Balloon angioplasty for postoperative pulmonary artery ... · artery stenosis was 51% (20 of 39...
8
JACCVol .22 .No .3 September1993:at59-fib all l_ TOS IONAKANISHI,MD,YASUTOSFII MAKOTONAKAZAWA,MD,YASUHA Tokyo,Japan Objectives .This studywasdesignedtoassessthesuccessrate anddeterminantsofsuccessorfailureofballoonangioplastyfor postoperativepulmonarystenosisinpatientswithtranspositionof thegreatarteries . Background.Previous reportshavesuggestedthatpulmonary stenosisthatdevelopsnt"erthearterialswitchoperationisnot likelytobedilated . Methods . Twenty-eightpatientswithtranspositionofthegreat arteriesunderwent39balloonangioplastyproceduresafterthe arterialswitchoperation .Themeanageatdilationwas4 .5±2.2 years(range0 .7to 9.8), andtheintervalbetweenoperationand balloondilationwas3.6±1 .8years .Thecriterionof successful dilationwasaj50%®increaseinpredilationdiameterora ? 50% decreaseinpredilationpressuregradient .Iftherightventricular/ aorticpressureratiodecreasedby ?0 .2, sothattheratiobecame <0 .68,reoperationwasthoughttobenotindLated. Results .Thesuccess rateofballoonangioplastyforpulmonary arterystenosiswas51%(20of39dilations) . Themean ageat dilationinthegroupwithsuccessfuldilation(3 .6years)was significantlyyoungerthanthatinthegroupwithunsuccessful Pulmonarystenosisoccursin7%to28%ofcasesafterthe arterialswitchoperationfortranspositionofthegreatarter- ies (1-4) . Balloonangioplastyhasbeenattemptedtorelieve thislesion,butbecauseballoondilationisnotusually successful,surgicaltreatmenthasbeenemployedinmost cases (1,2,4) . Saxenaetal . (5), whoperformedballoon angioplastyinfivepatientswithnosuccessfuldilation, concludedthatpulmonaryarterystenosisafterthearterial . switchoperationisnotlikelytobedilatedbyballoon angioplasty .Wereviewedourearlyresultsof39dilationsin 28patientsandtriedtodelineatethedeterminantsofsLccess orfailureofballoonangioplasty . FromtheDepartmentofPediatricCardiologyandPediatricCardiovascu- larSurgery,HeartInstituteofJapan,TokyoWomen'sMedicalCollege, Tokyo,Japan . ManuscriptreceivedOctober29,1992 ;revisedmanuscriptreceived February22,1993,acceptedMarch2,1993 . Address .forcoeiespondence ; ToshioNakanishi,MD,PediatricCardiol- ogy,HeartInstituteofJapan,TokyoWomen'sMedicalCollege,8-1Kawada- cho,Shinjuku,Tokyo,Japan . 01993bytheAmericanCollegeofCardiology Arte ATSUMOTO,MD,MASAS ISGUCI-II,MD, UI AI,MD,KAZUOMMMA,MD Y"I S1( 959 dilation (5 .4years) .Theintervalbetweenoperationand Math -r'_1 thesuccessfuldilationgroup(2 .4years)wassignificantly s, thatintheunsuccessfuldilationgroup(4 .6years) .In13pwele ._s whounderwentballoonangioplasty<3.5yearsafteroperation, balloondilationwassuccessfulin92% .Theballoonlarteryratio wassignificantlygreaterinthesuccessfulthanintheunsuccessful dilationgroup .Aright ventricular/aortic pressureratioX0 .68 wasobservedin20patients,andreoperationwasnotindicatedin 10patients(50%).Therewasnodeath,butonepulmonaryartery rupturethatdidnotrequiresurgicalinterventionoccurred . Aneurysmaldilationofthepulmonaryarterywasobservedin threepatients . Conclusions . Thesedataindicatethatalthoughthesuccessrate ofballoonangioplastyforpulmonaryarterystenosisafterthe arterialswitchoperationislow(=50%),balloonangioplastycan bethefirsttherapeuticchoiceowingtothelowcomplicationrate andthepotentialbenefitoftheprocedure .Thesuccessratecanbe highifangioplastyisperformed<3 .5yeasafteroperationanda balloonofadequatesizeisused . (JAmCollCardiol 1993,22 :859®66) Methods Studypatients .Balloondilationwasperformedtorelieve supravalvularpulmonarystenosisafterthearterialswitch operationfortranspositionofthegreatarteriesin28pa- tients .Atotalof39stenoticlesionsweredilatedfrom December1988toSeptember1992(Table1) .Fifteenpatients hadanintactventricularseptum,and13hadasignificant ventricularseptaldefect .Twenty-onepatientsunderwent primaryarterialswitchoperation,andsevenhadundergone Blalock-Taussigshuntorpulmonaryarteryhanding,orboth, initiallyandthenunderwentanarterialswitchoperation later .Inourinstitute,mostpatientswithtranspositionofthe greatarterieswithintactventricularseptumunderwentthe two-stagearterialswitchoperationfrom1982to1988 .We performedfollow-upcatheterizations5to6yearsafterthe operationinthesepatients .Since1988wehaveperformed theprimaryarterialswitchoperationinmostpatientsduring thenewbornperiodandfollow-upcatheterizationsIto3 yearsaftertheoperation .Throughouttheseperiods,anterior translocationofthemainpulmonaryartery(theLecompte maneuver [6]) wasperformedinallpatients .Apantaloon- 0735-1097/9356M
Transcript of Balloon angioplasty for postoperative pulmonary artery ... · artery stenosis was 51% (20 of 39...

