The American College of Obstetricians and Gynecologists (ACOG)
Upload
tim-walkerCategory
view
213download
1
T R A N S P L A N T A T I O N A N D C E L L U L A R T H E R A P Y
Awareness and acceptance of public cord blood banking amongpracticing obstetricians in the United States_3383 787..793
Tim Walker, Del Steckler, Stephen Spellman, Darlene Haven, Kathy Welte, and Michael Boo
BACKGROUND: This study measured: 1) levels ofawareness and understanding among practicing obste-tricians regarding umbilical cord blood (UCB) donationand the use of UCB in transplant therapy, 2) motiva-tions for obstetricians to support donation and collectionfor donation to a public cord blood bank (CBB), and 3)current practices for discussing this option with theirpatients.STUDY DESIGN AND METHODS: Obstetricians prac-ticing in major metropolitan areas in the United Stateswere randomly surveyed in 2009. Of 2041 surveysmailed, 295 were returned, 139 from obstetricians withprivileges at hospitals affiliated with a public CBB (affili-ated) and 156 from obstetricians without such privileges(nonaffiliated). Cross-tabulation analyses were con-ducted to compare responses between these twogroups.RESULTS: Both affiliated and nonaffiliated obstetriciansreport being somewhat or very familiar with the use ofcord blood in transplant therapy (88% vs. 82%,respectively; p = NS), but some misperceptions con-cerning clinical application exist. Eighty percent of affili-ated obstetricians feel confident discussing cord bloodoptions with their patients; however, 49% indicated thatthey have insufficient knowledge of cord blood donationto effectively answer patients’ questions about donation.CONCLUSION: Obstetricians are generally familiar withthe utility of donated cord blood in transplantation, butcould benefit from additional information regarding howcord blood is used in transplantation. Further, obstetri-cians play an important role in encouraging women todonate their baby’s cord blood to a public CBB, arewilling to do so, and indicate a desire for more informa-tion so they can effectively educate their patients.
Following a report in 1989 of the first umbilicalcord blood transplant (UCBT), umbilical cordblood (UCB) began to be collected and cryo-preserved for this use.1 Since then, UCBT has
evolved from an experimental treatment used primarily inchildren to an accepted therapy in children and adultsneeding allogeneic transplant.2,3 Survival after transplantusing UCB donated to public cord blood banks (CBBs) hasimproved steadily and outcomes are now comparable toallogeneic transplant using adult-donated cells in manypatient cohorts.4-8
Through legislation enacted in 2005, the US Congressprovided funding to expand the national inventory ofpublicly available UCB and formalized a program toaccess these units.9 This program, operated by theNational Marrow Donor Program (NMDP) through its BeThe Match Registry, has facilitated more than 4700 cordblood transplants (NMDP 2010 Annual Numbers, A00130rev. 9.0). Worldwide, more than 22,000 UCB units havebeen shipped for use in unrelated transplantation through
ABBREVIATIONS: ACOG = American College of Obstetricians
and Gynecologists; CBB = cord blood bank; NMDP = National
Marrow Donor Program; UCB = umbilical cord blood;
UCBT = umbilical cord blood transplant.
From the National Marrow Donor Program (NMDP) and the
Center for International Blood and Marrow Transplant Research
(CIBMTR), Minneapolis, Minnesota.
Address reprint requests to: Tim Walker, MA, National
Marrow Donor Program, 3001 Broadway Street NE, Minneapo-
lis, MN 55413; e-mail: [email protected].
Funding for the survey of practicing obstetricians was sup-
ported by a grant (N00014-08-1-1207) from the Office of Naval
Research. The survey was developed by the National Marrow
Donor Program with assistance from Anderson, Niebuhr &
Associates, Inc., Arden Hills, MN.
Received for publication July 14, 2011; revision received
August 16, 2011, and accepted August 17, 2011.
doi: 10.1111/j.1537-2995.2011.03383.x
TRANSFUSION 2012;52:787-793.
Volume 52, April 2012 TRANSFUSION 787

2009 (L. Foeken, World Marrow Donor Association, per-sonal communication, January 2011). The clinical use ofUCB has also spurred the development of a private(family) banking industry, providing an opport-unity for storage of a child’s UCB for autologous orfamily use.
