
Awareness of dietitians about their role in providing...
63
Awareness of dietitians about their role in providing parenteral nutrition service in some Khartoum State hospitals – Sudan. ATHESIS SUBMITTED IN THE FULFILLMENT OF THE REQUIREMENTS OF M.Sc. DEGREE IN HUMAN NUTRITION AND DIETETICS. By:Reem Osama Yousif Ali Supervisor:Prof. Omer Musa Izzeldin December, 2016 The National Ribat University Faculty of Graduate Studies and Scientific Research
Transcript of Awareness of dietitians about their role in providing...
Awareness of dietitians about their role in
providing parenteral nutrition service in some
Khartoum State hospitals – Sudan.
ATHESIS SUBMITTED IN THE FULFILLMENT OF THE
REQUIREMENTS OF M.Sc. DEGREE IN HUMAN NUTRITION
AND DIETETICS.
By:Reem Osama Yousif Ali
Supervisor:Prof. Omer Musa Izzeldin
December, 2016
The National Ribat University
Faculty of Graduate Studies and Scientific Research
I
اآلية
بِّ ِزْدنِي ِعْلًما(قال تعالى: ) َوقُل رَّ
(114)طه

II
Dedication This work is dedicated to my parents who never stop
giving support and hope, to my brother, sisters, other
beloved family members and friends.
I also dedicate this research to my teachers all through
my learning milestone since childhood up to
postgraduates.
Special dedication to my husband.
Reem.

III
Acknowledgements All praise is to Allah the most merciful most compassionate.
I would like to express my deepest gratitude to the people
who have extended their assistance for the completion of
this dissertation.
I am heartily thankful to my supervisor Prof.Omer Musa for
his continuousencouragement, support and kind supervision.
I am grateful to my father Dr. Osama AlGibali for his
unlimitedand priceless consultations he always shares.
I thank Mss. Ikhlas Abdo for her direction and corrections.
Special thanks to all the dietitians who participated in
responding to the questionnaire for their cooperation.
IV
Abstract:
When balanced nutrition is needed for all human beings, it is more required and essential
when they get sick. It helps in keeping the cell metabolism integrity, energy, maintain
the immunity functions, and fasten cure. Occasionally sick patients cannot tolerate oral
or enteral feeding, in such situations parenteral nutrition (PN) is the most suitable
alternative route for nutritional support. Dietitians are fundamental personnel in the
nutrition support team that provide different routes of nutritional support.
This research has been prepared to recognize the dietitian’s awareness about parenteral
nutrition and their role in providing this service.
Fifty formulated questionnaire forms were distributed to the working dietitians in the
targeted hospitals. The majority of the dietitians who responded to the questionnaire
were nutritional bachelor graduates, about 60% of them with working experience of less
than three years.
The results of this research showed that 76% of responded dietitians defined PN
correctly and more than 80% of them have exposed in their clinical practice to patients
whom were in need of PN. All the responders were aware about the advantages of PN,
and 60% of them were mindful about the PN side effects. Eighty four percent of the
responders recommend usage of PN as an alternative therapy whenever oral and eternal
feeding are unfeasible. Most of the dietitians were aware of the different assessment
measurements, have the knowledge for calculating parenteral nutrition prescription but
only 30% had a chance to formulate or participate in formulating a PN prescription for
real patients. The unavailability of the multidisciplinary team, lack of the required
equipment and financial support, and associated complications found the fundamental
obstacles to the provision of long term PN service in Khartoum state hospitals.
The study concludes that although the targeted dietitians in Khartoum State hospitals-
Sudan have good knowledge and information about PN definition, indications, accesses,
and assessment measures, they do not have the enough knowledge and clinical exposure
that make them confident to provide the PN service. Establishing few models of
parenteral nutrition units in tertiary hospitals will be of great help in providing this
service, as well as providing the dietitian’s training in the area of parenteral nutrition.
V
ملخص البحث:
إذا كانت التغذية المتوازنة ضرورية لإلنسان الصحيح فإنها بالنسبة للمرضى أكثر حوجه ألنها تحافظ على كمالية
الخاليا ووظائف المناعة وتساعد على تعجيل الشفاء. في بعض األحيان ال يستطيع المرضى تناول غذاءهم استقالب
عن طريق التغذية الفموية أو المعوية )التغذية باألنابيب(، في هذه الحاالت تعتبر التغذية الوريدية هي الخيار البديل
فراد أساسيون في فريق الدعم الغذائي لتوفير الطرق المختلفة األمثل لتقديم الدعم الغذائي. يعتبر أخصائيو التغذية أ
من الدعم الغذائي.
أجريت هذه الدراسة للتعرف على وعي أخصائيو التغذية عن التغذية الوريدية ودورهم في تقديم هذا النوع من الدعم
الغذائي.
المستشفيات المستهدفة والذي وجد أن تم توزيع استمارة االستبيان على خمسين من أخصائيين التغذية العاملين في
% ذوو خبرة أقل من ثالث سنوات.60أغلبهم خريجو مستوى البكالوريوس، وحوالي
% 80% من اختصاصي التغذية عّرفوا التغذية الوريدية بشكل صحيح وأكثر من 76أكدت نتائج هذا البحث أن
للتغذية الوريدية. أّكد جميع المستجيبين لهذه الدراسة منهم صادفوا خالل عملهم السريري حاالت مرضية في حوجه
% قد يوصون 84% منهم لهم المعرفة حول التأثيرات الجانبية لها، وأن 60إيجابيات استخدام التغذية الوريدية و
ق باستخدام التغذية الوريدية كوسيلة بديلة للدعم الغذائي لحاالت المرضى الغير قادرين على تحمل التغذية عن طري
الفم أو األنابيب. وجدت الدراسة أن معظم أخصائي التغذية المشاركين يملكون المعرفة حول طرق التقييم المختلفة
% فقط كانت لهم الفرصة 30للمرضى تحت التغذية الوريدية، ولديهم المعرفة لحساب وصفة التغذية الوريدية ولكن
ريدية لمريض خالل سنوات خبرتهم. ووجدت الدراسة كذلك الحقيقية لعمل او المشاركة في عمل وصفة للتغذية الو
أن العقبات األساسية لتوفير خدمة التغذية الوريدية الطويلة األمد في المستشفيات قد تكمن في عدم توفر الفريق
المتكامل، ونقص المعدات الالزمة والدعم المالي، إضافة الى المضاعفات المرتبطة باستخدام التغذية الوريدية.
السودان لديهم -وخلصت الدراسة إلى أنه بالرغم من أن خبراء التغذية المستهدفين في مستشفيات والية الخرطوم
الكمية الجيّدة من المعرفة حول تعريف التغذية الوريدية، ومؤشرات استخدامها، وطرق إيصال محاليلها، وتدابير
لهم باتخاذ الدور الحقيقي لتوفير ة المؤهلة تجربة السريرية الكافيالتقييم الالزمة لها، اال أنه ليس لديهم المعلومات أو ال
خدمة التغذية الوريدية.
وضع عدد قليل من النماذج لوحدات التغذية الوريدية في المستشفيات التخصصية سيكون عونا كبيرا في توفير هذه
دية.الخدمة، فضال عن توفير التدريب الختصاصي التغذية في مجال التغذية الوري
VI
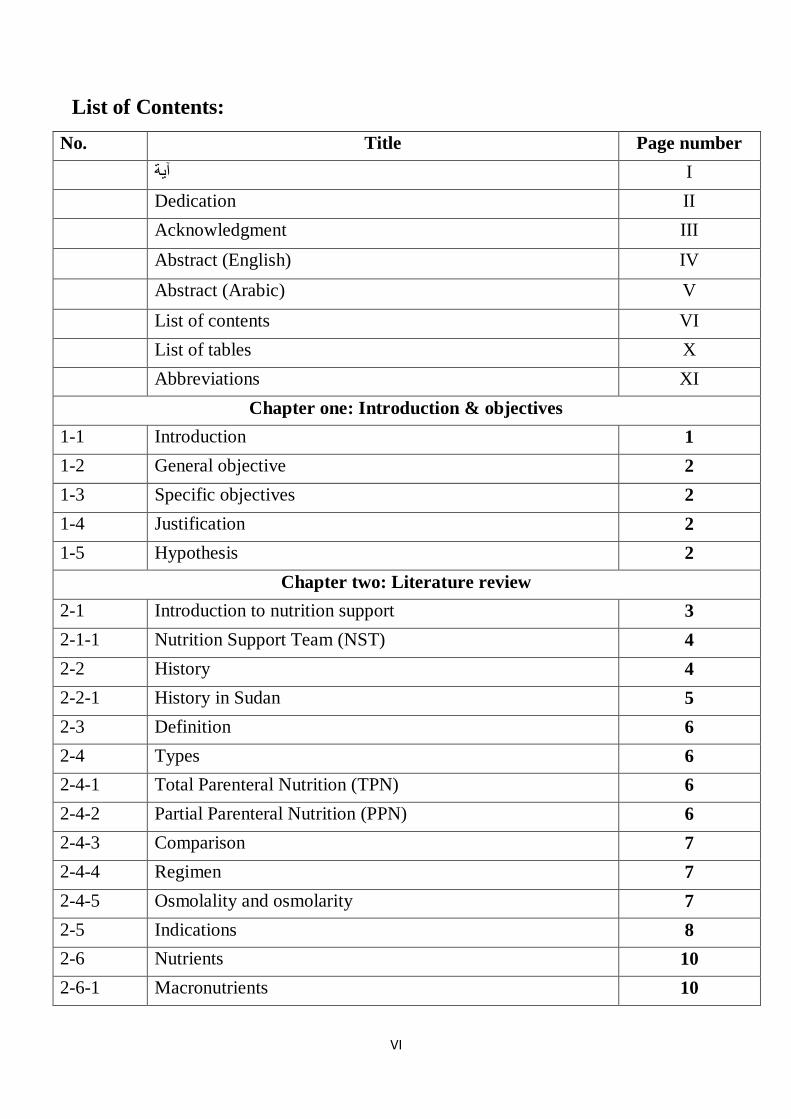
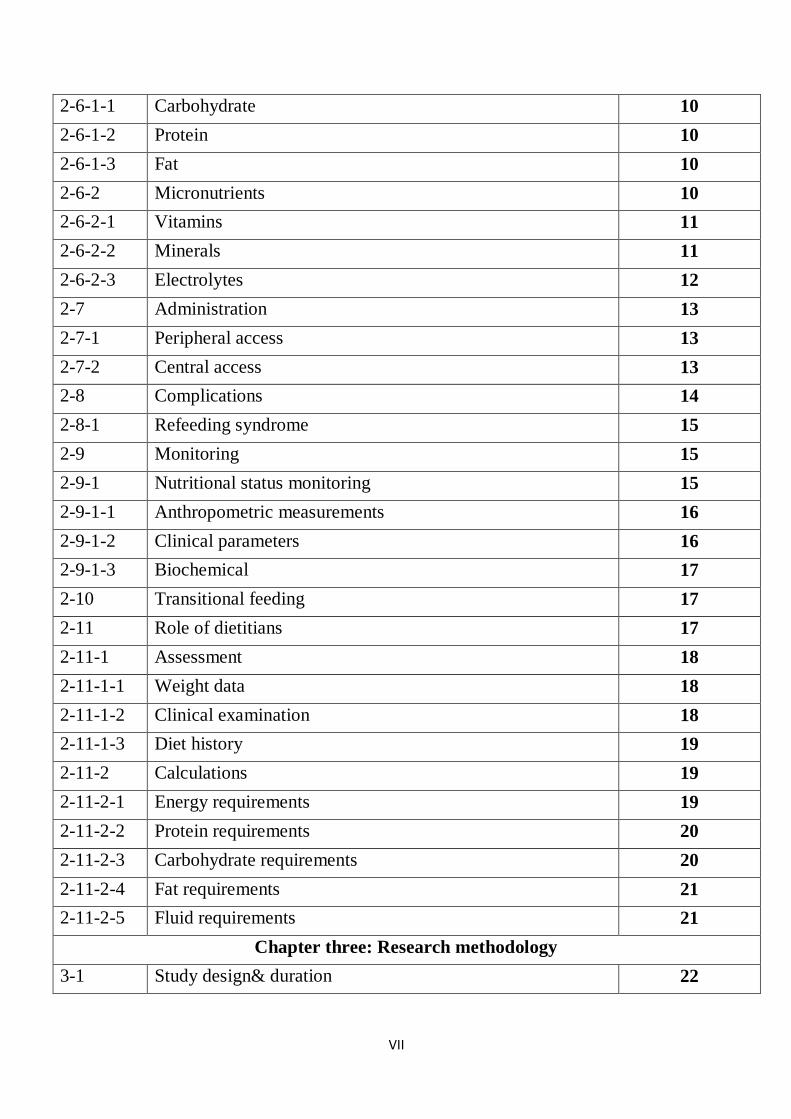
List of Contents:
No. Title Page number
I آية
Dedication II
Acknowledgment III
Abstract (English) IV
Abstract (Arabic) V
List of contents VI
List of tables X
Abbreviations XI
Chapter one: Introduction & objectives
1-1 Introduction 1
1-2 General objective 2
1-3 Specific objectives 2
1-4 Justification 2
1-5 Hypothesis 2
Chapter two: Literature review
2-1 Introduction to nutrition support 3
2-1-1 Nutrition Support Team (NST) 4
2-2 History 4
2-2-1 History in Sudan 5
2-3 Definition 6
2-4 Types 6
2-4-1 Total Parenteral Nutrition (TPN) 6
2-4-2 Partial Parenteral Nutrition (PPN) 6
2-4-3 Comparison 7
2-4-4 Regimen 7
2-4-5 Osmolality and osmolarity 7
2-5 Indications 8
2-6 Nutrients 10
2-6-1 Macronutrients 10
VII
2-6-1-1 Carbohydrate 10
2-6-1-2 Protein 10
2-6-1-3 Fat 10
2-6-2 Micronutrients 10
2-6-2-1 Vitamins 11
2-6-2-2 Minerals 11
2-6-2-3 Electrolytes 12
2-7 Administration 13
2-7-1 Peripheral access 13
2-7-2 Central access 13
2-8 Complications 14
2-8-1 Refeeding syndrome 15
2-9 Monitoring 15
2-9-1 Nutritional status monitoring 15
2-9-1-1 Anthropometric measurements 16
2-9-1-2 Clinical parameters 16
2-9-1-3 Biochemical 17
2-10 Transitional feeding 17
2-11 Role of dietitians 17
2-11-1 Assessment 18
2-11-1-1 Weight data 18
2-11-1-2 Clinical examination 18
2-11-1-3 Diet history 19
2-11-2 Calculations 19
2-11-2-1 Energy requirements 19
2-11-2-2 Protein requirements 20
2-11-2-3 Carbohydrate requirements 20
2-11-2-4 Fat requirements 21
2-11-2-5 Fluid requirements 21
Chapter three: Research methodology
3-1 Study design& duration 22

