Biology of EGFR Mutations and Acquired Resistance to EGFR TKIs

Preclinical Development
Inhibition of TGF-b Enhances the In Vivo Antitumor Efficacyof EGF Receptor–Targeted Therapy
Atul Bedi1,2,3, Xiaofei Chang1, Kimberly Noonan2, Vui Pham1, Rishi Bedi1, Elana J. Fertig2,Michael Considine2, Joseph A. Califano1,3, Ivan Borrello2,3, Christine H. Chung2,3,David Sidransky1,2,3, and Rajani Ravi1,2
AbstractEGF receptor (EGFR)–targeted monoclonal antibodies (mAb), such as cetuximab, execute their antitumor
effect in vivo via blockade of receptor–ligand interactions and engagement of Fcg receptors on immune effector
cells that trigger antibody-dependent cell-mediated cytotoxicity (ADCC).We show that tumors counteract the
in vivo antitumor activity of anti-EGFR mAbs by increasing tumor cell-autonomous expression of TGF-b. We
show that TGF-b suppresses the expression of key molecular effectors of immune cell–mediated cytotoxicity,
including Apo2L/TRAIL, CD95L/FasL, granzyme B, and IFN-g . In addition to exerting an extrinsic inhibition
of the cytotoxic function of immune effectors, TGF-b–mediated activation of AKT provides an intrinsic EGFR-
independent survival signal that protects tumor cells from immune cell–mediated apoptosis. Treatment of
mice-bearing xenografts of human head and neck squamous cell carcinoma with cetuximab resulted in
emergence of resistant tumor cells that expressed relatively higher levels of TGF-b compared with untreated
tumor-bearing mice. Although treatment with cetuximab alone forced the natural selection of TGF-
b–overexpressing tumor cells in nonregressing tumors, combinatorial treatment with cetuximab and a
TGF-b–blocking antibody prevented the emergence of such resistant tumor cells and induced complete tumor
regression. Therefore, elevated levels of TGF-b in the tumor microenvironment enable tumor cells to evade
ADCC and resist the antitumor activity of cetuximab in vivo. Our results show that TGF-b is a key molecular
determinant of the de novo and acquired resistance of cancers to EGFR-targeted mAbs, and provide a rationale
for combinatorial targeting of TGF-b to improve anti-EGFR–specific antibody therapy of EGFR-expressing
cancers. Mol Cancer Ther; 11(11); 2429–39. �2012 AACR.
IntroductionConcurrent chemoradiation for locally advanced head
and neck squamous cell carcinoma (HNSCC) is limited byits toxicity and the development of recurrent disease in30% to 40% of patients (1, 2). Efforts to improve thetreatment of HNSCC have targeted the EGF receptor(EGFR), a receptor tyrosine kinase that is overexpressedand aberrantly activated in almost all such neoplasms (3–5). Activation of EGFR signaling promotes tumor cell
proliferation and survival, and facilitates tumor angio-genesis (6, 7). Strategies to target EGFR have focused oneither EGFR tyrosine kinase inhibitors (TKI) or monoclo-nal antibodies (mAb) that specifically bind the extracel-lular domain of the receptor, such as the human–mousechimeric IgG1 mAb, cetuximab (8, 9). The direct effect ofEGFR-targeted mAbs on tumor cells involves specificblockade of EGFR signaling via interference with bindingof EGFR ligands to the extracellular domain of the recep-tor (10–12). In addition, the interaction of the Fc region ofan antibody to Fcg receptors on immune effector cells alsoinduces antibody-dependent cellular cytotoxicity (ADCC;refs. 12–16).
Treatment of patients with locoregionally advancedHNSCC with a combination of cetuximab and radiationimproved overall survival comparedwith radiation alone(17). With amedian follow-up of 54.0 months, the medianduration of overall survival was 49.0 months amongpatients treated with combined therapy and 29.3 monthsamong those treated with radiotherapy alone. However,the survival benefit from cetuximab was not uniformlyobserved across all patients. The beneficial effect of cetux-imab seemed to be preferentially evident in a subsetof patients with the typical characteristics of human
Authors' Affiliations: 1Division of Head and Neck Cancer Research,Department of Otolaryngology-Head and Neck Surgery; 2Department ofOncology, and 3Sidney Kimmel Comprehensive Cancer Center at JohnsHopkins, The Johns Hopkins University School of Medicine, Baltimore,Maryland
Note: Supplementary data for this article are available at Molecular CancerTherapeutics Online (http://mct.aacrjournals.org/).
Corresponding Authors: Rajani Ravi, Head and Neck Cancer ResearchDivision, Department of Otolaryngology-Head and Neck Surgery, 1550Orleans Street, Johns Hopkins University School of Medicine, CancerResearch Building II, Baltimore, MD 21231. Phone: 410-502-5153; Fax:410-614-1411; E-mail: [email protected]; and Atul Bedi, E-mail:[email protected]
doi: 10.1158/1535-7163.MCT-12-0101-T
�2012 American Association for Cancer Research.
MolecularCancer
Therapeutics
www.aacrjournals.org 2429
on January 15, 2021. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst August 27, 2012; DOI: 10.1158/1535-7163.MCT-12-0101-T

papillomavirus (HPV)-positive head and neck cancer(those with oropharyngeal cancer who were males andless than65years).After cetuximaband radiation therapy,patients with HPV-positive tumors showed a 60% 2-yearprogression-free survival (PFS) compared with only 23%PFS for patientswithHPV-negative tumors. Identificationof the molecular determinants of resistance to EGFR-targeted mAbs is crucial for improving their clinicalbenefit against HNSCC.
In this study, we find that patients with HPV-negativeHNSCC exhibit an abnormal elevation of serum levelsof TGF-b, a multifunctional cytokine that regulates cellgrowth and differentiation (18, 19). We show that TGF-bexerts an extrinsic inhibition of the cytotoxic functionof immune effectors while simultaneously providingan intrinsic EGFR-independent survival signal that pro-tects tumor cells from immune cell–mediated ADCC.Although the autonomous expression of TGF-b enablestumor cells to evade ADCC and resist the antitumoractivity of cetuximab in vivo, combinatorial treatmentwith cetuximab and a TGF-b–blocking antibody pre-vents the emergence of such resistant tumor cells andimproves the regression of HNSCC tumor xenografts.These results show that tumor cell expression of TGF-bis a key determinant of resistance to EGFR-targetedantibodies, and provide a rationale for combinatorialtargeting of TGF-b to improve the response of HNSCCand other EGFR-expressing cancers to cetuximab-basedtherapy.
Materials and MethodsMeasurement of serum levels of cytokines in patientswith HNSCC
Plasma samples were obtained from 47 patients withHNSCC and 10 patients with pleomorphic adenoma (asnon-HNSCC controls) who consented for the InstitutionalResearch Board-approved tissue banking protocol atJohns Hopkins University (Baltimore, MD). The serumlevels of TGF-b1, TGF-b2, TGF-b3, IL-10, IL-6, VEGF, IFN-a, IFN-g , IL-2, IL-12p70, IL-12p40/p70, IL-15, TNF-a,eotaxin, osteopontin, GCSF, SDF-1a, IL-4, GRO-a, andIL-8 were measured by multiplex bead assays usingreagents from Millipore and the Luminex 100 system inaccordance with the manufacturer recommended proto-cols (20). The HPV status was determined by in situhybridization using high-risk HPV-specific probes andp16 immunohistochemical staining as described (21).
