
Behavioral Medicine in Asthma GEOFFREY GATES, MD, FACP PEACE CORPS SEED GLOBAL HEALTH.
60
Behavioral Medicine in Asthma GEOFFREY GATES, MD, FACP PEACE CORPS SEED GLOBAL HEALTH
-
Upload
adelia-cross -
Category
Documents
-
view
213 -
download
0
Transcript of Behavioral Medicine in Asthma GEOFFREY GATES, MD, FACP PEACE CORPS SEED GLOBAL HEALTH.
Behavioral Medicine in AsthmaGEOFFREY GATES, MD, FACP
PEACE CORPS SEED GLOBAL HEALTH
Asthma Recurrent episodes of airway obstruction with symptoms of cough, wheezing and shortness of breathe. Lung function often returns to normal between episodes. Pathophysiology is a combination of exaggerated bronchoconstrictor responses to stimuli that have little or no effect in nonasthmatic subjects and inflammation of the airways with thickening of airway epithelium and excessive mucus production.
All of the following are causes of shortness of breathe in asthma except:
A. constriction of airway smooth muscle
B. thickening of airway epithelium
C. Irreversible destruction of alveoli
D. mucus blocking the airway
A. B. C. D.
33%
21%
42%
4%
All of the following are causes of shortness of breathe in asthma except: A. constriction of airway
smooth muscleB. thickening of airway
epitheliumC. Irreversible destruction of
alveoliD. mucus blocking the airway
“C” is false. Asthma is a disease of the airways (bronchi and bronchioles) caused by a combination of bronchoconstriction and inflammation, both of which processes are reversible. Asthma does not directly affect the alveoli.
Your football team is about to score. Does your heart rate increase before you jump up and cheer?
A. YesB. No
Yes No
17%
83%
Your football team is about to score. Does your heart rate increase before you jump up and cheer?
A. YesB. No
Yes is the correct. Anyone who has ever been excited about anything can answer this question from personal experience. Intense emotion can stimulate the heart to beat harder and faster without any work (like running or climbing stairs) that actually require an increase in cardiac output.
Emotions can affect airway smooth muscle.A. TrueB. False
True
False
3%
97%
Emotions can affect airway smooth muscle.A. TrueB. False
True is the correct answer based on the study that will be presented in the next few slides, but the answer is not obvious and not even accepted by all the specialists in this field. The effects of emotions on bronchoconstriction and inflammation in asthma are difficult to measure. Most studies are small. Small differences in measurements of pulmonary function that are statistically significant may not be important clinically.
Pathophysiology and treatment of Asthma
The pathophysiology of asthma is a combination of exaggerated bronchoconstrictor responses and inflammation of the airways.
Medications that treat asthma fall into 2 classes to treat the 2 main factors contributing to airway obstruction: bronchodilators (salbutamol) and anti-inflammatory (glucocorticoids)
Behavioral medicine is not yet a widely accepted treatment for asthma. Before behavioral medicine is accepted in clinical practice, it has to answer the 2 questions on the following slide.
Two questions for behavioral medicine What is the evidence that emotional factors contribute to bronchospasm and/or inflammation?
What is the evidence that behavioral interventions can relieve or prevent either bronchospasm and/or inflammation in asthma?
Airway response to emotional stimuli in asthma: the role of the cholinergic pathwayRITZ, T et al
J Appl Physiol 108:1542-1549, 2010
Recruitment and Experimental Design Patients with asthma (n = 54) and healthy participants (n = 25) received either ipratropium bromide inhaler (2 actuations of 20µg each) or a placebo inhaler in a double-blind cross-over design in two laboratory sessions with experimental emotion induction.
Stimuli were films and pictures of pleasant, unpleasant, and neutral quality.
Can films and pictures predictably stimulate emotion?
A. YesB. No
Yes No
3%
97%

Can films and pictures predictably stimulate emotion?A. YesB. No
There is not a ‘correct’ answer to this question. Some people cry watching a movie. Other people at the same movie may criticize the quality of the acting. A documentary on open heart surgery will have a different effect on a cardiovascular surgeon than on the relative of someone who has just experienced a heart attack.