VIII
3-2 Study area 22
3-3 Study population 22
3-4 Sampling 22
3-5 Data collection 22
3-6 Data analysis 22
3-7 Data presentation 23
3-8 Ethical considerations 23
Chapter four: Results
4-1 Academic qualification of the study population 24
4-2 Experience of the population in nutrition field 24
4-3 Are you aware about parenteral nutrition: 25
4-4 Definition of parenteral nutrition: 25
4-5 Have you come across medical conditions in need of
Parenteral nutrition
26
4-6 The most exposed category for parenteral nutrition 26
4-7 Parenteral nutrition is more indicated for 27
4-8 Positive influence of parenteral nutrition 27
4-9 Alternative route of oral or enteral nutrition support 28
4-10 Parenteral nutrition assessment measurements 28
4-11 Knowledge about parenteral nutrition calculations 29
4-12 Have you ever formulated a parenteral nutrition prescription
or participated in that
29
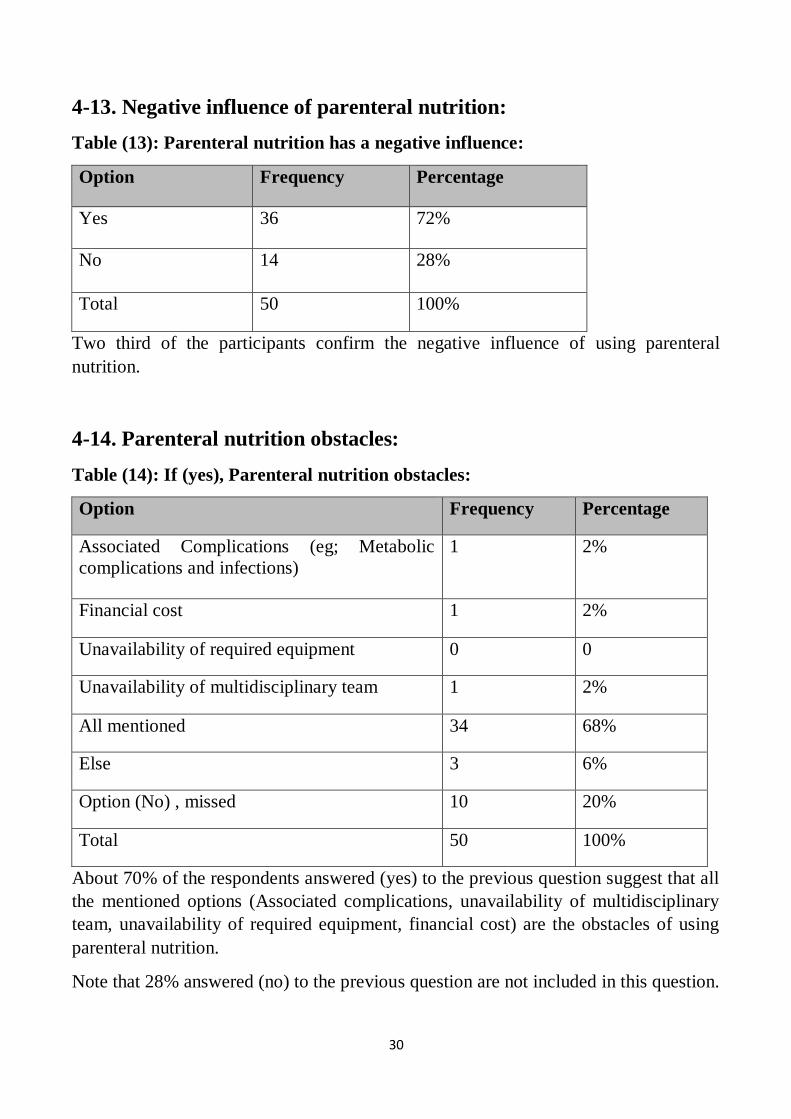
4-13 Negative influence of parenteral nutrition 30
4-14 Parenteral nutrition obstacles 30
Chapter five: Discussion
5-1 Discussion 31
5-2 Conclusions 32
5-3 Recommendations 33
*References 34
*Appendices
Appendix 1- Picture of nutrition support routes 38
Appendix 2- Picture of access to superior vena cava 39

IX
Appendix 3- Picture of peripheral inserted central catheter 40
Appendix 4- Questionnaire (Arabic) 41
Appendix 5- Questionnaire (English) 43
X
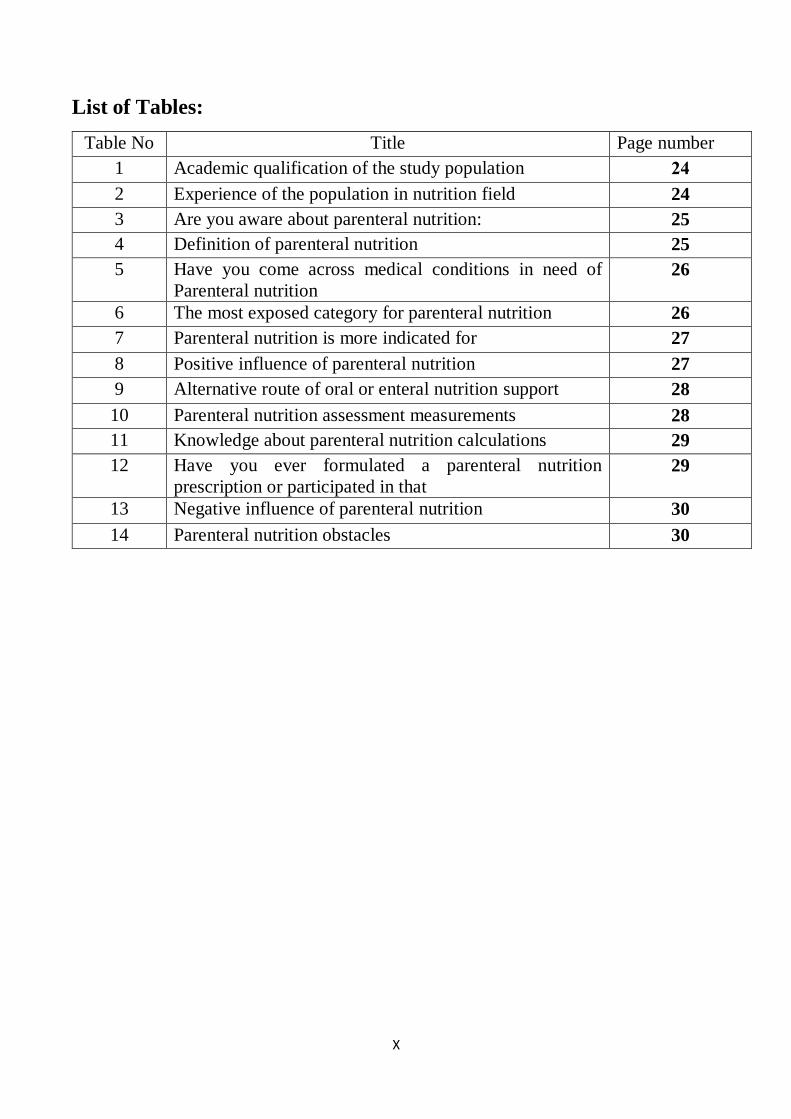
List of Tables:
Table No Title Page number
1 Academic qualification of the study population 24
2 Experience of the population in nutrition field 24
3 Are you aware about parenteral nutrition: 25
4 Definition of parenteral nutrition 25
5 Have you come across medical conditions in need of
Parenteral nutrition
26
6 The most exposed category for parenteral nutrition 26
7 Parenteral nutrition is more indicated for 27
8 Positive influence of parenteral nutrition 27
9 Alternative route of oral or enteral nutrition support 28
10 Parenteral nutrition assessment measurements 28
11 Knowledge about parenteral nutrition calculations 29
12 Have you ever formulated a parenteral nutrition
prescription or participated in that
29
13 Negative influence of parenteral nutrition 30
14 Parenteral nutrition obstacles 30
XI
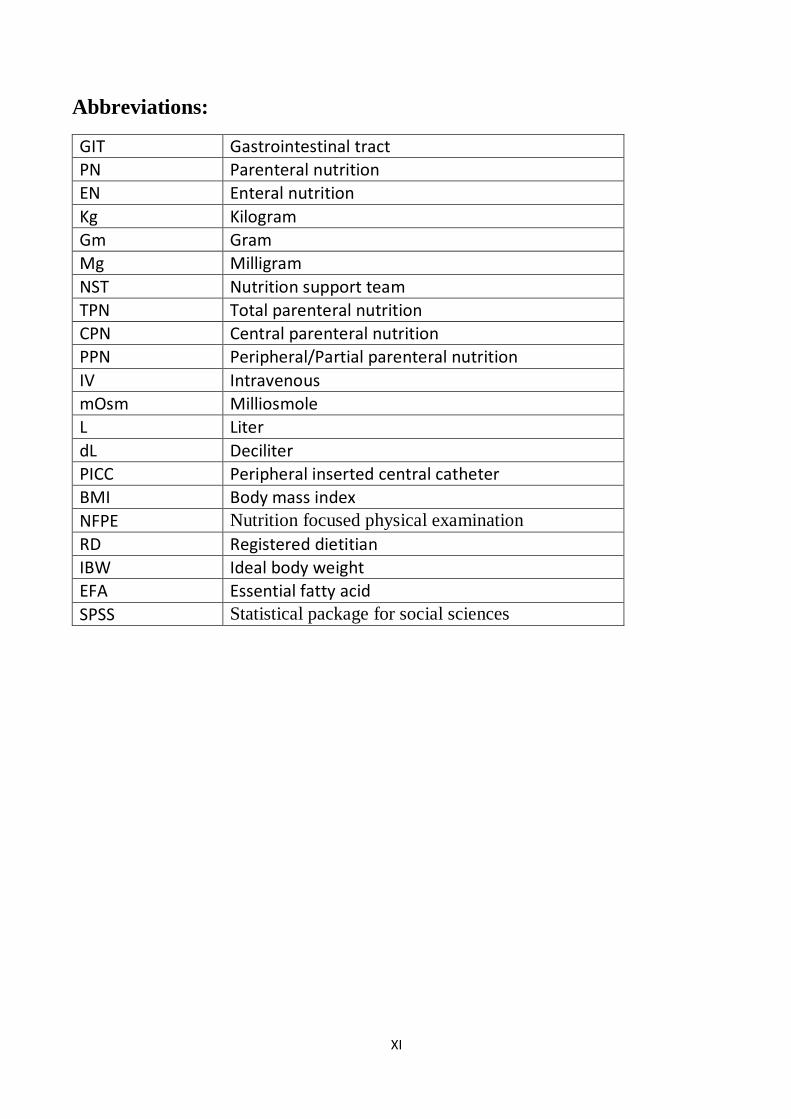
Abbreviations:
GIT Gastrointestinal tract
PN Parenteral nutrition
EN Enteral nutrition
Kg Kilogram
Gm Gram
Mg Milligram
NST Nutrition support team
TPN Total parenteral nutrition
CPN Central parenteral nutrition
PPN Peripheral/Partial parenteral nutrition
IV Intravenous
mOsm Milliosmole
L Liter
dL Deciliter
PICC Peripheral inserted central catheter
BMI Body mass index
NFPE Nutrition focused physical examination
RD Registered dietitian
IBW Ideal body weight
EFA Essential fatty acid
SPSS Statistical package for social sciences
I
Chapter One
Introduction
1
1-1. Introduction:
Nutrition support is the delivery of formulated enteral or parenteral nutrients for the
purpose of maintaining or restoring nutritional status when patients are unable to support
their nutritional needs for more than few days. (Mahan et al, 2012).Parenteral nutrition
(PN) is part of the nutrition support therapy, which is a method of getting nutrition into
the body through the veins directly into the bloodstream when it is not possible to meet
nutritional requirements via the gastrointestinal tract for significant time.(Baker
&Bojczuk, 2016)
The nonfunctional gastrointestinal tract (GIT) and inadequate gut function as in cases
of gastrointestinal obstructions, severe gastrointestinal inflammatory diseases, short
bowel syndrome, and intractable diarrhea or vomiting are some indications for
supplying PN.
A PN solution may comprise different nutrients of carbohydrate as dextrose, protein
as amino acids, lipid as fat emulsion, and micronutrients. When the prepared solution
contains all the nutritional requirements and given by a central vein it is called Total
Parenteral Nutrition (TPN), and when it supplies part of the nutritional needs and given
by a peripheral vein it is called Partial/Peripheral Parenteral Nutrition (PPN).
Although there are different associated complications of this therapy which might be
mechanical, infectious, or metabolic, with proper case selection and careful monitoring,
providing PN can improve clinical outcome, reduce hospitalization time, and reduce the
cost of patient care, (Thomovsky, 2007).
Dietitians are important personnel in the nutrition support team (NST) that is often
consist of physicians, dietitians, nurses, and pharmacists (Delegge& Kelley, 2013). NST
provides different routes of nutritional support by choosing proper nutritional support
interventions for the needy patients. They facilitate the appropriate initiation of PN and
avoid unnecessary episodes of the therapy. (Bhagavatula&Tuthill, 2011)
Nutrition assessment, determination of macronutrient and micronutrient
requirements, and monitoring the nutritional status are vital aspects of the provision of
PN support that benefit from the knowledge and experience of a dietitian. (McCare et
al,1993)
In Sudan, Total Parenteral Nutrition (TPN) services had been introduced in the
1980's in Soba University Hospital, soon after it has been used in developed countries,
and some other hospitals thereafter. However, it was mainly used for surgical patients
and was in the form of ready to infuse amino-acid solutions. TPN therapy was not
available for newborns and children until recently. Gaffar Ibn Ouf Children Teaching

