
Basal cell carcinoma. 2 Basal cell carcinoma is the most commonly diagnosed malignancy worldwide The...
13
1 Basal cell carcinoma
-
Upload
anabel-hampton -
Category
Documents
-
view
223 -
download
4
Transcript of Basal cell carcinoma. 2 Basal cell carcinoma is the most commonly diagnosed malignancy worldwide The...

Basal cell carcinoma

2
Basal cell carcinoma is the most commonly diagnosed malignancy worldwide
• The annual global incidence of non-melanoma skin cancer (NMSC) is 2–3 million cases1
• Basal cell carcinoma (BCC) constitutes ~80% of all NMSCs, accounting for ~2 million cases worldwide each year2,3
• Basal cell carcinoma (BCC) develops in the basal layer of the epidermis and is the most commonly diagnosed malignancy worldwide2,4-6
• BCC is mainly a Caucasian disease. The average lifetime risk for Caucasians to develop BCC is approximately 30%2,4
1. World Health Organization: http://www.who.int/uv/faq/skincancer/en/index1.html2. Rubin AI et al. N Engl J Med 2005;353:2262–9
3. Diepgen TL, Mahler V. Br J Dermatol 2002;146(suppl):1–64. Wong CSM et al. Br Med J 2003;327:794–8
5. Roewert-Huber J et al. Br J Dermatol 2007;157:47–516. Lear JT et al. J R Soc Med 1998;91:585–8

3
A major cause of BCC is exposure to UV radiation
• A major cause of BCC is exposure to UV radiation, leading to cumulative DNA damage and gene mutations1–5
• Epidemiological data suggest the overall incidence of BCC is increasing significantly and show marked geographical variation1,6–8
• Australia has the highest incidence rate of BCC in the world, reporting a rate of 1–2% per year1,6
5. Caro I, Low JA. Clin Cancer Res 2010;16:3335–96. Diepgen TL, Mahler V. Br J Dermatol 2002;146(suppl):1–6
7. Ting PT et al. J Cutan Med Surg 2005;9:10–158. Rogers HW et al. Arch Dermatol 2010;146:283–7
80% occur on the head and neck
15% occur on the trunk
5% occur on the arms, legs or other sites
Most sporadic cases of BCC arise from chronic sun-exposure1,2
1. Rubin AI et al. N Engl J Med 2005;353:2262–92. Wong CSM et al. Br Med J 2003;327:794–8
3. Roewert-Huber J et al. Br J Dermatol 2007;157:47–514. Lear JT et al. J R Soc Med 1998;91:585–8

4
The closer Caucasians live to the equator, the greater the risk of developing BCC
1. Diepgen TL, Mahler V. Br J Dermatol 2002;146(suppl):1–62. Bath-Hextall F et al. Int J Cancer 2007;121:2105–8
Country Year of report Male Female
AustraliaNambour1 1996 2074 1579Townsville1 1998 2055 1195
USNew Hampshire1 1991 159 87Rochester, MN1 1997 175 124US (other)1 1994 407 212
EuropeFinland1 1999 49 45The Netherlands1 1991 46 32Scotland (UK)1 1998 50 37Wales (UK)1 2000 128 105UK2 2003 177 148
EASR2 1996–2003 104 78WASR2 1996–2003 69 53
EASR: European age-standardised rate; WASR: World age-standardised ratePer 100,000 population
Age-standardised rates of BCC

