BASIC CONCEPTS IN TB - Home | Curry International ...nid... · Core Curriculum on Tuberculosis: ......
15
CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE May 26-28, 2015 Curry International Tuberculosis Center, UCSF 300 Frank H. Ogawa Plaza, Suite 520 Oakland, CA; Office (510) 238-5100 BASIC CONCEPTS IN TB OBJECTIVES Upon completion of this session, participants will be able to: 1. List three priority strategies that the Centers for Disease Control and Prevention recommends for public health agencies to implement in order to control and prevent tuberculosis 2. Identify several characteristics that distinguish active TB disease from latent TB infection (LTBI) 3. Appropriately apply the American Thoracic Society TB classifications INDEX OF MATERIALS PAGES 1. Basic concepts in TB-slide outline Presented by: April King-Todd, RN, BSN, MPH 1-9 SUPPLEMENTAL READING MATERIALS 1. CDC. Table 2.8: TB Classification System. In: Chapter 2: transmission and pathogenesis of tuberculosis. Core Curriculum on Tuberculosis: What the Clinician Should Know. Atlanta, GA: 2011:40 2. Resources on Tuberculosis 3. Acronyms and Abbreviations
Transcript of BASIC CONCEPTS IN TB - Home | Curry International ...nid... · Core Curriculum on Tuberculosis: ......
CASE MANAGEMENT AND CONTACT INVESTIGATION INTENSIVE May 26-28, 2015
Curry International Tuberculosis Center, UCSF
300 Frank H. Ogawa Plaza, Suite 520 Oakland, CA; Office (510) 238-5100
BASIC CONCEPTS IN TB
OBJECTIVES
Upon completion of this session, participants will be able to:
1. List three priority strategies that the Centers for Disease Control and Prevention recommends for public health agencies to implement in order to control and prevent tuberculosis
2. Identify several characteristics that distinguish active TB disease from latent TB infection (LTBI)
3. Appropriately apply the American Thoracic Society TB classifications
INDEX OF MATERIALS PAGES
1. Basic concepts in TB-slide outline Presented by: April King-Todd, RN, BSN, MPH
1-9
SUPPLEMENTAL READING MATERIALS
1. CDC. Table 2.8: TB Classification System. In: Chapter 2: transmission and pathogenesis of tuberculosis. Core Curriculum on Tuberculosis: What the Clinician Should Know. Atlanta, GA: 2011:40
2. Resources on Tuberculosis
3. Acronyms and Abbreviations

TB Case Management and Contact Investigation Intensive May 26-28, 2015 Curry International Tuberculosis Center
Basic Concepts in TB1
Basic Concepts in TB
Tuberculosis Case Management and Contact
Investigation Intensive May 26‐28, 2015
April King‐Todd, BSN, MPH
Nurse Manager
Los Angeles County TB Control Program
Basic Concepts in TB
TB Control Priorities in US
Pathogenesis
Transmission
Risk factors associated with transmission
TB vs LTBI
Drug resistant & MDR ‐TB
TB Classification system
1
Objectives
Upon completion of this session, participants will be able to:
1. List three priority strategies that the Centers for Disease Control and Prevention recommends for public health agencies to implement in order to control and prevent Tuberculosis
2. Identify several characteristics that distinguish active TB disease from latent TB infection (LTBI)
3. Appropriately apply the American Thoracic Society TB classifications

TB Case Management and Contact Investigation Intensive May 26-28, 2015 Curry International Tuberculosis Center
Basic Concepts in TB2
• Tuberculosis (TB) remains one of the world’s deadliest communicable diseases.
• In 2013, an estimated 9.0 million people developed TB and 1.5 million died from the disease,360 000 of whom were HIV-positive. TB
National Priorities for TB Control 2015‐2019
Priority 1:
• Identify & treat active cases
• Identify, evaluate & treat contacts
Priority 2:
• Evaluate & treat new immigrants & refugees with “Class B” TB notifications upon arrival to U.S.