2
Hospital in Khartoum was the first pediatric hospital to offer this kind of therapy in
Sudan. (Elamin&Norri, 2010)
This study was conducted to assess the awareness of the dietitians working in the
targeted chosen hospitals in Khartoum State about PN and their role in providing this
service.
1-2 General objective:
To study the awareness of dietitians about their role in providing PN service in some
Khartoum State hospitals.
1-3 Specific objectives: 1) To explore the dietitians awareness about the importance, indications, and
obstacles of PN.
2) To assess the current awareness of dietitians about their role in providing PN
service.
1-4 Justification: The researcher is interested in the topic and has accomplished a previous study
as a BSc graduation research in 2014. (AlGibali&AlSaad, 2014)
1-5 Hypothesis: The role of dietitians in providing PN service in Khartoum State hospitals is
ignored.
Chapter Two
Literature Review

2-1. Introduction to nutrition support:
Nutrition support therapy is part of nutrition therapy, which is a component of medical
treatment that can include oral, enteral, and parenteral nutrition. Nutrition support is the
delivery of formulated enteral or parenteral nutrients for the purpose of maintaining or
restoring nutritional status when patients are unable to support their nutritional needs
for more than few days. (Mahan et al, 2012)
The overall aim of nutrition support is to try to ensure that total nutrient intake (food
+ nutrition support) provides enough energy, protein, fluid and micronutrients to meet
all the patients’ needs. When feasible, it should be given via the gastrointestinal (GI)
tract. If the GI tract cannot be accessed or there is either partial or complete intestinal
failure, some or all of a patient’s nutritional needs may be met using an intravenous
infusion of PN. (National Collaborating Centre for Acute Care, 2006)
Because timely proper nutritional support aims to prevent malnutrition in those who
are at risk and treat those who are malnourished, healthcare professionals should
consider using oral, enteral or parenteral nutrition support, alone or in combination, for
people who are either malnourished (eg: BMI<18.5 kg/m2, have unintentional weight
loss greater than 10% within the last 3–6 months), or people who are at risk of
malnutrition (eg: have a poor absorptive capacity, and/or have high nutrient losses
and/or have increased nutritional needs). Potential swallowing problems should be taken
into account. (National Institute for Health and Care Excellence NICE Guidance, 2006)
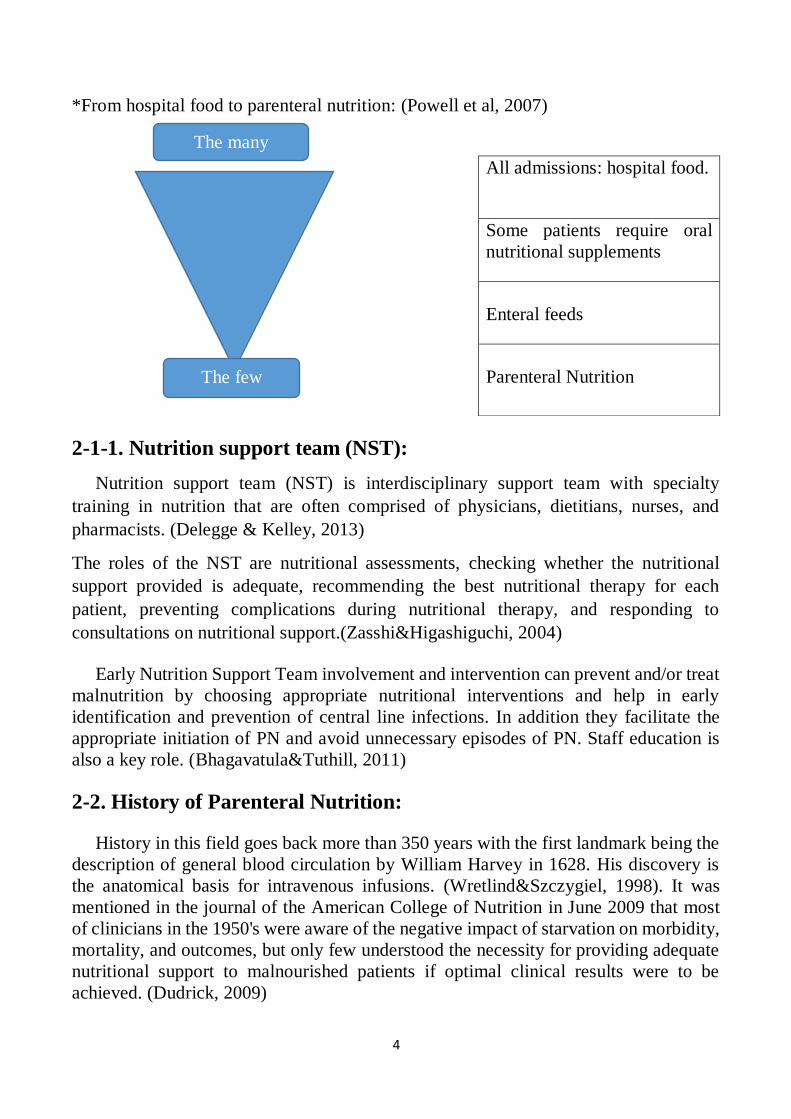
The provision of nutritional support can be seen as an inverted triangle in which the
majority of patients have their needs met by hospital food, a smaller number need
supplementation or sip feeds, still fewer need tube feeding and just a small minority
need PN. (Powell et al, 2007)
4
*From hospital food to parenteral nutrition: (Powell et al, 2007)
2-1-1. Nutrition support team (NST):
Nutrition support team (NST) is interdisciplinary support team with specialty
training in nutrition that are often comprised of physicians, dietitians, nurses, and
pharmacists. (Delegge & Kelley, 2013)
The roles of the NST are nutritional assessments, checking whether the nutritional
support provided is adequate, recommending the best nutritional therapy for each
patient, preventing complications during nutritional therapy, and responding to
consultations on nutritional support.(Zasshi&Higashiguchi, 2004)
Early Nutrition Support Team involvement and intervention can prevent and/or treat
malnutrition by choosing appropriate nutritional interventions and help in early
identification and prevention of central line infections. In addition they facilitate the
appropriate initiation of PN and avoid unnecessary episodes of PN. Staff education is
also a key role. (Bhagavatula&Tuthill, 2011)
2-2. History of Parenteral Nutrition:
History in this field goes back more than 350 years with the first landmark being the
description of general blood circulation by William Harvey in 1628. His discovery is
the anatomical basis for intravenous infusions. (Wretlind&Szczygiel, 1998). It was
mentioned in the journal of the American College of Nutrition in June 2009 that most
of clinicians in the 1950's were aware of the negative impact of starvation on morbidity,
mortality, and outcomes, but only few understood the necessity for providing adequate
nutritional support to malnourished patients if optimal clinical results were to be
achieved. (Dudrick, 2009)
All admissions: hospital food.
Some patients require oral
nutritional supplements
Enteral feeds
Parenteral Nutrition
The many
The few
5
The idea of providing nutrients intravenously in humans was first realized when Sir
Christopher Wren injected wine in dogs' way back in the middle of the 17th century
(Shamsuddin, 2003). In the late 1960s hypertonic parenteral nutrition solution were used
which was a major success in providing nutrition to patients with non-functional GIT.
Crystalline amino acids isolated from soyabeans and fat solutions were tried for PN in
1970. By 1983 three in one solution comprising carbohydrates, protein and fat were
tried as PN supplements.( Joshi, 2008)
Better understanding of the metabolic and pharmacological properties of the
macronutrients (protein, carbohydrates, and lipid), the micronutrients (trace elements,
and vitamins), and the electrolytes have made it possible to administer PN safely to all
types of patients where it is indicated. Continuous development and improvement in the
pharmaceutical presentations of these nutrients have helped to minimize the metabolic
problems seen in the early days of PN administration. (Shamsuddin, 2003)TPN has been
shown to be of very great clinical importance to prevent and treat starvation often related
to high morbidity and mortality.
2-2-1. History in Sudan:
In the Sudanese Journal for Medical Sciences (March - 2010) it was mentioned that TPN
services have been introduced in Sudan in the 1980 in Soba University Hospital, soon
after it has been used in developed countries, and some other hospitals thereafter.
However, it was mainly used for surgical patients and was in the form of ready to infuse
amino-acid solutions. It was also mentioned that IbnSeena Hospital in Khartoum was
the first to establish a unit, where TPN is prepared and different components mixed
according to patient’s requirement under completely aspetic conditions. TPN therapy
was not available for newborns and children until recently. Gaffar Ibn Ouf Children
Teaching Hospital in Khartoum is the first pediatric hospital to offer this kind of therapy
in Sudan. Patients in the neonatal and the gastroenterology units of the hospital are the
usual customers. The pharmacy department at Gaffar Ibn Ouf Hospital had the
expertise, the will and the resources to provide TPN mixtures to the in-patients of the
hospital and the needy children in other pediatric hospitals in Khartoum.
(Elamin&Norri, 2010)
Referring to the previous study of the researcher (In 2014), titled the present status
of PN in Khartoum State in Sudan, 110 different health professionals responded to the
questionnaire forms. Eighty percent of the responders believe that there are many
indications to provide PN in the targeted hospitals of the study, 50% of them believe
that PN is more needed in surgical cases, 85% of them agreed that provision of proper
PN service requires specialized team, knowledge, and the needed equipments. The study
showed that 50% of the responders think that lacking of the trained personnel, enough