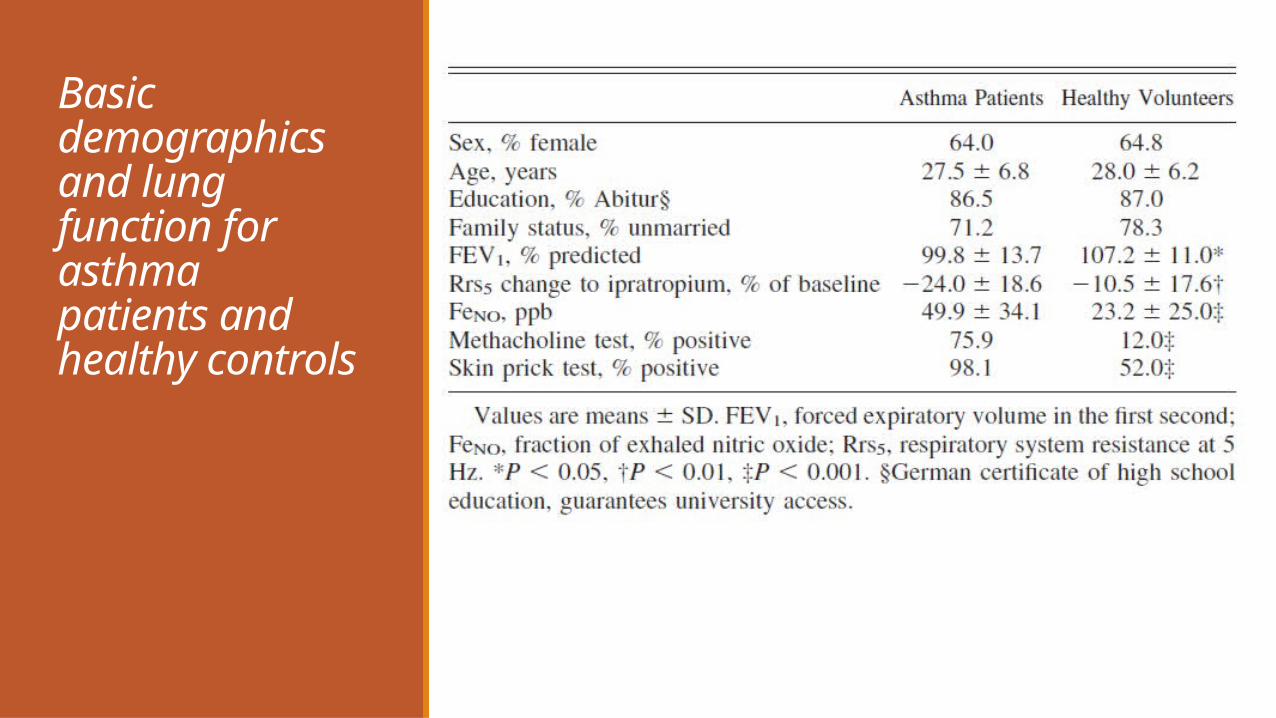
Basic demographics and lung function for asthmapatients and healthy controls
What is the main goal of randomization?
A. To recruit enough subjects to get a statistically significant result for publication.
B. To eliminate bias (assigning subjects who are expected to do better to the treatment group)
C. To give everyone the same chance of getting the new treatment (which is expected to be better)
A. B. C.
21%28%
52%
What is the main goal of randomization?
A. To recruit enough subjects to get a statistically significant result for publication.
B. To eliminate bias (assigning subjects who are expected to do better to the treatment group)
C. To give everyone the same chance of getting the new treatment (which is expected to be better)
If the healthiest subjects or the subjects most likely to respond to treatment are placed in the treatment group of a study (even if it is not intentional), then the study may conclude that the new treatment is effective when it is not.
A biased study is more likely to yield statistically significant results since the groups are unequal before the study starts. That is the reason to eliminate bias.
Many promising new treatments prove to be either ineffective or even harmful. Randomization is not an attempt to give everyone an equal chance at the best treatment.

Are the subjects in this study adequately randomized?A. YesB. NoC. This question is
unclear. (I hope its not on the test!)
A. B. C.
40%36%
24%
Are the subjects in this study adequately randomized?
A. YesB. NoC. This question
is unclear. (I hope its not on the test!)
‘C’ is the correct answer. The authors of the study are comparing subjects with asthma to subjects without asthma, so obviously the subjects without asthma have better lung function on baseline testing. The 2 groups are comparable in % female, age, education and % married. The double blind, crossover design of testing attempts to eliminate a number of factors that could ‘bias’ the question of whether stress induced bronchoconstriction is mediated by cholinergic pathways.
