loss, and suicidal ideation. During this firstadmission, Mr. S received 12 ECT treatments, afterwhich he and his wife reported subjective improve-ment in his symptoms.Hewas discharged home after a1-month stay, and his medication regimen was 20 mgof escitalopram daily, 30 mg of mirtazapine nightly,20 mg of olanzapine nightly, and 0.5 mg of clonaze-pam nightly as needed for insomnia. Following dis-charge, Mr. S continued his treatment with hisoutpatient psychiatrist. As per his wife, Mr. S had asustained antidepressant effect from the ECT for
Psychosomatics ]:], ] 2013
approximately 1 month; however, his previous depres-sive symptoms returned after that period.
Regarding his past psychiatric condition,Mr. S hada long history of depression dating back over 25 years.The current episode started 4 years ago, when he beganexperiencing depressive symptoms including low mood,psychomotor retardation, and anhedonia with noknown precipitating event. A review of his recordsindicated that over the past 4 years, Mr. S hadinadequate responses to therapeutic doses of multiplemedications. Mr. S had no prior suicide attempts andhad never had symptoms ofmania.He did not use illegalsubstances or alcohol. Mr. S and his family reported nomedical conditions other than hyperlipidemia treatedwith atorvastatin. Family history was significant fordepression in his father and a completed suicide byshooting in his paternal grandfather.
Because of the severity of his depressive symptomsand suicidal ideation, Mr. S was admitted to theinpatient unit with the plan of pursuing ECT as atreatment modality. On admission, a medical workupwas completed. A baseline chemistry panel andcomplete blood count were essentially within normallimits. His total cholesterol level was 139 mg/dL, levelsof triglycerides were 47 mg/dL, high-density lipopro-tein level was 47 mg/dL, and low-density lipoprotein
www.psychosomaticsjournal.org 1
Case Reports
level was 83 mg/dL. His urine drug screen testedpositive for benzodiazepines, and his electrocardio-gram findings were normal. A computed tomographyscan of the head was unremarkable.
The inpatient team offered ECT; however, Mr. Swas reluctant to pursue the treatment given his limitedduration of response 6 months before. He was thenoffered a trial of a ketamine infusion based on positivereports in the literature for the treatment of severedepression. He agreed to the ketamine infusion as aninterim measure to provide immediate relief of theintense depressive symptomswith the plan to reconsiderECT after the infusion. The clonazepam was decreasedwith the plan to discontinue the medication, admin-istration of trazodone nightly was begun for insomnia.