Recognizing the potential role of the obstetrician indecision-making and collection processes, the AmericanCollege of Obstetricians and Gynecologists (ACOG)issued a position statement in 2008 on UCB bankingurging obstetricians to present the advantages and dis-advantages of public versus private UCB banking totheir patients considering UCB donation.10 This report isthe first published study to measure obstetricians’awareness and understanding of unrelated UCBT andbarriers and motivations of supporting UCB educationand collection.
MATERIALS AND METHODS
Study populationThe NMDP contracted with a marketing research firm tosurvey a random sample of obstetricians in 57 cities andmetropolitan areas in the United States with public CBBs.In August 2009, a total of 2506 questionnaires with a coverletter were mailed: 1252 to obstetricians with privileges ata hospital affiliated with a public CBB (affiliated obstetri-cians) and 1254 to obstetricians without privilegesat a hospital affiliated with a public CBB (nonaffiliatedobstetricians).
Cover letters to each group were identical and identi-fied the sender as the NMDP. The purpose of the surveywas to “assess obstetricians’ perceptions and attitudesregarding collection and use of umbilical cord blood fortransplantation.” Obstetricians returning a completedsurvey received $75.
Data collectionA multimode method was employed to maximize thenumber of surveys returned. If necessary, postcardfollow-up reminders were mailed, followed by a secondsurvey mailing follow-up, and finally, telephone calls weremade inviting obstetricians to complete the mail survey orto complete the survey via telephone or fax. Oversamplingwas also employed to ensure a sufficiently large studypopulation.
After eliminating the surveys sent to obstetriciansfor whom the questionnaire was not appropriate(e.g., childbirth not part of practice, no longer inpractice), the adjusted survey population was 2041:1047 and 994 for affiliated and nonaffiliated obstetri-cians, respectively. Completed surveys were obtainedfrom 139 affiliated obstetricians and 156 nonaffiliated
obstetricians, resulting in response rates of 13 and 16%,respectively.
Questionnaire designThe NMDP developed a 25- or 26-question survey, foraffiliated and nonaffiliated obstetricians, respectively.(Differences were due to questions related to affiliationthat were relevant to only one group but not the other.)Most questions were multipart. Demographic informa-tion on respondents was requested, such as respondent’ssex, number of years in practice, and number of deliveriesperformed per month.
The survey was pretested with five obstetricians, andresponses were reviewed for patterns of skipped ques-tions and excessive “don’t know” responses that wouldindicate confusion and/or suggest that respondentsthought questions did not apply to them. No surveychanges were made between this pretest and main datacollection.
Questions were designed to gather information infour areas:
• Determine level of understanding by obstetricians onthe use of UCB in transplant therapy;
• Measure current level of awareness of UCBdonation;
• Measure obstetricians’ familiarity and willingnessto speak with expectant mothers about UCBdonation and the motivators and barriers of doingso; and
• Determine current UCB collection practices and will-ingness to collect UCB for public donation.
Most questions asked respondents to indicate theirlevel of agreement with statements using a Likert scale.Some questions asked respondents to estimate a percent-age (e.g., approximately what percentage of your patientsask you for information or your opinion about donatingcord blood to a public bank?). Only one open-ended ques-tion was asked: “If a patient asks you for your opinionabout what she should do with her baby’s cord blood,what do you tell her?”
Statistical analysisDescriptive statistics were compiled for overall data,and responses to the open-ended question were codedand grouped for reporting. Cross-tabulation analyseswere performed to compare responses between affiliatedand nonaffiliated physicians for common questions.Additional cross-tabulation analyses were performedseparately for affiliated and nonaffiliated physiciansbased on several factors, including hospital bed size,number of deliveries per month, and number of years inpractice.
WALKER ET AL.
788 TRANSFUSION Volume 52, April 2012

RESULTS
Demographics of survey respondents are shown inTable 1. A majority of respondents have been in practicebetween 10 and 29 years. Affiliated obstetricians were sig-nificantly more likely than nonaffiliated obstetriciansto supervise residents: 69% versus 38%, respectively(p < 0.05). There were significantly more males thanfemales among nonaffiliated respondents: 64% versus36%, respectively (p < 0.05). No other characteristics weresignificantly different between the responding affiliatedand nonaffiliated obstetricians.