Measurements of Airway Response Respiratory resistance and reactance at 5 and 20 Hz were measured continuously before and during presentations, together with respiration by impedance plethysmography and end-tidal PCO2 by capnometry.
In addition, measures of airway inflammation (fraction of exhaled nitric oxide), airway hyperreactivity (methacholine challenge), and reversibility of obstruction were obtained.
Results Respiratory resistance at 5 and 20 Hz increased during unpleasant stimuli in asthma patients. This response was partially blocked by ipratropium bromide.
Changes in resistance during unpleasant films in asthma patients given placebo were positively correlated with patients’ reports of psychological asthma triggers.
There were also changes in airway resistance in healthy subjects viewing unpleasant images, although the changes were less than in asthmatics and not significantly affected by ipratropium.
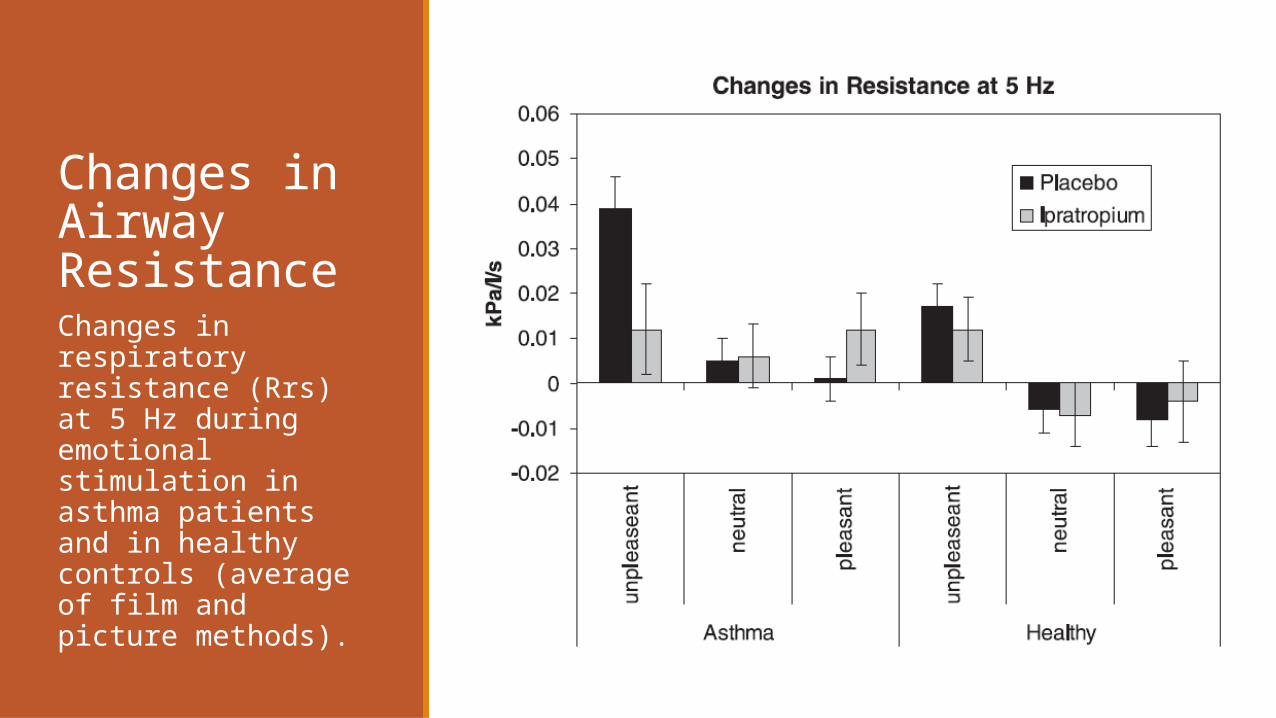
Changes in Airway ResistanceChanges in respiratory resistance (Rrs) at 5 Hz during emotional stimulation in asthma patients and in healthy controls (average of film and picture methods).
Conclusions Asthma patients (but not healthy controls) showed significant airway constriction to unpleasant stimuli that reached clinically relevant levels requiring medication in almost one fifth of patients with well controlled mild to moderate asthma.
Self-report of emotion-induced asthma symptoms in daily life predicted stronger responses to the unpleasant stimuli in the experiment.
Patients’ reports of emotion-induced asthma require medical and behavioral management strategies that acknowledge this specific pathway of exaggerated airway response.
Films and pictures that were emotionally disturbing increased airway resistance in subjects with asthma.