JACC Vol . 22 . No . 3September 1993:at59-fib
all l_
TOS IO NAKANISHI, MD, YASUTOSFII
MAKOTO NAKAZAWA, MD, YASUHA
Tokyo, Japan
Objectives . This study was designed to assess the success rateand determinants of success or failure of balloon angioplasty forpostoperative pulmonary stenosis in patients with transposition ofthe great arteries .
Background. Previous reports have suggested that pulmonarystenosis that develops nt" er the arterial switch operation is notlikely to be dilated .
Methods . Twenty-eight patients with transposition of the greatarteries underwent 39 balloon angioplasty procedures after thearterial switch operation . The mean age at dilation was 4 .5 ± 2.2years (range 0 .7 to 9.8), and the interval between operation andballoon dilation was 3.6 ± 1.8 years . The criterion of successfuldilation was a j50%® increase in predilation diameter or a ? 50%decrease in predilation pressure gradient . If the right ventricular/aortic pressure ratio decreased by ?0.2, so that the ratio became<0.68, reoperation was thought to be not indLated.
Results. The success rate of balloon angioplasty for pulmonaryartery stenosis was 51% (20 of 39 dilations) . The mean age atdilation in the group with successful dilation (3 .6 years) wassignificantly younger than that in the group with unsuccessful
Pulmonary stenosis occurs in 7% to 28% of cases after thearterial switch operation for transposition of the great arter-ies (1-4) . Balloon angioplasty has been attempted to relievethis lesion, but because balloon dilation is not usuallysuccessful, surgical treatment has been employed in mostcases (1,2,4) . Saxena et al . (5), who performed balloonangioplasty in five patients with no successful dilation,concluded that pulmonary artery stenosis after the arterial .switch operation is not likely to be dilated by balloonangioplasty . We reviewed our early results of 39 dilations in28 patients and tried to delineate the determinants of sLccessor failure of balloon angioplasty .
From the Department of Pediatric Cardiology and Pediatric Cardiovascu-lar Surgery, Heart Institute of Japan, Tokyo Women's Medical College,Tokyo, Japan .
Manuscript received October 29, 1992 ; revised manuscript receivedFebruary 22, 1993, accepted March 2, 1993 .
Address.for coeiespondence ; Toshio Nakanishi, MD, Pediatric Cardiol-ogy, Heart Institute of Japan, Tokyo Women's Medical College, 8-1 Kawada-cho, Shinjuku, Tokyo, Japan .
0 1993 by the American College of Cardiology
A rte
ATSUMOTO, MD, MASAS I S GUCI-II, MD,U I AI, MD, KAZUO M MMA, MD
Y "I S 1(
959
dilation (5 .4 years) . The interval between operation and Math - r'_1the successful dilation group (2 .4 years) was significantly s ,that in the unsuccessful dilation group (4 .6 years) . In 13 pwele ._swho underwent balloon angioplasty <3.5 years after operation,balloon dilation was successful in 92% . The balloonlartery ratiowas significantly greater in the successful than in the unsuccessfuldilation group . A right ventricular/aortic pressure ratio X0 .68was observed in 20 patients, and reoperation was not indicated in10 patients (50%). There was no death, but one pulmonary arteryrupture that did not require surgical intervention occurred.Aneurysmal dilation of the pulmonary artery was observed inthree patients .
Conclusions . These data indicate that although the success rateof balloon angioplasty for pulmonary artery stenosis after thearterial switch operation is low (=50%), balloon angioplasty canbe the first therapeutic choice owing to the low complication rateand the potential benefit of the procedure . The success rate can behigh if angioplasty is performed <3 .5 yeas after operation and aballoon of adequate size is used .