6
knowledge, and lacking of the required instruments are the main factors hinder the
starting proper PN service in Sudan. (AlGibali&AlSaad, 2014)
2-3. Definition:
Parenteral nutrition (PN), also known as intravenous feeding, is a method of getting
nutrition into the body through the veins directly into the bloodstream. (Stubblefield,
2014). PN is feeding a person intravenously, bypassing the gastrointestinal (GI) tract
and the usual process of eating, digestion and absorption. The designated person
receives nutritional formulas containing salts of minerals, glucose, amino acids, lipids
and added vitamins. (Elamin&Norri, 2010)
PN is intravenous administration of nutrition, which may include protein, carbohydrate,
fat, minerals and electrolytes, vitamins and other trace elements for patients who cannot
eat or absorb enough food through tube feeding formula to maintain good nutrition
status. (American Society for Parenteral and Enteral nutrition ASPEN, 2012).
Compared with enteral nutrition, PN is more technically demanding, less physiologic
that it does not preserve gastrointestinal (GI) tract structure and function, and is more
expensive. (Prittie, 2004)
2-4: Types of parenteral nutrition:
There are two types of PN:
2-4-1. Total Parenteral Nutrition (TPN), or Central Parenteral
Nutrition (CPN):
A solution containing all the required nutrients including protein, fat, carbohydrate,
vitamins, minerals, and electrolytes, is injected for several hours into a central vein. It
provides a complete and balanced source of nutrients for patients who cannot consume
a normal diet or use their gastrointestinal tract. (The Gale Group, 2008)
2-4-2. Partial Parenteral Nutrition (PPN):
A supplemental form of nourishment delivered intravenously to patients who are sick
or injured and cannot adequately feed themselves or use a feeding tube. Partial
parenteral nutrition (PPN) supplies only part of the daily nutritional requirements
intravenously, supplementing oral intake. (Harkin & Ling, 2014)

7
2-4-3. A simple comparison between the two types:
Difference TPN PPN
Used when patient Does not receive any other form of
nutrition.
he relies on it completely
The patient may be getting
nutrition from other sources
along with the PPN.
Contents concentration Higher concentration and can only
be administered through a central
vein.
Lesser concentration, and can
be delivered through a
peripheral vein.
Time Can be used for a very long time as
it is delivered through a central
vein.
It's unsafe to be used for long
time in peripheral line because
it is hyperosmolar solutions
2-4-4. Regimen of two types:
Central Peripheral
Osmolarity
>= 1800mOsm/L
650-900 mOsm/L
Caloric intake/day
2000-3000
700-1800
Lipid emulsion Minor caloric source, for essential
fatty acids (EFA)
Major caloric source
Duration >= 7days 5-7 days
(Joshi, 2008)
2-4-5. Osmolality and Osmolarity:
Osmolality is the number of millimoles of liquid or solid in a liter of solution.
Osmolarity is the number of attracting particles per weight of water in Kilograms. The
serum osmolarity is maintained in a narrow range (280-300 mOsm/kg), changes above
or below this range may lead to serious metabolic problems. Changes caused by PN in
serum osmolarity are regulated by rapid blood flow and by kidneys. However,
osmolality more than 900 mOsm/L cause irritation to peripheral veins, so solution
greater than this osmolality are infused through central vein. (Joshi, 2008)

8
2-5. Indications:
With proper case selection, providing PN can improve clinical outcome, reduce
hospitalization time, and reduce the cost of patient care. (Thomovsky, 2007)
PN should be used only when it is not possible to meet nutritional requirements via the
gastrointestinal tract for significant time: 1 to 3 days in infants, 4 to 5 days for children
and adolescents, and 7 to 10 days in adults. (Baker&Bojczuk, 2016) The major indication
of PN is nonfunctional GI tract. PN is also indicated for high caloric supplements, for
rapid buildup and to correct nitrogen balance. (Joshi, 2008)
Examples of inadequate gut function might include:
• Bowel obstruction or suspected gut ischaemia
• Some types/locations of gastrointestinal fistula
• Short bowel syndrome
• Persistent severe diarrhoea or significant malabsorption
• Persistent signs of significant gut dysmotility (a distended and/or painful
abdomen, persistent large gastric aspirates, no bowel output). (Ferry et al, 2011)
The gut is not accessible when oral intake is not possible, or an enteral feeding tube
cannot be inserted, due to:
• Facial injuries/surgery or malformation
• Upper gastrointestinal tract obstruction or malformation
• Risk of upper gastrointestinal tract bleeding (eg presence of oesophageal varices).
(Ferry et al, 2011)
In children, PN is indicated to prevent the adverse effects of malnutrition in
newborns and children who are unable to obtain adequate nutrients by oral or enteral
routes because of prematurity, necrotizing enterocolitis or other neonatal complications.
(Elamin&Norri, 2010) It may be used as a primary source of nutrition, providing full
nutrition support, or as a partial source, providing nutrition repletion or augmentation in
patients who are unable to tolerate full enteral nutrition. (Aqilina et al, 2007)
One study was done in London, UK (Oct 2013 – March 2014) to estimate if the
indications for PN prescribing in a tertiary referral children’s hospital were appropriate.
303 children (67 newborns) were enrolled. Patients were referred from different
departments across the hospital. The median duration of PN was 18 days. PN was
mainly prescribed to critically ill children on intensive care (66/303), those undergoing
surgery (63/303) and bone marrow transplantation (28/303). The use of PN was
considered inappropriate in 12/303 patients. The study was concluded by that although
the indications for inpatient PN in children is mostly justified, there is still a proportion
9
of patients receiving intravenous nutrition unnecessarily highlighting the need for more
PN training and better access to nutritional support teams. (Mantegazzaet al, 2016)
Different types of intravenous solutions deliver nutrients for different purposes. The
solution composition and the delivery method depend on the person’s medical and
nutrient needs, his nutritional status, and the length of time on intravenous (IV) nutrition
support. (Whitney et al, 2001)
Peripheral parenteral nutrition (PPN) is best for people with normal renal functions
who need only short term nutrition support (7-14 days), for people who need additional
nutrients temporarily to supplement oral or tube feeding, and when central veins are
medically unsound for intravenous (IV) catheter insertion. PPN relies on IV lipid
emulsions to provide concentrated source of calories in the form that is isotonic and less
irritating compared with dextrose which irritates peripheral veins and may collapse it.
(Whitney et al, 2001)
Central parenteral nutrition (CPN) or total parenteral nutrition (TPN) allows infusion
of concentrated IV solutions. Central veins lie close to the heart so large volume of
blood rapidly dilutes TPN solutions. CPN is best when PN is required for long periods,
when nutrients requirements are high, and when people are severely malnourished with
no capability of using GIT.
Possible indications for central TPN:
• Bone marrow transplants.
• Extensive small bowel resections.
• GI tract obstructions.
• High out-put enterocutaneous fistulas.
• Hypermetabolic disorders, or major surgery, when it is anticipated that the GI
tract will be unusable for more than 2 weeks.
• Intractable diarrhea.
• Intractable vomiting.
• Low birthweight with necrotizing enterocolitis (severe GI inflammatory disease)
or bronchopulmonary dysplasia (chronic lung disease).
• Severe acute pancreatitis.
• Severe malnutrition if surgical or intensive medical intervention is necessary.
• Severe nausea and vomiting associated with pregnancy (hyperemesis
gravidarum) when they last more than 14 days.
• When it is anticipated that enteral nutrition can not be established within 7-14
days of hospitalization. (Whitney et al, 2001)
10
2-6.Nutrients:
2-6-1. Macronutrients:
2-6-1-1. Carbohydrates:
Standard IV solutions provide carbohydrates as dextrose monohydrate. It is
concentrations range from 5-70% by volume. Dextrose monohydrate provides
3.4kcalories /gm. Excessive administration of carbohydrates may lead to
hyperglycemia, hepatic abnormalities, and respiratory problems. (Whitney et al, 2001)
Glucose is the body’s main source of energy, and a daily minimum of about 2g/kg
body weight is required to meet the needs of those cells (eg brain, kidney, erythrocytes)
that cannot readily use other fuels. (Ferry et al, 2011)
2-6-1-2. Protein:
Standard IV solutions contain essential and some of nonessential amino acids to meet
the body's protein needs. (Whitney et al, 2001) Amino acids in PN solutions are
available from 3-20% by volume, 10% of this solution provides 100gm/liter (1000 ml),
and 1 gram of it provides 4kcalories. Approximately 15-20% of total energy intake
should come from protein. (Mahan et al, 2012) Most patients receive protein at around
1.0 – 1.2 g/kg body weight if their energy needs are fully met with a standard parenteral
nutrition solution. (Ferry et al, 2011)
2-6-1-3. Fat:
Standard IV solutions provide lipid as lipid emulsion,Lipid emulsion is a soluble
form of fat that allows it to be infused safely into the blood. (Ferry et al, 2011) It is
considered to be as source of essential fatty acids and energy. (Whitney et al, 2001)
Lipid emulsions available in 10%, 20%, and 30% concentrations composed of soybean
oil, safflower oil, and egg yolk phospholipid as the emulsifier. (Mahan et al, 2012)
Cautious use of IV fat to severely stressed people, patients with atherosclerosis,
moderate liver disease, blood coagulation disorders, pancreatitis, and some lung
problems. (Whitney et al, 2001) A general recommendation has been made to keep lipid
around 1g/kg body weight. (Ferry et al, 2011) Patients can receive 25 to 30% total
calories as lipids. (Chowdary& Reddy, 2010)
2-6-2. Micronutrients:
It is highly likely that most patients commencing on PN will have had prior poor
nutrition intake and hence have suboptimal stores of micronutrients in addition to high
demands and losses. Vitamins, minerals and trace elements should be a standard
inclusion in PN.
2-6-2-1. Vitamins:

11
Most of the commercial preparation contain adequate amount of vitamins.
The current recommended daily amounts of vitamins for adults:
Water-soluble vitamins:
Thiamine 3 mg
Riboflavin 3.6 mg
Niacin 40 mg
Pantothenic acid 7.5 mg
Pyridoxine 4 mg
Vitamin B12 5 µg
Folic Acid 400 µg
Vitamin C 100 mg
Biotin 60 µg
Lipid-soluble vitamins
Vitamin A 1000 µg (1mg)
Vitamin D 5 µg (5mcg)
Vitamin E 10 mg
Vitamin K no recommendation made
(Sriram&Lonchyna, 2009)
2-6-2-2. Minerals:
Requirements of minerals in PN is less compared to enteral nutrition since absorption
is not required. Iron is not usually included in the PN solution due to increased risk of
infection especially in critically ill patients. (Joshi, 2008)
Recommended amounts in adult PN:
Chromium 0.2-0.4 µmol (10-20 µg)
Copper 5-20 µmol (0.3-1.2 mg)
Iodide 1.0 µmol (0.13 mg)
Iron 20 µmol (1 mg)
Manganese 5 µmol (275 µg)

12
Molybdenum 0.4 umol (38 µg)
Selenium 0.4-1.5 µmol (31.6-118 µg)
Zinc 50-100 µmol (3.3-6.6 mg)
Fluoride no recommendation made
(Russell, 1999)
2-6-2-3. Electrolytes:
Standard PN solutions usually contain electrolytes. Electrolyte requirements in PN
varies depending on electrolyte depletion, renal function, disease status, electrolyte loss,
body weight, catabolism, and other drug therapy. Close monitoring of inputs and losses
must be made to prevent electrolyte deficiencies and overloads. An important hazard of
excess cations in PN is formation of insoluable precipitates. (Joshi, 2008)
Daily electrolyte additions to adult PN formulation:
Electrolyte Standard Requirement
Calcium 10–15 mEq
Magnesium 8–20 mEq
Phosphorus 20–40 mmol
Sodium 1–2 mEq/kg
Potassium 1–2 mEq/kg
Acetate As needed to maintain acid-base balance
Chloride As needed to maintain acid-base balance
(Mirtallo et al, 2004)
Other components commonly added to parenteral solutions may include albumin
which can be added if serum albumin levels are very low, heparin the anticoagulant used
to prevent blood clots from forming on the IV catheter, and insulin which is used if
needed to regulate blood glucose levels.
2-7. Administration:
PN is administered through a needle or catheter and is usually delivered using an
ordinary intravenous (IV) pump. In general, IV pumps are a very expensive part of PN
therapy. (Ferry et al, 2011)

