Basics of arthroscopy ppt
120
GOOD MORNING
-
Upload
vishwanath-bhagavati -
Category
Health & Medicine
-
view
614 -
download
126
Transcript of Basics of arthroscopy ppt

GOOD MORNING

J.J.M. MEDICAL COLLEGE DAVANGERE
MODERATORS:DR. RAMESH R.PROFESSOR AND UNIT CHIEF
DR. MALLIKARJUN REDDYPROFESSOR
SEMINAR ON BASICS OF ARTHROSCOPY

CHANGE :the golden rule of life So the same here
rom invasive to less invasive……

MEANING OF ARTHROSCOPY
This word arthroscopy came from GREEK ,
"arthro" (joint) And "skopein" (to look).
The term literally means "TO LOOK WITHIN THE JOINT Simply as if you see a room through a key – hole instead of opening doors. ….

Basic instruments and Equipments Care and sterilization of instruments Irrigation system Tourniquet Leg holders Anesthesia Advantages and Disadvantages Indications and contraindications Basic Arthroscopic techniques Complications Knee arthroscopy Shoulder arthroscopy Ankle arthroscopy Hip arthroscopy

BASIC INSTRUMENTATION KIT
Arthroscope : 30 degree 70 degreeFibreoptic cableslight sourcesAccessory instrumentsTelevision camerasProbeScissorsBasket forcepsGrasping forcepsKnife bladesMotorized shaving systemselectrosurgical lasers & radio surgical instruments

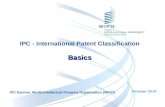
ARTHROSCOPY : EQUIPMENTS ASSEMBLY
Arthroscopecamera
Fibreoptic cable
light source
T. V. monitor
POWER
irrigation fluid bags
y connector

MONITOR It is the device
that projects the image created by the arthroscope and the camera head.

CAMERA HEADS
The camera head is the “brains” of the arthroscopic equipment.
This is a device that attaches to the arthroscope itself and is responsible for producing the image on the screen.
Inside the camera head there are small computer chips that capture the actual image into a digital image.
Cameras are sterilized usingethylene oxide gas or hydrogen peroxide gas

Camera head
arthroscope

LIGHT SOURCE WITH FIBRE OPTIC CABLES
All endoscopes utilize a light source to illuminate the inside of the joint during the procedure.
The light source consists of a box that houses the bulb (usually xenon or LED) that connects to the arthroscope via a sterile fiberoptic light cable.
The light cables should always be gas
sterilized and carefully coiled loosely to avoid breaking

Camera head
Light source
arthroscope

INSTRUMENTS AND EQUIPMENT

ARTHROSCOPE
An arthroscope is an optical instrument. Three basic optical systems have been used in rigid arthroscopes:
(1) the classic thin lens system, (2) the rod-lens system, and (3) the graded index (GRIN) lens system.


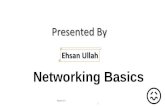
Certain features determine the optical characteristics of an arthroscope. Most important are the diameter, angle of inclination, and field of view.
The angle of inclination, which is the angle between the axis of the arthroscope and a line perpendicular to the surface of the lens, varies from 0 to 120 degrees.
Angle ofinclination

The 25- and 30-degree arthroscopes are most com monly used. The 70- and 90-degree arthroscopes are useful in seeing around corners, such as the posterior compartments of the knee

Field of view refers to the viewing angle encompassed by the lens and varies according to the type of arthroscope.
The 1.9-mm scope has a 65-degree field of view; the 2.7-mm scope, a 90-degree field of view; and the 4.0-mm scope, a 115-degree field of view.
Wider viewing angles make orientation by the observer much easier.

0 °Straight view not recommended
30 ° Increase the field of vision (90 )
Viewing angle

70 °For viewing special regions



ACCESSORY INSTRUMENTS The basic instrument kit consists of the
following: arthro scopes (30- and 70-degree); probe; scissors; basket forceps; grasping forceps; arthroscopic knives; motorized meniscus cutter and shaver; electrosurgical, laser, and radiofrequency instruments; and miscellaneous equipment.
These instruments are used in performing most routine arthroscopic surgical procedures.
Additional instruments are available and are occasionally used in special circumstances.

PROBE
The probe has become known over the years as “the extension of the arthroscopist’s finger.