(J Am Coll Cardiol 1993,22 :859®66)
MethodsStudy patients . Balloon dilation was performed to relieve
supravalvular pulmonary stenosis after the arterial switchoperation for transposition of the great arteries in 28 pa-tients. A total of 39 stenotic lesions were dilated fromDecember 1988 to September 1992 (Table 1) . Fifteen patientshad an intact ventricular septum, and 13 had a significantventricular septal defect . Twenty-one patients underwentprimary arterial switch operation, and seven had undergoneBlalock-Taussig shunt or pulmonary artery handing, or both,initially and then underwent an arterial switch operationlater. In our institute, most patients with transposition of thegreat arteries with intact ventricular septum underwent thetwo-stage arterial switch operation from 1982 to 1988 . Weperformed follow-up catheterizations 5 to 6 years after theoperation in these patients . Since 1988 we have performedthe primary arterial switch operation in most patients duringthe newborn period and follow-up catheterizations I to 3years after the operation . Throughout these periods, anteriortranslocation of the main pulmonary artery (the Lecomptemaneuver [6]) was performed in all patients . A pantaloon-
0735-1097/9356M

860 NAKANISHI ET AL .
JACC Vol . 22 . No . 3ANGIOPLASTY FOR PULMONARY STENOSIS AFTER ARTERIAL SWITCH
September 1993 :859-66
Table 1 . Clinical Summary and Hemodynamic Data
*Diameter of first balloon + Diameter of second balloon = Effective balloon diameter . tAge at reoperation (reop) excluded. tSignificantly different from thevalue in the unsuccessful dilation group. BT = Blalock-Taussig shunt ; LPA = left pulmonary artery ; MPA = main pulmonary artery ; PAB = pulmonary arterybanding ; Pt = patient ; RPA = right pulmonary artery ; VaIv = valvular .
shaped patch (7) (n = 8), two U-shaped patches (n = 10), tworound patches (n = 3), one round patch and one U-shapedpatch (8) (n ~ 5) or a triangular patch (Aubert technique (9])(n = 2) of preserved bovine pericardium were used to closeboth coronary artery sites and enlarge the neopulmonaryroot. The mean age at dilation was 4 .5 ± 2.2 years (range 0."1
Group A : Balloon Dilation Unsuccessful
to 9.8), and the interval between operation and balloondilation was 3 .6 ± 1 .8 years (range 0 .7 to 8.2) . In threepatients, balloon angioplasty was performed for the pulmo-nary artery stenosis developed after reoperation, which hadbeen performed to relieve right ventricular outflow obstruc-tion using a patch of preserved bovine pericardium .
I2
3/PAB4/PAB
5/PAB + BT678910It12/PAB + BT13/PAB + BT14/PAB + BT15
l6tPAB + BTMeanSD
6 mo2 mo
12 mo12 mo
7 ma6 mo9 mo1 mo2 mo1 mo3 yr (reop)12 moIt mo5 mo17 mo12 mo9 .8 mo (7.7 mot)8 .3 mo (4.9 mot
4 .13 .9
4 .85.7
5 .73 .34 .93 .96.34 .37 .79.26.36 .15 .36 .45 .41 .2
MPA (4.8)MPA (6 .9)RPA (6 .0)LPA (4 .8)MPA (9.2)MPA (8.0)RP. 1(7 .0)RPA (3 .5)MPA (9,0)MPA (6.8)MPA (5 .5)MPA (7.0)MPA (10)MPA (9.0)MPA (5 .2)LPA (3 .8)RPA (5 .1)Valv (13)Va1v (14)
(6.6)(1 .9)
1015
15
15
201010151820182020
20+10=25 .112 + 10 = 1810 f 0=20.6
2015
15
5 .27 .76 .04 .810 .48 .07 .04 .313 .08 .75 .5
8 .511 .19.06.64 .65,5
7 .42 .5
1376510135555
10115485070904070(4)209026575728
973510123452107527356073245033149014404124
Group B : Balloon Dilation Successful
17 6 yr (reop) 9 .8 MPA (8 .7) 10 + 15 w 20.6 13 .5 70 3218 10 days 2 .2 RPA (3 .7) 10 + 12 = 18 4,9 68 24
LPA (2 .0) 12 A 85 2319 10 days 1 .9 RPA (3 .7) IS 9 .2 40 8
LPA (5 .5) 10 + 15 = 20 .6 12 .3 30 020 9 mo 7 .9 MPA (7 .2) 20 8 .9 75 3521 13 days 2 .7 LPA (3 .5) 12 + 12 = 19 .6 6 .2 24 1222 21 days 2 .4 RPA (2 .5) I0 4 .6 35 2823 14 days 3 3 LPA (2 .8) 8+8=13.1 6.0 36 1024 13 days 0 .7 RNA (3 .2) 12 6.6 45 0
LPR (2.3) 12 5 .8 5e 025 26 days 1 .5 RPA (4.2) IS 16.1 10 0
Valv (8.8) 15 70 1026 I I days 1 .1 MPA (6.2) 20 11 .0 65 16
RPA (6 .4) 20 11 .3 24 1127 15 days 3.2 MPA (7.1) 20 20.7 20 10
RPA (5.4) 20 11 .0 22 2LPA (6.0) 20 11 .0 27 2
28 17 days 3.4 MPA (8.3) 15+I5=24.5 13.8 26 814 f yr (reop) 6.4 '(PA 0A 12 + 0 = 22 .1 12 .2 38 20Mean 12 mo (1 .3 mott) 3.6t (5. M 9 .9 42 13tSD 27 mo (2.6 mot 2.7 (2.10) 4 .4 22 11
Age at Location of Balloon Diameter Pressure Gradient (mm Hg)Pt Nod Dilation Stenosis Diameter After Dilation
Previous Operation Age at Switch (yr) (mm) (mm) (mm) Before Dilation After Dilation

JACC Vol . 22, No . 3September 1993 :859-66
Dilation technique . After standard premedication, vascu-lar access was established percutancoosly, usually usingfemoral vessels . In three patients who had bilateral ileofem-oral vein thrombosis, venous access was established usingan internal jugular vein . A catheter was advanced to measureright- and left-sided hemodynamic variables . Cardiac outputwas measured using a thermodilution method A smallcatheter was placed in the descending aorta to monitor bloodpressure. Angiograms were performed in the pulmonaryartery and the right ventricle . The decision to undertakeballoon angioplasty was made if angiography showed anarrowed segment with a pressure gradient ?20 mm Hg .This criterion was set tentatively, on the basis of ourexperience in one patient with a pros urc gradient of20 mm Hg who developed complete obstruction of the leftpulmonary artery without balloon angioplasty (see Fig . 5) .