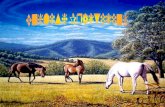
Level of understanding on use of UCB intransplant therapyA high percentage of both affiliated and nonaffiliatedobstetricians reported that they were familiar or veryfamiliar with the use of UCB in transplant therapy: 88%versus 82%, respectively (p = NS; Fig. 1). A significantlyhigher number of affiliated obstetricians said that theywere very familiar with the use of UCB in transplantationthan nonaffiliated obstetricians: 38% versus 23%, respec-tively (p < 0.05).
To assess the knowledge of obstetricians concerningthe clinical application of UCB in the transplant setting, aseries of statements on UCBT were presented and therespondents were asked to agree or disagree. Table 2shows the stated agreement or disagreement with selectedstatements and the accuracy of those statements as evi-denced by the references listed with each statement.
Respondents were asked to indicate their sources ofinformation on UCBT, and the most common source indi-cated by both affiliated and nonaffiliated obstetricianswere materials from private CBBs: 87% versus 84%, respec-tively (p = NS). Affiliated obstetricians were significantlymore likely than nonaffiliated obstetricians to indicatethey obtained information on UCBT through materialsfrom public CBBs: 68% versus 35%, respectively (p < 0.05).
Level of awareness of UCB donationNearly all obstetricians knew that private CBBs chargefees to collect and store UCB (98%, affiliated vs. 96%,nonaffiliated; p = NS). A significantly higher percentage ofaffiliated obstetricians knew that there is no cost towomen who donate their baby’s UCB to a public bank(86%, affiliated vs. 69%, nonaffiliated; p < 0.05).
Nearly all respondents reported that they were famil-iar with the ACOG position statement on UCB banking(89%, affiliated vs. 85%, nonaffiliated; p = NS). Familiaritywith UCB banking positions of other professional organi-zations never exceeded 25%: American Academy of
Pediatrics11 (25%, affiliated vs. 16%,nonaffiliated; p < 0.05), the AmericanMedical Association12 (25%, affiliated vs.15%, nonaffiliated; p < 0.05), and theAmerican Society for Blood and MarrowTransplantation13 (13%, affiliated vs. 8%,nonaffiliated; p = NS).
Willingness to speak about UCBdonation, adequacy of information,and approach to providing adviceA majority of both affiliated and nonaf-filiated obstetricians reported that theywere confident discussing UCB optionswith their patients: 80% versus 70%,
TABLE 1. Demographics of survey respondentsSurvey respondentdemographics Affiliated Nonaffiliated
Role in clinical practice n = 137 n = 155Supervise residents 69%* 38%*Do not supervise
residents31% 62%
Bed size of hospital n = 134 n = 143Mean bed size (standarddeviation)
484.5 (296.6) 320 (192.5)
Years in practice n = 138 n = 156<5 4% 3%5-9 15% 14%10-19 29% 30%20-29 34% 37%30-39 17% 15%�40 1% 1%
Number of deliveries permonth
n = 136 n = 151
5 or fewer 15% 9%6-9 14% 6%10-19 50% 58%20 or more 21% 27%Mean number of
deliveries/month (�SD)13.9 (�14.3) 16.1 (�12.3)
Sex of respondent n = 138 n = 155Male 51% 64%*Female 49% 36%*
* p < 0.05.
23% 59% 17% 1%Nonaffiliated
38% 50% 11% 1%Affiliated
0% 20% 40% 60% 80% 100%
% Familiar with UCB in transplant therapy
Very familiar Somewhat familiar Not very familiar Not at all familiar
Fig. 1. Familiarity of obstetricians with the use of UCB in transplant therapy.
AWARENESS OF PUBLIC CORD BLOOD BANKING
Volume 52, April 2012 TRANSFUSION 789

respectively (p = NS). In response to another question,however, obstetricians were less confident about theirability to answer patients’ questions about UCB donation.Among affiliated and nonaffiliated obstetricians, approxi-mately half (49 and 51%, respectively) disagreed orstrongly disagreed that they had enough informationabout donating UCB to answer questions patients mighthave.
