
ECG Rhythm Interpretation Module VII a Reading 12-Lead ECG’s.
Upload
jofandandrea-mendozaCategory
view
170download
2
BASIC ECG READINGElnah A. Gulliab, M.D.
Internal Medicine

Willem Einthoven receives Nobel Prize
The EKG is not only the oldest but, in fact, over 100 years after its introduction, continues as the most commonly used cardiovascular laboratory procedure.


What is an ECG?
Is a graphic recording of electric potentials generated by the heart.
Immediately available, non invasive, inexpensive and highly versatile test
It is use to detect arrythmias, conduction disturbances, myocardial ischemia, other related life threatening metabolic disturbances.

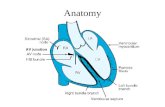
Normal Impulse Conduction
Sinoatrial node
AV node
Bundle of His
Bundle Branches
Purkinje fibers

Impulse conduction and ECG
Sinoatrial node
AV node
Bundle of His
Bundle Branches
Purkinje fibers

Limb Leads

Precordial Chest Leads

Precordial Leads

Anatomic Groups(Septum)

Anatomic Groups(Anterior Wall)

Anatomic Groups(Lateral Wall)

Anatomic Groups(Inferior Wall)

Anatomic Groups(Summary)

The ECG Paper
Horizontallybox - 0.04 One small sOne large box - 0.20 s
VerticallyOne large box - 0.5 mV

ECG paper
Every 3 seconds (15 large boxes) is marked by a vertical line.
This helps when calculating the heart rate.
3 sec
3 sec

ECG waveforms and Intervals
P wave - Atrial
depolarizationQRS - Ventricular depolarization
T wave - Ventricular repolarization

ECG waveforms and Intervals

ECG waveforms and Intervals
PR interval beginning of P wave to the beginning of the
next QRS Normally, < .2 seconds or one large box. If it is > .2 seconds, it is a first degree block

ECG waveforms and Intervals
QRS interval beginning of Q to the end of the S wave) should be < .12 seconds (< 3 small boxes) If QRS is > .12, check for bundle branch
block.

ECG waveforms and Intervals
QT interval beginning of QRS to end of T wave should be less than half of the preceding
RR interval - this varies with the rate For normal rates, QT < .4 seconds (2 large
boxes).

ECG Interpretation
Rate / Rhythm Axis Atrial Abnormality or Hypertrophy Heart Blocks Ischemia or Infarction Ventricular Hypertrophy Misc.
(Non specific ST wave changes,Persistent posterobasal forces)

I. RATE AND RHYTHM
Step 1: Calculate rate. Step 2: Determine regularity. Step 3: Assess the P waves. Step 4: Determine PR interval. Step 5: Determine QRS duration.

Step 1. Calculate Rate
Option 1OPTION # 1
Count the # of R waves in a 6 second rhythm strip, then multiply by 10.
INTERPRETATION?9 x 10 = 90 bpm
3 sec
3 sec

Step 1. Calculate Rate
Option 2 Find a R wave that lands on a bold line. Count the # of large boxes to the next R
wave. If the second R wave is 1 large box away the rate is 300, 2 boxes - 150, 3 boxes - 100, 4 boxes - 75, etc. (cont)
R wave

Step 1: Calculate Rate
Option 2 (cont) Memorize the sequence:
300 - 150 - 100 - 75 - 60 - 50
Interpretation? Approx. 1 box less than 100 = 95 bpm
300
150
100
75
60
50

Step 2: Determine Regularity
RR R R
Look at the R-R distances - using a caliper or markings on a pen or paperRegular (are they equidistant apart)?

Step 3: Assess the P waves
Look at the p waves:cycle length do not vary by 10%
rate is 60-100/minsame contour in same lead?
Upright in I, II, aVF & left precordial leads
followed by QRST?

Step 4: Determine PR interval
Normal: 0.12 - 0.20 seconds.
(3 - 5 boxes)
Interpretation? .12 seconds

Step 5: QRS duration
Normal: 0.04 - 0.12 seconds. (1 - 3 boxes)
Interpretation? 0.08 seconds

Rhythm / Rate Summary
Rate 90-95 bpm
Regularity regularP waves normalPR interval 0.12 sQRS duration 0.08 sInterpretation? Normal Sinus Rhythm

II. AXIS
Normal axis -30 to +90
Left axis deviation -30 to -90
Right axis deviation +90 to +/- 180
indeterminate -90 to +/- 180


What is the axis?

What is the axis?

III. ATRIAL ABNORMALITY/HYPERTROPHY
Right atrial hypertrophy Peaked P wave in lead II > 2.5mm amplitude. V1 has increase in the initial positive deflection.
Left atrial hypertrophy Notched wide (> 3mm) P wave in lead II. V1 has increase in the terminal negative deflection.

IV. BUNDLE BRANCH BLOCKS
Complete bundle branch block - QRS interval is >120ms in duration
Incomplete bundle branch blocks -QRS interval is between 100-120 ms in duration
May occur w/o structural abnormality (rbbb is more common than lbbb)
T wave is typically opposite in polarity to the last deflection of QRS

Right Bundle Branch Block
Terminal QRS vector is oriented to the right and anteriorly
Lead V1 = rSR ; Lead V6 = qRS

Left Bundle Branch Block
Major QRS vector is directed to the left and posteriorly
Lead V1 = wide QRS ; Lead V6 = positive R complex

What is your interpreatation?

V. ISCHEMIA / INFARCTION

ISCHEMIA

INFARCTION

VI. VENTRICULAR HYPERTROPHY
Left Ventricular Hypertrophy V1/V2 – S wave plus V5/V6 R wave =
>35mm (SV1 + RV5 or RV6)
AVL = > 12mm R wave

Right Ventricular Hypertrophy R wave is > S wave in V1 R wave decrease from V1 to V6

Common ECG abnormalities

Regularly occurring PQRSTRate < 60 / min
Sinus Bradycardia

Sinus Tachycardia
Regularly occurring PQRSTRate > 100 / min

Atrial Fibrillation
Irregular RR intervalNo discernible P waves

Premature Ventricular Contractions
Prematurely occurring complex.Wide, bizarre looking QRS complex.Usually no preceding P wave.T wave opposite in deflection to the QRS complex.Complete compensatory pause following every premature beat.

Ventricular Tachycardia
At least 3 consecutive PVC’s Rapid, bizarre, wide QRS complexes
(> 0.10 sec) No P wave (ventricular impulse origin)

Ventricular Fibrillation
Associated with coarse or fine chaotic
undulations of the ECG baseline No P wave No true QRS complexes Indeterminate rate

ECG reading exercise

What is your interpretation?

What is your interpretation?

What is your interpretation?

What is your interpretation?

What is your interpretation?

What is your interpretation?

What is your interpretation?

What is your interpretation?

What is your interpretation?

What is your interpretation?















![[Os 213] Ws 02 Ecg Reading](https://static.fdocuments.net/doc/165x107/563db931550346aa9a9af1b2/os-213-ws-02-ecg-reading.jpg)