The probe is essential for palpating intraarticular structures and in planning the approach to a surgical procedure.
The probe can be used to feel the consistency of a structure, such as the articular cartilage; to determine the depth of chondro malacic areas; to identify and palpate loose structures within the joint, such as tears of the menisci; to maneuver loose bodies into more accessible grasping positions; to palpate the anterior cruciate ligament and determine the tension in the ligamentous and synovial structures within the joint; to retract structures within the joint for exposure; to elevate a meniscus so that its undersurface can be viewed; and to probe the fossae and recesses

Most probes are right angled with a tip size of 3 to 4 mm, and this known size of the hook can be used to measure the size of intraarticular lesions.

SCISSORS Arthroscopic scissors are 3 to 4 mm in
diameter and are available in both small and large sizes. The jaws of the scissors may be straight or hooked . The hooked scissors are preferred because the configuration of the jaws tends to hook the tissue and pull it between the cutting edges of the scissors.

BASKET FORCEPS The standard basket forceps has
an open base that permits each punch or bite of tissue to drop free within the joint.
It is useful in trimming the peripheral rim of the meniscus, or it can be used instead of scissors to cut across meniscal or other tissue.
Configuration- straight or hooked Available in angles of 30, 45 and
90 degree. 15 degree up biting and down
biting curves are available.
Biting end
Open base

GRASPING FORCEPS Grasping forceps are
useful to retrieve material from the joint, such as loose bodies or synovium, or to place meniscal flaps and other tissues under tension while cutting with a second instrument.
The jaws of the grasping forceps may be of single- or double-action design and may have regular serrated interdigitating teeth.
Single action
Double action

KNIFE BLADES A variety of disposable blade
designs are available: hooked or retrograde blades; regular down-cutting blades, both straight and curved; and Smillie-type end-cutting blades.
These blades should be inserted through cannula sheaths or encased within a retractable sheath mechanism so that the cutting portion of the blade is exposed only when it enters the field of arthroscopic vision.


MOTORIZED SHAVING SYSTEMS Consists of an outer, hollow sheath and an
inner, hollow rotating cannula with corresponding windows .
The window of the inner sheath functions as a two-edged, cylindrical blade that spins within the outer hollow tube.
Suction through the cylinder brings the fragments of soft tissue into the window, and as the blade rotates, the fragments are amputated, sucked to the outside, and collected in a suction trap.

Uses : Designed for meniscal cutting or trimming,
for synovial resection, and for shaving of articular cartilage.

ELECTROSURGICAL, LASER, AND RADIOFREQUENCY INSTRUMENTS
Electrocautery has been used as an arthroscopic tool for cutting and hemostasis most often after arthroscopic synovectomy and subacromial decompression.
It also has been used for both cutting and hemostasis in lateral retinacular release for malalignment of the patella.
Reported complications of radiofrequency meniscal ablation include articular cartilage damage, osteonecrosis, and tissue damage caused by the irrigant.

IMPLANTS Suture anchors Meniscal repair devices Devices for tendon and ligament fixation and articular cartilage
repair.
Suture anchors


MISCELLANEOUS EQUIPMENT
Sheath
Blunt trocar
Sharp Trocar

CARE AND STERILIZATION OF INSTRUMENTS
Arthroscopy equipment that is heat stable may be autoclaved for sterility.
Heat- or moisture-sensitive equipment may be sterilized with a low-temperature hydrogen peroxide gas plasma.

IRRIGATION SYSTEMS

Irrigation and distention of the joint are essential to all arthroscopic procedures. Joint distention is maintained by lactated Ringer solution during arthroscopy.
It is physiologi cal and results in minimal synovial and articular surface changes.
Usually, two 5-L plastic bags of lactated Ringer solution, interconnected with a Y-connector.
The bag usually is placed 3 to 4 feet above the level of the joint, thus producing approximately 66 to 88 mm Hg of pressure.
Addition of epinephrine (1 mg per liter of saline) significantly increases visibility.

DISTENTION PRESSURE For knee 60-80 mmHg
For shoulder 30 mmHg less than systolic blood pressure.
For elbow and ankle 40-60 mmHg

TOURNIQUET During arthroscopic procedures of the knee, ankle,
elbow, and other distal joints, a tourniquet is almost always applied and is inflated as needed.
Advantages : 1) Increased visibility
Disadvantages : 1) Blanching of the synovium, which makes
differentiation and diagnosis of various synovial disorders difficult, and
2) The possibility of ischemic damage to muscle and nervous tissue with prolonged tourniquet time of more than 90 to 120 minutes.