Priority 3:
• Targeted testing and treatment of high‐risk populations
Source: Tuberculosis Elimination and Laboratory Cooperative Agreement, CDC‐RFA‐PS15‐1501 National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention
Introduction
Airborne disease caused by the bacterium Mycobacterium tuberculosis (M. tb)
M. tb complex (M. tb, M. bovis, M. africanum, M. microti,M. canetti, M. caprae, M. pinnipedii, and M. mungi) can cause TB disease
Majority of TB cases caused byM. tb
M. tb organisms also called tubercle bacilli
TB Case Management and Contact Investigation Intensive May 26-28, 2015 Curry International Tuberculosis Center
Basic Concepts in TB3
Transmission of M. tuberculosisM. tb spread via airborneparticles called dropletnuclei
Expelled when person withinfectious TB coughs, sneezes, shouts, or sings
Transmission occurs when droplet nuclei inhaled and reach the alveoli of the lungs, via nasal passages, respiratory tract, and bronchi
Probability TB will be Transmitted
Susceptibility of the exposed person
Infectiousness of person with TB (i.e., number of bacilli TB patient expels into the air)
Environmental factors that affect the concentration of M. tborganisms
Proximity, frequency, and duration of exposure (e.g., close contacts)
Can be transmitted from children, though less likely
PathogenesisDroplet nuclei containing tubercle bacilli are inhaled, enter the lungs, and travel to the alveoli.
Tubercle bacilli multiply in the alveoli.
TB Case Management and Contact Investigation Intensive May 26-28, 2015 Curry International Tuberculosis Center
Basic Concepts in TB4
Pathogenesis
A small number of tubercle bacilli enter the bloodstream and spread throughout the body. The tubercle bacilli may reach any part of the body, including areas where TB disease is more likely to develop (such as the brain, larynx, lymph node, lung, spine, bone, or kidney).
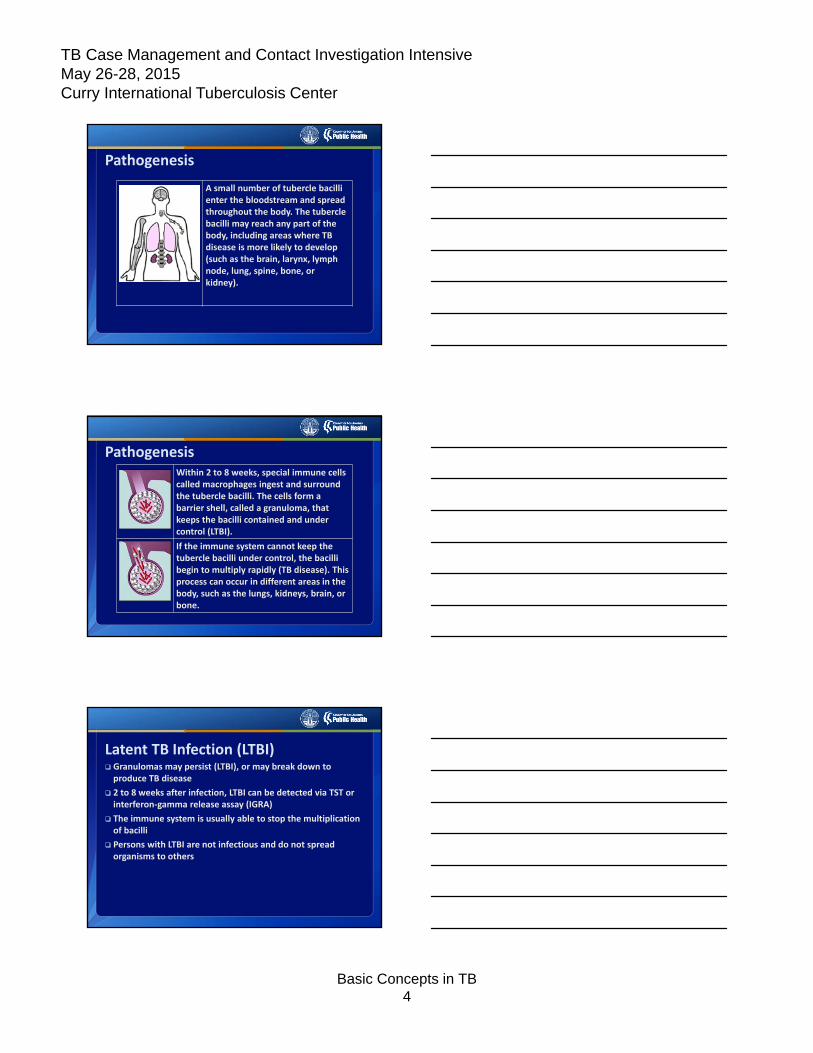
PathogenesisWithin 2 to 8 weeks, special immune cells called macrophages ingest and surround the tubercle bacilli. The cells form a barrier shell, called a granuloma, that keeps the bacilli contained and under control (LTBI).