A. TrueB. False
True
False
22%
78%
Films and pictures that were emotionally disturbing increased airway resistance in subjects with asthma.
A. TrueB. False
The correct answer is true. Quoting the paper: “Effect of emotion induction. Relatively uniform changes of resistance were observed across the frequency spectrum with emotion induction. Across all conditions and methods, unpleasant stimuli were associated with the strongest increases in resistance, with significant emotion effects (P < 0.001)
This study proved that subjects with asthma are more emotional than healthy subjects.
A. TrueB. False
True
False
35%
65%
This study proved that subjects with asthma are more emotional than healthy subjects.A. TrueB. False
The correct answer is false. It is a reasonable question to ask whether patients with asthma are more emotional than patients without asthma. The answer to this question may be either true or false, but this study did not ask and did not answer this question.
Why did the authors of the study give ipratropium to the subjects in the experiment?
A. To show that emotions affected airway resistance through specific neural pathways that could be selectively blocked.
B. To prove that ipratropium was an effective medication in asthma.
C. To relieve asthma symptoms that were caused by exposure to emotional stimuli.
A. B. C.
0% 0%0%
Why did the authors of the study give ipratropium to the subjects in the experiment?
A. To show that emotions affected airway resistance through specific neural pathways that could be selectively blocked.
B. To prove that ipratropium was an effective medication in asthma.
C. To relieve asthma symptoms that were caused by exposure to emotional stimuli.
The correct answer is ‘A’. The author’s hypothesis was that emotions affected airway resistance through cholinergic pathways so they blocked cholinergic pathways with the anti-cholinergic medication ipratropium and found that this reduced the airway effects of unpleasant emotional stimuli. This was not a randomized controlled trial to prove that Ipratropium is effective in asthma treatment. Ipatropium was given before the experiment. Rescue inhalers were used after the experiment if necessary.
School Examinations Enhance Airway Inflammation to Antigen ChallengeLIU L.Y. et al (University of Wisconsin and Mayo Clinic)
Am J Respir Crit Care Med 165:1062-1067, 2002.
Even small studies often require the cooperation of multiple specialties and institutions
Lin Ying Liu, Christopher L. Coe, Cheri A. Swenson, Elizabeth A. Kelly, Hirohito Kita, and William W. Busse School Examinations Enhance Airway Inflammation to Antigen Challenge Am J Respir Crit Care Med 165:1062-1067, 2002
Allergy and Immunology and Pulmonary and Critical Care Sections of the Department of Medicine; Department of Psychology, University of Wisconsin, Madison, Wisconsin; and Department of Internal Medicine, Mayo Clinic and Mayo Foundation, Rochester, Minnesota
Recruitment Twenty undergraduate college students (9 males, 11 females) with mild allergic asthma were studied. Each subject had a positive skin-prick test to an allergen and a history of asthma with previous use of asthma medication.
Note that this is an extremely small study (only 20 subjects) which unfortunately is typical of behavioral science studies due to the lack of funding for this specialty.
Study Design The study design was a randomized, two-phase crossover study. One segment was during a low stress period (mid-semester) and the other segment was during a high stress period (final exams week).
A graded inhaled antigen challenge (ragweed, cat dander, or house dust mite) was performed at baseline to determine the dose of antigen that caused an immediate fall in forced expiratory volume in 1 second (FEV1) of at least 20%. This same dose of antigen was given for the subsequent antigen inhalation challenges in both low stress (mid-semester) and high stress (final exams) study segments.