Contraindications : Thrombophlebitis and signifi cant peripheral
vascular disease

LEG HOLDERS
The biggest advantage of a leg holder is that it permits application of stress primarily to open the posteromedial compartment for better viewing, manipulation of the meniscus, and posterior horn meniscal surgery, especially in tight knees.

The lateral aspect of the distal thigh can be levered against this post for opening of the posteromedial compart ment.
The post does not confine or prevent the knee from being positioned in an almost unlimited number of positions, including flexion and the figure-four position; it therefore has advantages over many of the expensive commercial leg-holding devices.
If a patellofemoral joint or a lateral compartment problem is anticipated, a valgus stress post may be chosen to make viewing of these compartments easier. For endoscopic repair of the anterior cruciate ligament, a lateral post should be used or the end of the table should be flexed to allow full unobstructed knee flexion.

ANESTHESIA Diagnostic arthroscopy can be performed with
the patient under local, regional, or general anesthesia.
Local anesthesia can be used for many arthroscopic procedures around the knee and ankle in a cooperative patient with intravenous sedation .
Chondrotoxicity is known to occur with lidocaine and epinephrine.
Combined spinal and epidural is best for knee and ankle.

ADVANTAGES Reduced postoperative morbidity Smaller incisions Less intense inflammatory response Improved visualization Absence of secondary effects Reduced hospital stay Reduced complication rate Improved follow-up evaluation Possibility of performing surgical procedures
that are difficult or impossible to perform through open arthrotomy

DISADVANTAGES Working through small portals with delicate
and fragile instruments. Maneuvering the instruments within the tight
confines of the intraarticular space may produce significant scuffing and scoring of the articular surfaces.
Requires experienced surgeon Time consuming Requires special instruments Expensive

CONTRAINDICATIONS
When the risk of joint sepsis from a local skin condition is present or when a remote infection may be seeded in the operative site
RELATIVE CONTRAINDICATIONS
Partial or complete ankylosis around the joint
Major collateral ligamentous and capsular disruptions of the joint

TRIANGULATION TECHNIQUE

Triangulation involves the use of one or more instruments inserted through separate portals and brought into the optical field of the arthroscope, the tip of the instrument and the arthroscope forming the apex of a triangle.
Separation of the instruments from the arthroscope improves depth perception and, perhaps the most significant advantage, permits independent movement of the arthro scope and the surgical instrument, which is essential for operative arthroscopy.

COMPLICATIONS
Damage to Intraarticular structures
Damage to Menisci and Fat pad
Damage to Cruciate ligaments

DAMAGE TO INTRAARTICULAR STRUCTURES Most common complication of knee arthroscopy Damage to the articular cartilage surfaces by the tip
of the arthroscope or the operating instrument is the most common complication.
It leads to progressive chondromalacic changes and degenerative arthritis.
Prevention :
The joint should be opened with leverage or traction first and the arthroscope allowed to slide into the space created.
Use of a leg holder or a leverage post during knee surgery, as well as traction or distraction devices during shoulder, hip, and ankle procedures, is helpful.

DAMAGE TO MENISCI AND FAT PAD
The anterior horn of either meniscus of the knee can be damaged by incision or penetration if the anterior portals are located too inferiorly.
Repeated penetration of the fat pad causes swelling of the pad and obstruction of view and may also result in hemorrhage, hypertrophy, or fibrosis of that structure.

DAMAGE TO CRUCIATE LIGAMENTS
Occurs during meniscal excision when an intercondylar attachment is cut.
When motorized instruments are débriding the inter condylar notch.

DAMAGE TO EXTRAARTICULAR STRUCTURES

BLOOD VESSELS CAUSES Direct penetration or laceration From pressure caused by excessive fluid
extravasation.
Popliteal artery is at risk during meniscectomy when intercondylar attachments are cut, especially when arthroscopic knives are used.
Both the popliteal artery and vein have been damaged during meniscal repairs as the sutures are placed posteriorly.
Extensive arthroscopic synovectomies have been associated with injury to the genicular arteries.