If the immune system cannot keep the tubercle bacilli under control, the bacilli begin to multiply rapidly (TB disease). This process can occur in different areas in the body, such as the lungs, kidneys, brain, or bone.
Latent TB Infection (LTBI) Granulomas may persist (LTBI), or may break down to produce TB disease
2 to 8 weeks after infection, LTBI can be detected via TST or interferon‐gamma release assay (IGRA)
The immune system is usually able to stop the multiplication of bacilli
Persons with LTBI are not infectious and do not spread organisms to others
TB Case Management and Contact Investigation Intensive May 26-28, 2015 Curry International Tuberculosis Center
Basic Concepts in TB5
TB Disease
In some, the granulomas break down, bacilli escape and multiply, resulting in TB disease
Can occur soon after infection, or years later
Persons with TB disease are usually infectious and can spread bacteria to others
Positive M. tb culture confirms TB diagnosis
Sites of Disease
Lungs (pulmonary): most common site; usually infectious
Miliary: occurs when bacilli spread to all parts of the body; rare, but fatal if untreated
Central nervous system: usually occurs as meningitis, but can occur in brain or spine
Sites of Disease (cont.)Outside the lungs (extrapulmonary): usually not infectious, unless person has
Concomitant pulmonary disease,
Extrapulmonary disease in the oral cavity or larynx, or
Extrapulmonary disease with open site, especially with aerosolized fluid.
TB Case Management and Contact Investigation Intensive May 26-28, 2015 Curry International Tuberculosis Center
Basic Concepts in TB6