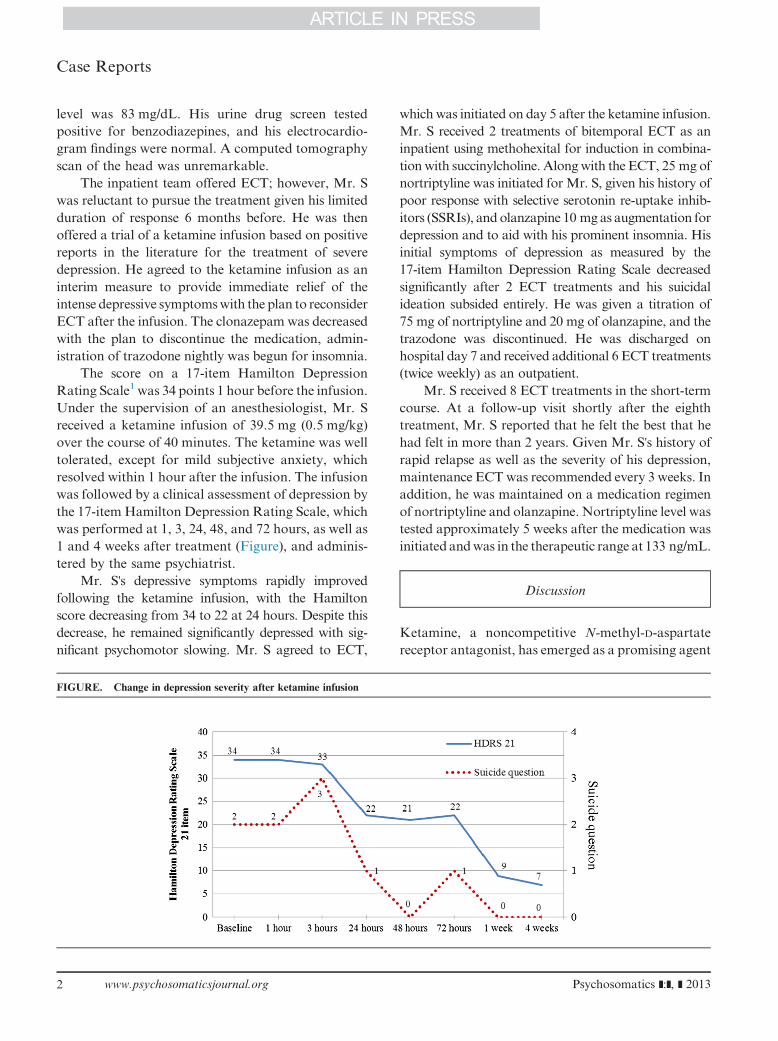
The score on a 17-item Hamilton DepressionRating Scale1 was 34 points 1 hour before the infusion.Under the supervision of an anesthesiologist, Mr. Sreceived a ketamine infusion of 39.5 mg (0.5 mg/kg)over the course of 40 minutes. The ketamine was welltolerated, except for mild subjective anxiety, whichresolved within 1 hour after the infusion. The infusionwas followed by a clinical assessment of depression bythe 17-item Hamilton Depression Rating Scale, whichwas performed at 1, 3, 24, 48, and 72 hours, as well as1 and 4 weeks after treatment (Figure), and adminis-tered by the same psychiatrist.
Mr. S's depressive symptoms rapidly improvedfollowing the ketamine infusion, with the Hamiltonscore decreasing from 34 to 22 at 24 hours. Despite thisdecrease, he remained significantly depressed with sig-nificant psychomotor slowing. Mr. S agreed to ECT,
FIGURE. Change in depression severity after ketamine infusion
2 www.psychosomaticsjournal.org
which was initiated on day 5 after the ketamine infusion.Mr. S received 2 treatments of bitemporal ECT as aninpatient using methohexital for induction in combina-tion with succinylcholine. Alongwith the ECT, 25 mg ofnortriptyline was initiated for Mr. S, given his history ofpoor response with selective serotonin re-uptake inhib-itors (SSRIs), and olanzapine 10 mgas augmentation fordepression and to aid with his prominent insomnia. Hisinitial symptoms of depression as measured by the17-item Hamilton Depression Rating Scale decreasedsignificantly after 2 ECT treatments and his suicidalideation subsided entirely. He was given a titration of75 mg of nortriptyline and 20 mg of olanzapine, and thetrazodone was discontinued. He was discharged onhospital day 7 and received additional 6 ECT treatments(twice weekly) as an outpatient.
Mr. S received 8 ECT treatments in the short-termcourse. At a follow-up visit shortly after the eighthtreatment, Mr. S reported that he felt the best that hehad felt in more than 2 years. Given Mr. S's history ofrapid relapse as well as the severity of his depression,maintenance ECT was recommended every 3 weeks. Inaddition, he was maintained on a medication regimenof nortriptyline and olanzapine. Nortriptyline level wastested approximately 5 weeks after the medication wasinitiated andwas in the therapeutic range at 133 ng/mL.