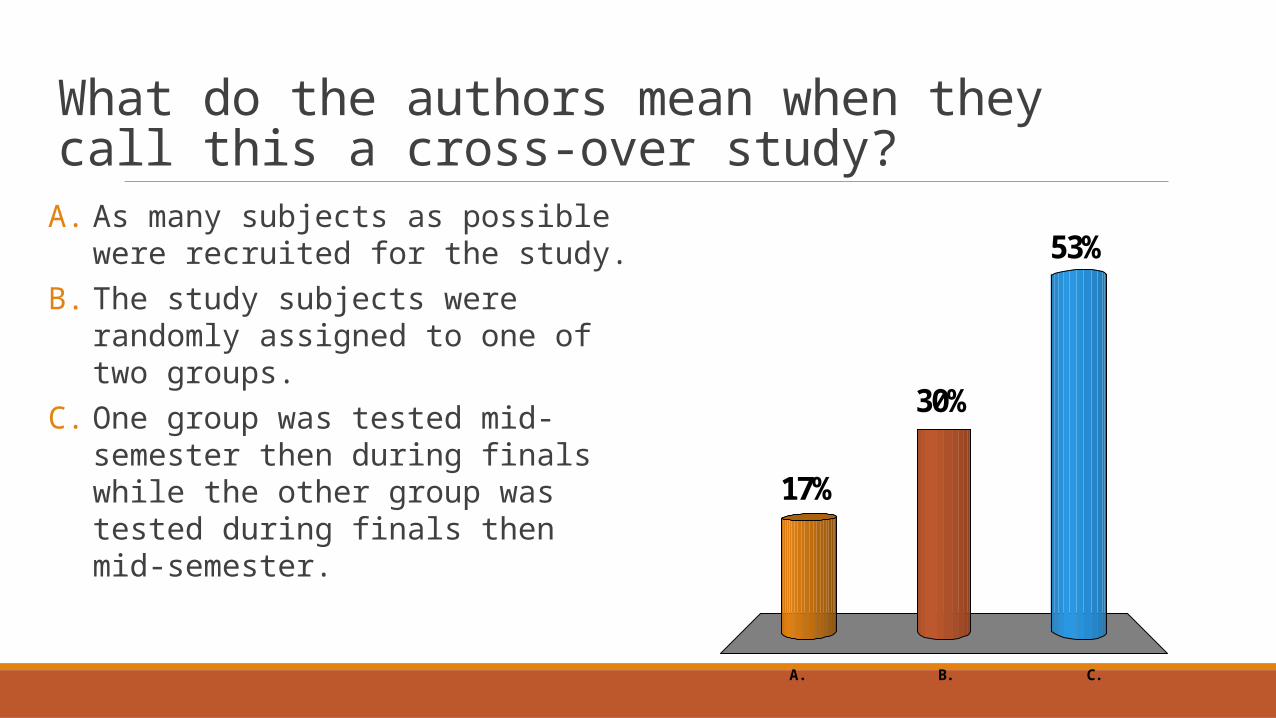
What do the authors mean when they call this a cross-over study?
A. As many subjects as possible were recruited for the study.
B. The study subjects were randomly assigned to one of two groups.
C. One group was tested mid-semester then during finals while the other group was tested during finals then mid-semester.
A. B. C.
17%
53%
30%
What do the authors mean when they call this a cross-over study?
A. As many subjects as possible were recruited for the study.
B. The study subjects were randomly assigned to one of two groups.
C. One group was tested mid-semester then during finals while the other group was tested during finals then mid-semester.
The correct answer is ‘C’. The authors were concerned that the order of the tests – mid-term then finals or finals and then mid-term – might influence the results. The group that had testing mid-semester first crossed over to have testing at finals while the other group had the opposite sequence.

Design of a cross-over study
Mid-term (low stress) Final exam week (high stress)
Group #1First test
Group #1Second test
Group #2Second test
Group #2First test
Study Design At each study period, a questionnaire was given to assess psychological stress, spirometry was performed to evaluate bronchoconstriction and blood and sputum samples were collected to evaluate for markers of inflammation.
Blood was analyzed for white blood cell count and differential (including eosinophils) and for basal cortisol levels.
Sputum was obtained for white blood cell count and differential (including eosinophils) and sputum was cultured for cytokines (IL-5 and IFN-γ) and EDN (eosinophil derived neurotoxin).
Results The psychological assessment indicated that although none of the students exhibited clinical levels of anxiety or depression, there was a small but significant increase in their emotional distress, as indicated by increases in STAI (30±0.9 low-stress versus 33±0.8 stress) and BDI scores (1.7±0.5 low stress versus 3.4±0.8 high stress) comparing mid-term to final examination week.
Plasma cortisol levels were not significantly increased during examination week (21.9 2.1 g/dl mid-term versus 24.6 2.7 g/dl final exams).
Results The final examination week did not have an effect on baseline lung function as measured by FEV1 (92.4±2.4% mid-term versus 92.1±2.8% final exams).
Total leukocyte count in induced sputum at six and 24 hours after a standardized antigen challenge was greater during final examination week than during the low stress period (p<0.01). This increase in sputum leukocytes was primarily eosinophils.