Stenotic segments and the pulmonary annulus were mea-sured using a I -cm grid . An end hole catheter was positionedpast thQ stenosis in the pulmonary artery, and an 0 .035-in .(0.089 cm) or 0 .038-in . (0 .096 cm) exchange wire was passeddistally as far as possible into the lungs . After removal of thecatheter, the angioplasty catheter (Medi-tech or Mansfield)was introduced through a sheath . The initial balloon size waschosen to be two to four times the diameter of the stenosedsegment, not exceeding 1 .7 times the pulmonary annulusdiameter (10) . The balloon was inflated until the maximalsafe pressure recommended by the manufacturers wasreached . The full inflation ranged from 5 to 10 s, and three tofour dilations were usually performed for each stenosis . Ineach patient was multiple stenosis, more than one vessel wasusually dilated ai the same catheterization . After dil",ations,the right and left hemodynamic variables were measuredagain, and angiograms were performed in the pulnonaryartery or the right ventricle, or both .
Successful angioplasty was defined arbitrarily as 1) a2t50% increase in the predilation diameter of the narrowedsegment on angiography, or 2) a >50% decrease in the
NAKANISHI ET AL .ANGIOPLASTY FOR PULMONARY STENOSiS AFTER ARTERIAL SWITCH
8-61
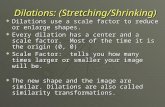
Figure 1, Anteroposterior pulmonary artencgq -am i~4 a 1-year oldpatient (Patient 19) demonstrates right (block triangle), aeR (W,-?«:Akarrowhead) and main (open arrowhead) pulmonary artery stenosis(A) and enlargement after balloon dilation (B) . An intimal or medialtear was visible after balloon dilation .
pressure gradient across the narrowed segment, using thecriteria of Zeevi et al . (4) .
The clinical impact of balloon angioplasty was studied ;postponement of reoperation was the only benefit for thepatients in the present study . If the systolic right ventricular/aortic pressure ratio decreased by `=l) .2, so that the ratiobecame <0.68, reoperation was thought to be not indicated .
Statistical analysis. Results were expressed as meanvalue ± SD. Comparison of two group means were per-formed using the Student i test or the Wilcoxon rank-sum test . The balloon/artery ratios in the groups withsuccessful and unsuccessful dilation were compared usingthe Wilcoxon rank-sum test . For analysis of group com-parisons we used a chi-square contingency analysis forcategoric variables Significance was defined as a p value <0.05 . For the success rates, the 95% confidence limits areshown .
ASKS
Successful dilation . Thirty-nine stenotic segments weredilated in 28 patients . The average increase in stenosisdiameter was 59 ± 63%, and the diameter increased X50 in19 segments. On the basis of the criteria, 13 (46%) of 28patients (confidence limits [CL] 27%, 66%) (20 [51%] of 39segments [CL 35%, 67%]) had successful dilation (Table 1,Fig. I to 3) .
A right ventricular/aortic pressure ratio X0 .68 was ob-served in 20 patients . This ratio decreased >0 .2, so that itbecame <0 .68 (clinical success) in 10 (50%) of these 20patients (CL 27%, 73%) . In the group with unsuccessful

862 NAKANISHL ET AL .ANGIOPLASTY FOR PULMONARY STENOSIS AFTER ARTERIAL SWITCH
September 1993 :859-66
Pore 2. Anteroposterior pulmonary artenogram in a 3-year oldchild (Patient 27) . Although stenosis is not clearly visualized, thecineangiogram showed stenosis at both sides of the bifurcation(
ai^rows) and at the main pulmonary artery (blot him*) (A)and enlargement after balloon dilation (s) . Aneurysmal dilation ofthe main pulmonary artery was observed,
dilation, the right ventricularlaortic pressure ratio beforedilation (0.86 ± 0.28, n - 16) did not change significantlyafter dilation (0.71 ± 0 .26). In contrast, in the group withsuccessful dilation, the right ventricular/aortic pressure ratiodecreased from 0 .76 ± 0.17 before dilation (n = 13) to t.49 ±0.10 after dilation .