Discussion
Ketamine, a noncompetitive N-methyl-D-aspartatereceptor antagonist, has emerged as a promising agent
Psychosomatics ]:], ] 2013

Sultan et al.
in the treatment of patients with depression.2,3 Ket-amine and related drugs target glutamate, the majorexcitatory neurotransmitter in the brain and one that iscurrently not directly affected by available antidepres-sants. Its action as primarily an antagonist of theN-methyl-D-aspartate receptor has presented an excit-ing new avenue for the treatment of depression asmostcontemporary antidepressants target the monoamineoxidase system. This potential new mechanism, whichis capable of mediating antidepressant action, is one ofthe most exciting developments in psychopharmacol-ogy in the last half of the century.4
There is emerging clinical data in support ofketamine's use as an antidepressant.3,5–7 Ketaminewas first reported to have therapeutic effects in apreliminary study of 8 patients with major depressivedisorder in 2000.8 Using a larger sample size (18patients) in a randomized controlled trail, Zarateet al.5 confirmed the findings from the preliminarystudy by Berman et al. and showed a robust and rapidantidepressant effect from a single intravenous dose ofketamine. In this randomized controlled trail, IVketamine had rapid, but transient, antidepressanteffects in individuals with treatment-resistant majordepressive disorder, including some patients who hadnot responded to ECT.5 Investigators sought toreplicate ketamine's antidepressant efficacy in bipolardepression and found that patients receiving a singleketamine infusion experienced a rapid and robustantidepressant response.6,7
Recently, Murrough et al.9 evaluated the rapidantidepressant efficacy of ketamine in a large group ofpatients with treatment-resistant major depression. Inthis 2-site, parallel-arm, randomized controlled trial, asingle infusion of ketamine was compared with anactive placebo-control condition with midazolam(n ¼ 73). The ketamine group had greater improve-ment in the Montgomery-Åsberg Depression RatingScale score than the midazolam group 24 hours aftertreatment, further supporting N-methyl-D-aspartatereceptor modulation as a novel mechanism for accel-erated improvement in severe and chronic forms ofdepression.
Ketamine's rapid onset in the improvement ofdepressive symptoms is in stark contrast to the severalweek duration needed for existing antidepressantmedications. However, ketamine lacks the mainte-nance and sustained effects of conventional treat-ments. ECT is a well-established, Food and Drug
Psychosomatics ]:], ] 2013
Administration–approved, and highly effective treat-ment for severe and treatment-resistant depression.10,11
ECT is the most rapid of the accepted treatmentsfor depression, yet there remains a delay in theantidepressant effect. Ketamine has been used as themain anesthetic agent in ECT, usually when it is notpossible to adequately induce seizures with barbitu-rates, given their inherent anticonvulsant properties.12
Two case studies report dramatic mood improvementsafter the use of ketamine anesthesia in ECT, suggest-ing synergistic antidepressant effects.13,14 Ostroffet al.15 reported a case of rapid response in depressivesymptoms in a patient receiving ketamine anesthesiafor ECT but not achieving an adequate seizure duringECT. Goforth et al.16 described a case with animmediate response to a treatment of bilateral ECTcombined with ketamine anesthesia in a patient withsevere major depressive disorder with psychotic fea-tures. Findings from an open-label trial suggestedthat ketamine anesthesia has an early antidepressanteffect during ECT that was superior to propofolanesthesia. This effect may come from the antidepres-sant effect of ketamine. A limitation of ketamine isthat its use at full anesthetic doses may lead to dose-related adverse psychotogenic effects such as halluci-nations. As these effects of ketamine are dose-related,subanesthetic doses of ketamine used in combinationwith alternate anesthetic agents may be an alternativeeffective augmentation strategy for patients withsevere depression.12
Although there is evidence supporting antidepres-sant effects of ketamine in its use as an anesthetic forECT, there are few data on the use of subanestheticdoses of ketamine as an augmentation strategy withECT to speed the response rate. Our case illustrates thenovel use of pretreatment of ketamine as an augmen-tation strategywithECT for treatment-resistant depres-sion in an individual with severe depressive andcatatonic symptoms. A potential confounding variableis that multiple treatment interventions were initiatedsimultaneously, including the addition of a tricyclicantidepressant (TCA) in combination with olanzapineand ECT. Therefore, it is possible that the observedresponse was not entirely attributable to ketamine.However, given the severity of the treatment resistanceand the chronicity ofMr. S's depression, ketamine likelyplayed a significant role in his treatment response.