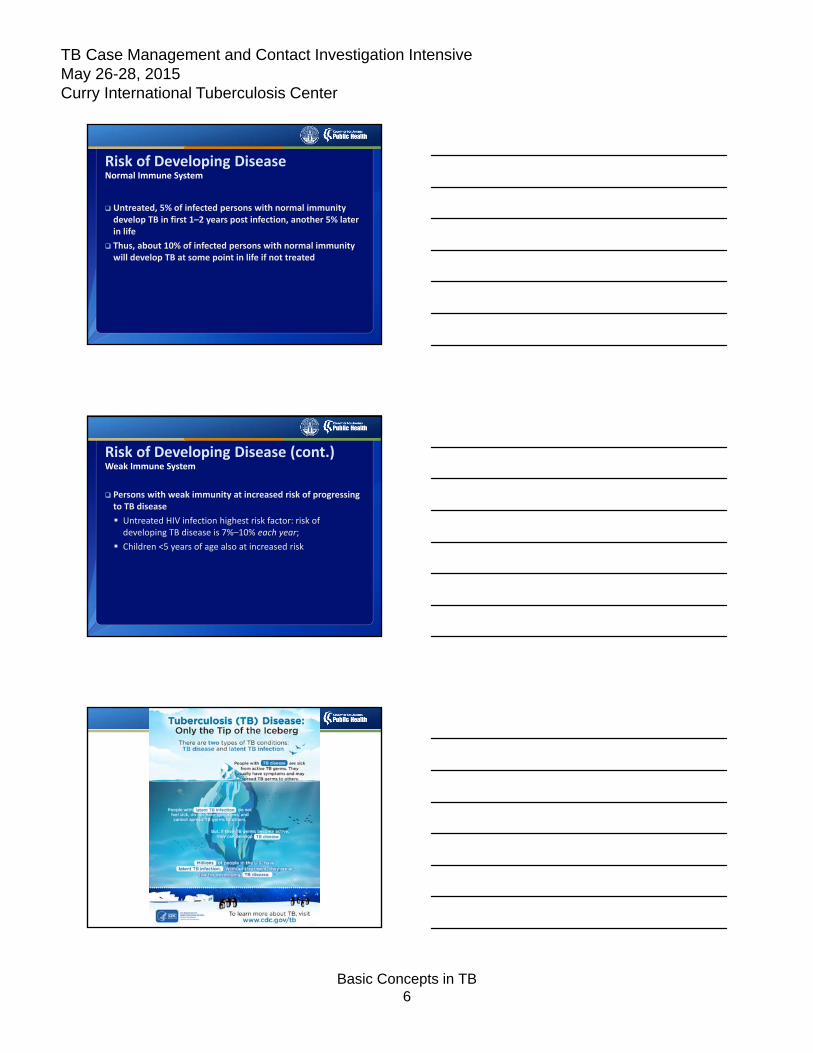
Risk of Developing DiseaseNormal Immune System
Untreated, 5% of infected persons with normal immunity develop TB in first 1–2 years post infection, another 5% later in life
Thus, about 10% of infected persons with normal immunity will develop TB at some point in life if not treated
Risk of Developing Disease (cont.)Weak Immune System
Persons with weak immunity at increased risk of progressing to TB disease
Untreated HIV infection highest risk factor: risk of developing TB disease is 7%–10% each year;
Children <5 years of age also at increased risk
TB Case Management and Contact Investigation Intensive May 26-28, 2015 Curry International Tuberculosis Center
Basic Concepts in TB7
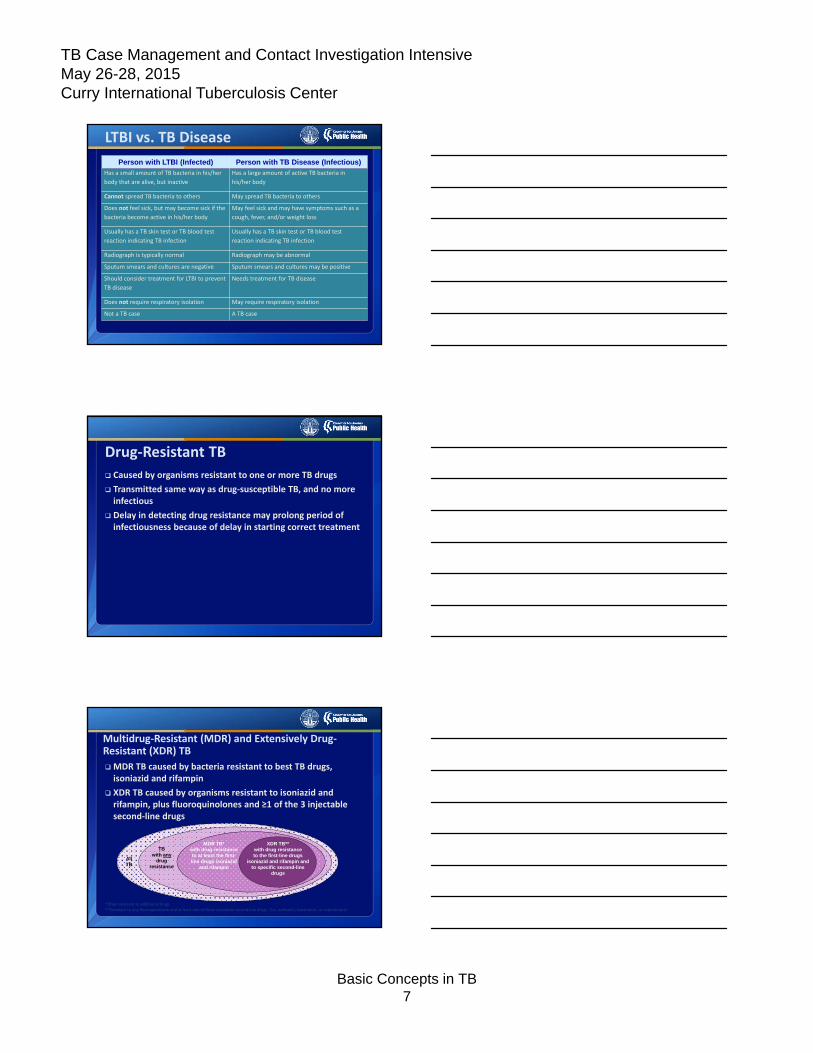
LTBI vs. TB Disease
Person with LTBI (Infected) Person with TB Disease (Infectious)
Has a small amount of TB bacteria in his/her
body that are alive, but inactive
Has a large amount of active TB bacteria in
his/her body
Cannot spread TB bacteria to others May spread TB bacteria to others
Does not feel sick, but may become sick if the
bacteria become active in his/her body
May feel sick and may have symptoms such as a
cough, fever, and/or weight loss
Usually has a TB skin test or TB blood test
reaction indicating TB infection
Usually has a TB skin test or TB blood test
reaction indicating TB infection
Radiograph is typically normal Radiograph may be abnormal
Sputum smears and cultures are negative Sputum smears and cultures may be positive
Should consider treatment for LTBI to prevent
TB disease
Needs treatment for TB disease
Does not require respiratory isolation May require respiratory isolation