Cell lines and cell culturesThe human HNSCC cell line UM-SCC-1 (designated
SCC-1 or SCC1) and its isogenic derivative 1CC8 (desig-nated SCC-1CC8 or 1CC8) were a kind gift from theUniversity of Michigan and maintained in 10% FBS inDulbecco’s Modified Eagle’s Medium (DMEM) supple-mented with 1% hydrocortisone. The erlotinib-resistantisogenic derivative of SCC-1 cells (designated SCC-1T)was generated via continuous exposure of SCC-1 cells toescalating concentrations of erlotinib over 6 months (22),
and maintained in culture medium supplemented witherlotinib. The humanHNSCC cell lines (HACAT,HO1u1,93VU147T, CAL27, SKN3, SCC25, HN5, SCC47, UNC7,SQ20B, HSC3, SQ9G, SCC6, HMS001, SCC61, FADU,SCC9, JHU22, SCC090, HSC2, JSQ3, SCC15, UNC10) andH358 lung carcinoma cells were cultured in their respec-tive recommended media. Cells were maintained in ahumidified atmosphere containing 5% CO2 at 37
�C. Eachcell line was authenticated using fingerprinting at theJohns Hopkins Genetic Resources Core Facility, and usedwithin 6 months of authentication.
Tumor xenografts and treatment of miceTumorxenograftsweregeneratedby implanting3� 106
tumor cells into the right flank of 5- to 6-week-old femaleathymicmice (nu/nu; National Cancer Institute, Bethesda,MD). Once the tumors reached a size of approximately100 mm3, the mice were randomized (8–10 mice pergroup), and treated with cetuximab [Imclone; 5 mg/kgintraperitoneally (i.p.) twice weekly for 4 weeks) and/orTGF-b antibody (Bioxcell; 5mg/kg i.p., once weekly for 4weeks). Tumor size was measured weekly and tumorvolumewas calculated using the formula (length�width� height). The animals were maintained in accordancewith guidelines of the American Association of Labora-tory Animal Care and a research protocol approved bythe Johns Hopkins University Animal Use and CareCommittee.
[18F]FDG-PET/CT imaging of miceThe night before imaging, mice were fasted for 12
hours. Water was provided ad libitum. On the day ofimaging, each mouse was injected with 250 mCi of[18F]FDG via the tail vein and imaged 45 minutes postinjection, using the Mosaic HP (Philips) small animalPET imagers with 15-minute static acquisition. A CTscan was done at the same time using the CT componentNanoSPECT/CT (Bioscan) in vivo animal imagers. Thestandard uptake values were computed by normalizingthe PET activity for each mouse to the injected dose andanimal weight and coregistered with CT images usingAmira 5.2.2 (Visage Imaging, Inc.).
Measurement of TGF-b in serum and tumor cellsupernatants
Serum was collected from mice by tail bleeding formeasurement of TGF-b using ELISA (R&D Systems).Tumor cells were extracted from xenografts using colla-genase digestion followed by RBC lysis, and cultured for48 hours in DMEM containing 0.1% FBS. Tumor cellsupernatants were evaluated by ELISA to determine theamount of TGF-b expressed by 1 � 106 cells per 24 hours.
Antibody-dependent cellular cytotoxicity assayHuman peripheral blood mononuclear cells (PBMC)
from normal donors were stimulated with recombinanthuman interleukin-2 (rh IL-2; 200 IU/mL; Chiron) inthe presence or absence of rhTGFb1 (5 ng/mL; R&D
Bedi et al.
Mol Cancer Ther; 11(11) November 2012 Molecular Cancer Therapeutics2430
on January 15, 2021. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst August 27, 2012; DOI: 10.1158/1535-7163.MCT-12-0101-T

Systems) in Adoptive Immunotherapy Media V (AIM V)containing low Ig FBS (Invitrogen) for 48 hours and usedas effectors. Tumor cells (5,000 cells/well) were culturedin a 96-well U-bottomed plate in growthmedium contain-ing low Ig serum for 24 hours before being used astargets. Target cells were washed and coated with cetux-imab 2 mg/mL and incubated for an hour in a CO2
incubator. PBMCs were washed, counted, and plated ontarget cells in a range of effector:target (E:T) ratios. Plateswere incubated for 3 to 4 hours and analyzed for ADCCusing an aCella-Tox kit (Cell Technology Inc.).
Reverse transcription and quantitative real-timePCRPBMCs were stimulated as described earlier (ADCC
assay) for 48 hours and RNA was extracted using TRIzol(Invitrogen) followed by RNAeasy kit cleanup (Qiagen).RNAwas reverse transcribed to cDNA using SuperscriptIII (Invitrogen) that then used as a template for real-timePCR. PCR primers were designed to amplify cDNA frag-ments approximately 150 to 250 bp in length using prim-er3 software. Gene products were amplified using iTaqSYBR green Supermix with Rox dye (Bio-Rad Laborato-ries) with the following amplification program for 40cycles: 95�C for 15 minutes, 60�C for 1 minute. All reac-tions were conducted in triplicate, with water controls,and relative quantity was calculated after normalizing toGAPDH expression. The following primer sequenceswere used: (i) NKG2D: 50-GGCTCCATTCTCTCACCC-A-30 (forward) and 50-TAAAGCTCGAGGCATAGAGT-GC-30 (reverse); (ii) granzyme A: 50-TCCTATAGATTT-CTGGCATCCTCTC-30 (forward) and 50-TTCCTCCAAT-AATTTTTTCACAGACA-30 (reverse); (iii) granzyme B:50-TCCTAAGAACTTCTCCAACGACATC-30 (forward)and 50-GCACAGCTCTGGTCCGCT-30 (reverse); (iv)Apo2L/TRAIL: 50-CCCCTGCTGGCAAGTCAA-30 (for-ward) and 50-TGAACTGTAGAAATGGTTTCCTCAGA-30 (reverse); (v) IFN-g : 50-GAAAAGCTGACTAATTATT-CGGTAACTG-30 (forward) and 50-GTTCAGCCATCA-CTTGGATGAG-30 (reverse); and (vi) GAPDH: 50-CAAC-TACATGGTTTACATGTTC-30 (forward) and 50-GCCA-GTGGACTCCACGAC (reverse). Expression of each spe-cific mRNA (gene) relative to GAPDH was calculatedbased on the threshold cycle (Ct) as 2�D(DCt), whereDðDCtÞ ¼ DCtgene � DCtGAPDH
.
Flow cytometric analysisPBMCs were stimulated as described earlier (ADCC
assay) for 3 days and stained extracellularly with anti-CD56 APC (BD Biosciences), anti-Apo2L/TRAIL PE, oranti-FAS-L PE (eBioscience) for 10 to 15 minutes at 4�C.The cells were washed twice and then run on the FACSCalibur (BD Biosciences) and evaluated with Cell Questsoftware.