Dele t of success. The age at arterial switch opera-tion or reoperation in the successful dilation group (9.8months) was not significantly different from that in the groupwith unsuccessful dilation (12 months, Table 1) ; however,balloon
ioplasty was successful in all patients who hadunder .one arterial switch operation in the newborn period .The success rate (100%, CL 69%, 100%) was significantlyhigher than that (16%, CL 3%, 40%) in patients who hadundergone the switch operation after the newborn period .
IACC Vol . 22 . No. 3
The age at balloon dilation in the group with successfuldilation (3 .6 years) was significantly younger than that in thegroup with unsuccessful dilation (5 .4 years, Fig . 4). Theinterval between arterial switch operation and balloon dila-tion in the group with successful dilation (2 .4 years) wassignificantly less than that in the group with unsuccessfuldilation (4 .6 years, Fig . 4) . In I1 patients aged <3.5 years atthe time of balloon dilation, balloon dilation was successfulin 91% (CL 64%, 100%). In 13 patients who underwentballoon angioplasty <3 .5 years after the arterial switchoperation, balloon dilation was successful in 92% (CL 04%,100%) .
The mean balloon/artery ratio was 333 ± 112% and wassignificantly greater in the group with successful dilation(381 ± 99%, n = 19) than in the group with unsuccessfuldilation (280 ± 106%, n = 17) . However, balloon size wasonly a partial determinant of success or failure of balloonangioplasty, Of 18 dilations perforated using a balloon sizex300%© of that of the stenotic artery, the balloon size in thegroup with successful dilation (386 ± 61%, n = 14) was notsignificantly different from that in the group with unsuccess-ful dilation (364 ± 28%, n = 6) ; all 14 successful dilationswere performed >3 .5 years after operation and 6 unsuccess-ful dilations were performed >3 .5 years after operation . Thisobservation suggests that when the balloon size is similar,the success rate of balloon angioplasty performed relativelyearly after operation is higher . The pressure gradient beforeballoon angioplasty in the group with successful dilation wasnot significantly different from that in the group with unsuc-cessful dilation (Fig . 4), suggesting that the severity of thestenosis was similar in the two groups .
There were 16 stenoses at the anastomotic segment in themain pulmonary artery and 19 stenoses at the bifurcation .There was no correlation between either the shape of thepatch used to reconstruct the neopulmonary artery andthe site of the stenosis or between the shape of the patch andthe success rate. The success rate of balloon angioplasty forbifurcation stenosis (74%, CL 49%, 91%) was significantlyhigher than that for main pulmonary artery stenosis (31%,CI. 11%, 59%). The success rate for left pulmonary arterystenosis (75%, CL 35%, 97%) was not significantly differentfrom that for right pulmonary stenosis (64%, CL 30%0, 89%) .Left branch pulmonary artery stenosis due to compressionby a dilated aortic root, which was observed in one patient(Patient 13), could not be dilated. Balloon valvuloptasty wassuccessful in one of three patients with valvular stenosis .
Unusaal approach . Of three patients who underwent bal-loon angioplasty using an internal jugular vein, the ballooncatheter could be manipulated across the stenosis in allthree, and balloon dilations were successful in two . Thesetwo patients iad an intramural left coronary artery arisingfrom the posterior sinus (type 5a of Shaher and Puddu'sclassification [11]) and had undergone the arterial switchoperation and coronary artery rerouting using the tee .Iniqueof Aubert et al. (9), creation of an aortopulmonary windowand an intrapulmonary tunnel to the coronary ostia . Balloon

JACC Vol . 22, No . 3September 1993:959-66
Figure 3 (alcove). Anteroposterior pulmonary ii .leriograin in an8-inonth old patient (Patient 24) demonstrates stenosis at both sidesof the bifurcation before dilation (lyre) and enlargement after balloondilation (Post) .
V(00N4)(0C:0
Successful
NAKAIRSHI ET AL .
@63ANGBOPLASTY FOR PULMONARY STENOStS AFTER ARTERIAL SIVETCH
a
Successful
Unsuccessful
Successful
Unsuccessful
Sol
0
0
000
OB 4)0090
Figure 4 (below). Age at balloon dilation, interval after operation,balloon size and pressure gradient in the groups with successfuland unsuccessful dilation . Bars are mean value ± SD. Age atdilation and interval after operation in the group with successfuldilation were significantly less than in the group with unsuccessfuldilation . Balloon size was significantly greater in patients withsuccessful than in those with unsuccessful dilation . Pressure gradi-ent before balloon dilation was similar in the two groups .
