Baran KW August 28, 2000 Kenneth W. Baran MD for the LIMIT AMI Investigators St. Paul Heart Clinic,...
23
Baran KW August 28, 2000 Kenneth W. Baran MD Kenneth W. Baran MD for the LIMIT AMI Investigators for the LIMIT AMI Investigators St. Paul Heart Clinic, St. Paul, MN, St. Paul Heart Clinic, St. Paul, MN, USA USA Sponsor: Genentech Inc., South San Francisco, Sponsor: Genentech Inc., South San Francisco, USA USA LIMIT AMI LIMIT AMI ( ( LI LI mitation of mitation of M M yocardial yocardial I I njury njury following following T T hrombolysis in hrombolysis in A A cute cute M M yocardial yocardial I I nfarction) nfarction) An angiographic safety and efficacy An angiographic safety and efficacy trial of a novel anti-CD18 therapy in trial of a novel anti-CD18 therapy in acute myocardial infarction in acute myocardial infarction in conjunction with thrombolysis conjunction with thrombolysis
-
Upload
randolph-holland -
Category
Documents
-
view
215 -
download
1
Transcript of Baran KW August 28, 2000 Kenneth W. Baran MD for the LIMIT AMI Investigators St. Paul Heart Clinic,...

Baran KW August 28, 2000
Kenneth W. Baran MDKenneth W. Baran MDfor the LIMIT AMI Investigatorsfor the LIMIT AMI Investigators
St. Paul Heart Clinic, St. Paul, MN, USASt. Paul Heart Clinic, St. Paul, MN, USA
Sponsor: Genentech Inc., South San Francisco, Sponsor: Genentech Inc., South San Francisco, USAUSA
LIMIT AMILIMIT AMI((LILImitation of mitation of MMyocardial yocardial IInjury following njury following
TThrombolysis in hrombolysis in AAcute cute MMyocardial yocardial IInfarction)nfarction)
An angiographic safety and efficacy trial of a An angiographic safety and efficacy trial of a novel anti-CD18 therapy in acute myocardial novel anti-CD18 therapy in acute myocardial infarction in conjunction with thrombolysisinfarction in conjunction with thrombolysis

Baran KW August 28, 2000

Baran KW August 28, 2000
rhuMAb CD18rhuMAb CD18
Antibody fragment [F(ab’)Antibody fragment [F(ab’)22]] Single dose administered as IV bolusSingle dose administered as IV bolus Plasma half-life 7 to 10 hoursPlasma half-life 7 to 10 hours 90% CD18-containing receptor 90% CD18-containing receptor
saturation maintained for ~ 24 hours saturation maintained for ~ 24 hours (0.5 mg/kg) and ~ 48 hours (2.0 mg/kg)(0.5 mg/kg) and ~ 48 hours (2.0 mg/kg)

Baran KW August 28, 2000
The LIMIT AMI Trial of rhuMAb CD18The LIMIT AMI Trial of rhuMAb CD18
• ST elevation > 2 leads• Symptoms < 12 hrs• No prior coronary surgery• No cardiogenic shock• No thrombolytic exclusions• No major immune-related risks
ScreeningScreeningScreeningScreening

Baran KW August 28, 2000
The LIMIT AMI Trial of rhuMAb CD18The LIMIT AMI Trial of rhuMAb CD18
• ST elevation > 2 leads• Symptoms < 12 hrs• No prior coronary surgery• No cardiogenic shock• No thrombolytic exclusions• No major immune-related risks
ScreeningScreeningScreeningScreening
Randomization 1:1:1 with administration prior to full-dose tPARandomization 1:1:1 with administration prior to full-dose tPARandomization 1:1:1 with administration prior to full-dose tPARandomization 1:1:1 with administration prior to full-dose tPA
2 mg/kg 0.5 mg/kg Placebo+ usual care including aspirin, IV heparin

