
AVDS Autumn 2015 newsletter Autumn... · comments that there is a different coloured tooth in ......
16
WELCOME to the Autumn edition of the AVDS Newsletter! Now the silly Season is behind us it’s time for the latest AVDS newsletter! It is full of information and practical tips. We hope you enjoy this edition and look forward to hearing your feedback so that we can deliver the member service that you want. ☺ AVA National Conference 2015 ☺ Exciting news for AVDS ☺ Blocking Periodontal Disease Progression with Anti- inflammatory agents ☺ What’s your diagnosis? ☺ Dangerous dentistry: keeping everyone safe. ☺ Meet your Committee – Kevin Ng ☺ Looking to learn more? ☺ Feedback: what do you want? ☺ Committee contacts Australian Veterinary Dental Society Newsletter Autumn 2015
Transcript of AVDS Autumn 2015 newsletter Autumn... · comments that there is a different coloured tooth in ......

WELCOME to the Autumn edition of the
AVDS Newsletter! Now the silly Season is behind us it’s time for the latest AVDS newsletter! It is full of information and practical tips. We hope you enjoy this edition and look forward to hearing your feedback so that we can deliver the member service that you want.
☺ AVA National Conference 2015
☺ Exciting news for AVDS
☺ Blocking Periodontal Disease Progression with Anti-inflammatory agents
☺ What’s your diagnosis?
☺ Dangerous dentistry: keeping everyone safe.
☺ Meet your Committee – Kevin Ng
☺ Looking to learn more?
☺ Feedback: what do you want?
☺ Committee contacts
Australian Veterinary Dental Society Newsletter
Autumn 2015

AVA National Conference 2015 The next AVA National Conference will be held in conjunction with the NZ Veterinary Association Conference at the Brisbane Convention and Exhibition Centre. Known as the PanPacific Veterinary Conference this huge event occurs once every 5 years and you are invited!
A full dental program is planned to stimulate and challenge your dental learning, with AVDS members sharing with small animal surgeons and anaesthetists for a number of combined sessions. A highly practical wetlab where you can learn new skills or polish your existing ones to make you a better clinician, follows. A “sneak peek” at the wetlab details is provided below to whet your appetite for learning. AVDS members receive substantial discounts to attend – 20% less than regular AVA members!
���The Extraction Workshop
11.5 Vet Ed points
Looking to brush up on your extraction skills? Acquire the advanced skills required for small animal dental exodontia? Then look no further. A day of hands-on learning, guided by some of Australia’s best.
The workshop will cover everything from simple extractions techniques to full surgical extraction of both dog and cat teeth. Included will be a workshop on small animal dental radiography. Working with equipment proudly supplied by iM3, attendees will have plenty of opportunities to use equipment they have only previously read about. Digital radiography solutions will be available for use at the workshop.
Bus departs from Brisbane Convention and Exhibition Centre at 7.30am and returns at 7.00pm.
Numbers are restricted so attendees have much more access to tutors. Book your place now!
AVA/NZVA member: $1000 SIG/SIB member: $800AVA/NZVA student member: $800Non-member: $2000

EXCITING NEWS FOR AVDS! The Federation of Asian Small Animal Veterinary Associations (FASAVA) Congress on 11–14 August 2017 now has yet another reason for you to clear your diary and make a beeline for the Gold Coast: the World Veterinary Dental Congress. ASAVA is working with the Australian Veterinary Dental Society (AVDS) to bring a not-to-be-missed dental stream to what already promises to be a huge line-up of local and international speakers covering cardiorespiratory, gastroenterology, emergency, neurology, oncology and surgery. Speakers are currently being sought and a program will be available soon. So pencil in these dates now – it will be four great days of veterinary dentistry!

WHAT IS YOUR DIAGNOSIS? A 5 month old entire male Staffordshire Bull Terrier is presented to your clinic for castration. Whilst performing the surgery your nurse monitoring the anaesthesia comments that there is a different coloured tooth in the front of the mouth. At the end of the surgery you examine the oral cavity (see photo below).
• Describe the lesion(s) present. • Why is the tooth discoloured and how did it occur? • How would you treat this clinical case? • What potential complications might you encounter?
ANSWER : Later in the newsletter!