Not a TB case A TB case
Drug‐Resistant TB
Caused by organisms resistant to one or more TB drugs
Transmitted same way as drug‐susceptible TB, and no more infectious
Delay in detecting drug resistance may prolong period of infectiousness because of delay in starting correct treatment
Multidrug‐Resistant (MDR) and Extensively Drug‐Resistant (XDR) TB
MDR TB caused by bacteria resistant to best TB drugs, isoniazid and rifampin
XDR TB caused by organisms resistant to isoniazid and rifampin, plus fluoroquinolones and ≥1 of the 3 injectable second‐line drugs
*Often resistant to additional drugs
**Resistant to any fluoroquinolone and at least one of three injectable second‐line drugs (i.e., amikacin, kanamycin, or capreomycin
MDR TB*with drug resistance to at least the first-line drugs isoniazid
and rifampin
TB with any
drug resistance
XDR TB**with drug resistanceto the first-line drugs
isoniazid and rifampin and to specific second-line
drugs
AllTB
TB Case Management and Contact Investigation Intensive May 26-28, 2015 Curry International Tuberculosis Center
Basic Concepts in TB8
Types of Drug ResistanceDrug resistance develops in two ways:
Primary resistance develops in persons initially infected with resistant organisms
Secondary (acquired) resistance develops during TB therapy
Circumstances Increasing the Risk of Drug‐Resistant TBRisk of drug‐resistant TB is increased with exposure to a person who
Has confirmed drug‐resistant TB
Had prior unsuccessful treatment for TB, and drug susceptibility results not known
Originated in a drug‐resistant TB prevalent country
Has positive smear and culture 2 months after treatment start
