Behavioral Health Initial form 1 - Home - AlohaCare · BEHAVIORAL HEALTH LOB: QUEST ACAP Service...
6
BEHAVIORAL HEALTH LOB: QUEST ACAP Service Type: MH CD Dual DX Auth Request Type: Standard Retro 1. Provider/Facility:______________________________________ Contact Person:________________________________________ Big Island Maui Oahu Molokai Kauai Lanai Phone: Fax: Request Date: 2. Member Name:_______________________________________________ Member ID:_______________________ DOB:_____/____/__________ Age:________ __ 3. DSM/ICD 10 Diagnostic codes: Primary:___________________________________________________ Secondary:_________________________________________________ __________________________________________________________ 4. Medical Conditions: ______________________________________________________________ 5. Z Codes: Please check areas of concern ( if applicable) Primary Support Group Legal System/Crime Housing Economic Social Environment Occupational Access to Care Educational Other:_________________________________________________________ 7. Requested # of Sessions:_________________________________________ From:_________________ ___________To: ___________________________ 8. Required Documentation: Please submit required clinical notes for either 6A or 6B as listed below: A. Outpatient Mental Health: Clinical Summary Behavioral Contract (If applicable) B. Chemical Dependency/Dual Diagnosis: UA results Behavioral Contract (If applicable); progress notes and relapse prevention plan. 9. If this is a Retrorequest please explain why: ___________________________ ____________________________________________________________________ 6. Level of Care Requested: Social Detox Res PHP IOP LIOP OPS Methadone Maintenance 10. Does member require an Interpreter? Yes No If yes, what language:___________________________________________________ Is Care Coordination requested: Yes No (If yes, please explain):____________________________________________________________________________________ QUEST only: Potential SMI/SPMI/SEBD: Yes No INITIAL MENTAL HEALTH OUTPATIENT AND/OR CHEMICAL DEPENDENCY PRIOR AUTH REQUEST FORM April 2016 Page 1 of 6
Transcript of Behavioral Health Initial form 1 - Home - AlohaCare · BEHAVIORAL HEALTH LOB: QUEST ACAP Service...

Page 1 of 3
BEHAVIORAL HEALTH LOB: QUEST ACAP
Service Type: MH CD Dual DX Auth Request Type: Standard Retro
1. Provider/Facility:______________________________________
Contact Person:________________________________________
Big Island Maui Oahu
Molokai Kauai Lanai
Phone: Fax: Request Date:
2. 2. Member Name:_______________________________________________ Member ID:_______________________ DOB:_____/____/__________ Age:________ __
3. DSM/ICD 10 Diagnostic codes:
Primary:___________________________________________________
Secondary:_________________________________________________
__________________________________________________________
4. Medical Conditions:
______________________________________________________________
5. Z Codes: Please check areas of concern ( if applicable)
Primary Support Group Legal System/Crime Housing Economic Social Environment Occupational Access to Care Educational
Other:_________________________________________________________
7. Requested # of Sessions:_________________________________________
From:_________________ ___________To: ___________________________
8. Required Documentation: Please submit required clinical notes for either 6A or6B as listed below:
A. Outpatient Mental Health: Clinical Summary Behavioral Contract (If applicable)
B. Chemical Dependency/Dual Diagnosis: UA results Behavioral Contract (If applicable); progress notes and relapse prevention plan.