ANKLE Anterior tibial artery is at risk during anterior
approaches for ankle arthroscopy, especially with the antero central approach.
ELBOW Brachial artery may be damaged during
establishment of either the anteromedial or anterolateral portal.
Fluid extravasation also may compress this vessel in the antecubital fossa.

SHOULDER The axillary artery may be injured by an
arthroscopic instrument plunging through the axillary pouch.
More often, axillary vessel occlusion is caused by fluid extravasation or excessive arm traction

COMPARTMENT SYNDROMES CAUSE From fluid extravasations
PREVENTION By using gravity inflow or lower pump
pressures and ensuring adequate outflow, most of these complications can be avoided.

NERVES CAUSES
Direct trauma from a scalpel or sharp trocar By traction from overdistraction By mechanical compression or compression
from fluid extravasation By prolonged ischemia from excessive
tourniquet use By a poorly defined mechanism of injury to
the anatomical nervous system that results in reflex sympathetic dystrophy

PREVENTION By marking portals appropriately Making sure the scalpel penetrates the skin
only Using a hemostat to spread down to the joint
capsule in proximity to a nerve Routinely using blunt trocars. Maintaining proper joint distention and
distraction Padding nerve and bony prominences, and Proper patient positioning

Saphenous nerve or sartorial branches of the femoral nerve are injured in knee arthroscopy.
Axillary nerve in shoulder arthroscopy.
Traction neurapraxia of the brachial plexus may occur when strong traction and distraction of the shoulder have been used.
Neurovascular injury is the major risk of elbow arthroscopy:
Anterior portals place the radial and posterior interosseous nerves at risk on the lateral side and the median nerve at risk on the medial side
Posteromedial portals place the ulnar nerve at risk.

LIGAMENTS AND TENDONS The medial collateral ligament may be
injured by accessory medial portals around the knee, or it may be torn by severe valgus stress in an attempt to open up the medial compartment.

OTHER COMPLICATIONS HEMARTHROSIS The superior lateral geniculate vessels
usually are cut in lateral retinacular releases, and the inferior lateral geniculate vessels may be lacerated just anterior to the popliteal hiatus during lateral meniscectomy and synovectomy.

THROMBOPHLEBITIS Incidence varies No specific risk factors are found for DVT Probable risk factors include Age > 50 years Tourniquet time > 60 minutes
PREVENTION : By using LMW heparin 12 hours prior to surgery and
continuing 48 hours postoperatively

INFECTION RISK FACTORS The use of intraarticular corticosteroids Prolonged tourniquet time Patient age of more than 50 years Failure to prepare the surgical site again
before conversion to arthrotomy Procedure complexity And history of previous procedures and noted
that several reported outbreaks of infection after arthroscopy were related to breaks in infection control or to contaminated instruments.

ANTIBIOTIC PROPHYLAXIS
1 g cefazolin intravenously within 1 hour of the skin incision.
Patients older than age 80 years are given 2 g.

TOURNIQUET PARESIS
Temporary paresis in the extremity occurs if tourniquet is used more than 90-120 minutes.
Carefully monitoring the tourniquet pressure and testing the accuracy of the tourniquet gauges minimize these problems.

SYNOVIAL HERNIATION AND FISTULAS
Small globules of fat and synovial tissue may herniate through any of the arthroscopic portals. Usually, the larger the portal, the greater the chance of this complication.
No specific treatment is required. If it persists then excision is required.
Fistulas more commonly are associated with posteromedial knee and ankle portals.
To improve closure, these portals should be sutured.
Patient should receive antibiotics, and the knee should be immobilized for 7 to 10 days.

INSTRUMENT BREAKAGE
0.03% incidence If an instrument breaks, the surgeon should
immediately close the outflow cannula but the inflow should be left open to keep the joint distended.
If the broken instrument is in the visual field, total attention to keeping it in view and removing it is essential.
If the broken piece is located, a suction apparatus or a magnet may be introduced through an accessory portal to stabilize and remove the small broken fragment.