Is,
I
0
0
a9L
Qg
Go
a
0
i
09
0r-
Unsuccessful
Successful
Unsuccessful

864 NAKANISHI ET AL.
JACC Vol . 22, No. 3ANGIOPLASTY FOR PULMONARY STENOSIS AFTER ARTERIAL SWITCH
September 1993 :859-66
dilation could be performed without complication of coro-nary artery compression in these patients .
Complications. There were no deaths . In one patient(Patient 28), the pulmonary artery ruptured at the bifurca-tion. Although the mediastinum widened immediately, nei-ther hypotension c or a decrease in hematocrit was observed,and the patient did not require surgical intervention . Thepulmonary artery was dilated aneurysmally in three patients(Patients 19, 25 and 27), and an intimal tear was visible on acineangiogram in Patient 19 .
Discusslorn
Sucem rate . Pulmonary stenosis occurs in 7% to 28% ofpatients after the arterial switch operation for transpositionof the great arteries (1-4) . Balloon angioplasty has beenattempted to relieve this lesion, but the success rates havenot been high . Zeevi et al. (4) reported that balloon angio-plasty was successful in only one of five patients . Saxena etal . (5) performed balloon angioplasty in five patients with nosuccess . They concluded that pulmonary artery stenosis thatdeveloped after the arterial switch operation is not likely tobe dilated by balloon (5) . In the present study the pulmonaryartery stenosis after arterial switch operation could be di-lated and the success rate was about 50%, which is similar tothe success rate for angioplasty for pulmonary stenosis ofother causes (12,13) .
Age. Ring et al . (14) suggested that the success rate forballoon pulmonary artery angioplasty is higher in youngerthan in older children . Similarly, the success rate in ourstudy was higher in patients aged <3 .5 years . Furthertnow,the success rate was higher if angioplasty was performedrelatively early (<3 .5 years) after operation (Fig. 4) . Saxenaet al. (5) performed balloon angioplasty in patients <3 .5 yearsold and <3 .5 years after operation in four of five patients . Thereason for the low success rate in the report of Saxtna et al . (5)is not clear, but they used a relatively small balloon size (<3times the stenosis diameter) in these patients .
Ten of 13 patients in the group with successful dilationhad undergone an arterial switch operation in the newbornperiod. How the age at the arterial switch operation influ-ences the success rate of balloon angioplasty is not clear. Inour institute, the patients who had undergone arterial switchoperation in the newborn period underwent follow-up cath-eterization relatively early after the operation. Because ofthis institutional bias, it was not possible to separate the ageat the switch operation from other variables, such as age atballoon dilation and the interval between operation andballoon dilation, as a determinant of the success rate ;however, in one patient (Patient 14), balloon angioplastyPerformed at 6.1 years of age (5 .6 years after the operation)was not successful, but the stenosis at the same site thatdeveloped after a reoperation was dilated successfully 5months after the reoperation . From this experience, wethink that the interval between or-.ration and balloon dila-
tion, rather than age at operation, is important as a determi-nant of the success or failure of the procedure .
Balloon size. In agreement with previous reports (12,13),a greater balloon size/stenosis ratio was associated with ahigher success rat . In the present study, no balloon angio-plasty using a balloon/stenosis ratio <230% was successful(Fig . 4). We currently choose a balloon size at least threetimes larger than the stenotic segment. Of 20 dilationsperformed using a balloon a300% of the stenotic artery,balloon size did not differ significantly between the groupswith successful and unsuccessful dilation, suggesting thatballoon size is not a single determinant of success or failureof balloon angioplasty .
Operation method . In patients reported by Saxena et al .(5), autologous pericardium or preserved bovine pericardiumWas used to reconstruct a neopulmonary artery during thearterial switch operation . We also used the preserved bovinepericardium in the present series . The operative technique(Lecompte maneuver [6D was similar throughout the studyperiod, except that the shape of the patch used to recon-struct the neopulmonary artery was different in each patient(a pantaloon-shaped patch, U-shaped patches or roundpatches). However, there was no correlation between theshape of the patch and the site of the stenosis or between theshape of the patch and the success rate . Whatever the shapeof the patch, the main pulmonary artery stenosis was ob-served at the anastomosis site and the bifurcation stenosis atthe site of left or right pulmonary angioplasty, or both .Therefore, it is unlikely that the success or failure of balloonangioplasty in the present study is dependent on the opei'a-live method . However, we did not perform balloon angio-plasty for the pulmonary stenoses that developed afterpulmonary artery reconstruction without using prostheticmaterials (15) . If the pulmonary stenosis is due to hypoplasiaresulting from "tension" on the anastomosis, balloon angio-plasty may be less effective, as suggested by Zeevi et al . (4) .
