Basics in gyne laparoscopy
46
Basic Principles in Basic Principles in Gyne- Laparoscopy Gyne- Laparoscopy DR.C.SURESH BABU DR.C.SURESH BABU PROFESSOR PROFESSOR DEPT.OF OBGYN DEPT.OF OBGYN College of Medicine, Abha, KKU, KSA College of Medicine, Abha, KKU, KSA
-
Upload
chaduvula-sureshbabu -
Category
Documents
-
view
232 -
download
3
Transcript of Basics in gyne laparoscopy

Basic Principles in Basic Principles in Gyne- LaparoscopyGyne- Laparoscopy
DR.C.SURESH BABUDR.C.SURESH BABUPROFESSORPROFESSOR
DEPT.OF OBGYNDEPT.OF OBGYNCollege of Medicine, Abha, KKU, KSACollege of Medicine, Abha, KKU, KSA

INTRODUCTIONINTRODUCTION KALK(1930) – FATHER OF INTERNALKALK(1930) – FATHER OF INTERNAL LAPAROSCOPYLAPAROSCOPY HOPE(1937) – FIRST GYNEACOLOGICAL HOPE(1937) – FIRST GYNEACOLOGICAL
REPORT ON ECTOPIC PREGNANCYREPORT ON ECTOPIC PREGNANCY BOESCH (1936)- COAGULATION BOESCH (1936)- COAGULATION PALMER (1943) –COLD LIGHT ENDOSCOPE.PALMER (1943) –COLD LIGHT ENDOSCOPE. FRANGENHEIM (1952)– CO2 INSUFFLATIONFRANGENHEIM (1952)– CO2 INSUFFLATION JORDEN PHILIPS – SPREAD OF JORDEN PHILIPS – SPREAD OF
LAPAROSCOPE THROUGHOUT THE WORLDLAPAROSCOPE THROUGHOUT THE WORLD SEMM (1970)-LAPAROSCOPIC SEMM (1970)-LAPAROSCOPIC
HYSTERECTOMYHYSTERECTOMY

BASIC PREREQUISITESBASIC PREREQUISITES
GOOD KNOWLEDGE ABOUT GOOD KNOWLEDGE ABOUT SURGICAL ANATOMYSURGICAL ANATOMY
GOOD AT CONVENTIONAL GOOD AT CONVENTIONAL SURGERIESSURGERIES
REASONABLE TRAININGREASONABLE TRAINING
GOOD EXPERIENCEGOOD EXPERIENCE

ANATOMYANATOMY

LAPAROSCOPY SET UPLAPAROSCOPY SET UP
BASIC REQUIREMENTS:BASIC REQUIREMENTS:
1.TWO ASSISTANTS1.TWO ASSISTANTS
2.WELL TRAINED SISTER2.WELL TRAINED SISTER
3.OT TECHNICIAN3.OT TECHNICIAN
4. ALL LAPAROSCOPIC 4. ALL LAPAROSCOPIC INSTRUMENTSINSTRUMENTS
5.TWO MONITORS5.TWO MONITORS
6.CO-OPERATIVE ANAESTHETIST6.CO-OPERATIVE ANAESTHETIST

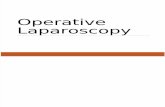
Verres NeedleVerres Needle

Gas InsufflatorGas Insufflator

INSTRUMENTSINSTRUMENTS

Trocar & CannulaTrocar & Cannula

CameraCamera

LaparoscopeLaparoscope

Xenon Light SourceXenon Light Source

Uterine ElevatorUterine Elevator

EquipmentsEquipments
Laparoscopic Tools
Video monitor

1. Bipolar grasper
2. Atraumatic grasper
3. Grasping forceps
4. Toothed forceps
5. Sharp-tipped monopolar device
6. 5-10mm suction-irrigation device
7. Scissors

Patient PositioningPatient Positioning
Low lithotomy position
30 degree Trendelenburg
Urinary catheter
NG tube (?)
Uterine cannulation

Trocar Placement for Trocar Placement for SurgerySurgery
A) 12mm optical trocar placed at umbilical level
B) and C) 5mm lateral operative trocars placed 3 fingerbreadths above the symphysis pubis

Peritoneum is inflated with CO2
Needle inserted at the umbilical level (primarily used) OR at Palmer’s point (3cm below costal margin in midclavicular line)
Pressure should not exceed 14 mmHg- respiratory compromise

OT SET UPOT SET UP

INDICATIONS FOR INDICATIONS FOR LAPAROSCOPYLAPAROSCOPY
Diagnostic:Diagnostic: 1] Infertility1] Infertility 2] Suspected Ectopic pregnancy2] Suspected Ectopic pregnancy 3] Misplaced Copper T3] Misplaced Copper T 4] Chronic pelvic pain etc.,4] Chronic pelvic pain etc., Therapeutic:Therapeutic: 1] Myomectomy1] Myomectomy 2] LAVH, TALH2] LAVH, TALH