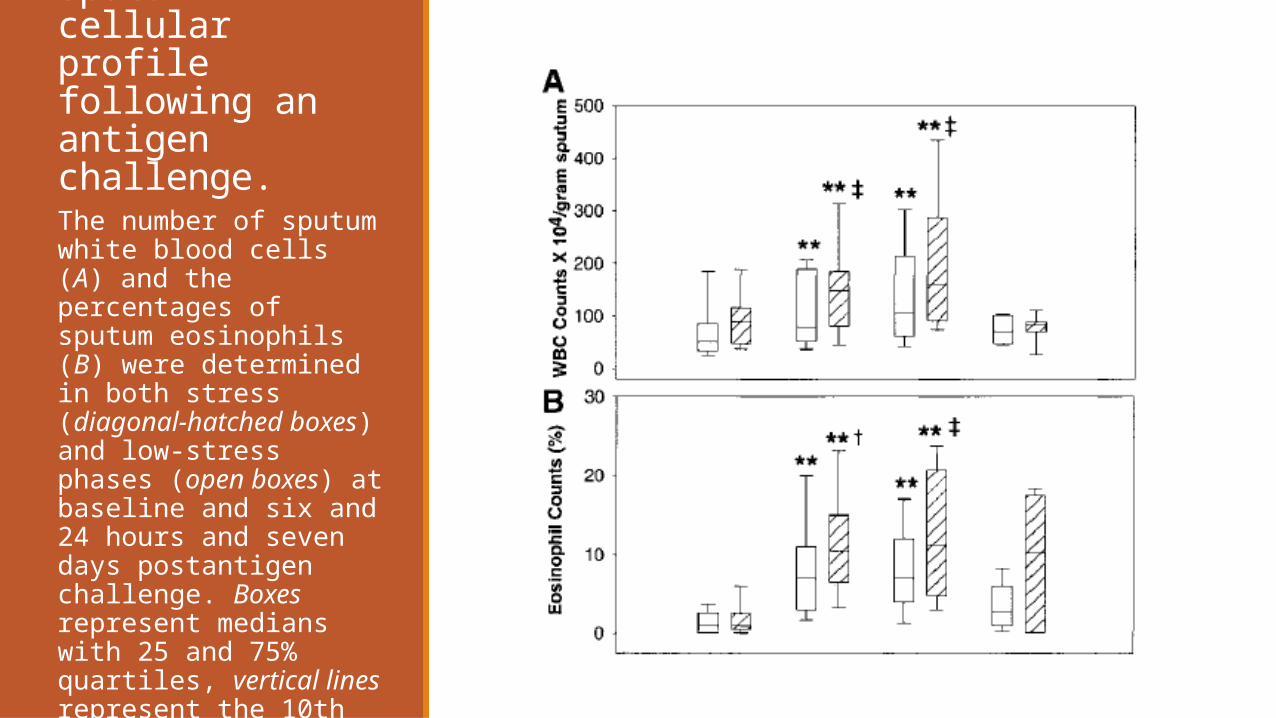
Effect of sputum cellular profile following anantigen challenge.The number of sputum white blood cells (A) and the percentages of sputum eosinophils (B) were determined in both stress (diagonal-hatched boxes) and low-stress phases (open boxes) at baseline and six and 24 hours and seven days postantigen challenge. Boxes represent medians with 25 and 75% quartiles, vertical lines represent the 10th and 90th percentiles. **p <0.01, versus baseline; †p< 0.05, ‡p< 0.01, high versus low-stress.