Baran KW August 28, 2000
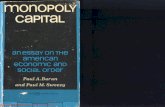
The LIMIT AMI Trial of rhuMAb CD18The LIMIT AMI Trial of rhuMAb CD18
• ST elevation > 2 leads• Symptoms < 12 hrs• No prior coronary surgery• No cardiogenic shock• No thrombolytic exclusions• No major immune-related risks
ScreeningScreeningScreeningScreening
Coronary angiography 90 minutes from tPA initiationCoronary angiography 90 minutes from tPA initiationCoronary angiography 90 minutes from tPA initiationCoronary angiography 90 minutes from tPA initiation
Randomization 1:1:1 to study drug or placebo then full-dose tPARandomization 1:1:1 to study drug or placebo then full-dose tPARandomization 1:1:1 to study drug or placebo then full-dose tPARandomization 1:1:1 to study drug or placebo then full-dose tPA
2 mg/kg 0.5 mg/kg Placebo
• Corrected TIMI Frame Count, TIMI Flow Grade• TIMI Myocardial Perfusion Grade• Angioplasty ± Gp IIb/IIIa inhibitors as required
+ usual care including aspirin, IV heparin

Baran KW August 28, 2000
The LIMIT AMI Trial of rhuMAb CD18The LIMIT AMI Trial of rhuMAb CD18
• Infarct size• sestamibi at rest, day 6-9• CKMB 0-72 hours
• ECG ST segment resolution• 180 minutes
• Fever• Antibiotic use• General Safety
Other endpointsOther endpointsOther endpointsOther endpoints

Baran KW August 28, 2000
Statistical AnalysisStatistical Analysis
Efficacy endpoint data analyzed by independent Efficacy endpoint data analyzed by independent and blinded Core Laboratoriesand blinded Core Laboratories
Time windows were used for efficacy endpoints Time windows were used for efficacy endpoints using imputation for missing data where possibleusing imputation for missing data where possible
““As treated” analysis of the evaluable cohortAs treated” analysis of the evaluable cohort Sensitivity analysesSensitivity analyses p values: non parametric testsp values: non parametric tests

Baran KW August 28, 2000
ResultsResults
Enrollment from September 1998 to March 2000Enrollment from September 1998 to March 2000 413 subjects randomized413 subjects randomized 394 treated with rhuMAb CD18 or placebo394 treated with rhuMAb CD18 or placebo 19 randomized but not treated 19 randomized but not treated
mainly due to review of exclusion criteriamainly due to review of exclusion criteria
60 centers in US and Canada60 centers in US and Canada

Baran KW August 28, 2000
Baseline characteristicsBaseline characteristics
Placebo 0.5 mg/kg 2.0 mg/kg
Age, mean 58.3 58.5 59.6
% Female 33 24 24
BMI, mean 29 28 29
% Previous MI 16 15 15
% Anterior MI 47 40 41
Time from pain onsetto tPA, mean (median)
3.6 (2.9) 3.3 (2.7) 3.4 (2.6)
% 0-6 hours 90 90 87

Baran KW August 28, 2000
Concomitant Concomitant InterventionsInterventions
Placebo 0.5 mg/kg 2.0 mg/kg
% Any PTCA 67 78 67
% PTCA with stent 60 71 61
% Any IIb/IIIa Day 1-2 27 29 30
% Plavix Day 1-2 58 61 55
% CABG 13 9 12

Baran KW August 28, 2000
Change in peripheral Change in peripheral venous blood white cell venous blood white cell counts - mean valuescounts - mean values
8
10
12
14
16
18
0 24 48 72
Time (hours)
WB
C (
x100
0)
Placebo 0.5 mg/kg 2.0 mg/kg

Baran KW August 28, 2000
Primary Endpoint: Corrected Primary Endpoint: Corrected TIMI Frame Count @90 TIMI Frame Count @90
minutesminutesC
orr
ec
ted
TIM
I Fra
me
Co
un
t
10
20
30
40
50
60
70
80
90
100
Placebo 0.5 mg/kg 2.0 mg/kg
Treatment Received
p = 0.2 p = 1.0
meanmeanmedianmedian

Baran KW August 28, 2000
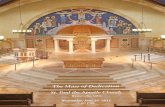
% TIMI Grade 3 flow% TIMI Grade 3 flow
0
10
20
30
40
50
60
70
Placebo 0.5 mg/kg 2.0 mg/kg
% T
IMI
3 F
low
Expected per protocol: placebo 55%, treatment 70%
N=114 N=111 N=108
66%
58%63%

Baran KW August 28, 2000
TIMI Flow Grades (all grades)TIMI Flow Grades (all grades)
0%10%20%30%40%50%60%70%80%90%
100%
Placebo 0.5 mg/kg 2.0 mg/kg
% T
IMI
Flo
w
TIMI 3TIMI 2TIMI 1TIMI 0
N=114 N=111 N=108