Classification System for TB
Based on TB pathogenesis (stage of disease)
Helps clinician track the development of TB in patients
Persons with class 3 or 5 TB should be reported to health department
Patients should not have class 5 classification for more than 3 months
TB Case Management and Contact Investigation Intensive May 26-28, 2015 Curry International Tuberculosis Center
Basic Concepts in TB9
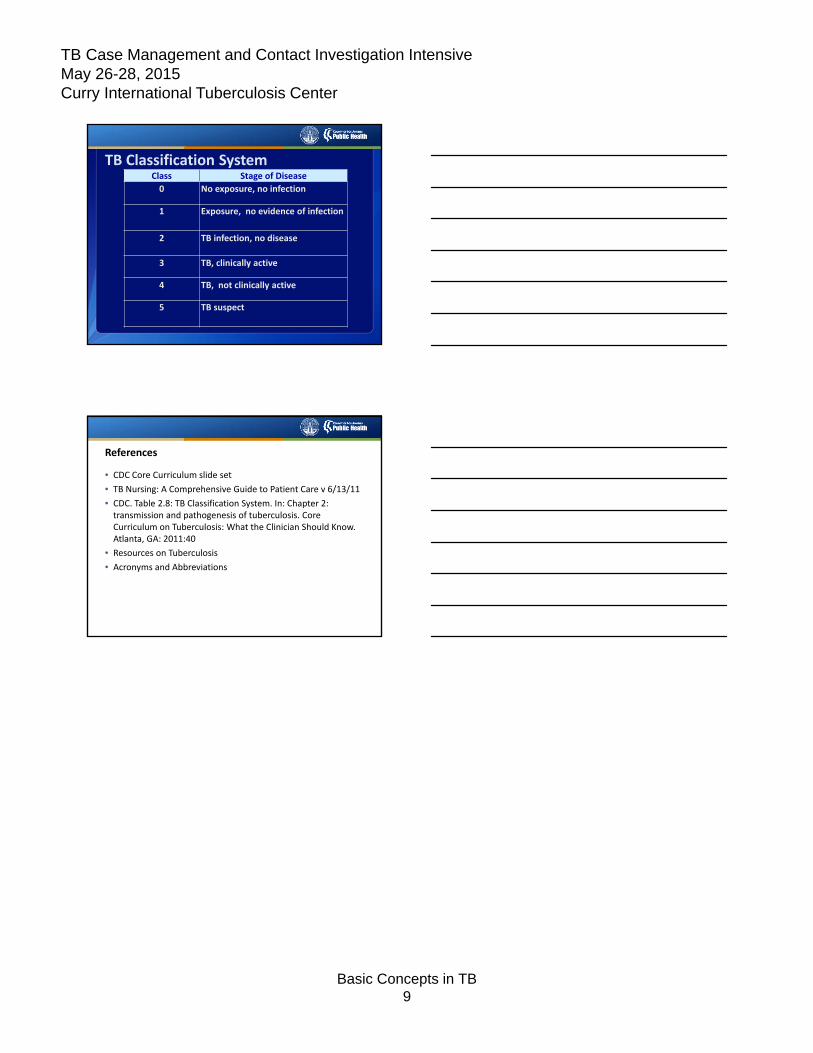
TB Classification SystemClass Stage of Disease
0 No exposure, no infection
1 Exposure, no evidence of infection
2 TB infection, no disease
3 TB, clinically active
4 TB, not clinically active
5 TB suspect
References
• CDC Core Curriculum slide set
• TB Nursing: A Comprehensive Guide to Patient Care v 6/13/11
• CDC. Table 2.8: TB Classification System. In: Chapter 2: transmission and pathogenesis of tuberculosis. Core Curriculum on Tuberculosis: What the Clinician Should Know. Atlanta, GA: 2011:40
• Resources on Tuberculosis
• Acronyms and Abbreviations
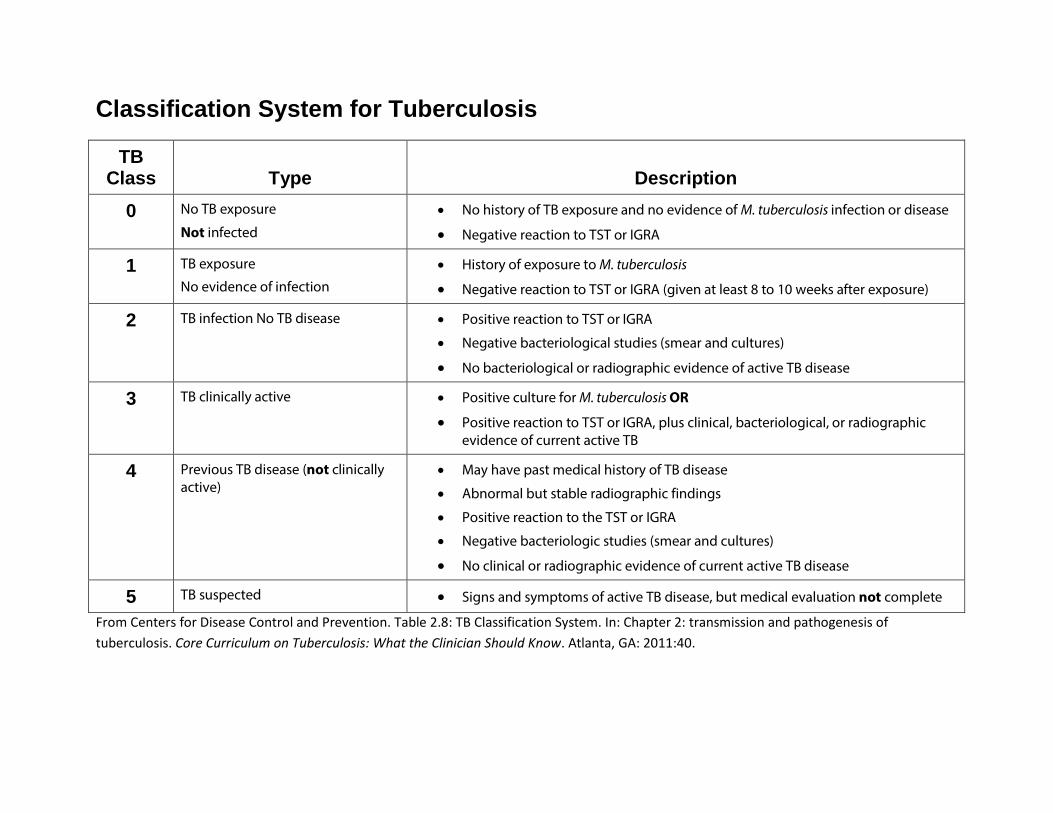
Classification System for Tuberculosis
TB Class
Type
Description
0 No TB exposure
Not infected • No history of TB exposure and no evidence of M. tuberculosis infection or disease
• Negative reaction to TST or IGRA
1 TB exposure
No evidence of infection • History of exposure to M. tuberculosis
• Negative reaction to TST or IGRA (given at least 8 to 10 weeks after exposure)
2 TB infection No TB disease
• Positive reaction to TST or IGRA
• Negative bacteriological studies (smear and cultures)
• No bacteriological or radiographic evidence of active TB disease