5
There are different clinical subtypes of BCC• Clinical subtypes of BCCs:1–3
1. Images reproduced with permission from BMJ Publishing Group Wong CSM et al. Br Med J 2003;327:794–8
2. Roewert-Huber J et al. Br J Dermatol 2007;157:47–513. Walling HW et al. Cancer Metastasis Rev 2004;23:389–402
• Occur frequently on sun-exposed areas of the head
• Often present as a papule or nodule
• Occur most frequently on the trunk
• Characterised by small buds of basaloid tumour cells extending from the epidermis
• Includes pigmented BCC and morpheaform BCC (also called sclerosing or fibrosing BCC)
• Morpheaform BCCs are aggressive infiltrating subtypes with ill-defined borders, making complete excision a challenge
Nodular (60%) Superficial (30%) Other (10%)
NB: if you wish to present, reproduce or adapt the images on this slide, please seek permission from the relevant publication house.
6
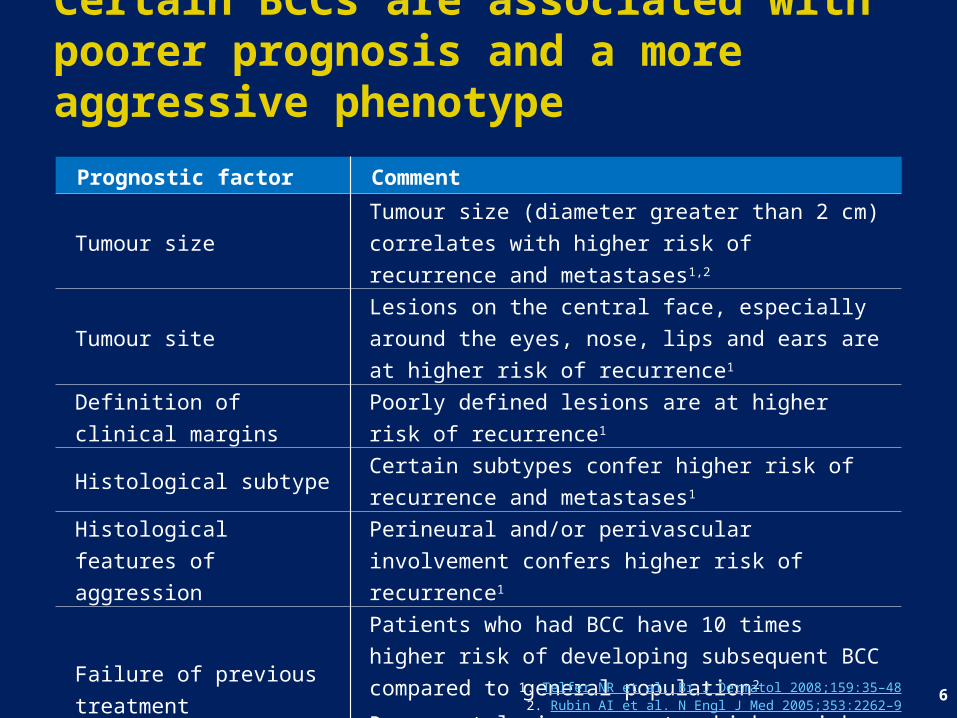
Prognostic factor Comment
Tumour size Tumour size (diameter greater than 2 cm) correlates with higher risk of recurrence and metastases1,2
Tumour site Lesions on the central face, especially around the eyes, nose, lips and ears are at higher risk of recurrence1
Definition of clinical margins Poorly defined lesions are at higher risk of recurrence1
Histological subtype Certain subtypes confer higher risk of recurrence and metastases1
Histological features of aggression
Perineural and/or perivascular involvement confers higher risk of recurrence1
Failure of previous treatment
Patients who had BCC have 10 times higher risk of developing subsequent BCC compared to general population2
Recurrent lesions are at a higher risk of further recurrence and metastases1
Immunosuppression Confers increased risk of recurrence and metastases (e.g. recipients of solid-organ transplants)2
1. Telfer NR et al. Br J Dermatol 2008;159:35–482. Rubin AI et al. N Engl J Med 2005;353:2262–9
Certain BCCs are associated with poorer prognosis and a more aggressive phenotype

7
In some cases BCC can progress to an advanced form
• Progression of BCC is generally characterised by slow growth and minimal soft tissue invasiveness and surgery cures most cases of BCC1,2
• However, BCC can develop into advanced BCC where surgery is inappropriate3,4
• Advanced BCC can be disfiguring or debilitating, lead to significant morbidity or even be fatal1,5
• Advanced BCC comprises locally advanced BCC (laBCC) and metastatic BCC (mBCC)3
1. Walling HW et al. Cancer Metastasis Rev 2004;23:389–4022. Lear JT et al. J R Soc Med 1998;91:585–8
3. Joshi AD, et al. J Clin Oncol 2011; 29 (Suppl: abstract e19001)4. Tang JY, Epstein EH. AccessMedicine 2010
5. Ting PT, et al. J Cutan Med Surg 2005;9(1):10–15
“