The use a subanesthetic dose of ketamine as anadjunct before the electroconvulsive treatment, while
www.psychosomaticsjournal.org 3

Case Reports
still using barbiturate anesthesia, could be a promisingstrategy in patients with treatment-resistant depres-sion. Its use as a facilitating agent while transitioningto a more permanent treatment strategy, such as ECTor pharmacologic treatments, provides practitionersof psychosomatic medicine another relatively low-risk
4 www.psychosomaticsjournal.org
strategy to consider in the management of complextreatment-resistant cases.
Disclosure: The authors disclosed no proprietary orcommercial interest in any product mentioned or con-cept discussed in this article.
References
1. Hamilton M: A rating scale for depression. J NeurolNeurosurg Psychiatry 1960; 23:56–62
2. Messer M, Haller IV, Larson P, Pattison-Crisostomo J,Gessert CE: The use of a series of ketamine infusions in twopatients with treatment-resistant depression. J Neuropsy-chiatry Clin Neurosci 2010; 22(4):442–444
3. Aan Het Rot M, Zarate CA Jr, Charney DS, Mathew SJ:Ketamine for depression: where do we go from here? BiolPsychiatry 2012; 72(7):537–547
4. Preskorn SH: Ketamine: the hopes and the hurdles. BiolPsychiatry 2012; 72(7):522–523
5. Zarate CA Jr, Singh JB, Carlson PJ, et al: A randomized trialof an N-methyl-D-aspartate antagonist in treatment-resistantmajor depression. Arch Gen Psychiatry 2006; 63(8):856–864
6. Diazgranados N, Ibrahim L, Brutsche NE, et al: Arandomized add-on trial of anN-methyl-D-aspartate antag-onist in treatment-resistant bipolar depression. Arch GenPsychiatry 2010; 67(8):793–802
7. Zarate CA Jr, BrutscheNE, IbrahimL, et al: Replication ofketamine's antidepressant efficacy in bipolar depression: arandomized controlled add-on trial. Biol Psychiatry 2012;71(11):939–946
8. Berman RM, Cappiello A, Anand A, et al: Antidepressanteffects of ketamine in depressed patients. Biol Psychiatry2000; 47(4):351–354
9. Murrough JW, Iosifescu DV, Chang LC, et al: Antide-pressant efficacy of ketamine in treatment-resistant major
depression: a two-site randomized controlled trial. Am JPsychiatry 2013; 170(10):1134–1142
10. Pagnin D, de Queiroz V, Pini S, Cassano GB: Efficacy ofECT in depression: a meta-analytic review. J ECT 2004;20(1):13–20
11. Swartz C: Electroconvulsive and Neuromodulation Thera-pies. 1st ed. New York, NY: Cambridge University Press;2009; P. 648
12. Loo C, Simpson B, MacPherson R: Augmentation strat-egies in electroconvulsive therapy. J ECT 2010; 26(3):202–207
13. Goforth HW, Holsinger T: Rapid relief of severe majordepressive disorder by use of preoperative ketamine andelectroconvulsive therapy. J ECT 2007; 23(1):23–25
14. McDaniel WW, Sahota AK, Vyas BV, Laguerta N,Hategan L, Oswald J: Ketamine appears associated withbetter word recall than etomidate after a course of 6 electro-convulsive therapies. J ECT 2006; 22(2):103–106
15. Ostroff R, Gonzales M, Sanacora G: Antidepressant effectof ketamine during ECT. Am J Psychiatry 2005; 162(7):1385–1386
16. Okamoto N, Nakai T, Sakamoto K, Nagafusa Y, HiguchiT, Nishikawa T: Rapid antidepressant effect of ketamineanesthesia during electroconvulsive therapy of treatment-resistant depression: comparing ketamine and propofolanesthesia. J ECT 2010; 26(3):223–227
Psychosomatics ]:], ] 2013