Blocking Periodontal Disease Progression with Anti-inflammatory Agents
By Dr David E Clarke (BVSc, Dip AVDC, FAVD, MANZCVS) Advances in the identification of specific immune inflammatory pathways of periodontal
disease and the host response to bacterial plaque suggests that the action of prostaglandins can be inhibited through the use of non-steroidal anti-inflammatory drugs
(NSAIDs). The tooth is held in the jaw bone by a ligament, which attaches on one side to the tooth and the other to the bone. The gum, or gingiva, surrounds the tooth forming a space at the gum margin. The bacteria enter the space initiating inflammation and attraction of the dog’s immune cells, which firstly fight off the invading bacteria, and secondly produce enzymes that erode the bone and destroy the ligament. The erosion and destruction is termed periodontal disease and results in loss of the attachment of the tooth to the bone and subsequently loose and missing teeth. The process occurs in stages over many months to years. Our understanding of the mechanism of periodontal tissue destruction begins with bacteria attaching to the supra-gingival tooth crown and soft tissue surfaces in the oral cavity. The bacteria form a biofilm, termed ‘plaque’, which initiates a complex sequence of events that make up the inflammatory process. The process commences when plaque enters the sub-gingival sulcus resulting in the initiation of two distinct stages: vasodilation and increased capillary permeability leading to gingivitis, followed by a chronic proliferative stage of leukocyte infiltration, enzyme production and tissue destruction and fibrosis. The immune-inflammatory sequence is modulated by several types of mediators, including prostaglandins, interleukins, complement, histamine, leukotrienes, platelet activating factor and tumour necrosis factor, which are all responsible for a role in destroying or repairing periodontal tissues. THE PROSTAGLANDINS Prostaglandins, a metabolite of arachidonic acid, are released into the gingival tissues in response to tissue damage, which may be caused by several factors including the bacteria from dental plaque. Phospholipase degrades the phospholipids in the plasma membrane of cells releasing arachidonic acid, which in turn is metabolized by either cyclooxygenase to produce prostaglandins (PGE) or lipoxygenase to produce leukotrienes (Fig 1). The metabolites of arachidonic acid have been implicated in periodontal disease including chemostaxis of neutrophils, increased vascular permeability, gingivitis and

alveolar bone resorption. Prostaglandins were first implicated in 1960 as mediators of gingival inflammation and potent stimulators of alveolar bone resorption. Using crevicular fluid and gingival tissue, research has determined that periodontally diseased tissues have significantly higher levels of prostaglandins than healthy tissues. Goodson et. al, found PGE2 levels to be 10 fold higher whilst El Attar found them to be as much as 20 fold higher. Offenbacher found crevicular fluid levels of PGE2 to be increased in patients with periodontal disease. It is considered that these metabolites contribute directly to the periodontal disease process.
NSAIDS AND THEIR EFFECT ON PERIODONTAL DISEASE It logically follows that researchers would look for methods to moderate the effect of prostaglandins. In 1970s, Vane et al found that aspirin exerted its effect primarily by interfering with arachidonic acid metabolism. Therefore, since arachidonic acid and its metabolites play such an important role in disease progression, NSAIDs might be useful in the eventual treatment of the disease. Over the last 40 years this has been the case. Human patients taking NSAIDs for the treatment of rheumatoid arthritis and ankylosing spondylosis showed lower gingivitis index and shallower periodontal pockets than those not taking the drugs. Feldman, in evaluating arthritic patients taking aspirin found they had fewer periodontal sites with 10% or greater alveolar bone loss. Del Puente et al reported that NSAIDs were effective in reducing change in attachment loss of 1,386 human adult patients. These studies show great promise for the treatment of bone loss related to periodontal disease. In respect to animals, rat, monkeys, dogs and hamsters have been used for research projects. Nichols reported that induced periodontal disease using ligatures in rats showed bone
tissue
membrane phospholipid
arachidonic acid
prostaglandins leukotrienes
Fig. 1 Arachidonic acid pathway
phospholipase
cyclooxygenase lipoxygenase