3 TB clinically active
• Positive culture for M. tuberculosis OR
• Positive reaction to TST or IGRA, plus clinical, bacteriological, or radiographic evidence of current active TB
4 Previous TB disease (not clinically active)
• May have past medical history of TB disease
• Abnormal but stable radiographic findings
• Positive reaction to the TST or IGRA
• Negative bacteriologic studies (smear and cultures)
• No clinical or radiographic evidence of current active TB disease
5 TB suspected • Signs and symptoms of active TB disease, but medical evaluation not complete
From Centers for Disease Control and Prevention. Table 2.8: TB Classification System. In: Chapter 2: transmission and pathogenesis of tuberculosis. Core Curriculum on Tuberculosis: What the Clinician Should Know. Atlanta, GA: 2011:40.
Websites Checked 5/7/2015
Resources on Tuberculosis (TB)
Centers for Disease Control and Prevention (CDC) Division of Tuberculosis Elimination (DTBE)
Guidelines: http://www.cdc.gov/tb/publications/guidelines/default.htm
Online Courses:
Self-Study Modules on Tuberculosis:
http://www.cdc.gov/tb/education/ssmodules/default.htm
Core Curriculum on Tuberculosis: What the Clinician Should Know:
http://www.cdc.gov/tb/education/corecurr/index.htm
Curry International Tuberculosis Center (CITC)
Medical Consultation Warmline: http://www.currytbcenter.ucsf.edu/consultation
877-390-6682 (toll-free)
Warmline inquiries can also be sent to the CITC email address, [email protected]
8:00 AM to 4:30 PM (Pacific Time), Monday through Friday (excluding holidays). Voicemail is available to record incoming messages 24 hours a day, 7 days a week.