9. If this is a Retro-‐request please explain why: ___________________________
____________________________________________________________________
6. Level of Care Requested:
Social Detox Res PHP IOP LIOP OPS Methadone Maintenance 8. 10. Does member require an Interpreter? Yes No If yes, what language:___________________________________________________
Is Care Coordination requested: Yes No (If yes, please explain):____________________________________________________________________________________
QUEST only: Potential SMI/SPMI/SEBD: Yes No
INITIAL MENTAL HEALTH OUTPATIENT AND/OR CHEMICAL DEPENDENCY PRIOR AUTH REQUEST FORM
Contact Person
April 2016 Page 1 of 6

Page 2 of 3
CLINICAL INFORMATION: (Please complete the following)
Substance Abuse Treatment History: Yes No (If Yes, please complete the grid below) Treatment #1 Treatment #2 Treatment #3 Treatment #4
Dates of TX: Facility: Level of Care: Substance: Length of TX: TX Outcome:
1. Why is member seeking treatment: ______________________________________________________________________________________________________________2. Any CWS (CPS) involvement? Yes No (If Yes, please provide name and phone # of CWS (CPS) worker):________________________________________________ 3. Any pending legal charges? Yes No (If Yes, please explain):___________________________________________________________________________________ 4. Probation/Parole officer name and # if applicable:_____________________________________________________________________ _____________________________5. Recent incarceration? Yes No (If yes, date of release):_________________________________________________________________________________________
6. Substance Use:Drug(s) of Choice: Age of Onset: Date of Last Use: Amount Used: How Often Used:
7. Psychiatric history? Yes No (If yes, please provide DX):________________________________________________________________________________________ 8. Any current psych. symptoms? Yes No (If yes, please describe):_________________________________________________________________________________
____________________________________________________________________________________________________________________________________________ 9. Potential safety risk? Yes No (If yes, please explain):_________________________________________________________________________________________
10. Current psychiatric medication? Yes No Unknown (If yes, please fill out box below): Medication Dose/Frequency Start Date Prescriber/Specialty
Is member adherent with meds? Yes No
April 2016 Page 2 of 6

Page 3 of 3
ASAM DIMENSIONS (please explain all medium and high ratings) 1. Alcohol Intox. And/or Withdrawal Potential
• Any risk of severe withdrawal/seizures?• Any current signs of withdrawal?
LOW MED HIGH EXPLAIN
2. Biomedical Conditions & Complications• Any current physical illness (besides withdrawal) that may
impact course of treatment?• Is member pregnant? Yes No
3. Emotional/ Behavioral or Cognitive Conditions & Complications• Any psych. Illness or psychological, behavioral, or emotional
problems that may impact the course of treatment?4. Readiness to Change (Treatment Acceptance/Resistance)
• Is the member objecting/resistant to treatment?• What is the member’s readiness to change?
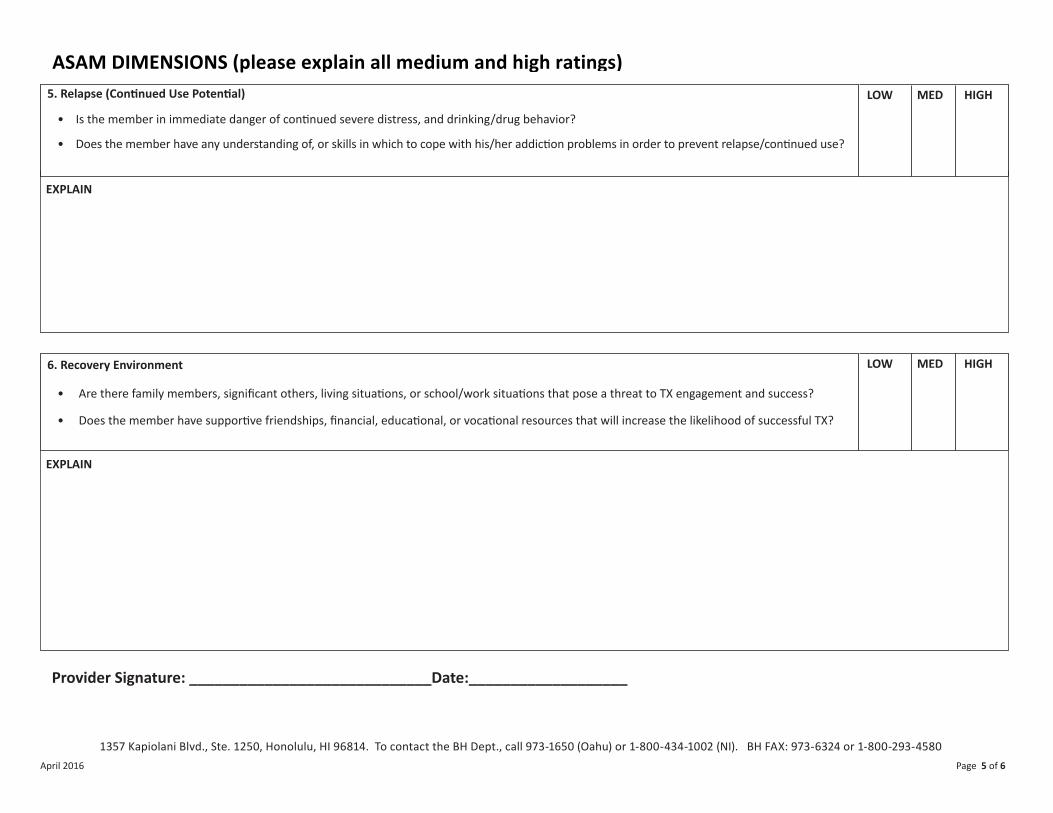
5. Relapse (Continued Use Potential)• Is the member in immediate danger of continued severe
distress, and drinking/drug behavior?• Does the member have any understanding of, or skills in
which to cope with his/her addiction problems in order toprevent relapse/continued use?
