Being a good medical intern
23
1 STEP GUIDE TO BEING A SUPERSTAR By Nick Gowen
-
Upload
nick-gowen -
Category
Health & Medicine
-
view
539 -
download
1
Transcript of Being a good medical intern

1 STEP GUIDE TO BEING A SUPERSTARBy Nick Gowen

Call and Response• Who is this man’s doctor?
•I am the doctor!

• You are on call. You are called about Ms. R, a 98 yo WW w HTN, DM2, CHF w EF 15%, ESRD on M/W/F HD, severe COPD, and stage 5 breast cancer admitted to F6 w pneumonia.
• The nurse is calling to tell you “she doesn’t look too good, she’s not breathing right”
• Terrified, you glance at your list and notice her code status says “full.”

What now?

Ms. R• You arrive to the room to find Ms. R lying still, not
appearing super “alive.” Some interns would run away crying, but you are a rock star, so you immediately yell out her name and rub her arm, but no answer. You put two fingers on her carotid and feel no pulse for 5 seconds.
• Now what?

Cry a lot? NO! Be the super star

Ms. R• You yell (LOUDLY) for help and press the code button,
and start chest compressions.• What’s the rate again? How deep?
• The rest of the code team arrives 4 minutes later, after you’ve been performing dual provider CPR with the nurse and are exhausted. You are relieved and pushed out of the room, CPR in progress.• Now What? Go cry? watch through the window? go buy a cookie?

Be even better than that• Because you are an incredible intern, you know that there
is more to be done here. You get into the electronic medical record and the physical chart of Ms. R, looking for a phone number of a next-of-kin to notify them (or to give the number to a UL to notify them). You find a durable DNAR/DNI. You give this to the nurse recorder, who gives it to the team leader. The team leader discusses with the team and ensures that this has not been recently reversed, and the code is stopped.

Case # 2: Mr. S• You’re still on call, a little teary from filling out Ms. R’s
death packet. Pager goes off again.• F 6 nurse: Mr. S (52 yo WM w cirrhosis admited today w
community acquired pneumonia) is really anxious. Can I get some ativan for her?
• What next?• You get some vitals: 100.9, 126, 34, 94/50, 98% on 2LNC• Do you have any questions for the nurse? What do you
do now?• You give some ativan, code pager goes off a few minutes
later

Case # 2: Mr. S• You’re still on call, a little teary from filling out Ms. R’s
death packet. Pager goes off again.• F 6 nurse: Mr. S (52 yo WM w cirrhosis admited today w
community acquired pneumonia) is really anxious. Can I get some ativan for him?
• What next?• You get some vitals: 100.9, 126, 34, 94/50, 98% on 2LNC• Do you have any questions for the nurse? What do you
do now?• You give some ativan, code pager goes off a few minutes
later • You are awesome, so you go EVALUATE the patient

Mr. S: What you see• You get some vitals: 100.9, 126, 34, 94/50, 98% on 2LNC

Mr. S• When you arrive Mr. S reports feeling “very anxious” and
requests some medicine so she can sleep.• You notice that he is tachypneic and wearing a 40% VM
(the notes said NC, the nurse didn’t mention to you the oxygen).
• What’s going on? Should you examine him further? What should you do?

Sepsis• Sepsis definition?
• SIRS + suspected infection• Fever/hypthermia, HR > 90, SBP < 90, MAP < 70, RR > 20, AMS,• Glucose >140 (in nondiabetics), WBC >12,000 or <4,000 or >10%
bands, Platelets < 100,000, high CRP, elevated lactate, INR >1.5, Creatinine increase by 0.5 or more.

Pager Backlog• Now you are feeling a little overwhelmed but also
confident and powerful after correctly diagnosing and managing Mr. S. As you walk out of his room, the pager goes off again. Now that you look at it, there have been 6 pages while you are on that room.
• Page #1: pain already has oxycodone, you do nothing• Page #2 : nausea already getting zofran, but is 4mg IV
q8h. That sounds low to you, so you check uptodate and notice that 8mg is the standard dose and you increase to 8mg IV q8h

Purging the backlog• Page #350 yo on ambien at home wants home ambien
to sleep. You check w the nurse to make sure his mental status has been perfect, ask yourself if there is any reason ambien might hurt him, and then prescribe his home ambien dose of 10mg qhs.
• Page #4 84 yo WW wants something for sleep. You take a moment to look at the notes and notice that her mental status has waxed and waned somewhat the last few days. You give her acetaminophen 650mg PO now and NO BENZOS or BENADRYL

Purging the backlog• Page #5an f4 pt’s family just arrived (at 9pm) and want
to see a doctor NOW to discuss the plan. You instruct the nurse to explain that the day team rounds from 6am-11am, and that if someone is here at those times she will be able to talk with a doctor. Further, you tell her that you will try to come by to talk to the family about what little you know, but it will be 1-4 hours.
• Page #6 F6 nurse to tell you that Mr. U is having chest pain. You remember that chest pain is sometimes bad, so you order a stat ECG and head straight over to his room to check it out.

Mr. U• Mr. U is a 36 yo WM w no PMH who presented 3 days
ago with community acquired pneumonia. He had been improving and was scheduled for DC in AM. Five minutes ago he began having sharp pain in left chest along with shortness of breath.
• Vitals: 97.8, 110, 28, 130/75, 90% on RA• You examine him. He is sweating, but his lungs are clear,
heart w sinus tach but no other findings, no edema, no tenderness, abd normal.
• Differential Dx of the new chest pain?

Mr. U: differential diagnosis• Myocardial infarction• Pulmonary embolus• Worsening pneumonia w empyema

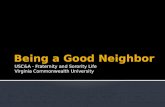
The ECG



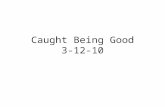
The radiograph

Mr. U• The troponin comes back <0.02, the ECG shows only
sinus tach, and the CXR is unrevealing. SLNG has no effect, but morphine helps a little. He remains dyspneic w pain on inspiration, however, so you become suspicious of something else.
• What could this be?• How can you prove it?• What do you need to know about a pt before ordering a
spiral CT scan PE protocol?• How do you treat it?• Should you do any other tests? US of the legs?