Avm and cellebellar hermorrege
35
Cerebellum damage caused by Arteriovenous malformation (AVM) - an abnormal connection between arteries and veins, bypassing the capillary system A Case Study
description
Final Project for "Understanding the Brain - The Neurobiology of Daily Life"
Transcript of Avm and cellebellar hermorrege

Cerebellum damage caused by Arteriovenous malformation (AVM)
- an abnormal connection between arteries and veins, bypassing the capillary system
A Case Study

Final Project ComponentsHere are the three components required for the peer review:
The project is mainly about a real case of AVM hemorrhage
which affect the brain stem function temporarily and the
cerebellum permanently. The former was life threatening, the
latter permanently impair movements (of thought, speech and
thought)
The main functions of the cerebellum is motor coordination and
motor learning (thought/cognition is also implicated)
Anatomy and functions of the cerebellum are covered in lecture 0
through 8 in Week 8

Legend
• The narrative of the case is in white• Annotation for terms used in the narrative is
in yellow. Please skip the yellow pages if you are familiar with the term.

Main IdeaThe cerebellum contains more neurons than the rest of the brain. But what does it do?

Modulation/regulation of movement

Background • Last year, during a school reunion cruise trip, I met the wife of
one of my school mate, who suffered a life threatening stroke 10 years ago.
• I was taking the Coursera course, “Medical Neuroscience” offered by Duke University at the time.
• The wife, Mrs X, has ataxic gait, a cardinal sign of a cerebellar damage (week 8 lecture 1), apparently caused by the stroke.
• After the trip, the husband sent me her medical record.• Since I am not a medical doctor, it took me some effort to
annotate and understand what happened.• With knowledge gained from the Medi-Neuro course and this
course, I was able to have a overall understanding of the case and the resulting disabilities Mrs X suffers.

Cerebellum Disorders
• Stanford Cerebellum Examination
Mrs. X exhibits symptoms of lesions to cerebellum• Ataxic gait – characterized by a broad stance, with
wide staggering quality• Decomposition of multi-joint movements• Dysdiadochokinesia - Inability to perform rapid
alternate movements (confirmed by her husband)• All these can be seen in the following link and
reviewing Week 8 lectures will help understanding these disorders

Key points for the case study
• Stroke– AVM hemorrhage and its consequences– Brainstem damages
• Cerebellum as the modulator of movement–Motor cortex– Brain stem

How It Happened
• One evening 10 years ago, Mrs. X suffered sudden onset of severe neck pain and headache
• She soon fainted and lapsed into coma• Her husband called the ambulance to rush her
to hospital

At the hospital
1. Intubated• the insertion of a tube into an external or internal
orifice of the body for the purpose of adding or removing fluids.
2. CT brain scan indicates• cerebellar hemorrahage, and• IVH - intraventricular hemorrhage

Diagnosis1. GCS 4 • Glasgow Coma Scale
o Severe, GCS < 8-9oModerate, GCS 9–12]
oMinor, GCS ≥ 13
2. Pupils equal but sluggish to light

Operation Procedures1 Urgent craniotomy and ICP done
– a large AVM was found occupying the left cerebellum
2. A craniectomy procedure includes the removal of a bone flap
– Craniectomy – the flap is not returned right after the procedure
– Craniotomy – the flap is returned after the procedure
3. Partial removal of a clot– Partial because of profuse bleeding
4. posterior fossa decompression done – The posterior cranial fossa is part of the intracranial cavity, located between
the foramen magnum and tentorium cerebelli. It contains
the brainstem and cerebellum

Posterior Cranial Fossa

Posterior Cranial Fossaarteries and veins

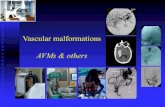
Atriovenous Malformation

Atriovenous Malformation
An AVM is a tangled bundle of blood vessels where arteries connect directly to veins with no capillary bed between.
AVM
Normal

Procedure Record (1)1. 6 cm ventricular catheter inserted – blood-stained ventricular CSF
under high pressure
2. Patient was then turned to prone position – face down
3. Supine first with right frontal burr hole made
• Supine is lying down with face up
4. Midline suboccipital incision made to expose Post Cranial Fossa and C1
(first cervical vertebrae)
Sub-occipital

Procedure Record (2)
5. The underlying brain was quite tense
6. Suboccipital craniotomy and C1 laminectomy performed• craniectomy procedure also includes the removal of a bone flap
• laminectomy is a surgical procedure that removes a portion of the vertebral bone called the lamina.
7. USG confirmed the hematoma was located at the left cerebellum, with a
diffuse AVM lying medial to the clot.• USG - ultrasound-based diagnostic imaging
• AVM – Atrovenous Malformation
8. The hematoma was actually inside the AVM nidus, making removal of clot
hazardous and bleeding from AVM arterioles was difficult
9. Finally hemostasis was secured• The cerebellum tension was fair
• ICP measured was about 10-12 mmHg