6. Recovery Environment• Are there family members, significant others, living
situations, or school/work situations that pose a threat to TXengagement and success?
• Does the member have supportive friendships, financial,educational, or vocational resources that will increase thelikelihood of successful TX?
Provider Signature: ______________________________________Date:_______________________
LEVEL OF CARE DETERMINATION: **For AC Use onlyLOC DATE OF
REQUESTSESSIONS START DATE END DATE TX PLAN
DUE DATETCDUE DATE
AUTH # CRITERIA USED
APPROVED: YES NO PARTIAL DATE OF DECISION: Reviewers signature____________________________ MD Signature:__________________________________
1357 Kapiolani Blvd., Ste. 1250, Honolulu, HI 96814. BH Phone: 973-‐2475 (Oahu) or 1-‐888-‐875-‐4979 (NI). BH FAX: 973-‐6324 or 1-‐800-‐293-‐4580
April 2016 Page 3 of 3
1357 Kapiolani Blvd., Ste. 1250, Honolulu, HI 96814. To contact the BH Dept., call 973-1650 (Oahu) or 1-800-434-1002 (NI). BH FAX: 973 -6324 or 1-800-293-4580
EXPLAIN
Page 3 of 3
ASAM DIMENSIONS (please explain all medium and high ratings)1. Alcohol Intox. And/or Withdrawal Potential
• Any risk of severe withdrawal/seizures?• Any current signs of withdrawal?
LOW MED HIGH EXPLAIN
2. Biomedical Conditions & Complications• Any current physical illness (besides withdrawal) that may
impact course of treatment?• Is member pregnant? Yes No
3. Emotional/ Behavioral or Cognitive Conditions & Complications• Any psych. Illness or psychological, behavioral, or emotional
problems that may impact the course of treatment?4. Readiness to Change (Treatment Acceptance/Resistance)
• Is the member objecting/resistant to treatment?• What is the member’s readiness to change?
5. Relapse (Continued Use Potential)• Is the member in immediate danger of continued severe
distress, and drinking/drug behavior?• Does the member have any understanding of, or skills in
which to cope with his/her addiction problems in order toprevent relapse/continued use?
6. Recovery Environment• Are there family members, significant others, living
situations, or school/work situations that pose a threat to TXengagement and success?
• Does the member have supportive friendships, financial,educational, or vocational resources that will increase thelikelihood of successful TX?
Provider Signature: ______________________________________Date:_______________________
LEVEL OF CARE DETERMINATION: **For AC Use onlyLOC DATE OF
REQUESTSESSIONS START DATE END DATE TX PLAN
DUE DATETCDUE DATE
AUTH # CRITERIA USED
APPROVED: YES NO PARTIAL DATE OF DECISION: Reviewers signature____________________________ MD Signature:__________________________________
1357 Kapiolani Blvd., Ste. 1250, Honolulu, HI 96814. BH Phone: 973-‐2475 (Oahu) or 1-‐888-‐875-‐4979 (NI). BH FAX: 973-‐6324 or 1-‐800-‐293-‐4580
April 2016 Page 3 of 3
1357 Kapiolani Blvd., Ste. 1250, Honolulu, HI 96814. To contact the BH Dept., call 973-1650 (Oahu) or 1-800-434-1002 (NI). BH FAX: 973 -6324 or 1- 800- 293-4580
April 2016 Page 3 of 6
• Any current physical illness (besides withdrawal) that may impact course of treatment?• Is member pregnant?
2. Biomedical Conditions & Complications HIGHLOW MED
Yes No
• Any risk of severe withdrawal/seizures?• Any current signs of withdrawal?
EXPLAIN
1. Alcohol Intox. And/or Withdrawal Potential HIGHLOW MED

Page 3 of 3
ASAM DIMENSIONS (please explain all medium and high ratings) 1. Alcohol Intox. And/or Withdrawal Potential
• Any risk of severe withdrawal/seizures?• Any current signs of withdrawal?