Of 16 patients with unsuccessful dilation, 7 had under-gone pulmonary artery banding (Table 1) . Because thesepatients also underwent balloon angioplasty S to 6 years afterthe arterial switch operation, it is difficult to determinewhether the previous pulmonary artery banding resulted inthe angioplasty failure . However, this possibility is unlikelybecause a neopulmonary artery was reconstructed afterpulmonary artery debanding in a similar fashion to that in thepatients without pulmonary artery banding .
Site of stenosis . In the present report, the success rate ofballoon dilation for bifurcation stenosis was higher than thatfor main pulmonary artery stenosis . However, this differ-ence in success rate is probably due to the fact that many ofour patients with main pulmonary artery stenosis underwentballoon angioplasty >3 .5 years after the operation . Becausethe stenotic segm°nt in the main pulmonary artery lies closeto the pulmonary valve, a balloon diameter >1 .7 times thediameter of the pulmonary annulus was not used in thepresent study (10). Despite these technical limitations, the

JACC Vol . 22, No . 3September 0993 :859-66
Figure 5 . Unsuccessful balloon dilation in a 5-year old patient (Patient14). A, Anteroposterior pulmonary arteriogram showing left pulmo-nary artery branch stenosis (open arrowhead), which was due to thedilated aorta, and mild right pulmonary artery stenosis (black triangle)at its bifurcation at age 5 months, immediately after arterial switchoperation. Pressure gradients of 20 and 10 mm Hg were noted aL theleft and right pulmonary arteries, respectively . B, Anteroposterioraortogram showing the dilated aorta . C, Anteroposterior right ven-triculogram showing obstruction of the left pulmonary artery andsevere stenosis of the right pulmonary artery (black arrow) at age 5years . Balloon angioplasty for right pulmonary artery stenosis was noteffective .
main pulmonary artery stenosis could be dilated if balloonangioplasty was performed <3 .5 years after operation .
Left pulmonary stenosis associated with dilated aorticroot could not be dilated . Although there are few patientswith this condition, it is unlikely that this type of stenosis canbe dilated by balloon . The result of balloon angioplasty forvalvular stenosis was also poor, mainly because of smallannular size and thick valvular tissue . Zeevi et al. (4) alsoreported the difficulty in dilating this type of stenosis .
Unusual approach . From our experience in three pa-tients, balloon angioplasty can be performed through aninternal jugular vein . In addition, we performed balloonangioplasty in two patients who underwent the arterialswitch operation using the method of Aubert et al . (9) .Initially we were concerned about compression of the in-
NAKANISHE ET AL,ANGIOPLASTY FOR PULMONARY STENOStS AFTER ARTERIAL SWITCH
trapulmonary tunnel in the coronary route during inflation ofthe balloon ; however, we encountered, no complicationsresulting from coronary compression . It seems , that pulmo-nary artery stenosis that develops after operation using theAubert technique (9) can be dilated safely .
Clinical impact . In previous studies, balloon angioplastywas reported to have no influence on the clinical care ofpatients with pulmonary stenosis after the arterial switchoperation (5,16) . In the present study, the right ventricularpressure decreased significantly, so that reoperation couldbe postponed in 9 of 19 patients whose right ventricularpressure was a-68% of left ventricular pressure . Thus, therewas a benefit from balloon angioplasty in about 5001o ofpatients who otherwise required reoperation ; however, wedo not know how long reoperation can be postponed by

866 NAKANISHI ET AL.
JACC Vol . 22, N . IANGIOPLASTY FOR PULMONARY STFNOSIS AFTER ARTERIAL SWITCH
September 9993 :859-6,
successful balloon angioplasty . The fate of pulmonary arterystenosis that is successfully dilated by balloon angioplastymust be determined in future studies .
Indications . We performed balloon angioplasty even inpatients with relatively mild pulmonary stenosis if there wasa pressure gradient >_20 mm Hg . In one patient (Patient 14)in the present series, left pulmonary branch stenosis wasmild immediately after operation, and no balloon angioplastywas performed at that time . A catheterization performed 5 .4years after the operation showed complete obstruction of theleft pulmonary artery and severe stenosis at the right pulmo-nary artery (Fig . 5) . Balloon angioplasty for the right pulmo-nary artery stenosis was not effective . Yam uchi et al . (3)also showed that the pulmonary artery stenosis after thearterial vitch operation progressed with age . From thesedata, in an attempt to prevent progression of the pulmonaryartery stenosis, we performed balloon angioplasty even for arelatively mild stenos -V- Long-term results of balloon angio-plasty for pulmonary artery stenosis after the arterial switchoperation are not known, and it remains uncertain whetherballoon angioplasty can indeed prevent the progression ofstenosis . However, because pulmonary artery stenosis canbe relieved if balloon angioplasty is performed early afteroperation, and balloon angioplasty becomes ineffective withage, we think that the procedure is indicated even forrelatively mild stenosis . If pulmonary artery stenosis can beestimated accurately with noninvasive methods, then theindication should be determined from the degree of stenosisand the patient's age or the interval from the operation .