8
Advanced BCC is less common but more serious than other BCCs
• Patients whose lesions are not appropriate for surgery, or who have medical contraindications to surgery
• Patients for whom surgery would result in substantial morbidity and/or deformity (e.g. invasion into skull, limb amputation, or enucleation)
• Rare but serious form of BCC (0.0028–0.55% of BCCs progress to mBCC)1
• Includes distant metastases (e.g. bone, lung and liver) or lymph node involvement1
• Poor prognosis (median survival: 8–14 months1-3; 5-year survival rate: 10%3,4)
Advanced BCC
1. Ting PT et al. J Cutan Med Surg 2005;9:10–152. von Domarus H, Stevens PJ. J Am Acad Dermatol 1984;10:1043–60
3. Lo JS et al. J Am Acad Dermatol 1991;24:715–194. Wong CSM et al. Br Med J 2003;327:794–8
Advanced BCC• Occurs in a small proportion of patients• Advanced BCC patients have lesions that are not appropriate for surgery, or for whom surgery would
result in substantial deformity, e.g. because of the location of the lesion Locally advanced BCC (laBCC) Metastatic BCC (mBCC)
Locally advanced BCC
mBCC Metastatic BCC
BCC
laBCC

9
Surgery is the most common treatment for BCC, but is not always appropriate
• Surgical techniques are the most common treatment for BCC and have a high success rate, particularly in uncomplicated BCC cases1,2
• However, surgery can be debilitating and disfiguring, and is sometimes inappropriate
Surgical technique2 5-year cure rate*2
Surgical excision ≥95%Curettage and cautery ≥95%Cryosurgery ≥95%Mohs micrographic surgery ~99%
3. Goldberg LH et al. Arch Dermatol 2010;146:17–9 Copyright © 2010 American Medical Association. All rights reserved
4. Von Hoff DD et al. New Engl J Med 2009;361:1164–72 Copyright © 2009 Massachusetts Medical Society. All rights reserved
InoperableOperable
1. Walling HW et al. Cancer Metastasis Rev 2004;23:389–402
2. Image reproduced with permission from BMJPublishing Group. Wong CSM et al. Br Med J 2003;327:794–8
4.3.2.
*5-year cure rate for primary BCC
NB:
if y
ou w
ish
to p
rese
nt, r
epro
duce
or a
dapt
the
imag
es o
n th
is
slid
e, p
leas
e se
ek p
erm
issi
on fr
om th
e re
leva
nt p
ublic
ation
hou
se.

10
Current treatment options are limited for patients with advanced BCC for whom surgery is inappropriate
• Tumours that are not appropriate for surgery, or for which surgery would result in substantial deformity (i.e. in difficult-to-treat locations) may require treatment with non-surgical approaches, such as: Radiotherapy,1 photodynamic therapy,2 chemotherapy,3 topical therapy4,5
Most have significant drawbacks and for many patients may not be appropriate6,7
• For example, radiotherapy is: Contraindicated: in genetic syndromes predisposing to skin cancer,8,9 or for BCC that has recurred after prior radiotherapy10
Restricted: in tumours located near eyes or on eyelids, which are difficult to treat,10 or in people who are nearing their maximum safe lifetime dose of radiation11
Generally reserved for patients ≥ 60 years, given that new skin cancers can arise from radiotherapy scars9
1. Wong CSM et al. Br Med J 2003;327:794–82. Szeimies RM et al. Acta Derm Venereol 2005;85:483–90
3. Tucker SB et al. J Am Acad Dermatol 2006;54:1033–84. Alessi SS et al. Clinics (Sao Paulo) 2009;64:961–6
5. Gross K et al. Dermatol Surg 2007;33:433–9
6. Goppner D, Leverkus M. J Skin Cancer 2011;doi:10.1155/2011/6502587. Von Hoff DD et al. N Engl J Med 2009;361:1164-1172
8. Loncaster J et al. Clin Oncol (R Coll Radiol) 2009;21:502–89. Samarasinghe V. J Skin Cancer. 2011;2011:328615
10. Telfer NR et al. Br J Dermatol 2008;159:35–4811. Mills WA. Health Phys 1985;48:701–4

11
There is a current unmet medical need in advanced BCC
• For patients with advanced BCC, current treatment options are suboptimal 1,2 and may add further morbidity 3,4
• At present, patients with inoperable advanced BCC or in whom surgical resection would result in substantial deformity have very few therapeutic options There is no standard therapy for advanced BCC 5
• Once BCC has metastasised, it is highly malignant and has a poor prognosis 6
• Therefore, new treatment options are needed for advanced BCC
1. Goppner D, Leverkus M. J Skin Cancer 2011; doi:10.1155/2011/650258.2. Ting PT, et al. J Cutan Med Surg 2005;9(1):10-15
3. Wong CSM et al. Br Med J 2003;327:794–84. Walling HW et al. Cancer Metastasis Rev 2004;23:389–402
5. Von Hoff DD et al. New Engl J Med 2009;361:1164–726. Ozbek N et al. N Z Med J 2004;117:U874