13
2-7-1. Peripheral access:
Nutrient solutions not exceeding 800-900 mOsm/kg of solvent can be infused
through a routine peripheral intravenous antigocatheter. Close monitoring should be
done to avoid thrombophlebiteis, the principle complication of peripheral catheters.
Extended Dwell Catheter or midline or midclavicular catheter is a beneficial
development in peripheral catheter technology that can remain for 3-6 weeks. (Mahan
et al, 2012)
2-7-2. Central Access:
Short-term central catheters commonly inserted in the subclavian vein and advanced
until the catheter tip is in the superior vena cava, other veins to superior vena cava are
external or internal Jugular veins. The tunneled catheter is commonly used for long-
term central PN which can be placed in the Cephalic, Subclavian, and internal Jugular
veins into the Seuperior Vena Cava vein. A subcutaneous tunnel is created where the
catheter exits the skin several inches from its venous entry site. Care of long-term
catheters requires specialized handling and extensive patient education. (Mahan et al,
2012)
The peripheral inserted central catheter (PICC) is a catheter inserted into a peripheral
vein and advanced into a central vein. It can be used for short or long term. Compared
with a direct central catheter, PICC has fewer insertion and infection related
complications. (Whitney et al, 2001)
There are a number of considerations that need to be made when choosing the route
of venous access. These include:
• History of patient (e.g thrombosis, lymphedema)
• Individual circumstances (e.g hematological stability,allergies)
• Osmolarity of the solution
• Risk of infection
• Duration of PN
• Type of line access available
• Other IV therapies required by the patient. (Agency of Clinical Innovation ACI, 2011)
2-8. Complications:
PN is associated with different complications categorized in four groups:
• Mechanical complications : during insertion or the use of the catheter such as:

14
▪ Air embolism
▪ Pneumothorax (Presence of air in the chest cavity)
▪ Hemothorax ( Presence of blood in the chest cavity)
▪ Central vein thrombophlebitis
▪ Catheter perforation
• Infection and sepsis: which can be caused through:
▪ Catheter entrance site
▪ Contamination during insertion
▪ Long-term catheter placement
▪ Solution contamination
• Gastrointestinal complications: Such as:
▪ Cholestasis
▪ Gastrointestinal villous atrophy
▪ Hepatic abnormalities
• Metabolic complications: Many can arise during PN therapy such as:
▪ Dehydration
▪ Electrolyte imbalance
▪ Essential fatty acids deficiency
▪ Trace minerals deficiency
▪ Uremia
▪ Hyperammonemia
▪ Hyperglycemic coma
▪ Hyperlipidemia
▪ Hypercalcemia, hypocalcemia
▪ Hyperphosphatemia, hypophosphatemia
▪ Hypomagnesemia (Mahan et al, 2012)
The physician mostly monitors the mechanical, infection, and gastrointestinal
complications, while the metabolic complications are highly associated with the
dietitian's involvement and monitoring.
2-8-1. Refeeding syndrome:
Aggressive administration of nutrition, particularly via the intravenous route can
develop refeeding syndrome which is defined as derangements in serum electrolytes
(phosphate, potassium, magnesium), vitamin deficiency, and fluid as well as sodium
retention occurring in malnourished patients after initiation of PN (Schneeweiss,
2016)

15
Metabolic abnormalities include:
• Hypophosphataemia
• Hypokalaemia
• Hypomagnesaemia and occasionally hypocalcaemia
• Altered glucose metabolism (hyperglycaemia)
• Vitamin deficiency
• Cardiac failure, pulmonary oedema and dysrhythmias
• Acute circulatory fluid overload or fluid depletion
These abnormalities can lead to cardiac, respiratory, neuromuscular, haematologic,
hepatic and gastrointestinal complications. If untreated they can be fatal. (Nutrition team
and referrals, 2010)
The refeeding syndrome occurs when energy substrates, particularly carbohydrates,
are introduced into the plasma of anabolic patients. Proliferation of new tissue requires
increased amounts of glucose, potassium, phosphorus, magnesium, and other nutrients
essential for tissue growth. Rapid infusion of carbohydrate stimulates insulin release,
which reduces water and salt excretion and increases the chance of cardiac and
pulmonary complications from fluid overload. (Mahan et al, 2012)
The initial PN formulation should usually contain 25-50% of goal dextrose
concentration and be increased slowly to avoid the consequences of hypophosphatemia,
hypokalemia, and hypomagnesemia.
2-9. Monitoring:
Monitoring during PN is particularly important because the patient is at greater risk
of toxicity, deficiency, and other complications.
2-9-1. Monitoring of nutritional status:
Nutritional status is most effectively assessed and monitored through a combination
of anthropometric data, biochemical and clinical measures.
2-9-1-1 Some important anthropometric measurements:
Parameter Frequency To assess
Weight Daily if fluid balance concerns.
Otherwise weekly.
Fluid balance and
nutritional status.
Height Baseline.
Review with growth/degeneration.
Body Mass Index

16
(British Association for Parenteral and Enteral Nutrition (BAPEN), 2016)
2-9-1-2. Clinical parameters:
Parameter Frequency To assess
Temperature Daily Signs of sepsis and review fluid
requirements.
Fluid balance Daily, then at each
planned review once
stable.
Hydration and compare nutrition
prescribed vs delivered.
Access route Daily Signs of line infection or access issues.
Clinical condition
and medical plan
Daily initially,
reducing to twice
weekly once stable
Whether goals of PN are being met.
Nutritional requirements.
Appropriateness of PN and manage
potential complications.
Medications Baseline then at each
review once stable
Drug-nutrient interactions. Establish
whether medications are affecting gastro-
intestinal function/clinical condition.
GI function and
enteral intake
Daily initially,
reducing to twice
weekly
Ability to take enteral nutrition. Tolerance
to enteral nutrition. Establish the amount
of PN required to meet nutritional needs.
(British Association for Parenteral and Enteral Nutrition (BAPEN), 2016)
2-9-1-3. Biochemistry:
These are some variables to be monitored for inpatient PN:
Variable
Suggested frequency
initial period Later period (A steady
Metabolic State)
BMI Baseline, then repeated if dry weight or
height changes.
Nutritional status
Mid-arm
circumference
Baseline, then monthly Estimate body
composition and
function.
Triceps skin fold Baseline, then weekly Estimate body
composition and
function.

17
Serum electrolytes Daily 1-2/week
Blood Urea Nitrogen 3/week Weekly
Serum calcium, inorganic
phosphorus, magnesium
3/week Weekly
Serum glucose Daily 3/week
Serum triglycerides Weekly Weekly
Liver function enzymes 3/week Weekly
Hemoglobin, hematocrit Weekly Weekly
Platelets Weekly Weekly
WBC count As indicated As indicated
(Mahan et al, 2012)
2-10. Transitional feeding:
The decision to recommence oral or enteral nutrition requires an assessment of GI
tract anatomy, function and absorption. (Agency of Clinical Innovation (ACI), 2011)
The transition from IV feeding to an enteral diet can be accomplished in different
ways and often involves a combination of feeding methods. One way is to start an oral
diet while the person is still on IV nutrition. The diet is often progressive, beginning
with liquids provided in small amounts. If the person cannot eat enough food to meet at
least 50 percent of daily nutrient needs within a few days, and intake does not seem to
be improving, a tube feeding may be considered. The volume of IV solution is reduced
as the volume of enteral feeding is increased. PN can be discontinued when at least 70
to 75 percent of estimated energy needs are being met by oral intake, tube feeding, or
combination of the two. (Whitney et al, 2001)
2-11. Role of the dietitian in Parenteral nutrition:
The role of the dietitian in PN support involves direct patient care, consultative
services, education, program development, and research. Nutrition assessment,
determination of macronutrient and micronutrient requirements and monitoring are vital
aspects of the provision of PN support that benefit from the knowledge and experience
of a dietitian. (McCare et al, 1993) The dietitians therefore need to develop hospital
protocols and care pathways on nutrition support, and to participate in the nutritional
education of the entire clinical workforce. (National Collaborating Centre for Acute
Care, 2006)
2-11-1. Assessment of the patients requiring parenteral nutrition:
When providing nutrition support to patients it is important to assess their nutritional
status. A formal assessment based on anthropometry, biochemistry, clinical and diet

18
history should be carried out by the dietitian. The nutrition assessment is used to
determine priorities of nutritional management, to estimate the patient’s nutritional
requirements, and to provide a baseline measure for monitoring the effectiveness of
intervention. Based on this assessment, a treatment goal can be set and a nutrition care
plan developed. This care plan will change over time, particularly for patients on long-
term PN (longer than three to six months). (Ferry et al, 2011) Nutrition assessment also
helps to gather necessary data to direct the timing of nutrition support in hospitalized
patients based on the route for feeding. Malnutrition usually refers to protein-energy
malnutrition resulting from extended periods of negative balance of energy and protein
below metabolic requirements. (Kirby & Corrigan, 2013)
2-11-1-1. Weight Data:
Body mass index (BMI) is commonly used to compare height and weight and is
calculated as weight in kilograms divided by height in meters squared [BMI= weight
(kg) / height (m2)]. A BMI less than 18.5 meets criteria for malnutrition, a BMI between
18.5 and 24.9 indicates a healthy weight status, a BMI from 25-29.9 is overweight, and
a BMI greater than or equal to 30 is classified as obese.
BMI is simple to calculate and provides a snapshot of the current weight category.
Changes in recent weight most accurately assess current nutritional risk. Involuntary
weight loss of greater than 10% of usual body weight over 6 months or loss of greater
than 5% of usual body weight in 1 month is considered strong evidence of malnutrition.
(Kirby & Corrigan, 2013)
2-11-1-2. Clinical Examination:
A Nutrition Focused Physical Examination (NFPE) assists clinicians in gathering
information about the patient's nutritional status. It begins with a general visual
inspection of the patient from head to toe. Overt or obscure signs of malnutrition may
be identified and require further testing to confirm the presence of the nutritional
deficiency. (Kirby & Corrigan, 2013)
2-11-1-3. Diet History:
A registered dietitian (RD) utilizes many tools to obtain a diet history including
dietary recall methods, food diaries, or intake and output records. The RD also obtains
information on changes in weight, appetite, and oral intake along with physical activity
levels/functional status, food allergies/intolerances, bowel habits, use/dose of vitamin
supplements, religious diet restrictions, and nutrition support regimes (oral nutritional

19
supplements, enteral tube feeding regimes, or PN regimes). If a change in oral intake
was noted, the RD would also gather more data on the time frame and identify possible
reasons for the change (i.e. chewing/swallowing problems, nausea/vomiting, early
satiety, pain associated with oral intake, reflux, depression, inability to prepare or
procure food, etc.). (Kirby & Corrigan, 2013)
Combining findings from the NFPE, diet history, laboratory studies, and
anthropometric measures, helps determine the presence of malnutrition.
2-11-2. Calculations:
2-11-2-1. Energy requirements:
Dextrose solution and lipid emulsions are common macronutrients used to provide
energy in parenteral solution. Nitrogen for protein synthesis is obtained from synthetic
crystalline amino acid solutions. (Maynard, 2015)
After assessing the patient and determining the need for the PN to supply full or part
of energy requirements, energy needs (as kcal/day) can be calculated by using Harris-
Benedict equation putting into consideration the activity and stress factors.
• Harris-Benedict equation:
Males Basal Energy Expenditure (BEE) =
66.47 + (13.75 x Weight in kg) + [(5.0 x Height in cm) - (6.75 x Age in years)]
Females Basal Energy Expenditure (BEE) =
665.1 + (9.65 x Weight in kg) + [(1.86 x Height in cm) - (4.668 x Age in years)]
(Spodayrk&Kobylarz, 2005)
In addition, energy requirements can be estimated as Kcal/Kg based on the following
scale:
Normal need: 25-30 Kcal/kg/day
Elective surgery: 28-30 kcal/kg/day
Severe injury: 30-40 kcal/kg/day
Extensive trauma/burn: 45-55 kcal/kg/day
20
(Maynard, 2015)
For the obese patients who require PN adjusted body weight must be calculated as
below:
Adjusted IBW for obesity
Female: ([actual weight – IBW] x 0.32) + IBW
Male: ([actual weight – IBW] x 0.38) + IBW
Ideal body weight (wt) may be calculated using the Hamwi method
Men: 50 kg + 2.3 kg for each inch over 5 feet
Women: 45.5 kg + 2.3 kgfor each inch over 5 feet
(Chowdary& Reddy, 2010)
2-11-2-2. Protein requirements:
The common recommendation for the amino acid dose ranges from 1.2 to 1.5 g per
kilogram of the ideal body weight per day for most patients with normal renal and
hepatic function, although some guidelines recommend higher doses (2.0 to 2.5 g per
kilogram per day) under specific conditions (eg; burns or severe trauma). Patients with
chronic renal failure should be given 0.6 – 0.8 gm/kg/day and patients with acute hepatic
encephalopathy should have a temporary restriction of protein to 0.8 gm/kg/day.
Patients on haemodialysis or peritonealdialysis would require 1.2 – 1.3 gm/kg/day.
Parenteral proteins were earlier provided as casein solutions, which had higher
microbicidal growth rates due to contamination, but now they are provided in the form
of crystalline amino acids, which have better nitrogen balance and do not promote
microbial growth. (Chowdary& Reddy, 2010)
2-11-2-3. Carbohydrate requirements:
In central venous PN, a reasonable initial guideline is to provide 60 to 70% of non–
amino acid calories as dextrose and 30 to 40% of non–amino acid calories as fat
emulsion (Ziegler, 2009) but in peripheral PN, solutions may contain lipid up to 60% of
total non-protein calories to reduce the osmolarity of the PN solution and minimise the
risk of peripheral vein thrombosis. (Agency of Clinical Innovation (ACI), 2011)
Carbohydrate intake of 3.0–3.5 g of /kg body weight/day is recommended. In patients
with a high risk of hyperglycaemia (critically ill, diabetes, sepsis, or steroid therapy) 1–
2 g/kg body weight/day is recommended to achieve normoglycaemia. The blood glucose
level should be maintained between 80–110 mg/dL. At least a glucose level of <145

