Behavioral Economics and Health
20
Behavioral Economics and Health Congressional Staff Briefing April 12, 2013 Department of Department of Health Care Health Care Management Management Center for Health Center for Health Incentives and Incentives and Behavioral Behavioral Economics, Economics, Leonard Davis Leonard Davis Institute Institute CHERP, CHERP, Philadelphia VA Philadelphia VA Medical Center Medical Center University of University of Pennsylvania Pennsylvania School of Medicine School of Medicine Kevin Volpp, MD, PhD
description
Behavioral Economics and Health. Congressional Staff Briefing April 12, 2013. Kevin Volpp, MD, PhD. Department of Health Care Management. Center for Health Incentives and Behavioral Economics, Leonard Davis Institute. University of Pennsylvania School of Medicine. - PowerPoint PPT Presentation
Transcript of Behavioral Economics and Health

Behavioral Economics and Health
Congressional Staff BriefingApril 12, 2013
Department of Health Department of Health Care ManagementCare Management
Center for Health Center for Health Incentives and Incentives and Behavioral Economics, Behavioral Economics, Leonard Davis Institute Leonard Davis Institute
CHERP, Philadelphia CHERP, Philadelphia VA Medical CenterVA Medical Center
University of Pennsylvania University of Pennsylvania School of MedicineSchool of Medicine
Kevin Volpp, MD, PhD

Kevin Volpp, MD, PhD – not for reproduction without permission
22
Employers report poor health habits as top challenge to maintaining affordable benefits
Source: 2012 17th Annual Towers Watson/ NBGH Employer Survey on Purchasing Value in Healthcare

Kevin Volpp, MD, PhD – not for reproduction without permission
33
Employers are increasingly using incentives to drive better health behaviors
Use of incentives by large employers (>1,000) 2009-13
Source: NBGH/Towers Watson 2011 Staying@ Work survey and 2012 Towers Watson/NBGH Employer Survey on Purchasing Value in Healthcare

Kevin Volpp, MD, PhD – not for reproduction without permission
44
Public policy also reflecting importance of incentives. . .
•Section 2705 of the Affordable Care Act allows penalties or rewards of 30-50%
• Premium adjustment may primarily result in cost shifting
Most effectively changing individual behavior likely requires behavioral economics
Source: Volpp KG, Asch DA, Galvin R, Loewenstein G. NEJM. 2011 365: 388-390,Funded by National Institute of Aging

Kevin Volpp, MD, PhD – not for reproduction without permission
55
Making medications free is not enough to drive increased adherence
Medication Adherence
Source: Choudhry et al, NEJM 2011
• 2 RCTs among patients discharged after myocardial infarctionA. $0 CopaymentsB. Standard Copay
• Did not reduce rate of first major vascular event or revascularization

Kevin Volpp, MD, PhD – not for reproduction without permission
66
Drive engagement by using decision errors to help people ($≠$≠$)
Loewenstein, G., Brennan, T. and Volpp, K. (2007). Protecting People from Themselves: Using Decision Errors to Help People Improve Their Health. JAMA. 298(20), 2415-2417; Volpp, Pauly, Loewenstein, Bangsberg, (2009) Pay for Performance for Patients. Health Affairs 28(1): 206-14
Funding from Veterans Administration, CDC, Commonwealth of PA, NIMH, NIAAA,
Doris Duke Foundation

Kevin Volpp, MD, PhD – not for reproduction without permission
77
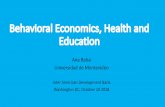
Tied payments are effective: Long-term smoking cessation rates triple in incentive group
Volpp, Troxel, Pauly, Asch, Galvin et al, New England Journal of Medicine. 2009; 360(7): 699-709.
p-value for difference <0.0001
Quit rates at 12 Months
• 878 Subjects from 85 General Electric worksites throughout US
• 2-arm Randomized controlled trial • Information about cessation programs • Information plus incentives worth $750
• Eligibility tied to quitting within first 6 months
• Quit rate ratio • 2.9 at 12 months (14.7% vs. 5.0%) • 2.6 at 18 months (9.4% vs. 3.6%)
• GE implemented nationwide plan in 2010 with 152,000 employees
Funding from CDC

Kevin Volpp, MD, PhD – not for reproduction without permission
88
Rates of non-adherence to warfarin significantly lower using daily lottery-based incentives
Volpp, Loewenstein, Doshi, Troxel, Kimmel, BMC Health Service Research 2008
Level of non- adherence under lotteries compared to historic controls
Percent incorrect
doses
• Warfarin: anti-stroke medication with large benefits but high non-adherence rates
• Designed lottery – 1 in 5 or 2 in 5 chance of
winning $10 a day– 1 in 100 chance of
winning $100 each day IF took warfarin previous day
Funding from NHLBI/NIH

9
Lotteries and deposit contracts both effective in achieving initial weight loss
Control Lottery Deposit contract
Volpp, KG, Troxel AB, Norton, Fassbender, Loewenstein JAMA 2008;300:2631-2637
Funding by NIA, NICHD, USDA, Hewlett Foundation
Mean weight loss by condition after 16 weeks Pounds
About 50% reached goal in intervention arms compared to 10% in control group