Cell viability and drug sensitivity assayTumor cells were plated at a density of 3,000 per well in
96-well plates. The followingday, cellswere treatedwith 0
to 10 mmol/L erlotinib for an additional 72 hours. Cellviability was subsequently assayed using the MTT color-imetric assay. The plates were read using a SpectraMaxplate reader (Molecular Devices Corp.) at 570 nm with areference wavelength of 650 nm. A minimum of 6 wellswere tested for each erlotinib dose. In some experiments,tumor cells were pretreated with either rhTGFb1 orrhTGFb3 (5 ng/mL; R&D Systems) to evaluate the effectof TGF-b on their sensitivity to erlotinib. The effect ofTGF-b on the response of SCC47 cells to erlotinib wasevaluated after transfection with either 100 nmol/L AKTsiRNA or Control siRNA (Cell Signaling Technology) for48 to 72 hours.
Immunoblot analysisXenograft samples were homogenized in radioimmu-
noprecipitation assay (RIPA) buffer followed by sonica-tion. In some experiments, cells were plated at a density of500 per well in 6-well plates and cultured with eitherrhTGFb1 (5 ng/mL; R&D Systems) or TGFbRII-Fc (500ng/mL; refs. 23, 24) for 1 to 7 days before immunoblotanalysis. Cells were lysed in RIPA lysis buffer containingprotease inhibitors (Roche Diagnostic Systems) and phos-phatase inhibitor cocktail (Sigma-Aldrich). Lysate proteinconcentrations were determined by the Lowry proteinassay (Bio-Rad Laboratories). Equal amounts of proteinwere mixed with Laemmli sample buffer (62.5 mmol/LTris-HCl, pH 6.8, 2% SDS, 10% glycerol, 0.1 mol/L DTT,and0.01%bromophenol blue), runon4% to 12%NuPAGEgels and transferred to nitrocellulose membrane (Bio-RadLaboratories). The membrane was blocked with PBS sup-plemented with 0.1% Tween 20 and 5% nonfat milk for 1hour at room temperature, and probed with primaryantibody for 1 hour at room temperature or overnight at4�C followed by HRP-conjugated appropriate secondaryantibodies (Santa Cruz Biotechnology). The followingprimary antibodies were used: antibodies against EGFR,phospho-EGFR, AKT, phospho-AKT (Ser473), E-cad-herin, vimentin (Cell Signaling Technology), andanti–b-actin antibody (Sigma-Aldrich). Signals fromimmunoreactive bands were detected by enhancedchemiluminescence (GE Healthcare).
Statistical analysisDifferentially expressed cytokines were determined
comparing non-HNSCC controls versus HNSCC, HPV-positive versusHPV-negative, and collection at the timeofnew diagnosis versus recurrence diagnosis. Studentunpaired t tests were used for statistical analysis to com-pare each of the 2 groups. When comparing across cyto-kines, results with Benjamini–Hotchberg adjusted Pvalues (25) below 0.05 were considered significant. Whenmaking comparisons between classes for single cytokines,results with unadjusted P < 0.05 were considered signif-icant. All statistical analyses of cytokines were conductedusing R according to the script in Supplementary Infor-mation (SupplementaryMethods). Student unpaired t testwas used for all other statistical analyses between 2
Inhibition of TGF-b Improves Anti-EGFR Antibody Therapy
www.aacrjournals.org Mol Cancer Ther; 11(11) November 2012 2431
on January 15, 2021. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst August 27, 2012; DOI: 10.1158/1535-7163.MCT-12-0101-T

groups. Results with P < 0.05 were considered significant.Statistical analyses were conducted using GraphPadInStat version 3.0a for Macintosh (GraphPad Software).
ResultsPatientswithHPV-negativeHNSCCexhibit elevatedlevels of serum TGF-b
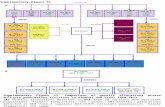
Plasma samples were procured from 47 patients withHNSCC (Supplementary Table S1) and 10 patients withpleomorphic adenoma (as benign non-HNSCC controls).Thirty-six samples were obtained at the time of newdiagnosis of HNSCC and 11 samples were obtained atthe time of recurrence.Measurement of serum levels of 20cytokines showed that TGF-b1 was significantly elevatedin patients with HNSCC compared with non-HNSCCcontrols (P ¼ 0.0085; Fig. 1A and Supplementary Fig.S1). A striking variation in serum levels of TGF-b1 wasalso noted among patients with HNSCC (Fig. 1A andSupplementary Table S2). Univariate analysis of samplesfromnewlydiagnosedpatients showed thatTGF-b1 levelswere significantly higher in HPV-negative HNSCC com-pared with non-HNSCC controls (P < 0.0003; Fig. 1B).Whereas patients with HPV-negative tumors showed anabnormal elevation of serum TGF-b1, patients with HPV-positive tumors exhibited relatively lower levels of TGF-b1 that were not significantly higher than non-HNSCCcontrols (Fig. 1B).
Tumor cell expression of TGF-b inhibits theexpression of cytotoxic effectormolecules in immunecells and suppresses their ability to inducecetuximab-mediated ADCC of tumor cells
TodeterminewhetherHNSCC cells express and secreteTGF-b into the tumor microenvironment, the amount ofTGF-b produced by 25 different human HNSCC cell linesin supernatants of tumor cells was measured by ELISA.Akin to the variable serum levels of TGF-b observed in
patients with HNSCC, HNSCC cell lines produced dif-fering amounts of TGF-b in vitro (Fig. 2A). Significantly,isogenic variants of the same cell line (SCC-1) expressedstrikingly different levels of TGF-b. Although parentalSCC-1 cells expressed low levels of TGF-b (37.8 pg/106
cells/24 h), derivatives of SCC-1 cells selected for resis-tance to cetuximab (SCC-1CC8) or the EGFRTKI, erlotinib(SCC-1T), expressed significantly higher levels of TGF-b[SCC-1CC8, 124.5 pg/106 cells/24 h (P ¼ 0.004); SCC-1T,550 pg/106 cells/24 h (P < 0.001); Fig. 2A]. To determinewhether tumor cell production of TGF-b influences theability of immune effector cells to induce cetuximab-mediated ADCC, cetuximab-coated tumor cells wereexposed to normal human PBMCs that were pretreatedwith rhIL-2 in the presence or absence of rhTGF-b1 for 48hours. HNSCC cell lines exhibited variable susceptibilityto cetuximab-mediated ADCC (Fig. 2B). Exposure ofPBMCs to rhTGF-b1 resulted in a marked decline in theirability to induce cetuximab-mediated ADCC of allHNSCC cell lines, including HPV-positive cell lines(SCC47, SCC90) andHPV-negative cell lines (SCC1, 1CC8,SCC-1T, SCC6, UNC10; Fig. 2B). Exposing PBMCs torhTGF-b resulted in a significant diminution in theirexpression of several cytotoxic effector molecules, includ-ing granzyme B, Apo2L/TRAIL, CD95L/FasL, and IFN-g(Fig. 2C and D). Real-time PCR showed that exposure torhTGF-b resulted in approximately 6-fold reduction in themRNA levels of granzyme B and Apo2L/TRAIL, as wellas approximately 4-folddecrease in levels of IFN-gmRNA(Fig. 2C). Similarly, flow cytometry analysis showed asignificant reduction of surface expression of Apo2L/TRAIL and CD95L/FasL on CD56þ NK cells after expo-sure to rhTGF-b (Fig. 2D). These data indicate that theautonomous production of TGF-b by tumor cells can exerta tumor cell-extrinsic inhibition of the cytotoxic functionof immune effectors that induce cetuximab-mediatedADCC.