LOW MED HIGH EXPLAIN
2. Biomedical Conditions & Complications• Any current physical illness (besides withdrawal) that may
impact course of treatment?• Is member pregnant? Yes No
3. Emotional/ Behavioral or Cognitive Conditions & Complications• Any psych. Illness or psychological, behavioral, or emotional
problems that may impact the course of treatment?4. Readiness to Change (Treatment Acceptance/Resistance)
• Is the member objecting/resistant to treatment?• What is the member’s readiness to change?
5. Relapse (Continued Use Potential)• Is the member in immediate danger of continued severe
distress, and drinking/drug behavior?• Does the member have any understanding of, or skills in
which to cope with his/her addiction problems in order toprevent relapse/continued use?
6. Recovery Environment• Are there family members, significant others, living
situations, or school/work situations that pose a threat to TXengagement and success?
• Does the member have supportive friendships, financial,educational, or vocational resources that will increase thelikelihood of successful TX?
Provider Signature: ______________________________________Date:_______________________
LEVEL OF CARE DETERMINATION: **For AC Use onlyLOC DATE OF
REQUESTSESSIONS START DATE END DATE TX PLAN
DUE DATETCDUE DATE
AUTH # CRITERIA USED
APPROVED: YES NO PARTIAL DATE OF DECISION: Reviewers signature____________________________ MD Signature:__________________________________
1357 Kapiolani Blvd., Ste. 1250, Honolulu, HI 96814. BH Phone: 973-‐2475 (Oahu) or 1-‐888-‐875-‐4979 (NI). BH FAX: 973-‐6324 or 1-‐800-‐293-‐4580
April 2016 Page 3 of 3
1357 Kapiolani Blvd., Ste. 1250, Honolulu, HI 96814. To contact the BH Dept., call 973-1650 (Oahu) or 1-800-434-1002 (NI). BH FAX: 973 -6324 or 1-800-293-4580
EXPLAIN
EXPLAIN
Page 3 of 3
ASAM DIMENSIONS (please explain all medium and high ratings)1. Alcohol Intox. And/or Withdrawal Potential
• Any risk of severe withdrawal/seizures?• Any current signs of withdrawal?
LOW MED HIGH EXPLAIN
2. Biomedical Conditions & Complications• Any current physical illness (besides withdrawal) that may
impact course of treatment?• Is member pregnant? Yes No
3. Emotional/ Behavioral or Cognitive Conditions & Complications• Any psych. Illness or psychological, behavioral, or emotional
problems that may impact the course of treatment?4. Readiness to Change (Treatment Acceptance/Resistance)
• Is the member objecting/resistant to treatment?• What is the member’s readiness to change?
5. Relapse (Continued Use Potential)• Is the member in immediate danger of continued severe
distress, and drinking/drug behavior?• Does the member have any understanding of, or skills in
which to cope with his/her addiction problems in order toprevent relapse/continued use?
6. Recovery Environment• Are there family members, significant others, living
situations, or school/work situations that pose a threat to TXengagement and success?
• Does the member have supportive friendships, financial,educational, or vocational resources that will increase thelikelihood of successful TX?
Provider Signature: ______________________________________Date:_______________________
LEVEL OF CARE DETERMINATION: **For AC Use onlyLOC DATE OF
REQUESTSESSIONS START DATE END DATE TX PLAN
DUE DATETCDUE DATE
AUTH # CRITERIA USED
APPROVED: YES NO PARTIAL DATE OF DECISION: Reviewers signature____________________________ MD Signature:__________________________________
1357 Kapiolani Blvd., Ste. 1250, Honolulu, HI 96814. BH Phone: 973-‐2475 (Oahu) or 1-‐888-‐875-‐4979 (NI). BH FAX: 973-‐6324 or 1-‐800-‐293-‐4580
April 2016 Page 3 of 3
1357 Kapiolani Blvd., Ste. 1250, Honolulu, HI 96814. To contact the BH Dept., call 973-1650 (Oahu) or 1-800-434-1002 (NI). BH FAX: 973 -6324 or 1- 800- 293-4580
April 2016 Page 4 of 6
• Is the member objecting/resistant to treatment?• What is the member’s readiness to change?
4. Readiness to Change (Treatment Acceptance/Resistance) HIGHLOW MED
• Any psych. Illness or psychological, behavioral, or emotional problems that may impact the course of treatment?3. Emotional/ Behavioral or Cognitive Conditions & Complications HIGHLOW MED
Page 3 of 3
ASAM DIMENSIONS (please explain all medium and high ratings) 1. Alcohol Intox. And/or Withdrawal Potential
• Any risk of severe withdrawal/seizures?• Any current signs of withdrawal?