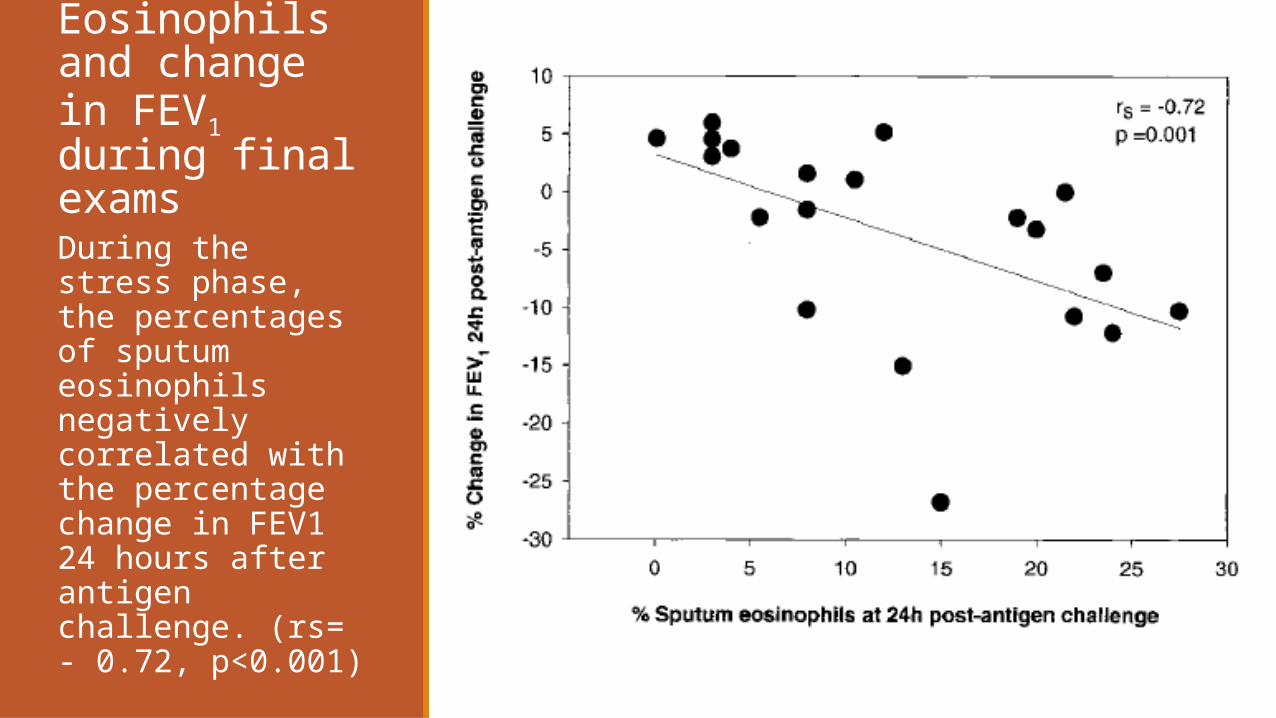
Eosinophils and change in FEV1 during final examsDuring the stress phase, the percentages of sputum eosinophils negatively correlated with the percentage change in FEV1 24 hours after antigen challenge. (rs= - 0.72, p<0.001)
What could the authors conclude from their study?
A. Mild stress (final exam week) significantly reduced FEV1 in subjects with mild asthma.
B. Even relatively mild stress increases markers of airway inflammation including WBC and eosinophils.
C. Students at the University of Wisconsin are remarkably calm about final exams.
A. B. C.
42%
12%
46%
What could the authors conclude from their study?
A. Mild stress (final exam week) significantly reduced FEV1 in subjects with mild asthma.
B. Even relatively mild stress increases markers of airway inflammation including WBC and eosinophils.
C. Students at the University of Wisconsin are remarkably calm about final exams.
The correct answer is ‘B’. Both total WBC and eosinophils in sputum after an antigen challenge increased significantly more during finals week than during the semester (p<0.05 to p<0.01). There was a correlation of decreased FEV1 with eosinophil count but not sufficient to be seen in a comparison of high/low stress.
I would never put ‘C’ in a real test, but UW students really didn’t seem all that stressed.
Conclusions The study findings suggest that stress associated with final examinations can increase eosinophilic airway inflammation to antigen challenge and thus may enhance asthma severity.
Functional Relaxation and Guided Imagery as Complementary Therapy in Asthma: A Randomized Controlled Clinical TrialC. LAHMANN et al
PSYCHOTHER PSYCHOSOM 2009;78:233–239
Functional Relaxation for Asthma 64 patients with well controlled extrinsic asthma were randomized into 3 treatment groups and a control group.
The average age of all participants was 42.9±12.2 years, 64% were female.
The treatment groups were given one hour of instruction in functional relaxation and/or guided imagery once weekly for 4 weeks.
Measures of pulmonary function (FEV1 and sRaw) were assessed at baseline, immediately after treatment and at 4 months.
Functional Relaxation for Asthma Participation in functional relaxation (FR), guided imagery (GI)and a combination of both led to increases in FEV1 (% predicted) of 7.6±13.2, 3.3±9.8, and 8.3±21.0, respectively, as compared to –1.8 ±11.1 in the control group at the end of the therapy.
At 4 months after the training sessions, the increases in FEV 1 were 6.9±10.3 (p = 0.009) in the FR group, 4.4±7.3 (p = 0.072) in the GI, 4.5±8.1 (p =0.066) in the FR/GI and –2.8±9.2 in the control.