Figure1. PatientswithHPV-negativeHNSCCexhibit elevated levels of serumTGF-b. A, heatmap showingdifferential serum levels of the indicatedcytokines inpatients with HNSCC and pleomorphic adenoma (noncancer control). B, differential levels of serum TGF-b1 in patients with HPV-negative HNSCC,HPV-positive HNSCC, and pleomorphic adenoma (noncancer control).
Bedi et al.
Mol Cancer Ther; 11(11) November 2012 Molecular Cancer Therapeutics2432
on January 15, 2021. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst August 27, 2012; DOI: 10.1158/1535-7163.MCT-12-0101-T

Autonomous expression of TGF-b activates AKT andenables EGFR-independent survival of tumor cellsThe SCC-1T cell line was derived by culturing SCC-1
cells in the presence of escalating concentrations of theEGFR TKI, erlotinib. Although SCC-1 cells exhibited adose-dependent reduction of viability in response to erlo-tinib, SCC-1T cells were relatively resistant to treatment(Fig. 3A). SCC-1T cells expressedmore than 10-foldhigherlevels of TGF-b compared with SCC-1 cells (Fig. 3B). Theelevation in autonomous expression of TGF-b in SCC-1Tcells was associated with increased phosphorylation ofAKT and epithelial–mesenchymal transition (EMT), asshowed by the loss of expression of E-cadherin andappearance of vimentin (Fig. 3C). Because tumor cellacquisition of an erlotinib-resistant phenotype was cose-lectedwith an increase in autonomous expression of TGF-b, we investigated whether exposure to TGF-b directly
enables EGFR-independent survival of tumor cells.Immunoblot analyses showed that treatment of EGFR-expressing H358 tumor cells with either rhTGF-b1 orrhTGF-b3 resulted in increased expression of phosphor-ylated AKT (p-AKT) that was apparent after 7 days ofexposure (Fig. 3D). The constitutive activation ofAKTwasassociated with TGF-b—induced EMT, as evidenced bythe appearance of vimentin and concurrent reduction inthe expression of E-cadherin (Fig. 3D). The acquisition ofan EMTphenotype by tumor cells after exposure to TGF-bwas attendedwith a concurrent decrease in the expressionof phosphorylated EGFR (p-EGFR; Fig. 3D). These effectsof TGF-bwere also confirmed in 3HNSCCcell lines [SCC6(HPV-negative), SCC47 (HPV-positive), and UNC10(HPV-negative)]. Exposure of HNSCC cell lines to TGF-b resulted in increased expression of p-AKT, EMT, anddecreased p-EGFR expression (Fig. 3E).
Figure 2. Tumor cell expression of TGF-b inhibits the expression of cytotoxic effector molecules in immune cells and suppresses their ability to inducecetuximab-mediated ADCC of tumor cells. A, differential levels of TGF-b produced by human HNSCC cell lines in tumor cell supernatants analyzed byELISA. B, comparative susceptibility of the indicated HNSCC cell lines to anti-EGFR mAb (cetuximab)-mediated ADCC induced by normal PBMCstimulated with rhIL-2 in the presence or absence of rhTGFb1 for 48 hours. C, TGF-b inhibits the expression of cytotoxic effector molecules in immuneeffector cells. Normal PBMCs were stimulated with rhIL-2 in the presence or absence of rhTGFb1 for 48 hours, and expression of the specific mRNA(granzyme B, Apo2L/TRAIL, and IFN-g ) was quantified by real-time PCR. D, TGF-b inhibits surface expression of Apo2L/TRAIL and CD95L/FasL on immuneeffector cells. Normal PBMCs were stimulated with rhIL-2 in the presence or absence of rhTGFb1 for 72 hours, and surface expression of Apo2L/TRAIL andCD95L/FasL on CD56þ NK cells were analyzed by flow cytometry.
Inhibition of TGF-b Improves Anti-EGFR Antibody Therapy
www.aacrjournals.org Mol Cancer Ther; 11(11) November 2012 2433
on January 15, 2021. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst August 27, 2012; DOI: 10.1158/1535-7163.MCT-12-0101-T

To determine whether the TGF-b–induced switch oftumor cells from an active EGFR/low p-AKT phenotypeto an inactive EGFR/high p-AKT phenotype rendersthem independent of EGFR-activated survival signals,HNSCC cell lines (SCC6, SCC47, and UNC10) or H358cells that were pretreated with either TGF-b1 or TGF-b3and their untreated counterparts (control) were exposedto graded concentrations of erlotinib (26).Although SCC6,SCC47, andH358 cells exhibited a dose-dependent reduc-tion of viability after treatment with erlotinib, pretreat-mentwith TGF-b rendered all 3 lines relatively resistant toerlotinib (Fig. 3F). We further established the importanceof AKT activation in TGF-b–mediated resistance to EGFR-targeted therapy using siRNA-mediated knockdown ofAKT in SCC47 cells (Fig. 3F and G). Treatment of SCC47cells with siRNA against AKT inhibited TGF-b–inducedelevation of p-AKT (Fig. 3G). siRNA-mediated loss ofAKT sensitized SCC47 cells to erlotinib and counteractedthe ability of TGF-b to confer resistance to erlotinib(Fig. 3F).
Treatment of tumor-bearing animals with cetuximabresults in the in vivo selection of resistant tumorcells with elevated expression of TGF-b andTGF-b–dependent activation of AKT
To investigatewhether autonomous expression of TGF-bmodulates the response of tumor cells to EGFR-targetedmAbs in vivo, we examined the effect of cetuximab ontumor xenografts comprising either SCC-1 cells or itsderivative, SCC-1CC8 (1CC8). Although the in vivogrowth of SCC-1 tumors was arrested by cetuximab(untreated vs. treated, P < 0.05), 1CC8 tumors wererelatively less responsive to the same treatment (untreatedvs. treated, P ¼ 0.09; Fig. 4A). However, cetuximab alonewas not sufficient to induce regression of either SCC-1 or1CC8 tumor xenografts. Because TGF-b inhibited cetux-imab-mediated ADCC of tumor cells in vitro, we investi-gated whether treatment of tumor-bearing mice withcetuximab results in the in vivo selection of resistanttumor cells that express higher levels of TGF-b. Tumorcells extracted from residual tumors in untreated or
Figure 3. Autonomous expression of TGF-b activates AKT and enables EGFR-independent survival of tumor cells. A, sensitivity of SCC-1 and SCC-1T cells tothe EGFR TKI, erlotinib. Cells were exposed to erlotinib for 72 hours, and cell viability was assayed using theMTT assay. B, differential expression of TGF-b bySCC-1 cells (blue) and its isogenic variant, SCC-1T cells (red), in tumor cell supernatants analyzed by ELISA. C, immunoblot analysis of phospho-AKT,AKT, E-cadherin, and vimentin in SCC-1 and SCC-1T cells showing increased phosphorylation of AKT and EMT in SCC-1T cells. D and E, in vitrotreatment of tumor cells with rhTGF-b results in activation of AKT, induction of EMT, and loss of EGFR activity. H358 cells (D) or the indicated HNSCCcell lines (E) treatedwith either rhTGF-b1or rhTGF-b3 for the indicated time and their untreated controlswere subjected to immunoblot analyses for expressionof AKT, phospho-Akt (Ser473), vimentin, E-cadherin, EGFR, and phospho-EGFR. F, TGF-b activates EGFR-independent AKT-mediated survival signals thatrender tumor cells relatively resistant to erlotinib. HNSCC cell lines (UNC10, SCC6, AKT siRNA- or control siRNA-transfected SCC47) or H358 cellsthat were pretreated with either TGF-b1 or TGF-b3 and their untreated counterparts (control) were exposed to the indicated concentrations of erlotinibfor 48 hours and subsequently assessed for cell viability. G, treatment of SCC47 cells with siRNA against AKT inhibits TGF-b–induced elevation ofp-AKT. Immunoblot analysis of p-AKT in SCC47 cells (with or without TGF-b for 48 or 72 hours) after transfection with either siRNA against AKT (siAKT)or control siRNA.