KNEE In general, knee arthroscopy is performed for diagnosing and treating a
variety of knee problems. The common indications are: 1. Meniscal tears 2. ACL tears 3. PCL tears 4. Removal of loose bodies 5. Synovectomy (removal of diseased synovial tissue) in cases of: a. Rheumatoid arthritis b. Infections (pyogenic arthritis, tuberculous arthritis) c. Pigmented villonodular synovitis d. Synovial chondromatosis (multiple loose bodies) 6. Joint debridement & washout for osteoarthritis 7. Articular cartilage injuries and defects requiring: a. Abrasion arthroplasty b. Mosaicplasty c. Autologous cartilage implantation (ACI) 8. Lateral retinacular release for patellar maltracking 9. Patellar clunk syndrome following total knee replacement 10. Evaluating knee joint prior to doing Unicompartmental knee replacement
(UKR) or High tibial osteotomy (HTO) 11. Arthroscopic assisted fixation of tibial plateau fractures

PATIENT POSITIONING

STANDARD PORTALS


Anteromedial Anterolateral Posteromedial Superolateral

ANTEROLATERAL Almost all structures clearly visualised except
PCL Anterior portion of lateral meniscus Periphery of posterior horn of medial meniscus
1cm above lateral joint line 1cm lateral to patellar tendon 1cm below patella

The trochar and sleeve are inserted at 70° of knee flexion.
Firm, gradual pressure applied until there is a reduction in resistance, indicating that the trochar has passed through the joint capsule.
knee is extended to around 20° of flexion and the trochar advanced, passing through the patellofemoral joint.
Its intra-articular position can be confirmed by sweeping the arthroscope gently from side to side – it can be felt to be beneath the patella.
If it is outside the knee joint, it will not sweep from side to side.
position of the arthroscope should be confirmed before removing the trochar, introducing the camera and turning on the saline inflow


PRECAUTIONS Portal too near the joint line-
the ant. horn of the lateral meniscus can be lacerated
difficulty in maneuvering the scope. Too superior to the joint line-
prevents viewing of the posterior horns of the menisci and other posterior structures.
Immediately adjacent to the edge of the patellar tendon can penetrate the fat pad, difficulty in viewing
and in maneuvering the scope within the joint.

ANTEROMEDIAL This portal is located similarly to the
anterolateral portal: 1 cm above the medial joint line, 1 cm inferior to the tip of the patella, and 1 cm medial to the edge of the patellar tendon.
For additional visualisation of lateral compartment and to probe lateral and medial compartment structures.
Needle inserted such that it exits just above medial meniscus

POSTEROMEDIAL 1cm above PM joint line in line with
lateral border of medial femoral condyle ‘soft spot’ between the tendon of
semimembranosus, the medial head of gastrocnemius and the medial collateral ligament.
Before distention of the joint, this small triangle can be palpated easily with the knee flexed to 90 degrees.
The knee must be maximally distended with irrigating solution so that the posteromedial compartment balloons out like a bubble when the knee is flexed to 90 degrees (saphaneous nerve)

For repair or removal of displaced posterior horn meniscal tears and for removal of posterior loose bodies that cannot be displaced into the medial compartment and removed through an anterior portal.
For total synovectomy.

SUPEROLATERAL Most useful for viewing the
dynamics of the patellofemoral articulation.
Lateral to the quadriceps tendon and about 2.5 cm superior to the SL corner of the patella.
Evaluation of patella tracking, patellar congruity, and lateral overhang of the patella and for suprapatellar synovectomy.

OPTIONAL PORTALS Posterolateral Portal
Proximal Midpatellar Medial and Lateral Portals
Accessory Far Medial and Lateral Portals
Central Transpatellar Tendon (Gillquist) Portal

ARTHROSCOPIC EXAMINATION OF THE KNEE
A methodical sequence of examination should be developed, progressing from one compartment to another and systematically carrying out this sequence in every knee.
The knee should be divided routinely into the following compartments for arthroscopic examination
1. Suprapatellar pouch and patellofemoral joint 2. Medial gutter 3. Medial compartment 4. Intercondylar notch 5. Posteromedial compartment 6. Lateral compartment 7. Lateral gutter and posterolateral compartment



SHOULDER Indications for shoulder arthroscopy
1. Shoulder instability (recurrent dislocation of shoulder) 2. Impingement syndrome (pain on lifting the arm) 3. Rotator cuff tears 4. Calcific tendonitis tendinitis (calcium deposition in the
rotator cuff) 5. SLAP tears 6. Tears of long head of biceps tendon 7. Frozen shoulder (periarthritis) 8. Removal of loose bodies 9. Synovectomy for: a. Inflammatory conditions like RA b. Infections (like TB) c. Synovial chondromatosis