Therapeutic IndicationsTherapeutic Indications
3] Ovarian Drilling in PCOD3] Ovarian Drilling in PCOD 4] Ovarian Cystectomy4] Ovarian Cystectomy 5] Retrieval of misplaced copper T5] Retrieval of misplaced copper T 6] Cauterisation of Emdometriotic 6] Cauterisation of Emdometriotic
spotsspots 7] Radical Hysterectomy for cancer 7] Radical Hysterectomy for cancer
cervix etc.,cervix etc.,

LAPAROSCOPYLAPAROSCOPY General AnesthesiaGeneral Anesthesia
Trendlenberg’s positionTrendlenberg’s position
Lights should be offLights should be off
Well trained staffWell trained staff
Electrical technical assistantElectrical technical assistant


Anatomical ReviewAnatomical Review
1. Medial tubal A.
2. Lateral tubal A.
3. Uterine A.
4. Ovarian A.

Laparoscopic Laparoscopic SalpingectomySalpingectomy
Main Risk:Main Risk: devascularization of the ovary devascularization of the ovary Operate close to the tube, away from Operate close to the tube, away from
ovarian vessels and suspensory ligamentovarian vessels and suspensory ligament

1.1. Proximal tube divisionProximal tube division Isthmus is held upwards and Isthmus is held upwards and
outwardsoutwards Isthmus is cauterizedIsthmus is cauterized Take care not to cauterized the Take care not to cauterized the
internal ovarian A. and ovarian internal ovarian A. and ovarian branch of the uterine A.branch of the uterine A.
Divide tube with scissorsDivide tube with scissors

2.2. Mesosalpinx DivisionMesosalpinx Division Divide the mesosalpinx Divide the mesosalpinx
with scissorswith scissors
Cauterize and divide Cauterize and divide the infundibulo-ovarian the infundibulo-ovarian ligaments and the ligaments and the lateral tubal A. lateral tubal A.

3.3. Extraction of the tubeExtraction of the tube Remove tube through an Remove tube through an
extraction bagextraction bag Verification of hemostasisVerification of hemostasis Careful lavageCareful lavage Removal of equipmentRemoval of equipment Suture/ Steri-strip Suture/ Steri-strip
laparoscopic incisionslaparoscopic incisions
Caution:
• Endometriosis
• Utero-peritoneal fistula

Positive methyline blue test
Positive methyline blue test
Normal left adnxa
Normal left adnxa and Douglas pouch

Mild fimbrial adhesion Fimbria
Fine band of adhesion
FimbriaFine adhesion
Fimbria
Broad band of adhesion
Moderate adhesion
DouglasPouch

Severe Adhesions
Dr.Sherbiny

Hydrosalpin
x

Adhesiolysis of the left tube with micro- scissor
Uterus
L. Ovary
L. Tube

R .Ovary
R .tube
Cutting band of adhesion

Phimosis of the fimbrial end: Dilatation with Maryland forceps
Dr.Sherbiny
Phimosis with methyline Blue jet
Phimosis: delayed methyline blue spill
Free methyline blue spill
Dilatation with Maryland forceps

Classic bluish black endometriotic implants
Typical Endometriosis
Black Endometriosis Blue Endometriosis
Black Blue

Atypical Endometriosis
White Endometriosis
Peritoneal Defect
Red Endometriosis(Flam-like)Yellow Brown Endometriosis

Red Endometriosis (Pink)
Yellow Brown EndometriosisClear Endometriosis

Endometriotic Endometriotic CystCyst = =
Endometrioma Endometrioma

PCO

Laparoscopic ovarian drilling with Laparoscopic ovarian drilling with either diathermy or laser is an either diathermy or laser is an effective treatment for effective treatment for anovulation in women with anovulation in women with clomiphene-resistant PCOS. clomiphene-resistant PCOS.
PCOS: PCOS: Laparoscopic Laparoscopic DDrillingrilling
RCOG Guidelines : Grade A
58National Institute of Clinical Excellency (NICE) 2004

Tubal bipolar coagulation
Cutting of the medial part of the tube
Salpingostomy Salpingost
omyLaparoscopic tubal occlusion & salpingostomy of Hydrosalpinges prior to IVF to improve pregnancy rate

COMPLETE SPECIMENNCOMPLETE SPECIMENN

ADVANTAGES ADVANTAGES
QUICK RECOVERYQUICK RECOVERY EARLY ORAL FEEDINGEARLY ORAL FEEDING EARLY AMBULATIONSEARLY AMBULATIONS BLADDER DYSFUNCTION IS LESSBLADDER DYSFUNCTION IS LESS POSTOPERATIVE COMPLICATIONS POSTOPERATIVE COMPLICATIONS
ARE LESSARE LESS

COMPLICATIONSCOMPLICATIONS
1] Bowel injury1] Bowel injury 2] Vascular injury2] Vascular injury 3] Bladder injury 3] Bladder injury 4] Cautery burns to surrounding 4] Cautery burns to surrounding
organsorgans 5] Anesthesia complications5] Anesthesia complications 6] Surgical emphysema etc.,6] Surgical emphysema etc.,

THANK THANK YOUYOU