Bedi et al.
Mol Cancer Ther; 11(11) November 2012 Molecular Cancer Therapeutics2434
on January 15, 2021. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst August 27, 2012; DOI: 10.1158/1535-7163.MCT-12-0101-T

cetuximab-treated mice were cultured ex vivo, and theproduction of TGF-b in tumor cell supernatants wasmeasuredbyELISA. Explanted SCC-1 tumor cells derivedfrom residual nonregressed tumors after cetuximabtreatment expressed significantly higher levels of TGF-b(135 pg/106 cells/24 h) compared with either SCC-1cells derived from untreated tumor-bearing animals(40 pg/106 cells/24 h; P ¼ 0.01) or SCC-1 cells beforeinoculation intomice (37.8 pg/106 cells/24 h;P¼ 0.01; Fig.4B). Indeed, the elevated level of expression of TGF-b in
residual SCC-1 tumor cells derived from cetuximab-treated mice approximated that of residual 1CC8 cellsafter cetuximab therapy (P¼ 0.6; Fig. 4B). Consistent withthe increase in the autonomous expression of TGF-b,tumor-derived SCC-1 cells from cetuximab-treated ani-mals exhibited increased phosphorylation of AKT andreduced expression of E-cadherin, a marker of EMT (Fig.4C). Treatment of residual SCC1 or 1CC8 tumor cells witha TGF-b antagonist (TGFbRII-Fc) reversed the phosphor-ylation of AKT, indicating that tumor cell–derived TGF-b
Figure 4. Treatment of tumor-bearing animalswith cetuximab results in the in vivo selection of resistant tumor cellswith elevated expression of TGF-bandTGF-b–dependent activation of AKT. A, in vivo response of tumor xenografts of SCC-1 cells or its isogenic variant 1CC8 to treatment with EGFRmAb (cetuximab).Athymic (nu/nu) mice injected subcutaneously with SCC-1 or 1CC8 tumor cells were treated with cetuximab (5 mg/kg i.p. twice weekly � 3 weeks) or PBS(untreated control). Tumor volumewasmeasuredweekly. B, treatment with EGFRmAb (cetuximab) results in selection of tumor cells with higher autonomousexpression of TGF-b. Explanted tumor cells derived from tumors in untreated mice or from residual tumors after cetuximab treatment were cultured ex vivo,and the amount of TGF-b in cell supernatants was measured by ELISA. C, in vivo treatment with cetuximab forces selection of SCC1 tumor cells that exhibitautonomous TGF-b–dependent activation of AKT and EMT. Explanted tumor cells derived from tumors in untreated mice or from residual tumors aftercetuximab treatment were analyzed for expression of AKT, phospho-Akt (Ser473), and E-cadherin by immunoblot assays. D, TGF-b mediates EGFR-independent activation of AKT in tumor cells from cetuximab-treated animals. Explanted tumor cells derived from residual SCC1 and 1CC8 tumors aftercetuximab treatment were cultured for 24 hours in the presence or absence of a TGF-b antagonist (TGFbRII-Fc, 500 ng/mL), and analyzed for expression ofAKT and phospho-Akt (Ser473) by immunoblot assays. E, serum levels of TGF-b in naïvemice (nontumor bearing) and in SCC1- or 1CC8–tumor-bearingmicetreated with EGFR mAb (cetuximab), TGF-b antibody (TGF-b Ab) or a combination of EGFR mAb with TGF-b antibody.
Inhibition of TGF-b Improves Anti-EGFR Antibody Therapy
www.aacrjournals.org Mol Cancer Ther; 11(11) November 2012 2435
on January 15, 2021. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst August 27, 2012; DOI: 10.1158/1535-7163.MCT-12-0101-T

was responsible for EGFR-independent activation ofAKT (Fig. 4D). In accordance with the in vivo selection ofTGF-b–overexpressing resistant tumor cells in cetuximab-treated animals, serum levels of TGF-b were equallyelevated in SCC-1- and 1CC8–tumor-bearing mice aftercetuximab therapy, but were restored to that of na€�vemice after treatment with an antagonist TGF-b antibody(TGF-b antibody; Fig. 4E).
Inhibition of TGF-b improves the in vivo antitumorefficacy of cetuximab against tumor xenografts ofHNSCC cells
Because treatment with cetuximab resulted in theselection of TGF-b–overexpressing resistant tumor cells,we investigated whether inhibition of TGF-b with TGF-b antibody can improve the in vivo antitumor efficacy ofcetuximab against tumor xenografts of HNSCC cells.Consistent with the selection of TGF-b–overexpressingvariants of SCC-1 tumor cells in cetuximab-treated ani-mals, cetuximab alone was not sufficient to induceregression of either SCC-1 or 1CC8 tumor xenografts(Fig. 5A and B). However, combinatorial treatment ofmice with TGF-b antibody improved the antitumorefficacy of cetuximab against tumor xenografts ofSCC-1 cells as well as 1CC8 cells (Fig. 5A and B). Unlikecetuximab alone, combined treatment with cetuximaband TGF-b antibody resulted in regression of both SCC-1 and 1CC8 tumor xenografts (Fig. 5A and B). In animalsbearing 1CC8 tumor xenografts, treatment for 30 dayswith the combination of cetuximab and TGF-b antibodyresulted in significantly smaller tumors (mean � SEM ¼15 � 6 mm3) compared with cetuximab alone (mean �
SEM ¼ 109 � 11 mm3; P < 0.0001). Analyses of tumor-free survival by in vivo PET-CT imaging at day 50showed that cetuximab alone failed to induce completetumor regression in any animal bearing either SCC-1tumors (0/8) or 1CC8 tumors (0/10; Fig. 5C). In contrast,combined treatment with cetuximab and TGF-b anti-body resulted in complete regression of SCC-1 tumorsin 7 of 8 mice (87.5%) and 1CC8 tumors in 9 of 10 mice(90%; Fig. 5C). Treatment with TGF-b antibody alonedid not have any appreciable effect on the growth ofeither SCC-1 or 1CC8 tumor xenografts. These datashowed that combinatorial treatment with cetuximaband TGF-b antibody significantly improved tumor-freesurvival in comparison to either TGF-b alone or cetux-imab alone in mice bearing either SCC1 tumors (P <0.0001) or 1CC8 tumors (P < 0.0001). Therefore, inhibi-tion of TGF-b not only negated the relative de novoresistance of 1CC8 tumors to cetuximab, but also aug-mented the antitumor efficacy of cetuximab againstSCC-1 tumors. Moreover, there was no evidence oftoxicity in animals treated with either cetuximab aloneor the combination of cetuximab and TGF-b.