Online Products: http://www.currytbcenter.ucsf.edu/products
(selected highlights only—check the web page for the full list)
Drug-Resistant Tuberculosis: A Survival Guide for Clinicians, 2nd edition
Radiographic Manifestations of Tuberculosis: A Primer for Clinicians, Second Edition
Tuberculosis Infection Control: A Practical Manual for Preventing TB
Websites Checked 5/7/2015
Curry International Tuberculosis Center (continued) Online Courses & Presentations: http://www.currytbcenter.ucsf.edu/products
(selected highlights only—check the web page for the full list)
Asking the Right Questions
Medical Management of Tuberculosis
Pediatric Tuberculosis
Practical Solutions for TB Infection Control: Infectiousness and Isolation
TB Prevention in the HIV-infected Patient: Screening, Testing, and Treatment of LTBI
Tuberculosis Radiology Resource Page
Archived Webinars: http://www.currytbcenter.ucsf.edu/trainings/webinar-archive Classroom Trainings: http://www.currytbcenter.ucsf.edu/trainings
National Tuberculosis Controllers Association (NTCA)
Tuberculosis Nursing, 2nd Edition:
http://www.tbcontrollers.org/resources/tb-nursing- manual/#.VFuW7Wf4pws
Interjurisdictional Transfer Form and Contacts:
http://www.tbcontrollers.org/resources/interjurisdictional-transfers/#.VFuW3Wf4pws
California Tuberculosis Controllers Association (CTCA)
California Department of Public Health/CTCA Joint Guidelines:
http://www.ctca.org/index.cfm?fuseaction=page&page_id=5074
CTCA Directory: http://www.ctca.org/index.cfm?fuseaction=page&page_id=5071

Tuberculosis (TB) Acronyms and Abbreviations
AFB acid-fast bacilli
AIDS acquired immune deficiency syndrome
ALT alanine aminotransferase
ARPE Aggregate Reports for Tuberculosis Program Evaluation
ART antiretroviral therapy
AST aspartate aminotransferase
ATBD active tuberculosis diease
ATS American Thoracic Society
BCG bacilli Calmette-Guérin
CBC complete blood count
CC cultural competency
CDC Centers for Disease Control and Prevention
CI contact investigation
CNS central nervous system
CXR chest x-ray
DTBE Division of Tuberculosis Elimination
DOT directly observed therapy
DST drug sensitivity testing
EMB ethambutol
ESRD end-stage renal disease
FQN fluoroquinolone
IA injectable agent
IDSA Infectious Diseases Society of America
HIV human immunodeficiency virus
HPLC high performance liquid chromatography
IGRA interferon gamma release assay
INH isoniazid
IP infectious period
IUATLD International Union Against Tuberculosis and Lung Disease
LEP limited English proficiency
LFT liver function test
LJ Lowenstein-Jensen
LTBI latent TB infection
M. tb Mycobacterium tuberculosis
MDR-TB multidrug-resistant TB
MGIT mycobacteria growth indicator tube
MIRU mycobacterial interspersed repetitive units
MMCP MediCal Managed Care Plan
MMWR Morbidity and Mortality Weekly Report
MOTT mycobacteria other than tuberculosis
NAAT nucleic amplification test
NNRTI non-nucleoside reverse transcriptase inhibitor
NRTI nucleoside reverse transcriptase inhibitor
NTCA National Tuberculosis Controllers Association
NTIP National Tuberculosis Indicators Project
NTM nontuberculous mycobacteria
NTNC National Tuberculosis Nurse Coalition
OTIS Online Tuberculosis Information System
PCR polymerase chain reaction
PI protease inhibitor
PPD purified protein derivative
PZA pyrazinamide
QA quality assurance
QI quality improvement
QFT-GIT QuantiFERON®-TB Gold In-Tube test
RBT rifabutin
RPT rifapentine
RIF rifampin
RTMCC Regional Training and Medical Consultation Center
RVCT Report of Verified Case of Tuberculosis
TDR totally drug-resistant tuberculosis
TNF-α tumor necrosis factor-alpha
TST tuberculin skin test
T-Spot T-SPOT®.TB test
SAT self-administered therapy
SM streptomycin
WHO World Health Organization
XDR-TB extensively drug-resistant tuberculosis