Respondents were asked to estimate the percentageof their patients who ask for information about: 1) donat-ing their baby’s UCB to a public bank and 2) privatelystoring their baby’s UCB. The mean percentage of patientsasking about public donation was significantly higheramong affiliated obstetricians compared to nonaffiliatedobstetricians: 24.5% versus 9.7%, respectively (p < 0.05).There was no significant difference in the percentage ofpatients asking about private storage: 27.3%, affiliatedversus 22.1%, nonaffiliated (p = NS).
Female affiliated obstetricians report that signifi-cantly more patients asked them for information aboutdonating UCB to a public CBB compared to their malecolleagues: 30.2% versus 18.9%, respectively (p < 0.05).
Respondents were asked the open-ended question “Ifa patient asks you for your opinion about what she shoulddo with her baby’s cord blood, what do you tell her?”Responses were coded and categorized for comparisonand are summarized in Table 3.
The most common response, among both affiliated(37%) and nonaffiliated (41%) obstetricians, was todiscuss all options and benefits, but let the patient decide.This is consistent with the ACOG position statement onUCB banking.10
Willingness to collect UCB for public donation andperception of barriers to UCB collectionRespondents were asked to estimate the frequency of thefour postdelivery actions regarding UCB: discard, collectfor public CBB, collect for private CBB, or collect forresearch (Table 4). Each respondent’s estimates wererequired to add up to 100%. Nonaffiliated obstetricianswere significantly more likely to discard UCB and, not sur-prisingly, significantly less likely to collect UCB for dona-tion to a public CBB.
TABLE 2. Percentage of respondents who agree or strongly agree with statements on UCBT with referencesprovided for accuracy of statement
Statement on clinical use of UCBT
% Agree or strongly agree Accuracy ofstatementAffiliated Nonaffiliated
A cord blood transplant is a suitable alternative to a transplant from an adult marrow donor 70 65 Accurate2-8
Many patients who could benefit from a cord blood transplant would be able to find amatching cord blood unit from an unrelated donor
56 55 Accurate3,17-19
Cord blood is especially useful for patients who need a transplant quickly 48* 41* Accurate2,17,20,21
A transplant with a person’s own cord blood is almost always preferable to using cord blooddonated from someone else
53 64 Inaccurate10,11,13
Cord blood transplants are only used for pediatric patients 4 7 Inaccurate2,3,5-8
*p < 0.05.
TABLE 3. Coded and categorized responses to “If a patient asks you for your opinion about what she should dowith her baby’s cord blood, what do you tell her?”*
Response Affiliated (%) Nonaffiliated (%)
Discuss all options and benefits—leave decision to patients 37 41Encourage donation to a public bank 32 11Recommend either public donation or private storage; discourage patient from discarding 11 17If family history warrants it, privately store the blood 9 12Privately bank baby’s blood if it is affordable 8 11Private banking is the best option 5 10Private banking is not worth the cost 5 5
* Respondents could offer more than one response. Only responses mentioned by at least 5% of respondents are shown.
TABLE 4. Mean percentages of the disposition of UCB after deliveryDisposition of UCB after delivery Affiliated (%) Nonaffiliated (%) p value
Discard umbilical cord and cord blood 58 82 <0.05Collect cord blood for donation to a public CBB 26 5 <0.05Collect cord blood for storage with a private CBB 13 10 NSCollect cord blood for a research study 3 3 NS
WALKER ET AL.
790 TRANSFUSION Volume 52, April 2012

To assess perceptions about barriers to public UCBcollection, respondents were given a list of reasons whyobstetricians might not collect UCB for public donationand asked whether they agreed or disagreed with thestatements (Table 5). More than one-third of affiliated andnonaffiliated obstetricians strongly agreed or agreed thatlack of compensation for doctors is a barrier to a publicUCB collection: 36% versus 35%, respectively (p = NS).This reason topped the list of barriers to collection. Sig-nificantly more nonaffiliated obstetricians agreed thatprivate UCB collection was easier than collection for apublic bank and that there were too many restrictions ondonating UCB for public banking.