DiscussionThe mechanisms by which anti-EGFR antibodies,
such as cetuximab, execute their antitumor effect in vivoinclude blockade of receptor–ligand interactions thatstimulate tumor cell survival and growth and engage-ment of Fcg receptors on immune effector cells thattrigger ADCC of EGFR-expressing tumor cells (11,12, 15, 27). The importance of both these mechanismsto the in vivo efficacy of anti-EGFR mAbs is supported
Figure 5. Inhibition of TGF-b improves the in vivo antitumor efficacy of cetuximab against tumor xenografts of HNSCC cells. The 3 � 106 tumor cells wereimplanted into the right flank of female athymic mice (nu/nu) to generate tumor xenografts of SCC1 or 1CC8 cells. Once the tumors reached a size ofapproximately 100mm3, themice were treated with cetuximab (5mg/kg i.p. twice weekly for 4 weeks) and/or TGF-b antibody (5 mg/kg i.p., once weekly for 4weeks). A and B, tumor volume was evaluated weekly. C, in vivo PET-CT imaging analyses showing the comparative responses and tumor-free survival ofmice bearing HNSCC xenografts to treatment with either cetuximab alone, TGF-b antibody alone, or a combination of cetuximab and TGF-b antibody.
Bedi et al.
Mol Cancer Ther; 11(11) November 2012 Molecular Cancer Therapeutics2436
on January 15, 2021. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst August 27, 2012; DOI: 10.1158/1535-7163.MCT-12-0101-T

by previous studies that showed that the F(ab0)2 frag-ment of the anti-EGFR antibody 225 (on which cetux-imab is based) was able to reduce the in vivo growth ofA431 tumor cells with only 50% of the activity shown bythe intact antibody comprising a functional Fc domain(11). The crucial contribution of ADCC in mediating thein vivo antitumor activity of therapeutic mAbs is alsoevident from studies showing that the ability of theseagents to arrest growth of tumors in normal mice isimpaired in FcRg�/�mice that are deficient in activatingFc receptors (27). Although the antibody Fc regiontriggers the activation of immune effector cells, theconcomitant blockade of EGFR-mediated survival sig-nals in tumor cells by the EGFR-specific antibody mayalso serve to render tumor cells more susceptible toimmune effector cell-mediated death (28). The datapresented here indicate that tumors play an active rolein counteracting both these actions of anti-EGFR mAbsby increasing tumor cell-autonomous expression ofTGF-b (29).Our data show that tumor cell expression of TGF-b
can exert a 2-pronged inhibitory effect on cetuximab-mediated ADCC of tumor cells. We find that TGF-bsuppresses the expression of several key moleculareffectors of immune cell–mediated cytotoxicity, includ-ing Apo2L/TRAIL, CD95L/FasL, granzyme B, andIFN-g . In addition to exerting a tumor cell extrinsicinhibition of the cytotoxic function of immune effectors,TGF-b also promotes the activation of AKT (30), there-by providing an intrinsic EGFR-independent survivalsignal that protects tumor cells from the direct- andimmune cell–mediated cytotoxic effects of cetuximab orerlotinib. Our data indicate that treatment with cetux-imab results in the selection of tumor cells that expresshigher levels of TGF-b, thereby counteracting ADCCand limiting the efficacy of treatment. Conversely,combinatorial treatment with TGF-b–blocking antibodycounteracts the selection of TGF-b–overexpressingtumor cells and immune suppression in tumor-bearinganimals treated with cetuximab, thereby restoringADCC and enhancing the antitumor efficacy of cetux-imab in vivo. These results identify TGF-b as a keymolecular determinant of the de novo or acquired resis-tance of cancers to EGFR-targeted mAbs, and provide arationale for combinatorial targeting of TGF-b toimprove the antitumor efficacy of EGFR-specific anti-body therapy.Although TGF-b exerts a tumor-suppressive effect on
normal epithelial cells, tumor cells frequently becomerefractory to the growth inhibitory effect of TGF-b andacquire an ability to increase expression and secretion ofTGF-b (31–34). This switch enables tumor cells to lever-age the tumor promoting effects of TGF-b in the tumormicroenvironment to facilitate tumor progression, inva-sion, and metastasis via promotion of EMT in carcinomacells and suppression of immune responses (31–39).Many human cancers, including a majority of HNSCC,overexpress TGF-b, and the elevation of TGF-b is cor-
related with tumor progression, invasion, metastases,and poor prognosis. As such, the production TGF-b bytumor cells may be a frequent mechanism by whichcancers induce immune tolerance in the tumor micro-environment and evade elimination by cetuximab. TGF-b–mediated resistance to cetuximab is distinct frompreviously described mechanisms associated withreduced therapeutic efficacy of cetuximab, such asmutated EGFR variants, redundant autocrine, or para-crine signaling by other EGFR receptors or insulin-likegrowth factor receptor (IGF-1R), or constitutive activa-tion of either PI3K/AKT or Ras (40–45). The abnormalelevation of serum TGF-b in patients with HPV-negativeHNSCC may underlie the relatively lower benefit ofcetuximab-based therapy in these patients comparedwith that observed in patients with HPV-positiveHNSCC who exhibit relatively lower levels of TGF-b.Our studies suggest that the clinical efficacy of anti-EGFR antibodies against HNSCC and other EGFR-expressing cancers could be enhanced by strategies tosimultaneously sequester and counteract TGF-b in thetumor microenvironment (46–48).
Disclosure of Potential Conflicts of InterestDr. Califano is the Director of Research of the Milton J. Dance Head
and Neck Endowment. The terms of this arrangement are being managedby the Johns Hopkins University in accordance with its conflict of interestpolicies. Dr. Christine Chung received research funding from AstraZe-neca, Lilly Oncology and Bayer, and honoraria fromBristol-Myers Squibb,Amgen, Boehringer Ingelheim and Merck for educational lectures andserving on ad hoc scientific advisory boards. No potential conflicts ofinterest were disclosed by the other authors.