12
Summary
• BCC is the most commonly diagnosed cancer and is a mainly Caucasian disease caused by UV exposure• Progression of BCC is generally characterised by s low growth and minimal soft tissue invasiveness, and surgery cures most cases of BCC• BCC can develop into advanced BCC where surgery is inappropriate. It can be disfiguring or debilitating, lead to s ignificant morbidity (locally advanced BCC) or even be fatal (metastatic BCC)• For patients with advanced BCC current treatment options are suboptimal and may add further morbidity• New treatment options are needed for advanced BCC

13
Alessi SS, et al. Treatment of cutaneous tumors with topical 5% imiquimod cream. Clinics (Sao Paulo) 2009;64:961–966.Bath-Hextall F, et al. Trends in incidence of skin basal cell carcinoma. Additional evidence from a UK primary care database study. Int J Cancer 2007;121:2105–2108.Caro I, Low JA. The role of the hedgehog signaling pathway in the development of basal cell carcinoma and opportunities for treatment. Clin Cancer Res 2010;16:3335–3339.Diepgen TL, Mahler V. The epidemiology of skin cancer. Br J Dermatol 2002;146(suppl):1–6.Goldberg LH, et al. Basal cell nevus syndrome: a brave new world. Arch Dermatol 2010;146:17–19.Goppner D, Leverkus M. Basal cell carcinoma: from the molecular understanding of the pathogenesis to targeted therapy of progressive disease. J Skin Cancer. 2011;2011:650258.Gross K, et al. 5% 5-Fluorouracil cream for the treatment of small superficial Basal cell carcinoma: efficacy, tolerability, cosmetic outcome, and patient satisfaction. Dermatol Surg 2007;33:433–439.Joshi AD, et al. J Clin Oncol 2011; 29 (Suppl: abstract e19001).Lear JT, et al. Basal cell carcinoma. J R Soc Med 1998;91:585–588.Lo JS, et al. Metastatic basal cell carcinoma: report of twelve cases with a review of the literature. J Am Acad Dermatol 1991;24:715–719.Loncaster J, et al. Efficacy of photodynamic therapy as a treatment for Gorlin syndrome-related basal cell carcinomas. Clin Oncol (R Coll Radiol) 2009;21:502–508.Mills WA. Regulatory consideration in radiation protection. Health Phys 1985;48:701–704.Ozbek N, et al. Metastatic basal cell carcinoma. N Z Med J 2004;117:U874
Roewert-Huber J, et al. Epidemiology and aetiology of basal cell carcinoma. Br J Dermatol 2007;157:47–51.Rogers HW, et al. Incidence estimate of nonmelanoma skin cancer in the United States, 2006. Arch Dermatol 2010;146:283–287.Rubin AI, et al. Basal-cell carcinoma. N Engl J Med 2005;353:2262–2269.Samarasinghe V. Beyond the scalpel: targeting hedgehog in skin cancer prevention. J Skin Cancer. 2011;2011:328615.Szeimies RM, et al. Photodynamic therapy for non-melanoma skin cancer. Acta Derm Venereol 2005;85:483–490.Telfer NR, et al. Guidelines for the management of basal cell carcinoma. Br J Dermatol 2008;159:35–48. Tang JY, Epstein EH. AccessMedicine 2010. Available from http://www.medscape.com/viewarticle/720380 Last accessed February 2012.Ting PT, et al. Metastatic basal cell carcinoma: report of two cases and literature review. J Cutan Med Surg 2005;9:10–15.Tucker SB, et al. Long-term follow-up of basal cell carcinomas treated with perilesional interferon alfa 2b as monotherapy. J Am Acad Dermatol 2006;54:1033–1038.von Domarus H, Stevens PJ. Metastatic basal cell carcinoma. Report of five cases and review of 170 cases in the literature. J Am Acad Dermatol 1984;10:1043–1060.Von Hoff DD, et al. Inhibition of the hedgehog pathway in advanced basal-cell carcinoma. New Engl J Med 2009;361:1164–1172.Walling HW, et al. Aggressive basal cell carcinoma: presentation, pathogenesis, and management. Cancer Metastasis Rev 2004;23:389–402.Wong CSM, et al. Basal cell carcinoma. Br Med J 2003;327:794–798.World Health Organization: http://www.who.int/uv/faq/skincancer/en/index1.html Accessed February 2012.
ReferencesBasal cell carcinoma


