Kevin Volpp, MD, PhD – not for reproduction without permission
10
Competition between individuals can augment individual motivation to increase weight loss
Mean weight loss
pounds
Kullgren J, Troxel AB, Loewenstein G, Norton L, Volpp KG. 2013 Annals of Internal medicine
Funding by National Institute of Aging
Mean Cumulative Weight Change by Month during 24-Week Intervention
Period

Kevin Volpp, MD, PhD – not for reproduction without permission
1111
Social incentives an important alternative . . .
6 month Randomized Control Trial study
•Control – usual care
•Peer mentor – talk at least weekly
•Incentives - $100 to drop one point; $200 to drop two points or achieve HbA1c of 6.5%
Long JA, Jahnle E, Loewenstein G, Richardson D, Volpp KG. Annals of Internal Medicine. 2012.
Mean change in HbA1c
Funding by National Institute of Aging

Kevin Volpp, MD, PhD – not for reproduction without permission
1212
Hovering is a key ingredient for population-based financing (ACOs, medical homes) to succeed. . .
Typical Americans may spend 1-2 hours a year with a doctor
They spend their remaining 5,000+ waking hours elsewhere
Physicians don’t know much about what patients are doing during these 5,000 hours – nor do they have effective tools to affect their behavior (e.g. medication adherence, obesity)
Proliferation of wireless technologies and advance in understanding of behavioral economics create new opportunities to improve population health
Health engagement requires a substantial amount of “hovering.”
Asch DA, Muller R, Volpp KG. 2012. NEJM
Funding by National Institute of Aging, VA HSR&D

Kevin Volpp, MD, PhD – not for reproduction without permission
1313
Applying behavioral economics increases engagement with wireless devices and applications
Participant “passively” takes medication, uses scale, pedometer etc.
Device automatically transmits information to server
Program captures behavior and calculates incentive. Transmits communication to participant
Funds electronically transferred to participant
Data CaptureData Capture Data Transmission
Data Transmission
Rewards Communication
Rewards Communication
Funds Fulfillment
Funds Fulfillment
Funded by National Institute of Aging RC2 AG036592-01 (Asch and Volpp PIs)

Kevin Volpp, MD, PhD – not for reproduction without permission
1414
Regret contest incentives are effective at improving daily device use and improving glycemic control
Sen A, Sewell T, Bellamy S et al 2013 under review
Mean change in HbA1c
3 months
Monthly Adherence Rate
Funded by National Institute of Aging

Kevin Volpp, MD, PhD – not for reproduction without permission
1515
Automated hovering solutions being tested. . .
• Smoking cessation (CVS Caremark employees) – NCI/NIH
• Obesity - Group incentives, deposit contracts, premium adjustments vs. lotteries (CHOP, Horizon, UPHS employees) – NIA/NIH, Horizon, Mckinsey, UPHS
• Potential medical home 2.0 initiatives:– Glycemic control through remote monitoring (UPHS) – NIA/NIH– Peer mentoring (UPHS diabetic patients) – NIDDK/NIH– CPAP use (UPHS, Lankenau) – NIA/NIH
• Medication adherence
– Patient vs. Provider incentives for high-risk cardiac patients (UPHS, Geisinger, Harvard Vanguard Medical Associates) – NIA/NIH
– Automated hovering post-AMI (UPHS, Aetna, Horizon BCBS, Independence BCBS, Keystone Mercy, HealthFirst, CVS-C) – CMMI/CMS
– Habit formation for medication adherence (CVS Caremark) – NIA/NIH
– Social incentives (CVS Caremark) – CMMI/CMS

Kevin Volpp, MD, PhD – not for reproduction without permission
1616
RC4 – Bring behavioral economics into Physician P4P (Volpp, Asch, Stewart, Loewenstein, Rosenthal, Sequist)
–New study at Penn/Geisinger/HVMA:• Target patients with very high risk of cardiovascular disease (>20% over next 10 years) or known CAD and who have LDL>120 or moderately high risk and LDL>140 and no contraindications for statins
• 1st study to test provider vs. patient incentives
• Addresses several limitations to P4P– Reward improvement or attainment of single threshold– Align incentives for physicians and patients– Give providers feedback on patient daily adherence– Unbundled payments
Funded by National Institute of Aging RC4AG039114 (Asch/Volpp PIs)

Kevin Volpp, MD, PhD – not for reproduction without permission
1717
CMMI project: Automated hovering post-AMI(Volpp, Asch, Terwiesch, Troxel, Mehta)
Funded by CMMI/CMS

Kevin Volpp, MD, PhD – not for reproduction without permission
1818
New Model of Automated Hovering 1.0
Funded by CMMI/CMS

Kevin Volpp, MD, PhD – not for reproduction without permission
1919
Promising future directions. . .
• Employers, insurers, pharmacy benefit managers, consumer product companies are starting to use behavioral insights to improve program effectiveness
• Behavioral economics can help improve efficiency of resources already being spent on incentives
• Population-based financing will help bring about significant opportunities for improvement in quality and cost of chronic care management using technology and social science engagement strategies

Kevin Volpp, MD, PhD – not for reproduction without permission
2020
Questions?
Email: [email protected]
Research: chibe.upenn.edu