Authors' ContributionsConception and design: A. Bedi, X. Chang, K. Noonan, J. A. Califano, I.Borrello, D. Sidransky, R. RaviDevelopment of methodology:A. Bedi, X. Chang, K. Noonan, E. J. Fertig,C. H. Chung, R. RaviAcquisition of data (provided animals, acquired and managed patients,provided facilities, etc.): A. Bedi, X. Chang, K. Noonan, V. Pham, C. H.Chung, R. RaviAnalysis and interpretation of data (e.g., statistical analysis, biostatis-tics, computational analysis): A. Bedi, K. Noonan, R. Bedi, E. J. Fertig, M.Considine, J. A. Califano, I. Borrello, C. H. Chung, R. RaviWriting, review, and/or revision of the manuscript: A. Bedi, K. Noonan,R. Bedi, E. J. Fertig, M. Considine, J. A. Califano, C. H. Chung, R. RaviAdministrative, technical, or material support (i.e., reporting or orga-nizingdata, constructingdatabases):A.Bedi,V. Pham,R. Bedi, E. J. Fertig,M. Considine, C. H. Chung, R. RaviStudy supervision: A. Bedi, R. Ravi
AcknowledgmentsThe authors thank the Center for Infection and Inflammation Imaging
Research (CI3R—www.hopkinsmedicine.org/ci3r) and Dr. Sanjay Jainfor conducting PET/CT imaging analysis of mice.
Grant SupportThis work was supported by Grant NIH R01CA123277 from the
National Cancer Institute, NIH to A. Bedi and R. Ravi; National CancerInstitute SPORE (5P50CA096784-05) to J.A. Califano; NIH R01 DE017982to C.H. Chung; and NIH K25CA141053 to E.J. Fertig.
The costs of publication of this article were defrayed in part by thepayment of page charges. This article must therefore be hereby markedadvertisement in accordance with 18 U.S.C. Section 1734 solely to indicatethis fact.
Received February 2, 2012; revised July 3, 2012; acceptedAugust 9, 2012;published OnlineFirst August 27, 2012.
Inhibition of TGF-b Improves Anti-EGFR Antibody Therapy
www.aacrjournals.org Mol Cancer Ther; 11(11) November 2012 2437
on January 15, 2021. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst August 27, 2012; DOI: 10.1158/1535-7163.MCT-12-0101-T

References1. Forastiere AA, Goepfert H, Maor M, Pajak TF, Weber R, Morrison W,
et al. Concurrent chemotherapy and radiotherapy for organ pres-ervation in advanced laryngeal cancer. N Engl J Med 2003;349:2091–8.
2. Cooper JS, Pajak TF, Forastiere AA, Jacobs J, Campbell BH, SaxmanSB, et al. Postoperative concurrent radiotherapy and chemotherapyfor high-risk squamous-cell carcinoma of the head and neck. N EnglJ Med 2004;350:1937–44.
3. Arteaga CL. Overview of epidermal growth factor receptor biology andits role as a therapeutic target in human neoplasia. Semin Oncol2002;29:3–9.
4. Mendelsohn J. Targeting the epidermal growth factor receptor forcancer therapy. J Clin Oncol 2002;20:1S-13S.
5. Brashears J, Clyburn V, Shirai K. Introduction to molecular agents inthe treatment of head and neck cancer: focus on Cetuximab. CancerTherapy 2008;6:997–1004.
6. Huang SM, Bock JM, Harari PM. Epidermal growth factor receptorblockade with C225 modulates proliferation, apoptosis, and radio-sensitivity in squamous cell carcinomas of the head and neck. CancerRes 1999;59:1935–40.
7. Huang SM, Harari PM. Modulation of radiation response after epider-mal growth factor receptor blockade in squamous cell carcinomas:inhibition of damage repair, cell cycle kinetics, and tumor angiogen-esis. Clin Cancer Res 2000;6:2166–74.
8. Mendelsohn J, Baselga J. Status of epidermal growth factor receptorantagonists in the biology and treatment of cancer. J Clin Oncol2003;21:2787–99.
9. Graham J, Muhsin M, Kirkpatrick P. Cetuximab. Nat Rev Drug Discov2004;3:549–50.
10. Masui H,MoroyamaT,Mendelsohn J.Mechanismof antitumor activityin mice for anti-epidermal growth factor receptor monoclonal anti-bodies with different isotypes. Cancer Res 1986;46:5592–8.
11. Fan Z, Masui H, Altas I, Mendelsohn J. Blockade of epidermal growthfactor receptor function by bivalent and monovalent fragments of 225anti-epidermal growth factor receptor monoclonal antibodies. CancerRes 1993;53:4322–8.
12. Bleeker WK, Lammerts van Bueren JJ, van Ojik HH, Gerritsen AF,Pluyter M, Houtkamp M, et al. Dual mode of action of a human anti-epidermal growth factor receptor monoclonal antibody for cancertherapy. J Immunol 2004;173:4699–707.
13. Clynes R, Takechi Y, Moroi Y, Houghton A, Ravetch JV. Fc receptorsare required in passive and active immunity to melanoma. Proc NatlAcad Sci U S A 1998;95:652–6.
14. Ravetch JV, Bolland S. IgG Fc receptors. Annu Rev Immunol 2001;19:275–90.
15. Lopez-Albaitero A, Ferris RL. Immune activation by epidermal growthfactor receptor specific monoclonal antibody therapy for head andneck cancer. Arch Otolaryngol Head Neck Surg 2007;133:1277–81.
16. Takai T, Li M, Sylvestre D, Clynes R, Ravetch JV. FcR gamma chaindeletion results in pleiotrophic effector cell defects. Cell 1994;76:519–29.
17. Bonner JA, Harari PM, Giralt J, Azarnia N, Shin DM, Cohen RB, et al.Radiotherapy plus cetuximab for squamous-cell carcinoma of thehead and neck. N Engl J Med 2006;354:567–78.
18. Massague J. A very private TGF-beta receptor embrace. Mol Cell2008;29:149–50.
19. Groppe J, Hinck CS, Samavarchi-Tehrani P, Zubieta C, SchuermannJP, Taylor AB, et al. Cooperative assembly of TGF-beta superfamilysignaling complexes is mediated by two disparate mechanisms anddistinct modes of receptor binding. Mol Cell 2008;29:157–68.
20. Byers LA, Holsinger FC, Kies MS, William WN, El-Naggar AK, Lee JJ,et al. Serum signature of hypoxia-regulated factors is associated withprogression after induction therapy in head and neck squamous cellcancer. Mol Cancer Ther 2010;9:1755–63.
21. Ang KK, Harris J, Wheeler R, Weber R, Rosenthal DI, Nguyen-Tan PF,et al. Human papillomavirus and survival of patients with oropharyn-geal cancer. N Engl J Med 2010;363:24–35.
22. BenaventeS,HuangS,ArmstrongEA,ChiA,HsuKT,WheelerDL, et al.Establishment and characterization of a model of acquired resistance
to epidermal growth factor receptor targeting agents in human cancercells. Clin Cancer Res 2009;15:1585–92.
23. Komesli S, Vivien D, Dutartre P. Chimeric extracellular domain type IItransforming growth factor (TGF)-beta receptor fused to the Fc regionof human immunoglobulin as a TGF-beta antagonist. Eur J Biochem1998;254:505–13.
24. Muraoka RS, Dumont N, Ritter CA, Dugger TC, Brantley DM, Chen J,et al. Blockade of TGF-beta inhibits mammary tumor cell viability,migration, and metastases. J Clin Invest 2002;109:1551–9.
25. Benjamini Y, Yektueli D. The control of the false discovery rate inmultiple testing under dependency. Ann Stat 2001;29:1165–88.
26. Chen G, Kronenberger P, Teugels E, Umelo IA, De Greve J. Targetingthe epidermal growth factor receptor in non-small cell lung cancercells: the effect of combining RNA interference with tyrosine kinaseinhibitors or cetuximab. BMC Med 2012;10:28.