Procedure Record (3)10. No further attempt of clot removal was tried 11. Duraplasty done with fascia graft
• A reconstructive operation on the open dura mater that involves a primary closure or secondary closure with another soft tissue material (muscle, fascia, allograft dura).
12. Dura was covered with gelfoam
13. Wound closed in layers with vicryl and nylon
14. 1 wound drain Inserted
15. Keep Systolic Blood Pressure < 110 mm Hg and control
Intracranial Pressure
16. Procedure completed
17. Haematunia (blood in urine) subsided after 18 days

Procedure Record (4)
• At 23rd day, pre-operative embolization of the Left PICA done
• Posterior inferior cerbellar artery (PICA) is the largest branch of the vertebral artery, one
of three main arterial blood supplies for the cerebellum
• Embolization – deliberately blocking a blood vessel
• At 30th day, pre-operative embolization of distal right superior cerebellar artery
• At 66th day, operation to remove AVM
• Condition improved to GCS 15 points (see slide 11)
• 2 times of pre-op embolization done
• Admit for removal of AVM
• Total removal done
• Confirmed by intra-op angiogram

Summary – Principal Diagnosis
Acute bilateral cerebellar haemorrhage• underlying absormality, arteriovenous malformation• cerebellar AVM bleeding
Hydrocephalus• "water on the brain," is a medical condition in which
there is an abnormal accumulation of cerebrospinal fluid (CSF) in the ventricles, or cavities, of the brain
Respiratory failure and loss of consciousness • Temporary damages to the brain stem

Pathology
• The resulting tangle of blood vessels, often called
a nidus (Latin for "nest"), has no capillaries. It can be
extremely fragile and prone to bleeding

The Cause
• AVM in the cerebellum
• Hemorrhage caused damage to cerebellum and
brainstem
• Brainstem damage caused the cessation of normal
breathing and induced coma – loss of consciousness
• CO2 detection in the pons ; Breathing pattern generation in
the medulla (lecture 9.6)
• Lasting cerebellum disorders

Cerebellar DysfunctionMrs. X shows many effects of cerebellar damages (see Stanford Video on slide 6)
1. Ataxic gait - walking
2. Decomposition of movements– For example, touching one’s finger to one’s nose
requires the coordinated activity of shoulder, elbow, and wrist joints. Cerebellar patients must first perform the shoulder movement, then the elbow movement, and finally the wrist movement in sequence, rather than as one, uniform motion
3. Dysmetria– Instability of a limb as it approaches a target, typically
overshooting or undershooting

Cerebellar Dysfunction (cont.)
4. Intention tremor– When making a movement to a target, cerebellar
patients often produce an involuntary tremor that increases as they approach closer to the target
5. Dysdiadochokinesia– Impairment of rapid, alternate, repetitive movements
(see Stanford Video on slide 6)
6. Deficits in motor learning– cerebellar damage causes deficits in motor learning
in both human patients

Non-motor effects
• “There are ways in which the processing that the cerebellum does for motor output could also be applied to non-motor output “– thought and emotion
• In social situation, Mrs. X’s social interaction is not as agile– Slurred speech– Following multi-facet arguments or narratives
• Similar to multi-joint movement, thought process involves chunking that requires a normally functioning cerebellum

Cerebellar Plasticity and Rehabilitation
• According to some recent research, after an injuries to the cerebellum, there is a critical period of up to a few months when the cerebellum becomes plastic and relearning is easier. Many movement disorders can be reduced during this period.
• It appears that Mrs X did not receive adequate therapy and her disorders was not significantly reduced.
• There are evidences that cerebellum modulate not just movements, it also modulates thoughts and cognition. It is apparent that Mrs. X suffer, to some degree, her mental agility.

Observation
• The cerebellum is critical to all movements in our daily life; Without a
fully functioning cerebellum, our motions, motor-learning and even
thought agility will be all compromised.
• The brain is the most complex organ in our body. It is both very fragile
and plastic. A simple bleeding in the brain can cause massive, even fatal
damages. Our brain can also recover given proper treatment and
rehabilitation.

Purkinje cell sketch by Santiago Ramón j Cajal.
“I am very moved by the aesthetics of neurons that look so gorgeous like this.” - Prof. Peggy Mason, U. of Chicago
Purkinje cells of the cerebellum

Additional images

Cerelbellum

Cerelbellum

Brain Stem

Cerebellum and Brain Stem

END OF PRESENTATION
THANK YOU!