LOW MED HIGH EXPLAIN
2. Biomedical Conditions & Complications• Any current physical illness (besides withdrawal) that may
impact course of treatment?• Is member pregnant? Yes No
3. Emotional/ Behavioral or Cognitive Conditions & Complications• Any psych. Illness or psychological, behavioral, or emotional
problems that may impact the course of treatment?4. Readiness to Change (Treatment Acceptance/Resistance)
• Is the member objecting/resistant to treatment?• What is the member’s readiness to change?
5. Relapse (Continued Use Potential)• Is the member in immediate danger of continued severe
distress, and drinking/drug behavior?• Does the member have any understanding of, or skills in
which to cope with his/her addiction problems in order toprevent relapse/continued use?
6. Recovery Environment• Are there family members, significant others, living
situations, or school/work situations that pose a threat to TXengagement and success?
• Does the member have supportive friendships, financial,educational, or vocational resources that will increase thelikelihood of successful TX?
Provider Signature: ______________________________________Date:_______________________
LEVEL OF CARE DETERMINATION: **For AC Use only LOC DATE OF
REQUEST SESSIONS START DATE END DATE TX PLAN
DUE DATE TC DUE DATE
AUTH # CRITERIA USED
APPROVED: YES NO PARTIAL DATE OF DECISION: Reviewers signature____________________________ MD Signature:__________________________________
1357 Kapiolani Blvd., Ste. 1250, Honolulu, HI 96814. BH Phone: 973-‐2475 (Oahu) or 1-‐888-‐875-‐4979 (NI). BH FAX: 973-‐6324 or 1-‐800-‐293-‐4580
April 2016 Page 3 of 3
1357 Kapiolani Blvd., Ste. 1250, Honolulu, HI 96814. To contact the BH Dept., call 973-1650 (Oahu) or 1-800-434-1002 (NI). BH FAX: 973 -6324 or 1- 800- 293-4580
EXPLAIN
EXPLAIN
Provider Signature: _____________________________Date:___________________
• Does the member have supportive friendships, financial, educational, or vocational resources that will increase the likelihood of successful TX?
• Are there family members, significant others, living situations, or school/work situations that pose a threat to TX engagement and success?
6. Recovery Environment HIGHLOW MED
• Is the member in immediate danger of continued severe distress, and drinking/drug behavior?
• Does the member have any understanding of, or skills in which to cope with his/her addiction problems in order to prevent relapse/continued use?
5. Relapse (Continued Use Potential) HIGHLOW MED
April 2016
Page 3 of 3
ASAM DIMENSIONS (please explain all medium and high ratings) 1. Alcohol Intox. And/or Withdrawal Potential
• Any risk of severe withdrawal/seizures?• Any current signs of withdrawal?
LOW MED HIGH EXPLAIN
2. Biomedical Conditions & Complications• Any current physical illness (besides withdrawal) that may
impact course of treatment?• Is member pregnant? Yes No
3. Emotional/ Behavioral or Cognitive Conditions & Complications• Any psych. Illness or psychological, behavioral, or emotional
problems that may impact the course of treatment?4. Readiness to Change (Treatment Acceptance/Resistance)
• Is the member objecting/resistant to treatment?• What is the member’s readiness to change?
5. Relapse (Continued Use Potential)• Is the member in immediate danger of continued severe
distress, and drinking/drug behavior?• Does the member have any understanding of, or skills in
which to cope with his/her addiction problems in order toprevent relapse/continued use?
6. Recovery Environment• Are there family members, significant others, living
situations, or school/work situations that pose a threat to TXengagement and success?
• Does the member have supportive friendships, financial,educational, or vocational resources that will increase thelikelihood of successful TX?
Provider Signature: ______________________________________Date:_______________________
LEVEL OF CARE DETERMINATION: **For AC Use only LOC DATE OF
REQUEST SESSIONS START DATE END DATE TX PLAN
DUE DATE TC DUE DATE
AUTH # CRITERIA USED
APPROVED: YES NO PARTIAL DATE OF DECISION: Reviewers signature____________________________ MD Signature:__________________________________
1357 Kapiolani Blvd., Ste. 1250, Honolulu, HI 96814. BH Phone: 973-‐2475 (Oahu) or 1-‐888-‐875-‐4979 (NI). BH FAX: 973-‐6324 or 1-‐800-‐293-‐4580
April 2016 Page 3 of 3
1357 Kapiolani Blvd., Ste. 1250, Honolulu, HI 96814. To contact the BH Dept., call 973-1650 (Oahu) or 1-800-434-1002 (NI). BH FAX: 973 -6324 or 1- 800- 293-4580Page 5 of 6

Page 3 of 3
ASAM DIMENSIONS (please explain all medium and high ratings)1. Alcohol Intox. And/or Withdrawal Potential
• Any risk of severe withdrawal/seizures?• Any current signs of withdrawal?