27. Clynes RA, Towers TL, Presta LG, Ravetch JV. Inhibitory Fc receptorsmodulate in vivo cytoxicity against tumor targets. Nat Med 2000;6:443–6.
28. Ravi R, Fuchs EJ, Jain A, Pham V, Yoshimura K, Prouser T, et al.Resistance of cancers to immunologic cytotoxicity and adoptiveimmunotherapy via X-linked inhibitor of apoptosis protein expressionand coexisting defects in mitochondrial death signaling. Cancer Res2006;66:1730–9.
29. Zou W. Immunosuppressive networks in the tumour environment andtheir therapeutic relevance. Nat Rev Cancer 2005;5:263–74.
30. Yi JY, Shin I, Arteaga CL. Type I transforming growth factor betareceptor binds to and activates phosphatidylinositol 3-kinase. J BiolChem 2005;280:10870–6.
31. Bierie B, Moses HL. Tumour microenvironment: TGFbeta: the molec-ular Jekyll and Hyde of cancer. Nat Rev Cancer 2006;6:506–20.
32. Lu SL, Herrington H, Reh D,Weber S, Bornstein S, Wang D, et al. Lossof transforming growth factor-beta type II receptor promotes meta-static head-and-neck squamous cell carcinoma. Genes Dev 2006;20:1331–42.
33. Koli KM, Arteaga CL. Complex role of tumor cell transforming growthfactor (TGF)-beta s on breast carcinoma progression. J MammaryGland Biol Neoplasia 1996;1:373–80.
34. Wang SE, Yu Y, Criswell TL, Debusk LM, Lin PC, Zent R, et al.Oncogenic mutations regulate tumor microenvironment throughinduction of growth factors and angiogenic mediators. Oncogene2010;29:3335–48.
35. Li MO, Wan YY, Sanjabi S, Robertson AK, Flavell RA. Transforminggrowth factor-beta regulation of immune responses. Annu Rev Immu-nol 2006;24:99–146.
36. Thomas DA, Massague J. TGF-beta directly targets cytotoxic T cellfunctions during tumor of immune surveillance. Cancer Cell 2005;8:369–80.
37. Trotta R, Col JD, Yu J, Ciarlariello D, Thomas B, Zhang X, et al. TGF-beta utilizes SMAD3 to inhibit CD16-mediated IFN-gamma productionand antibody-dependent cellular cytotoxicity in human NK cells. JImmunol 2008;181:3784–92.
38. Chow A, Arteaga CL, Wang SE. When tumor suppressor TGFbetameets theHER2 (ERBB2) oncogene. JMammaryGlandBiol Neoplasia2011;16:81–8.
39. Muraoka-Cook RS, Kurokawa H, Koh Y, Forbes JT, Roebuck LR,Barcellos-Hoff MH, et al. Conditional overexpression of active trans-forming growth factor beta1 in vivo accelerates metastases of trans-genic mammary tumors. Cancer Res 2004;64:9002–11.
40. Montagut C, Dalmases A, Bellosillo B, Crespo M, Pairet S, Iglesias M,et al. Identification of a mutation in the extracellular domain of theepidermal growth factor receptor conferring cetuximab resistance incolorectal cancer. Nat Med 2012;18:221–3.
41. Karapetis CS, Khambata-Ford S, Jonker DJ, O'Callaghan CJ, Tu D,Tebbutt NC, et al. K-ras mutations and benefit from cetuximab inadvanced colorectal cancer. N Engl J Med 2008;359:1757–65.
42. Viloria-Petit A, Crombet T, Jothy S, Hicklin D, Bohlen P, Schlaeppi JM,et al. Acquired resistance to the antitumor effect of epidermal growthfactor receptor-blocking antibodies in vivo: a role for altered tumorangiogenesis. Cancer Res 2001;61:5090–101.
Bedi et al.
Mol Cancer Ther; 11(11) November 2012 Molecular Cancer Therapeutics2438
on January 15, 2021. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst August 27, 2012; DOI: 10.1158/1535-7163.MCT-12-0101-T

43. Prenzel N, Fischer OM, Streit S, Hart S, Ullrich A. The epidermal growthfactor receptor family as a central element for cellular signal trans-duction and diversification. Endocr Relat Cancer 2001;8:11–31.
44. Perera AD, Kleymenova EV, Walker CL. Requirement for the vonHippel-Lindau tumor suppressor gene for functional epidermal growthfactor receptor blockade by monoclonal antibody C225 in renal cellcarcinoma. Clin Cancer Res 2000;6:1518–23.
45. Chandarlapaty S, Sawai A, Scaltriti M, Rodrik-Outmezguine V, Grbo-vic-Huezo O, Serra V, et al. AKT inhibition relieves feedback suppres-
sion of receptor tyrosine kinase expression and activity. Cancer Cell2011;19:58–71.
46. Yingling JM, Blanchard KL, Sawyer JS. Development of TGF-betasignalling inhibitors for cancer therapy. Nat Rev Drug Discov 2004;3:1011–22.
47. Akhurst RJ. Large- and small-molecule inhibitors of transforminggrowth factor-beta signaling. Curr Opin Investig Drugs 2006;7:513–21.
48. Arteaga CL. Inhibition of TGFbeta signaling in cancer therapy. CurrOpin Genet Dev 2006;16:30–7.
Inhibition of TGF-b Improves Anti-EGFR Antibody Therapy
www.aacrjournals.org Mol Cancer Ther; 11(11) November 2012 2439
on January 15, 2021. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst August 27, 2012; DOI: 10.1158/1535-7163.MCT-12-0101-T

2012;11:2429-2439. Published OnlineFirst August 27, 2012.Mol Cancer Ther Atul Bedi, Xiaofei Chang, Kimberly Noonan, et al.
Targeted Therapy−ReceptorEGF Antitumor Efficacy of In Vivo Enhances the βInhibition of TGF-
Updated version
10.1158/1535-7163.MCT-12-0101-Tdoi:
Access the most recent version of this article at:
Material
Supplementary
http://mct.aacrjournals.org/content/suppl/2012/11/09/1535-7163.MCT-12-0101-T.DC1
Access the most recent supplemental material at:
Cited articles
http://mct.aacrjournals.org/content/11/11/2429.full#ref-list-1
This article cites 48 articles, 17 of which you can access for free at:
Citing articles
http://mct.aacrjournals.org/content/11/11/2429.full#related-urls
This article has been cited by 9 HighWire-hosted articles. Access the articles at:
E-mail alerts related to this article or journal.Sign up to receive free email-alerts
Subscriptions
Reprints and
To order reprints of this article or to subscribe to the journal, contact the AACR Publications Department at
Permissions
Rightslink site. Click on "Request Permissions" which will take you to the Copyright Clearance Center's (CCC)
.http://mct.aacrjournals.org/content/11/11/2429To request permission to re-use all or part of this article, use this link
on January 15, 2021. © 2012 American Association for Cancer Research. mct.aacrjournals.org Downloaded from
Published OnlineFirst August 27, 2012; DOI: 10.1158/1535-7163.MCT-12-0101-T