Complications. In the present study, intimal tear wassometimes visible on cineangiography (Fig. 1). We do notthink that this in itself is a complication because Edwards etal . (17) showed that successful balloon angioplasty for pul-monary artery stenosis was associated with intimal andmedial disruption. Aneurysmal dilation of the pulmonaryartery was observed in three patients, Because the naturalhistory of the dilated segment of the pulmonary artery isunknown, we think that close observation of then patients isnecessary. There was one rupture of the pulmonary arteryduring balloon dilation . The rupture was not associated withlarger balloon size or other technical failures . Because thesite of angioplasty of the pulmonary artery is usually se-verely adhesive to the surrounding tissue, vessel rupturemay not necessarily result in severe hemorrhage .
Conclusions. Pulmonary stenosis after the arterial switchoperation can be dilated with a success rate of '50% . Ifballoon angioplasty is performed early after operation (<3 .5years), and an appropriate balloon size is used, the success
rate can be higher (-90% 1, . We consider balloon angioplastyto be a useful procedure in the management of pulmonarystenosis developed after arterial switch operation. However,long-term effects are unknown, and follow-up studies mustbe performed in the future .
References
I . Wernovsky G, Hou;en TJ, Walsh EP, et al . Midterm results after thearterial switch operation for transposition of the great arteries with intactventricular septum ; clinical, hemodynamic, echocr, :cliographic, and elce-trocardiogrsarhic delta. Circo ;ation 19118 ;77 :1333-48,
2 . Lupiuetti FM, Bove EL . Minich LL, et d . Intermediate-term survival andfunctional results after arterial repair for transposition of the greatarteries . J Thorac Cardiovasc Surg 1992 ;103 :421-7 .
3 . Yamaguchi M, Hosokawa Y, Imai Y, et al . Early and midterm results ofthe arterial switch operation for transposition of the great arteries inJapan . J . Thorne Cardiovasc Surd 1990 ;l0i 261--9 .
4. Zeevi B, Keane JF, Perry S'L Lock JE . Balltxan dilation of post-operative right ventricular u~aalow obstnrctions, a Am Coll Cardiol1990 ;14 :401-8 .
5 . Saxena A, Fong LV, Ogilvie BC, Keeton BR . Use of balloon diiatation totreat supravalvar pulmonary stenosis developing after anatomical correc-tion for complete transposition. Br Heart J 1990;64:15 c-5 .
6. Lecompte Y, Zannini L, Haaan E, et al. Anatomic correction of Irans-position of the great arteries . J Thorac Cardiovasc Surg 1931 :82 :629-31 .
7 . Idriss FS, Ilbawi MN, DeLeon SY, et al . Arterial switch in simple andcomplex transposition of the great arteries . J Thorac Cardiovase Surg1988;95 :29-35.
8 . Quacgebeur JM . Rohmer J, Ottenkamp J, et al . The art;rial switchoperation . J Thorac Cardiovasc Surg 1986 ;92 :361-84 .
9 . Aubert J, Pannetier A, Couvelly JP, Unal D, Rounault F, Delarue A .Transposition of the great in °ries ; New technique for anatomical correc-tion. Br Heart J 1978 ;40:204 .8.
10, Ring JC, Kulik'TJ . Burke HA . Lock JE . Morphologic changes induced bydilation of the pulmonary valve anulus with overlarge balloons in normalnewborn lambs . Am J Cardiol 1984 ;55 :210-4.
I I . Shaher RM, Puddu GC . Coronary arterial anatomy in complete transpo-sition of the great vessels . Am J Cardiol 1966 ;17:355-61 .
12. Kan JS, Marvin WJJ, Bass JL, Muster AJ, Murphy J . Balloon angio-plasty-branch pulmonary artery stenosis : results from the Valvuloplastyand Angioplasty of Congenital Anomalies Registry . Am J Cardiol 1990,65 :798-801 .
13. Rothman AR, Perry SB, Keane JF, Lock JE . Early results and follow-upof balloon angioplasty for branch pulmonary artery stenosis . J Am CollCardiol 1990 :15 :1109-17 .
14. Ring JC, Bass JL, Marvin W, el al . Management of congenital stenosis ofa branch pulmonary artery with balloon dilation angioplasty . J ThoracCardiovasc Surg I 5 ;90 :35-44.
15 . Pacifico AD, Stewart RW . Bargeron LM Jr. Repair of transposition of thegreat arteries with ventricular septal defect by an arterial switch opera-tion. Circulation 1983 ;68(suppl 11) :11-49-55 .
16 . Hosking MK . Thomaidis C, Hamilton R, Burrows PE, Freedom RM .Benson LN . Clinical impact of balloon angioplasty for branch pulmonaryarterial stenosis. Am J Cardiol 1992 ;69 :1467-70 .
17 . Edwards BS, Lucas RV, Lock JE, Edwards JE . Morphologic changes inthe pulmonary arteries after percutaneous balloon angioplasty fur puhuo-nary arterial stenosis . Circulation 1985 ;71 :195-201 .