LOW MED HIGH EXPLAIN
2. Biomedical Conditions & Complications• Any current physical illness (besides withdrawal) that may
impact course of treatment?• Is member pregnant? Yes No
3. Emotional/ Behavioral or Cognitive Conditions & Complications• Any psych. Illness or psychological, behavioral, or emotional
problems that may impact the course of treatment?4. Readiness to Change (Treatment Acceptance/Resistance)
• Is the member objecting/resistant to treatment?• What is the member’s readiness to change?
5. Relapse (Continued Use Potential)• Is the member in immediate danger of continued severe
distress, and drinking/drug behavior?• Does the member have any understanding of, or skills in
which to cope with his/her addiction problems in order toprevent relapse/continued use?
6. Recovery Environment• Are there family members, significant others, living
situations, or school/work situations that pose a threat to TXengagement and success?
• Does the member have supportive friendships, financial,educational, or vocational resources that will increase thelikelihood of successful TX?
Provider Signature: ______________________________________Date:_______________________
LEVEL OF CARE DETERMINATION: **For AC Use onlyLOC DATE OF
REQUEST SESSIONS START DATE END DATE TX PLAN
DUE DATE TC DUE DATE
AUTH # CRITERIA USED
APPROVED: YES NO PARTIAL DATE OF DECISION: Reviewers signature____________________________ MD Signature:__________________________________
1357 Kapiolani Blvd., Ste. 1250, Honolulu, HI 96814. BH Phone: 973-‐2475 (Oahu) or 1-‐888-‐875-‐4979 (NI). BH FAX: 973-‐6324 or 1-‐800-‐293-‐4580
April 2016 Page 3 of 3
1357 Kapiolani Blvd., Ste. 1250, Honolulu, HI 96814. To contact the BH Dept., call 973-1650 (Oahu) or 1-800-434-1002 (NI). BH FAX: 973 -6324 or 1- 800- 293-4580
LEVEL OF CARE DETERMINATION: ** FOR AC Use Only
Page 3 of 3
ASAM DIMENSIONS (please explain all medium and high ratings)1. Alcohol Intox. And/or Withdrawal Potential
• Any risk of severe withdrawal/seizures?• Any current signs of withdrawal?
LOW MED HIGH EXPLAIN
2. Biomedical Conditions & Complications• Any current physical illness (besides withdrawal) that may
impact course of treatment?• Is member pregnant? Yes No
3. Emotional/ Behavioral or Cognitive Conditions & Complications• Any psych. Illness or psychological, behavioral, or emotional
problems that may impact the course of treatment?4. Readiness to Change (Treatment Acceptance/Resistance)
• Is the member objecting/resistant to treatment?• What is the member’s readiness to change?
5. Relapse (Continued Use Potential)• Is the member in immediate danger of continued severe
distress, and drinking/drug behavior?• Does the member have any understanding of, or skills in
which to cope with his/her addiction problems in order toprevent relapse/continued use?
6. Recovery Environment• Are there family members, significant others, living
situations, or school/work situations that pose a threat to TXengagement and success?
• Does the member have supportive friendships, financial,educational, or vocational resources that will increase thelikelihood of successful TX?
Provider Signature: ______________________________________Date:_______________________
LEVEL OF CARE DETERMINATION: **For AC Use onlyLOC DATE OF
REQUESTSESSIONS START DATE END DATE TX PLAN
DUE DATETCDUE DATE
AUTH # CRITERIA USED
APPROVED: YES NO PARTIAL DATE OF DECISION: Reviewers signature____________________________ MD Signature:__________________________________
1357 Kapiolani Blvd., Ste. 1250, Honolulu, HI 96814. BH Phone: 973-‐2475 (Oahu) or 1-‐888-‐875-‐4979 (NI). BH FAX: 973-‐6324 or 1-‐800-‐293-‐4580
April 2016 Page 3 of 3
1357 Kapiolani Blvd., Ste. 1250, Honolulu, HI 96814. To contact the BH Dept., call 973-1650 (Oahu) or 1-800-434-1002 (NI). BH FAX: 973 -6324 or 1- 800- 293-4580
April 2016 Page 6 of 6