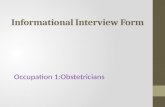
Nonaffiliated obstetricians were asked to rate theirlikelihood of participating in four different UCB-relatedactivities if their hospital became affiliated with a publicCBB. A majority were likely or somewhat likely to support
public UCB banking activities, such as discussing andencouraging patients to donate UCB and collaboratingwith colleagues and hospital administration to supportpublic banking efforts (Fig. 2).
DISCUSSION
Overall, obstetricians have a good understanding of UCBTand the differences between public donation and privatestorage of UCB, although some misperceptions exist. Alarge majority of the obstetricians surveyed know thatUCBT is a suitable alternative to a transplant from anadult marrow donor. This is consistent with research pub-lished in the past decade showing that UCBT outcomesusing HLA-matched or partially mismatched unrelatedUCB (i.e., UCB units from public CBBs) can be compa-
TABLE 5. Barriers to collecting UCB for public donation, showing percentage of respondents who agree orstrongly agree with statements shown
Statement
% Agree or strongly agree
Affiliated Nonaffiliated
There is no compensation for doctors to collect cord blood for donation 36 35Hospital administration is not supportive of efforts to collect cord blood for donation 14 N/AIt is better for parents to store their baby’s cord blood with a private bank 13 18Easier to collect cord blood for a private bank rather than for a public bank 9* 18*Collecting cord blood takes too much time after delivery 7 10Lack of familiarity with cord blood collection techniques 4 6There are too many restrictions regarding which women can donate their cord blood 3* 11*Many of my patients would not be eligible to donate cord blood 3 6
* p < 0.05.
49%
62%
67%
33%
33%
30%
14%
4%
2%
4%
1%
1%
Encourage colleagues to collect cord blood for donation
Encourage patients to donate their baby's cord blood
Talk to patients about donating their baby's cord blood
%61%53%64 3%
0% 20% 40% 60% 80% 100%
Work with hospital administration
to encourage a partnership
with a public CBB
Very likely Somewhat likely Not likely Don't know
Fig. 2. Likelihood of nonaffiliated obstetricians participating in UCB donation activities if their hospital were to become affiliated
with a public CBB.
AWARENESS OF PUBLIC CORD BLOOD BANKING
Volume 52, April 2012 TRANSFUSION 791

rable to transplant outcomes using unrelated donormarrow or peripheral blood stem cells obtained fromadult donors.4-8
In addition, a significant majority of the obstetricianssurveyed are aware of the utility of UCBT in adults: a highpercentage of respondents disagreed or strongly disagreedthat UCBT is only used for pediatric patients (87%, affili-ated vs. 77%, nonaffiliated; p = NS). Thus, obstetriciansseem aware of current research showing that UCBT isbeing increasingly and successfully used in adultpatients.2,5-8 However, the survey also revealed some mis-perceptions concerning the clinical application of UCB,most notably the belief by a majority of obstetricians thatUCBT with a person’s own UCB, that is, autologous, isalmost always preferable to using UCB donated fromsomeone else.
Research has shown that autologous transplantationusing the baby’s own UCB is not suitable for treatmentof genetic diseases such as genetic marrow failure andimmunodeficiency syndromes, metabolic storage dis-eases, and hemoglobinopathies.14,15 As stated in the ACOGcommittee opinion, autologous UCB cells would carry thesame genetic mutation that leads to the original disease.10
Further, although there have been limited reports ofautologous UCBT for leukemia,15 research has shown thatleukemic or preleukemic cells may be present in the neo-natal blood of children later diagnosed with leukemia.16 Inaddition, the lack of a graft-versus-leukemia effect inautologous transplantation would suggest that an autolo-gous UCBT would not be the optimal cell source forpatients with leukemia.10
Although nearly all obstetricians knew that privateCBBs charge fees to collect and store UCB, significantlyfewer nonaffiliated obstetricians were aware that there isno cost to women who donate their baby’s UCB to a publicbank (69%, nonaffiliated vs. 86%, affiliated; p < 0.05). Thisindicates an area where more education could improvethe accuracy of information obstetricians are providing toexpectant mothers.