21
mg/dL should be achieved, because levels above 145 mg/dL have been associated with
higher morbidity and mortality. (Ebener C et al, 2009)
2-11-2-4. Fat requirements:
Patients can receive 25 to 30% total calories as lipids. It is estimated that 2-4% of
Kcal must be from essential fatty acids (EFA) and a per needs 1 to 2.5 gram of fat/Kg.
Maximal tolerance level of lipid is considered to be 2.5 gm/Kg body weight and 60%
of energy from fat is also considered to be upper limit. More than 60% of energy from
fat may result in hyperlipidemia due to impaired lipid clearance by the body. (Maynard,
2015)
2-11-2-5. Fluid requirements:
Fluid management in PN depends on the hydration status of the patient and the
clinical conditions, such as, renal failure, congestive heart failure and so on. The total
amount of fluid taken is restricted by making the nutritional fluid more hypertonic in
patients with renal failure, patients with CHF and so on. (Chowdary& Reddy, 2010)
In general, 30-50ml/kg body weight is suggested. Maximum volume of central
parenteral nutrition (CPN) rarely exceeds 3L, with typical prescriptions of 1.5-3L daily.
(Mahan et al, 2012)One method of calculating fluid needs is by adding 100 cc/kg for
first 10 kg body weight + 50 cc/Kg for the second 10 Kg + 20 cc/Kg for each additional
Kg. (Maynard, 2015)

22
Chapter Three
Research Methodology
22
3-1. Study design and duration:
This is a descriptive cross-sectional study conducted in four tertiary hospitals, in
Khartoum State-Sudan, during the period September to December 2016.
3-2. Study area:
The four selected hospitals were Soba University Hospital, Gafar Bin Ouf Children
Teaching Hospital, The Omdurman Military Hospital, and Royal Care Hospital where
three are located in Khartoum locality and one in Omdurman locality. The selection
based on their tertiary level and they also possess variable nutrition services through
recognized dietary departments.
3-3. Study population:
The study focused on a number of dietitians selected randomly from the working
dietitians in the targeted hospitals. All of them were available during the period of data
collection.
3-4. Sampling: Hospital name Number of dietitians
available in hospital
Number of dietitians
responded to the questionnaire
Royal Care Hospital 7 5
Soba University Hospital 10 5
Gafar Bin Ouf Hospital 8 6
Omdurman Military
Hospital
* 34
*It’s a military hospital so the number of dietitians working in the hospital could not be
known.
3-5. Data collection:
Fifty questionnaire forms were distributed to the target group composed of 12
questions.
The questionnaire has two main goals. The first was to collect the demographic data
of the responded dietitians including their gender, educational qualification, and clinical
experience. The second was to evaluate their understanding and awareness of parenteral
nutrition including PN definition, indications, assessment measurements, calculations,
advantages, disadvantages, undesired outcomes, complications, difficulties, and the
obstacles of providing PN in Khartoum state hospitals.
3-6. Data analysis:
The statistical package for 2Wsocial sciences (SPSS) program was used for data
entry and analysis.

23
3-7. Data presentation:
The data were presented in tables.
3-8. Ethical considerations:
An official letter was sent to the hospitals for permission and cooperation. Verbal
consent was taken from the study population to participate in the study and filling the
questionnaire.
Chapter Four
Results

24
4-1. Academic qualification of the study population:
Table (1): Academic qualification of the study population:
Percentage Frequency Qualification
4% 2 Diploma
82% 41 Bachelor
14% 7 Master
0 0 PhD
100% 50 Total
From the dietitians working in the targeted hospitals, more than 80% have Bachelor
academic qualification.
4-2. Experience of the population in nutrition field:
Table (2): Experience of the population in nutrition field:
Percentage Frequency Experience
62% 31 Less than 3 years
16% 8 4-6 years
22% 11 More than 6 years
100% 50 Total
More than 60% of the participants have less than 3 years of experience in the nutrition
practice, 22% have more than 6 years of experience.

25
4-3. Are you aware about parenteral nutrition:
Table (3): Are you aware about parenteral nutrition:
Percentage Frequency Option
94% 47 Yes
6% 3 No
100% 50 Total
Surprising enough that 94% of the targeted population reported that they are aware
about the basics of providing parenteral nutrition.
4-4. Definition of parenteral nutrition:
Table(4): The comprehensive definition of parenteral nutrition:
Percentage Frequency Parenteral nutrition is:
6% 3 Supply the patient with nutritional needs through a
special tube into the stomach or intestines.
10% 5 Supply the patient with nutritional needs through a
peripheral vein.
8% 4 Supply the patient with nutritional needs through a
central vein.
76% 38 Both 2 & 3
100% 50 Total
Three quarters of the responders define parenteral nutrition as supplying the nutritional
needs to the patient through central or peripheral vein. however 6% of the responders
mixed parenteral nutrition with enteral nutrition.

26
4-5. Have you come across medical conditions in need of Parenteral
nutrition:
Table (5): Have you come across medical conditions in need of Parenteral
nutrition:
Percentage Frequency Option
84% 42 Yes
16% 8 No
100% 50 Total
More than 80% of the dietitians revealed that they have exposed in their practice of
clinical nutrition to patients in need of parenteral nutrition. Only 16% have not had such
experience.
4-6.The most exposed category for parenteral nutrition:
Table(6):The most exposed category for parenteral nutrition:
Percentage Frequency Category
10% 5 Pediatrics
4% 2 Adults
24% 12 Elderly
62% 31 All mentioned
100% 50 Total
Most of the responders show that the need of parenteral nutrition is distributed in a wide
range of patients in different age groups.

27
4-7. Parenteral nutrition is more indicated for:
Table (7): Parenteral nutrition is more indicated for:
Percentage Frequency Condition
4% 2 Surgical cases
4% 2 Medical cases
0 0 Oncology patients
4% 2 Malnutrition and disabilities
88% 44 All mentioned
100% 50 Total
88% of the working dietitians in the targeted hospitals confirm that all the mentioned
conditions (Surgical, medical, oncology, malnutrition) may be in need for parenteral
nutrition.
4-8. Positive influence of parenteral nutrition:
Table (8): parenteral nutrition has a positive influence:
Percentage Frequency Option
100% 50 Yes
0 0 No
100% 50 Total
All the respondents confirm the positive influence of using parenteral nutrition.

28
4-9. Alternative route of oral or enteral nutrition support:
Table (9): When patient is unable to tolerate oral or enteral nutrition for a week,
do you recommend parenteral nutrition with the medical team?
Percentage Frequency Option
84% 42 Yes
16% 8 No
100% 50 Total
The study shows that most of the responders recommend parenteral nutrition as an
alternative way to support their patients whenever the sick people are not able to tolerate
oral or eternal feeding.
4-10.Parenteral nutrition assessment measurements:
Table (10): Parenteral nutrition assessment measurements:
Percentage Frequency Parameter
2% 1 Anthropometric measurements
10% 5 Biochemical analysis
88% 44 All mentioned
100% 50 Total
88% of the responders agree that both anthropometric assessment and biochemical data
form basics for the assessment of a patient in need of parenteral nutrition.

29
4-11. Knowledge about parenteral nutrition calculations:
Table (11): Do you have knowledge about calculating the nutritional requirements
for a patient receiving parenteral nutrition?
Percentage Frequency Option
62% 31 Yes
38% 19 No
100% 50 Total
About 60% of the respondents believe that they have knowledge about calculating the
nutritional needs for parenteral nutrition. About 40% do not have that knowledge.
4-12. Have you ever formulated a parenteral nutrition prescription or
participated in that:
Table (12): Have you ever formulated a parenteral nutrition prescription or
participated in that?
Percentage Frequency Option
30% 15 Yes
70% 35 No
100% 50 Total
Although most of the targeted population are aware about the indications, assessment
measurements, and calculating the energy requirements for patients in need of parenteral
nutrition, the study shows that the majority of the responded dietitians have not had a
chance to formulate or participate in formulating a parenteral nutrition prescription for
real patients.
30
4-13. Negative influence of parenteral nutrition:
Table (13): Parenteral nutrition has a negative influence:
Percentage Frequency Option
72% 36 Yes
28% 14 No
100% 50 Total
Two third of the participants confirm the negative influence of using parenteral
nutrition.
4-14. Parenteral nutrition obstacles:
Table (14): If (yes), Parenteral nutrition obstacles:
Percentage Frequency Option
2% 1 Associated Complications (eg; Metabolic
complications and infections)
2% 1 Financial cost
0 0 Unavailability of required equipment
2% 1 Unavailability of multidisciplinary team
68% 34 All mentioned
6% 3 Else
20% 10 Option (No) , missed
100% 50 Total
About 70% of the respondents answered (yes) to the previous question suggest that all
the mentioned options (Associated complications, unavailability of multidisciplinary
team, unavailability of required equipment, financial cost) are the obstacles of using
parenteral nutrition.
Note that 28% answered (no) to the previous question are not included in this question.
Chapter Five
Discussion
31
5-1. Discussion:
The aim of the present study is to recognize the dietitian’s awareness about the
importance, indications, obstacles of parenteral nutrition, and their role in providing this
service whenever it is required.
In this study, three quarters of the dietitians have enough knowledge to define correctly
what is parenteral nutrition and its usable routes. One quarter of the responders missed
the right definition of parenteral nutrition or mixed between parenteral nutrition and
enteral nutrition or were not aware about the proper accesses through which parenteral
nutrition is given (central and peripheral).
More than 80% of the dietitians in the study population revealed that they had the
chance coming across patients who were in need of parenteral nutrition as a part of
therapeutic support. This finding demonstrates that there are a quite number of patients
who are in need for parenteral nutrition in Khartoum State hospitals. It was observed
that most of the newly graduate dietitians (graduated three years ago or less) in this
study have not come across such experience.
Although the review of the literature concerning parenteral nutrition in Sudan
showed that the surgical patients were in more need of parenteral nutrition
(Elamin&Norri, 2010), unlike the results of this study show that most of the working
dietitians in the targeted hospitals confirm that there is no preference among patients
who are in need of parenteral nutrition. They stated that wide spectrum of patients are
equally in need of parenteral nutrition including surgical, medical, oncology, and
malnutrition patients.
Thomovsky (2007) reported that with proper case selection, providing parenteral
nutrition (PN) can improve clinical outcome, reduce hospitalization time, and reduce
the cost of patient care. All the participants confirm the positive impact of using
parenteral nutrition when it's used for the needy patients.
When patients are not able to tolerate oral or enteral feeding to meet their nutritional
requirements, this is one of the main indications for using parenteral nutrition. Five-
sixths of the responders in this study recommend parenteral nutrition as an alternative
way to give the patients their nutritional needs whenever they are not able to tolerate
oral or eternal feeding for a period of week regardless of the age. Few of the responders
do not recommend the use of parenteral nutrition, most likely they are unaware of
parenteral nutrition as an alternative nutritional support route, or they are overbalancing
the risks of using parenteral nutrition.
Ferry et al(2011) mentioned that the dietitians should carry a formal assessment
based on anthropometry and biochemistry measurements for starting and monitoring
32
parenteral nutrition for the needy patients. It is the same opinion of the participants in
this research as most of them answered that they are going to use the same measures to
assess their patients before and after the starting parenteral nutrition. About 12% of the
responders revealed in their answers that they are either going to use biochemical
assessment alone or anthropometry measurements alone.
Regarding calculations of parenteral nutrition formulation, about two-third of the
dieticians in this study have enough knowledge to carry it for the patients who are in
need of parenteral nutrition, and one-third do not have sufficient knowledge to carry it.
Although most of the targeted population are aware about the indications, assessment
measurements, and calculating the energy requirements for patients in need of parenteral
nutrition, the study shows that the majority of the responded dietitians have not had a
chance to formulate or participate in formulating a parenteral nutrition prescription for
real patients. From the previous study of the researcher, it seems that the facilities and
resources in Khartoum State hospitals are not feasible for the dietitians to get the proper
chance to calculate or prescribe parenteral nutrition.
Nutrition assessment, determination of the required macronutrient and micronutrient,
and monitoring the patient's nutritional status are essential to provide proper parenteral
nutrition support and minimize the side effects. This usually requires well trained
dietitian (McCare J D et al,1993). The result of this study shows clearly that dietitians
who spent more than 6 years in clinical practice are more knowledgeable and familiar
with the preparation and the calculation of parenteral nutrition compared with the newly
dietitians whom their clinical experience is less than 3 years.
Although all the participants were found aware about the benefits and advantages of
parenteral nutrition when indicated, one third of them do not aware about the risks and
side effects of it.
The unavailability of the multidisciplinary team, lack of the required equipment and
financial support. In addition to the associated complications including but not limited
to metabolic complications, infections, and catheter related complications, those are
considered the fundamental obstacles to the provision of long term parenteral nutrition
service in Khartoum State hospitals.
5-2. Conclusions:
• In this study the dietitian’s awareness about the importance, indications,
obstacles of parenteral nutrition, and their role in providing this service whenever
it is required in the targeted chosen hospitals in Khartoum state were
investigated.
33
• Most of the dietitians who participated in this study were found knowledgeable
about parenteral nutrition definition, indications, accesses, and assessment
measurements. However in this review about 40% of the dietitians do not have
the enough knowledge and the enough clinical experience that allow them to
take the real role to provide the parenteral nutrition service in form of
calculations, prescription, and overcome any emerge undesired complications in
Khartoum state hospitals.
• The study showed that the majority of the responded dietitians (70%) have not
had a chance to formulate or participate in formulating a parenteral nutrition
prescription for real patients.
• Although all the participants were found aware about the benefits and advantages
of parenteral nutrition when indicated, one third of them do not aware about the
risks and side effects of it.
5-3. Recommendations:
• From the present results, the awareness of parenteral nutrition among all
dietitians work in hospitals should be raised by using different education media
(Such as manuals, brochures, simulation sessions) and by holding workshops.
• Academic courses and educational syllabuses about parenteral nutrition must be
included in the curriculum of dietician’s colleges in the Sudanese universities.
• The high health authority may need to take levelheaded plans and decisions to
give all logistic support that helps in providing PN services in Sudan.
• Establishing models of PN units in few of the tertiary level health institutes and
hospitals will be of great help in providing this service, as well will be
appreciable environment for the dietitian’s training in the area of parental
nutrition.
References:

34
• Agency of Clinical Innovation (ACI). (2011). Parenteral nutrition pocket book:
for adults, reviewed on 3 Dec 2016 from:
http://www.aci.health.nsw.gov.au/__data/assets/pdf_file/0010/159805/aci_paren
teral_nutrition_pb.pdf.
• AlGibali R O, AlSaad O M. (2014). Awareness of the present status of
parenteral nutrition in Khartoum State, Sudan. BSc dissertation, Omdurman
Islamic University, Khartoum State – Sudan.
• Amy Speech & Language Therapy. (2010). Enteral and parenteral nutrition
(picture). Accessed on 5-Dec-2016 from:
http://www.amyspeechlanguagetherapy.com/tube-feeding.htmlInc.
• Aqilina A, Bisson R, Brennan J, Carricato M, Connolly B, Green G, Harrison
D, Harvey E, Herridge J, Hagen L, Kean P. (2007). Guidelines for the
Administration of Enteral and Parenteral Nutrition in Paediatrics. 3rd ed.
Indications for use pp 57. Canada.
• American Society for Parenteral and Enteral Nutrition. (2012). (ASPEN)
parenteral nutrition fact sheet, pp 1-2.
• Baker B J,Bojczuk G. (2016). Parenteral nutrition in infants and children.
Reviewed on 30 Nov 2016 from:http://www.uptodate.com/contents/parenteral-
nutrition-in-infants-and-children
• British Association for Parenteral and Enteral Nutrition (BAPEN). (2016).
Parenteral nutrition monitoring. Reviewed on 4-Dec-2016
from:http://www.bapen.org.uk/nutrition-support/parenteral nutrition/monitoring
• Bhagavatula M, Tuthill D. (2011). Paediatrics and Child Health Journal. The
role of a hospital nutrition support team. 211(9):389-
393.http://www.paediatricsandchildhealthjournal.co.uk/article/S1751-
7222%2811%2900116-8/abstract?cc=y
• EbenerC, HaunerH, JauchK. W, KreymannG, OckengaJ, TraegerK. (2009).
Carbohydrates – Guidelines on Parenteral Nutrition - Chapter 5. GMS German
Medical Science — an Interdisciplinary Journal.
doi: 10.3205/000082https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2795380/
• Cancer research UK. (2015). Intravenous chemotherapy, peripheral inserted
central catheter (PICC Line) picture. Accessed on 6-Dec-2016
from:http://www.cancerresearchuk.org/about-cancer/cancers-in-
general/treatment/chemotherapy/having/iv-chemotherapy
• Chowdary K V and Reddy P N. (2010). Parenteral nutrition: Revisited, Indian
Journal of Anasthesia. 54(2): 95-103.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC2900762/
• Delegge M H, Kelley A T. (2013). State of nutrition support teams. Journal of
Nutrition in Clinical Practice. Vol 28, Issue 6.
http://ncp.sagepub.com/content/early/2013/10/29/0884533613507455
35
• Dudrick S J. (2009). History of parenteral nutrition. Journal of the American
College of Nutrition, 28(3):243-51.
https://www.ncbi.nlm.nih.gov/pubmed/20150597
• Elamin A, Norri A. (2010). Essentials of Parenteral nutrition; A Review.
Sudanese Journal of Medical Sciences. 5 (1):128-134.
• Ferry S, Daniells S, Cook T, Giumelli L, Lamb S, Matterson K, Moss C, Pang
G, Storer K, Wright S, Zuppa J. (2011). Parenteral nutrition manual for adults in
health care facilities. Dietitians association of Australia.
• Harkin R, Ling A J. (2014). Partial Parenteral Nutrition. Last modified date: 20-
Oct-2016. Reviewed on 30Nov2016 from: http://www.wisegeek.com/what-is-
partial-parenteral-nutrition.htm
• Joshi Y K. (2008). Basics of clinical nutrition. 2nd ed. Chapter 10; parenteral
nutrition: an overview pg; 178-189. India.
• Kirby D F and Corrigan M L. (2013). Principles of nutrition support. The
Cleveland Clinic Foundation.Reviewed on 3 Dec 2016 from
http://www.clevelandclinicmeded.com/medicalpubs/diseasemanagement/gastro
enterology/principles-of-nutrition-support/
• Mahan L K, Stump S E, Raymond J L. (2012). Krause's Food and the Nutrition
Care Process. 13th Ed. Ch 14 pp 306 – 322, Elsevier Inc, USA.
• Mantegazza C, Landy N, Hill S M, Zuccotti G V, and Koglmeier J. (2016).
Medical & Clinical reviews, Parenteral nutrition in hospitalized children,
London UK. http://medical-clinical-reviews.imedpub.com/parenteral-nutrition-
in-hospitalized-children.php?aid=8372
• Maynard D C. (2015). Calculating parenteral feedings. Harvard Stem Cell
Institute HSCI 368. Reviewed on 23 Nov 2016:
http://health.csusb.edu/dchen/368 stuff/TPN calculation.htm
• McCare J D, O'shea R, Udine L M. (1993).Parenteral nutrition: hospital to
home. US National Library of MedicineNational Institutes of Health. 93(6):664-
70,673. https://www.ncbi.nlm.nih.gov/pubmed/8509591
• Mirtallo J, Canada T, Johnson D, Kumpf V, Petersen C, Sacks G, Seres D, and
Guenter P. (2004). Special report; Safe Practices for Parenteral Nutrition.
Journal of Parenteral and Enteral Nutrition. 28(6):54.
• National Collaborating Centre for Acute Care. (2006). Nutrition Support for
Adults Oral Nutrition Support, Enteral Tube Feeding and Parenteral Nutrition,
ch 5 pp 70. London.
• National Institute for Health and Care Excellence (NICE) Guidance. (2006).
Clinical guideline (CG32) Nutrition support for adults: oral nutrition support,
enteral tube feeding and parenteral nutrition
https://www.nice.org.uk/guidance/cg32/chapter/1-guidance

36
• Nutrition team and referrals. Parenteral/ Enteral nutrition, Indications for
Parenteral IV Access, Organisation& Supervision of PN, last updated July
2010, accessed on 5-Dec 2016 from:
www.ldh.nhs.uk/EasySiteWeb/GatewayLink.aspx?alId=1283
• Powell J, Wilson R, Wood S, Howard P, Fellows I, Cartwright A, White R,
Radcliffe J. (2007). Organization of food and nutritional support in hospitals.
British Association for Parenteral and Entral Nutrition (BAPEN), pub no. 18
99467 06; pg 11.
• Prittie J. (2004). Route of nutrient delivery. Clinical Techniques in small animal
practice 19 (1), 6-8. Accessed on 5-Dec-2016 from:
https://www.ncbi.nlm.nih.gov/labs/articles/15025192/
• Russell D. (1999). Guidelines for intravenous trace elements and vitamin.
Australian Society for parenteral and enteral nutrition AuSPEN. Reviewed on
28-Nov-2016 from:
http://www.auspen.org.au/wpontent/uploads/2014/11/AuSPEN-Micronutrients-
Guidelines.pdf
• Schneeweiss B. European society for enteral and parenteral nutrition (ESPEN).
Refeeding syndrome. Accessed on 5-Dec-2016 from
www.espen.org/presfile/Schneeweisz-2-010812-web.doc
• Shamsuddin A F. (2003). Brief History and Development of Parenteral
Nutrition Support. Malaysian Journal of Pharmacy, 1(3):69-75.
• Sriram K, Lonchyna V A. (2009). Micronutrient supplementation in adult
nutrition therapy. Journal of Parenteral and Enteral Nutrition, 33:548-562.
• Spodayrk M and Kobylarz K, (2005). The usability of Harris-Bendict and
Curreri equations in nutritional management of thermal injuries,
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3187981/
• Stubblefield H. (2014). Parenteral nutrition written by Heaven Stubblefield
Medically reviewed on January 21, 2014 by George Krucik, retrieved on 23
Nov 2016 from: http://www.healthline.com/health/parenteral-nutrition
• The Gale Group. (2008). Gale Encyclopedia of Medicine TPN definition,
reviewed 23 Nov 2016 from
http://medical-dictionary.thefreedictionary.com/TPN
• Thomovsky E. (2007). Parenteral Nutrition: Uses, Indications, and
Compounding. National center for biotechnology information, Compend Contin
Educ Vet 29 (2), 76-8,-5. Accessed on 5 Dec 2016 from:
https://www.ncbi.nlm.nih.gov/labs/articles/17727158/