PATIENT POSITIONING

Lateral decubitus position

PORTALS

Before making arthroscopic portals, a thorough understanding of the local anatomy is necessary to prevent damage to neurovascular structures

POSTERIOR PORTAL Primary entry portal for
shoulder arthroscopy. It allows examination of
most of the joint and assists in the placement of subsequent portals .
This portal is located 1.5 to 3.0 cm inferior and 1.0 cm medial to the posterolateral tip of the acromion.
Between the infraspinatus and teres minor muscles.

POSTEROINFERIOR 7-O’CLOCK PORTAL

ANTERIOR PORTAL Observation of the
posterior capsule and the rotator cuff and for an anterior view of the glenohumeral ligaments and the subscapularis tendon.
Anterior portal is made slightly lateral to a point halfway between the anterolateral tip of the acromion and the coracoid process.

ANTEROINFERIOR 5-O’CLOCK PORTAL Along the leading edge
of the inferior glenohumeral ligament at the 5-o’clock position along the glenoid rim.
The portal travels through the subscapularis and lateral to the conjoined tendon.
Allows appropriate access to the leading edge of the inferior glenohumeral ligament.

SUPERIOR PORTAL This portal penetrates
the trapezius muscle and passes through the supraspinatus muscle belly.
The suprascapular nerve and artery lie approximately 3 cm medial to the superior portal at its closest point
Useful for passage of suture retrieval devices for rotator cuff repair.

LATERAL PORTAL The lateral portal
is the primary operative portal for the subacromial space. It is located 3 cm lateral to the lateral border of the acromion and passes through the deltoid muscle.

PORTAL OF WILMINGTON Providing access to the
glenoid and superior labrum.
The location is 1 cm anterior and 1 cm lateral to the posterior acromial angle.

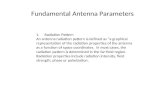
DIAGNOSTIC ARTHROSCOPY
Superior part of shoulder joint with biceps tendon inserting into superior labrum. Humeral head is superior right, and glenoid is inferior.

Superior glenohumeral ligament and subscapularis tendon on right with middle glenohumeral ligament inferiorly

Normal sublabral hole

Buford complex showing insertion of middle glenohumeral ligament directly into biceps anchor

Middle cord variant of glenohumeral ligament crossing subscapularis tendon.

Inferior pouch. Glenohumeral ligaments and labrum are seen

Capsular attachment to humeral head observed through inferior pouch.

Rotator cuff evaluated for fraying, partial tears, or calcification. Supraspinatus tendon is seen superiorly with biceps tendon in center of picture.

Posterior articular surface, posterior labrum, posterior pouch, and posterior capsule observed with arthroscope inserted anteriorly.

Posterior band of inferior glenohumeral ligament

Anterior band of inferior glenohumeral ligament observed from anterior portal. Humeral insertion of ligament is superior.

Capsulolabral attachment to glenoid observed through anterior portal

View of subacromial space with cuff below and acromion above

DIAGNOSTIC SHOULDER ARTHROSCOPY VIDEO

ANKLE Indications for diagnostic ankle arthroscopy include the following:
Unexplained pain, swelling, stiffness, instability Locking and popping
Indications for therapeutic ankle arthroscopy include the following: Articular injury Soft-tissue injury Posttraumatic soft-tissue impingement Bony impingement Arthrofibrosis Instability Arthroscopic-assisted fracture fixation Synovitis Loose bodies Intra-articular bands Tendinitis Osteophytes Osteochondral defects Arthrodesis Septic arthritis

PATIENT POSITIONING

PORTALS

HIP One of the most common indications for hip
arthroscopy is Management of femoroacetabular
impingement (FAI) and associated labral tears.
Loose bodies Chondral pathology Degenerative joint disease Avascular necrosis (AVN) Synovial disease Instability Internal and external snapping hip Joint sepsis

PORTALS
Anterior portal
Anterolateral portal
Lateral portal
1 cm superior and anterior to the anterior edge of the greater trochanter.
1 cm posterior and superior to the greater trochanter.
intersection of a line drawn from the tip of the greater trochanter and a line extending inferiorly from the anterior superior iliac spine.