It is interesting to note that a majority of obstetriciansreport awareness of the current ACOG committee opinionon UCB banking, although the survey did reveal thatapproximately half of obstetricians (49%, affiliated; 51%,nonaffiliated) feel that they have insufficient knowledge ofUCB donation to effectively answer patients’ questionsabout donating UCB. This indicates a need for educationalopportunities for obstetricians to become more aware ofUCB collection and the utility of UCB donated to a publicbank compared with private storage.
The survey also found that obstetricians will supportefforts to grow the public inventory of UCB units in thefuture: Nonaffiliated obstetricians indicated that theywere likely or somewhat likely to support public bankingby encouraging their patients to donate (95%) and byencouraging their colleagues to collect (82%).
UCB collections for private storage are comparable ataffiliated and nonaffiliated hospitals (13% vs. 10%, respec-tively) suggesting that the opportunity to increase publicUCB donation would not appear to be at the expense ofprivate storage. Therefore, concerns about competitionbetween public and private banking seem minimal.
There also do not appear to be any significant barriersto increasing donations. As shown in Table 5, there are nomajor barriers that could affect the ability of achievingthis goal. Only one potential barrier had a noteworthyresponse, the lack of compensation to obstetricians forUCB collection, and only 36% of affiliated and 35% of non-affiliated obstetricians raised this as a concern.
There is a good basis to assume that as efforts toincrease the national inventory of publicly available UCBunits move ahead, there will continue to be supportamong obstetricians. This will be key to achieving inven-tory goals, because obstetricians play an important role inthe decision to donate as well as the actual donationprocess.
The steady increase in UCBT during the past decadewould not have been possible without the altruistic dona-tions from mothers of their baby’s UCB to public banksand the support of their obstetricians. Expansion of thiseffective therapy to more patients will come aboutthrough increasing collection activity. This effort will beadvanced if practitioners take steps to strengthen knowl-edge of public UCB donation and remove barriers to UCBcollection.
ACKNOWLEDGMENTS
The authors wish to thank Barbara Krinke for assistance in survey
development, and Tammy Miller and Daniel Campbell for assis-
tance in manuscript preparation.
CONFLICT OF INTEREST
The authors declare that they have no conflict of interest or finan-
cial involvement with this manuscript.
REFERENCES
1. Gluckman E, Broxmeyer HE, Auerbach AD, Friedman HS,
Douglas GW, Devergie A, Esperou H, Thierry D, Socie G,
Lehn P, Cooper S, English D, Kurtzberg J, Bard J, Boyse EA.
Hematopoietic reconstitution in a patient with Fanconi’s
anemia by means of umbilical-cord blood from an HLA-
identical sibling. N Engl J Med 1989;321:1174-8.
2. Ooi J. Cord blood transplantation in adults. Bone Marrow
Transplant 2009;44:661-6.
3. Smith AR, Wagner JE. Alternative haematopoietic stem cell
sources for transplantation: place of umbilical cord blood.
Br J Haematol 2009;147:246-61.
WALKER ET AL.
792 TRANSFUSION Volume 52, April 2012

4. Eapen M, Rubinstein P, Zhang MJ, Stevens C, Kurtzberg J,
Scaradavou A, Loberiza FR, Champlin RE, Klein JP, Horow-
itz MM. Outcomes of transplantation of unrelated donor
umbilical cord blood and bone marrow in children with
acute leukaemia: a comparison study. Lancet 2007;369:
1947-54.
5. Eapen M, Rocha V, Sanz G, Scaradavou A, Zhang MJ,
Arcese W, Sirvent A, Champlin RE, Chao N, Gee AP, Isola L,
Laughlin MJ, Marks DI, Nabhan S, Ruggeri A, Soiffer R,
Horowitz MM, Gluckman E, Wagner JE. Effect of graft
source on unrelated donor haemopoietic stem-cell trans-
plantation in adults with acute leukaemia: a retrospective
analysis. Lancet Oncol 2010;11:653-60.