37
• Tonk R S, Khurana T R, Chatterjee S. (2015). Total parenteral nutrition
(Picture), accessed on 6-Dec-2016 from:
http://www.slideshare.net/gopal_ghosh1986/total-parenteral-nutrition-55863878
• Whitney E N, Cataldo C B, DeBruyne L K, Rolfed S R. (2001). Nutrition for
health and health care. Second ed. Ch18, pp 430-447. USA.
• Wretlind A, Szczygiel B. (1998). Total parenteral nutrition history, present time
& future. PubMed US National Library of Medicine, 4(22):181-5.
https://www.ncbi.nlm.nih.gov/pubmed/9770991
• Zasshi N G, Higashiguchi T. (2004). The roles of a nutrition support team.
Pubmed US national library of medicine,105(2):206-12.
https://www.ncbi.nlm.nih.gov/pubmed/15027162
• Ziegler T R. (2009). Parenteral nutrition in the critically ill patient. HHs public
access; 361(11): 1088-1097.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3064749/
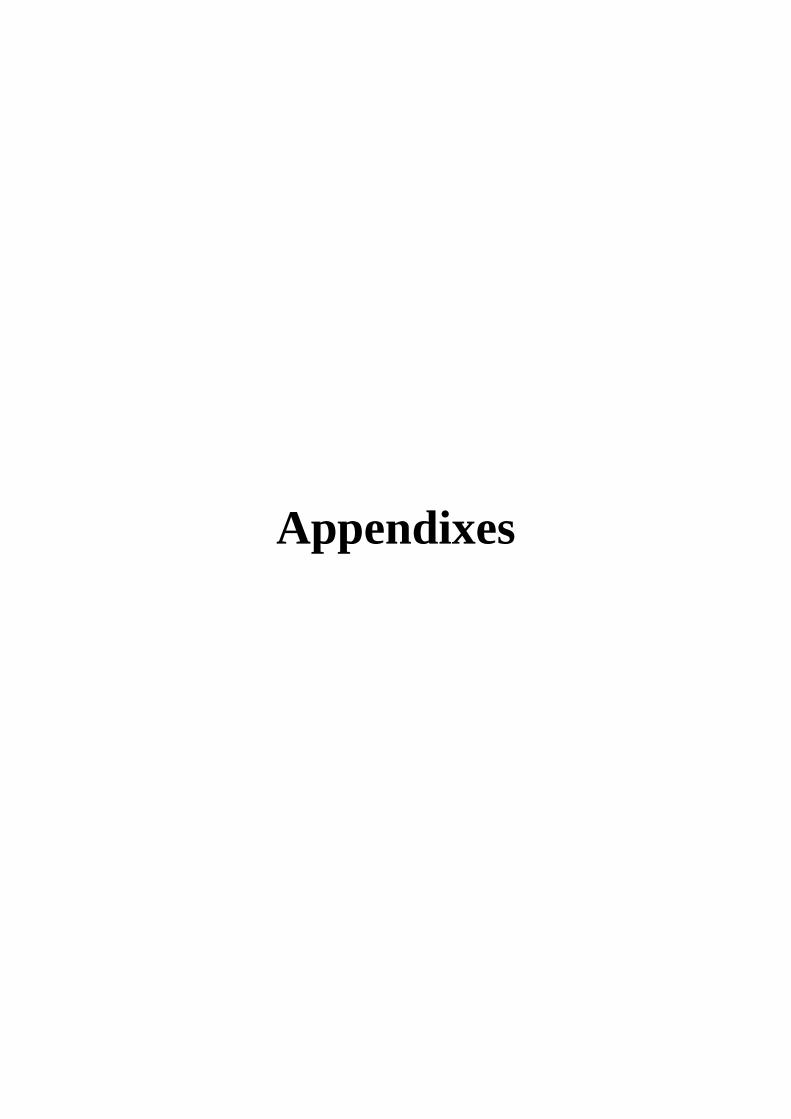
Appendixes
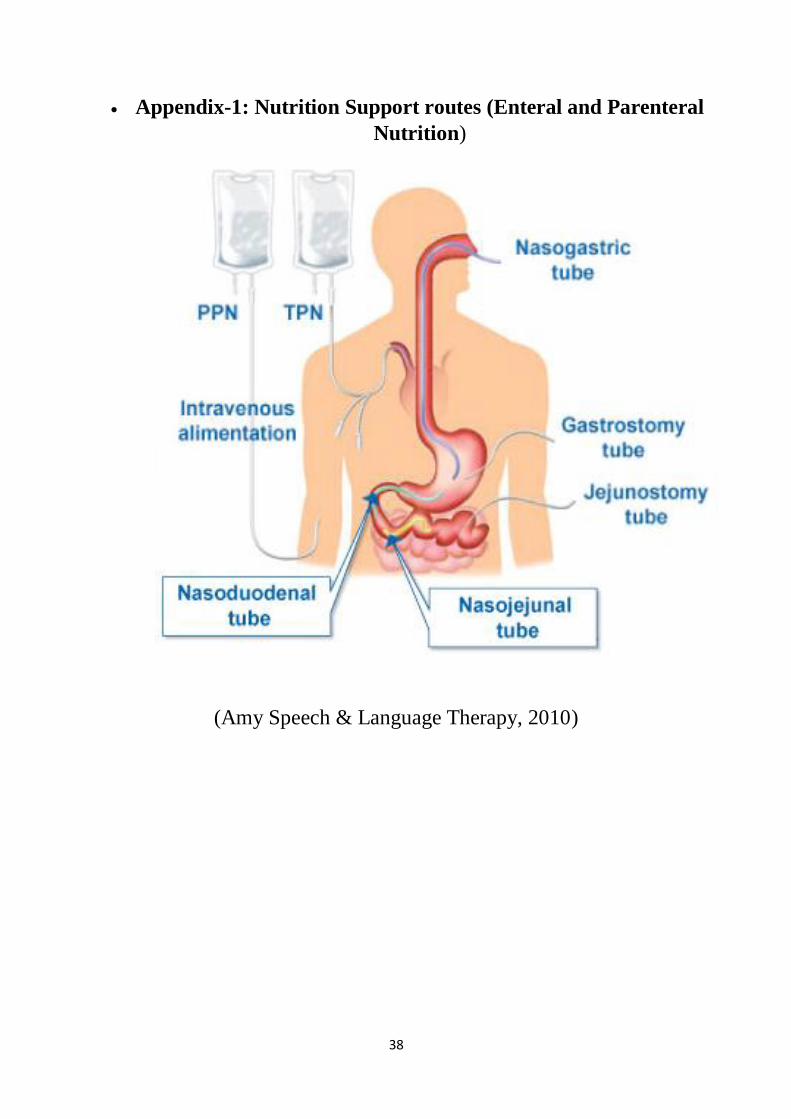
38
• Appendix-1: Nutrition Support routes (Enteral and Parenteral
Nutrition)
(Amy Speech & Language Therapy, 2010)

39
*Appendix-2: Peripheral Inserted Central Catheter (PICC line)
(Cancer research UK, 2015)

40
*Appendix-3: Access to Superior Vena Cava
(Tonk R S et al, 2015)
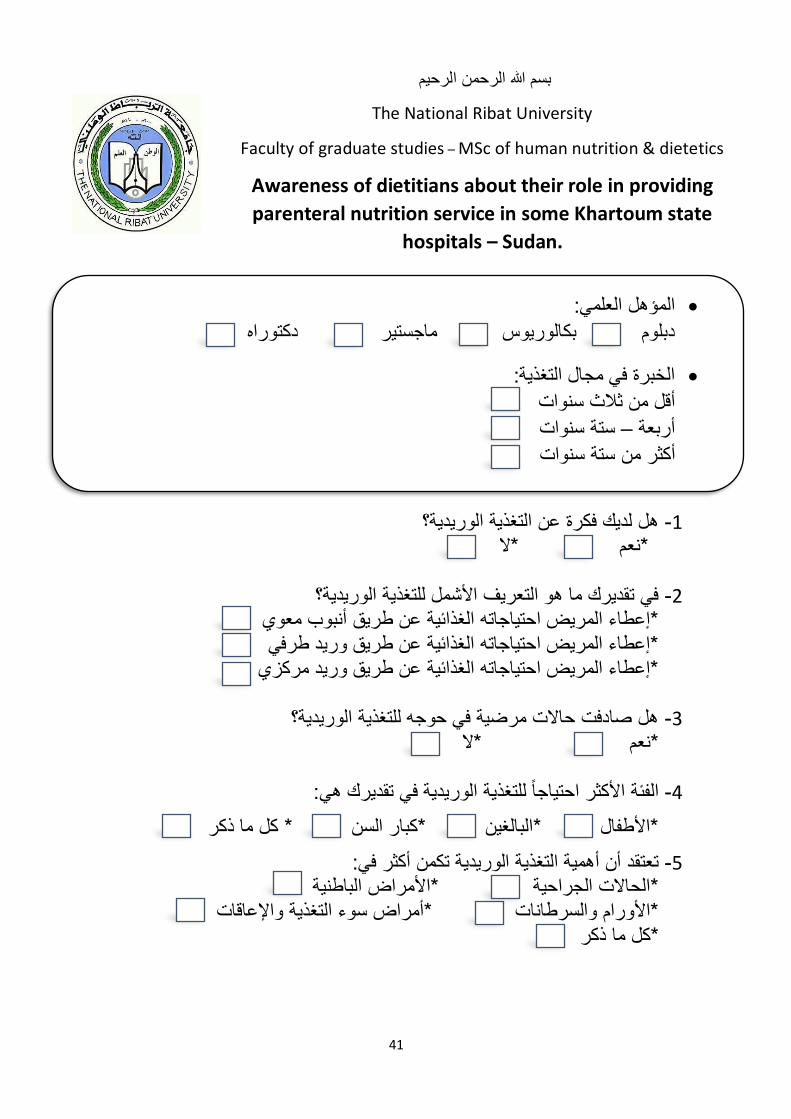
41
هل لديك فكرة عن التغذية الوريدية؟ -1 *نعم *ال
في تقديرك ما هو التعريف األشمل للتغذية الوريدية؟ -2
*إعطاء المريض احتياجاته الغذائية عن طريق أنبوب معوي *إعطاء المريض احتياجاته الغذائية عن طريق وريد طرفي
*إعطاء المريض احتياجاته الغذائية عن طريق وريد مركزي
هل صادفت حاالت مرضية في حوجه للتغذية الوريدية؟ -3 *نعم *ال
احتياجاً للتغذية الوريدية في تقديرك هي:الفئة األكثر -4
*األطفال *البالغين *كبار السن * كل ما ذكر
تعتقد أن أهمية التغذية الوريدية تكمن أكثر في: -5 *األمراض الباطنية*الحاالت الجراحية
سوء التغذية واإلعاقات*أمراض *األورام والسرطانات كل ما ذكر*
المؤهل العلمي: • دكتوراه دبلوم بكالوريوس ماجستير
الخبرة في مجال التغذية:• أقل من ثالث سنوات
ستة سنوات –أربعة
أكثر من ستة سنوات
بسم هللا الرحمن الرحيم
The National Ribat University
Faculty of graduate studies – MSc of human nutrition & dietetics
Awareness of dietitians about their role in providing
parenteral nutrition service in some Khartoum state
hospitals – Sudan.
42
حسب خبرتك ومعرفتك هل تعتقد أن التغذية الوريدية لها مردود إيجابي؟ -6 *نعم *ال
هل توصي بالتغذية الوريدية مع الفريق الطبي في حالة عدم تناول التغذية الكافية عن -7 المعوية لمدة أسبوع؟ طريق الفم أو التغذية
*نعم *ال
حسب خبرتك ومعرفتك ما هي أهم مقاييس تقييم مريض يعتمد على التغذية الوريدية؟ -8 * القياسات الجسمانية
* التحاليل المعملية * االثنان معاً
عن كيفية حساب االحتياجات الغذائية لمريض تحت التغذية هل تتوفر لديك معلومات -9
الوريدية؟ *نعم *ال
هل قمت بعمل وصفة للتغذية الوريدية لمريض أو شاركت في ذلك؟ -10
*نعم *ال
وريدية لها مردود سلبي؟حسب خبرتك ومعرفتك هل تعتقد أن التغذية ال -11 *نعم *ال
معّوقات استخدام التغذية الوريدية؟إذا كانت إجابتك السابقة )نعم( ما هي أهم -12
* التعقيدات المصاحبة الستخدامها كااللتهابات والتعقيدات االستقالبية *التكلفة.
* عدم توفر المعدات الالزمة. * عدم وجود فريق متكامل.
* كل ما ذكر
شكراً لحسن تعاونك
43
1- Are you aware about parenteral nutrition?
*Yes * No
2- In your opinion, the comprehensive definition of parenteral
nutrition is:
* Supply the patient with nutritional needs through a special tube into
the stomach or intestines.
* Supply the patient with nutritional needs through a peripheral vein.
* Supply the patient with nutritional needs through a central vein.
* Both answers 2 & 3
3- Have you come across medical conditions in need of Parenteral
nutrition?
*Yes *No
4- The most exposed category for parenteral nutrition: *Pediatrics *Adults *Elderly *All mentioned
• Academic qualification: DiplomaBachelorMasterPhD
• Experience in nutrition field:
Less than 3 years
4-6 years
More than 6 years
بسم هللا الرحمن الرحيم
The National Ribat University
Faculty of graduate studies – MSc of human nutrition & dietetics
Awareness of dietitians about their role in providing
parenteral nutrition service in some Khartoum state
hospitals – Sudan.
44
5- In your opinion,Parenteral nutrition is more indicated for:
* Surgical cases
* Medical cases * Oncology patients
* Malnutrition and disabilities
* All mentioned
6- Depending on your experience and knowledge, parenteral
nutrition has a positive influence:
* Yes * No
7- When patient is unable to tolerate oral or enteral nutrition for a
week, do you recommend parenteral nutrition with the medical
team?
*Yes *No
8- Depending on your experience and knowledge, the most
important assessment measurement for a patient on Parenteral
nutrition is: *Anthropometric measurements
*Biochemical analysis
*All mentioned
9- Do you have knowledge about calculating the nutritional
requirements for a patient receiving parenteral nutrition? * Yes * No
10- Have you ever formulated a parenteral nutrition
prescription or participated in that? *Yes * No
11- Depending on your experience and knowledge, parenteral
nutrition has a negative influence:
*Yes * No

45
12- If (yes), the main obstacles to the use of parenteral nutrition
are:
* Associated Complications (eg; Metabolic complications and
infections) * Financial cost
* Unavailability of required equipment
*Unavailability of multidisciplinary team
*All mentioned
Thank you for
your cooperation










![Eating Disorders Resource Directory: Dietitians [ 2020 ]](https://static.fdocuments.net/doc/165x107/61a8790a1a7dc3025e34e4e3/eating-disorders-resource-directory-dietitians-2020-.jpg)