The analyses relating to changes in FEV1 revealed that only the FR group reached a level of statistical significance when compared to the control.
The study authors’ conclusions Our study confirms a positive effect of FR on respiratory parameters and suggests a clinically relevant long-term benefit from FR as a nonpharmacological and complementary therapy treatment option.
My Comments There are many studies of various behavioral interventions in asthma but relatively few well designed randomized trials with the power to show clinically significant improvements in pulmonary function.
The response to behavioral interventions are less than what would be considered clinically significant for medications (see discussion of post-bronchodilator response in spirometry).
As the authors of this study point out, (quote) “relaxation therapies are still not recommended in treatment guidelines due to a lack of methodological quality in many of the trials.”
Post-Bronchodilator Response Performance of spirometry before and after bronchodilator is used to determine the degree of reversibility of airflow limitation.
Salbutamol (4 inhalations of 90 to 100 mcg) is administered by metered dose inhaler with a spacer or chamber device. Spirometry is repeated 10 to 15 minutes after administration of a bronchodilator and compared to the patient’s baseline.
In a patient with airway obstruction, an increase in the FEV1 of more than 12 percent and greater than 0.2 L suggests acute bronchodilator responsiveness.
Should behavioral therapy be part of the treatment for asthma.
A. YesB. No
Yes No
6%
94%
Should behavioral therapy be part of the treatment for asthma.A. YesB. No
There is no ‘correct’ answer to this question. My own opinion is that the treatment of asthma with symptoms that significantly interfere with the patient’s quality of life or present a risk of acute respiratory distress requires the thoughtful use of medications. Having said that, behavioral therapy can improve the quality of a patient’s life by reducing anxiety and improving medication compliance.
Other potential roles for behavioral medicine in the treatment of asthma Medication adherence Beliefs about illness and treatment Perception of airway obstruction Specific health habits
◦ Smoking cessation (for smokers)◦ Obesity◦ Physical fitness

The Value of Breathing Technique and Reassurance for Severe Asthma: an anecdotal experienceGEOFFREY GATES, MD, FACP
United Airlines Flight from London to Chicago 2005
The value of breathing technique and reassurance
I was on a flight from London to Chicago in 2005 when an airline stewardess asked if there was a doctor on the flight. I responded in accordance with the ethical obligation of physicians to offer assistance to patients in need.
The patient was a 58 year old male with a history of asthma who had been on vacation in London. His asthma had worsened in the week before he was scheduled to return home, but he did not want to go to a doctor in a foreign country so he simply increased the use of his rescue inhaler. While he felt tightness in his chest on boarding the aircraft, he was not obviously short of breathe or audibly wheezing.
The value of breathing technique and reassurance
As the plane ascending to the cruising altitude of 12,000 meters, he became acutely short of breath. He began to wheeze audibly, which gradually diminished even as he become more visibly short of breathe. The stewardess got a portable oxygen tank and called for a doctor.
Airliners maintain cabin pressure below 2,400 meters while cruising at altitudes up to 12,000 meters, but the air at 2,400 meters has 25% less oxygen than at sea level.
The value of breathing technique and reassurance
I gave him an injection of adrenaline. When he showed some improvement, I administered his inhaled bronchodilator with appropriate technique.
Equally important was improving his breathing technique and calming him.
His rapid breathing at twice the normal rate promoted air trapping because he did not give sufficient time to exhale against resistance.
His fear and struggling increased his consumption of oxygen at the same time that his asthma was hindering his ability to take in the oxygen he needed.
The value of breathing technique and reassurance
With reassurance to calm him and instructions to improve the mechanics of his breathing, he became more comfortable. The improvement was reflected in his vitals and auscultation of his chest.
When paramedics met the flight on the runway in Chicago, they complained to me that they should not have been called since he didn’t appear to be seriously ill. He became frightened by the aggressive tactics to get him on a stretcher and promptly began to wheeze audibly and struggle for breathe. He was then carried off the plane in obvious distress.
Three lessons from this anecdote The first lesson is that reassurance of an exceptionally anxious patient can make a difference in whether the patient improves or deteriorates.
The second lesson is that patient education (in this case breathing technique) is an often neglected aspect of patient care.
The third lesson is that the way in which you care for a patient is sometimes as important as the medications that you administer.
(The fourth lesson is that the airline will give you a bottle of champagne from 1st class and a note of thanks for offering to help.)



