6. Hwang WY, Samuel M, Tan D, Koh LP, Lim W, Linn YC. A
meta-analysis of unrelated donor umbilical cord blood
transplantation versus unrelated donor bone marrow
transplantation in adult and pediatric patients. Biol Blood
Marrow Transplant 2007;13:444-53.
7. Atsuta Y, Suzuki R, Nagamura-Inoue T, Taniguchi S, Taka-
hashi S, Kai S, Sakamaki H, Kouzai Y, Kasai M, Fukuda T,
Azuma H, Takanashi M, Okamoto S, Tsuchida M, Kawa K,
Morishima Y, Kodera Y, Kato S. Disease-specific analyses of
unrelated cord blood transplantation compared with unre-
lated bone marrow transplantation in adult patients with
acute leukemia. Blood 2009;113:1631-8.
8. Takahashi S, Iseki T, Ooi J, Tomonari A, Takasugi K, Shimo-
hakamada Y, Yamada T, Uchimaru K, Tojo A, Shirafuji N,
Kodo H, Tani K, Takahashi T, Yamaguchi T, Asano S.
Single-institute comparative analysis of unrelated bone
marrow transplantation and cord blood transplantation for
adult patients with hematologic malignancies. Blood 2004;
104:3813-20.
9. Stem cell therapeutic and research reauthorization act of
2010, rev. 42 U.S.C. 274k.
10. Committee on Obstetric Practice; Committee on Genetics.
ACOG committee opinion No. 399: umbilical cord blood
banking. Obstet Gynecol 2008;111:475-7.
11. American Academy of Pediatrics Section on Hematology/
Oncology; American Academy of Pediatrics Section on
Allergy/Immunology, Lubin BH, Shearer WT. AAP policy
statement: cord blood banking for potential future trans-
plantation. Pediatrics 2007;119:165-70.
12. American Medical Association Code of Medical Ethics.
Opinion 2.165: umbilical cord blood banking. Issued June
2008, based on Report of the Council on Ethical and Judi-
cial Affairs. CEJA Report 9-I-07; adopted November 2007.
13. Ballen KK, Barker JN, Stewart SK, Greene MF, Lane TA.
ASBMT committee report: collection and preservation of
cord blood for personal use. Biol Blood Marrow Transplant
2008;14:356-63.
14. Johnson FL. Placental blood transplantation and autolo-
gous banking-caveat emptor. J Pediatr Hematol Oncol
1997;19:183-6.
15. Hayani A, Lampeter E, Viswanatha D, Morgan D, Salvi SN.
First report of autologous cord blood transplantation in
the treatment of a child with leukemia. Pediatrics 2007;119:
e296-e300.
16. Gale KB, Ford AM, Repp R, Borkhardt A, Keller C, Eden OB,
Greaves MF. Backtracking leukemia to birth: identification
of clonotypic gene fusion sequences in neonatal blood
spots. Proc Natl Acad Sci U S A 1997;94:13950-4.
17. Brunstein CG, Weisdorf DJ. Future of cord blood for oncol-
ogy uses. Bone Marrow Transplant 2009;44:699-707.
18. Querol S, Rubinstein P, Marsh SG, Goldman J, Madrigal JA.
Cord blood banking: “providing cord blood banking for a
nation.” Br J Haematol 2009;147:227-35.
19. Barker JN, Byam CE, Kernan NA, Lee SS, Hawke RM, Doshi
KA, Wells DS, Heller G, Papadopoulos EB, Scaradavou A,
Young JW, van den Brink MR. Availability of cord blood
extends allogeneic hematopoietic stem cell transplant
access to racial and ethnic minorities. Biol Blood Marrow
Transplant 2010;16:1541-8.
20. Wagner JE, Gluckman E. Umbilical cord blood
transplantation: the first 20 years. Semin Hematol 2010;47:
3-12.
21. Barker JN, Krepski TP, DeFore TE, Davies SM, Wagner JE,
Weisdorf DJ. Searching for unrelated donor hematopoietic
stem cells: availability and speed of umbilical cord blood
versus bone marrow. Biol Blood Marrow Transplant
2002;8:257-60.
AWARENESS OF PUBLIC CORD BLOOD BANKING
Volume 52, April 2012 TRANSFUSION 793