Baran KW August 28, 2000
TIMI Myocardial Perfusion TIMI Myocardial Perfusion GradeGrade
0%10%20%30%40%50%60%70%80%90%
100%
Placebo 0.5 mg/kg 2.0 mg/kg
TIM
I P
erfu
sion
Gra
de
%
Grade 2,3Grade 0,1
N=107 N=101 N=102

Baran KW August 28, 2000
ECG ST segment elevation ECG ST segment elevation resolutionresolution
at 180 minutesat 180 minutes
0%10%20%30%40%50%60%70%80%90%
100%
Placebo 0.5 mg/kg 2.0 mg/kg
% E
CG
ST
Seg
men
t E
leva
tion
R
esol
utio
n
=>70%30 to <70%< 30%
N=109 N=103 N=106

Baran KW August 28, 2000
Infarct Size by sestamibi Infarct Size by sestamibi scan Day 6-9scan Day 6-9
LV
de
fect
%
0
10
20
30
40
50
60
70
80
Placebo 0.5 mg/kg 2.0 mg/kg
Treatment Received
meanmeanmedianmedian

Baran KW August 28, 2000
Clinical outcomes at Day Clinical outcomes at Day 3030
Placebo(n=134)
0.5 mg/kg(n=129)
2.0 mg/kg(n=131)
Death 5.9% 3.1% 5.3%
Recurrent MI* 3.7% 2.3% 3.1%
CHF** 6.7% 7.8% 12.2%
Death/MI/CHF*** 11.9% 10.9% 15.3%
* Adverse Event report, complications CRF, or readmission diagnosis** CHF Killip III or IV, or CHF readmission, or CHF Adverse Event (serious or severe or cardiogenic shock)*** Death, CHF or recurrent AMI

Baran KW August 28, 2000
Safety - fever and Safety - fever and antibiotic useantibiotic use
0
5
10
15
20
25
30
Placebo 0.5 mg/kg 2.0 mg/kg
%
Fever all AE T => 101.5F Antibiotic Day 1-7
N=129 N=131N=134

Baran KW August 28, 2000
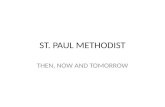
Safety - Likely bacterial Safety - Likely bacterial infectionsinfections
02468
1012141618202224
Placebo 0.5 mg/kg 2.0 mg/kg
%
Mild-moderate Severe
N=134 N=129 N=131
95% CI

Baran KW August 28, 2000
General SafetyGeneral Safety
No effect on fibrinogen or d-dimer levelsNo effect on fibrinogen or d-dimer levels No increase in “serious and life-threatening No increase in “serious and life-threatening
bleeding”bleeding” Slight trend towards increases in overall bleeding Slight trend towards increases in overall bleeding
adverse events (adverse events ( 10%) and transfusions ( 10%) and transfusions ( 20%) 20%) Small number of mild thrombocytopenia cases Small number of mild thrombocytopenia cases
< 100,000/mm< 100,000/mm33: placebo 2 cases, 0.5 mg/kg 1 case, : placebo 2 cases, 0.5 mg/kg 1 case, 2.0 mg/kg 5 cases2.0 mg/kg 5 cases
No specific anti-rhuMAb CD18 antibody formation*No specific anti-rhuMAb CD18 antibody formation*
* Except for one 30 Day sample with possible low level anti-CDR activity still under investigation.

Baran KW August 28, 2000
ConclusionsConclusions
rhuMAb CD18, in conjunction with rhuMAb CD18, in conjunction with thrombolysis, had no effect on coronary flow, thrombolysis, had no effect on coronary flow, infarct size or ECG ST segment resolutioninfarct size or ECG ST segment resolution
These results are consistent with the findings of These results are consistent with the findings of another Phase II study of an anti-CD18 antibody another Phase II study of an anti-CD18 antibody in Primary Angioplasty on infarct size (HALT in Primary Angioplasty on infarct size (HALT MI*)MI*)
There may be non CD18- dependent leukocyte There may be non CD18- dependent leukocyte binding and transmigration in AMIbinding and transmigration in AMI
Leukocytes may not be key to ischemia-Leukocytes may not be key to ischemia-reperfusion injury in human AMIreperfusion injury in human AMI
* Faxon D, Annual Meeting of the American Heart Association, Atlanta, November 1999