metabolism was reduced in those rats treated with NSAIDs but not in those untreated. Using silk ligatures in Beagles, Nyman et al showed that when administered daily, NSAIDs slowed the initial inflammatory response as well as osteolytic bone resorption. Weakes-Dybvig et al administered NSAIDs to squirrel monkeys and found reduced loss of alveolar bone mass and loss of bone height. In addition, a decrease in osteoclast density was observed, strongly suggesting that NSAIDs are able to reduce bone loss due to periodontal disease. Interestingly though, it appeared that a NSAID is at its most effective when the animal are plaque free. As plaque accumulated at the gingival margin, the drug appeared to be less able to decrease the effects of the ongoing inflammatory process suggesting other factors are important as well. One very interesting study by Howell et al was the topical application of piroxicam on developing gingivitis in Beagles. During the 3 week study, the gingival index and number of bleeding sites was found to be significantly reduced compared to the control groups. The results suggest that topically-applied piroxicam can significantly inhibit the development of gingival inflammation in beagle dogs.
HOW DOES THIS AFFECT US IN OUR PRACTICE? Well it appears that NSAIDs are best used in conjunction with a routine regimen of oral home care and scaling and polishing. There is little point is reaching for the NSAIDs as the first line of treatment, without an adequate plaque control and elimination program in place. The use of NSAIDS in conjunction with scaling and polishing, root planning and home care should show improvements in periodontal health, reductions in gingival inflammation and alveolar bone loss. It is too early to promote a single NSAIDs over another, as no studies have been conducted in the dog and cat population, so one could assume that they all may work equally or there may indeed be a stand out. Further research should give us the much needed information to determine the best usage of these compounds in the treatment of dog and cat periodontal disease. References available on request. Please contact Dr David Clarke for more information at:
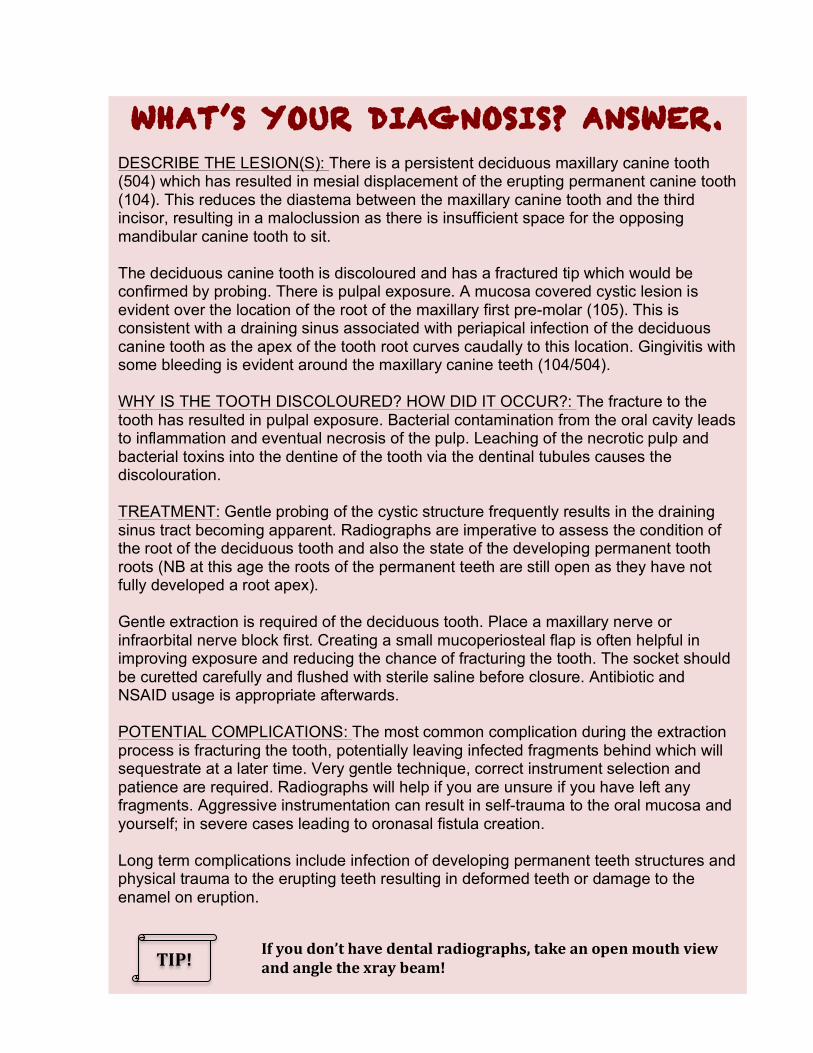
WHAT’S YOUR DIAGNOSIS? ANSWER. DESCRIBE THE LESION(S): There is a persistent deciduous maxillary canine tooth (504) which has resulted in mesial displacement of the erupting permanent canine tooth (104). This reduces the diastema between the maxillary canine tooth and the third incisor, resulting in a maloclussion as there is insufficient space for the opposing mandibular canine tooth to sit. The deciduous canine tooth is discoloured and has a fractured tip which would be confirmed by probing. There is pulpal exposure. A mucosa covered cystic lesion is evident over the location of the root of the maxillary first pre-molar (105). This is consistent with a draining sinus associated with periapical infection of the deciduous canine tooth as the apex of the tooth root curves caudally to this location. Gingivitis with some bleeding is evident around the maxillary canine teeth (104/504). WHY IS THE TOOTH DISCOLOURED? HOW DID IT OCCUR?: The fracture to the tooth has resulted in pulpal exposure. Bacterial contamination from the oral cavity leads to inflammation and eventual necrosis of the pulp. Leaching of the necrotic pulp and bacterial toxins into the dentine of the tooth via the dentinal tubules causes the discolouration. TREATMENT: Gentle probing of the cystic structure frequently results in the draining sinus tract becoming apparent. Radiographs are imperative to assess the condition of the root of the deciduous tooth and also the state of the developing permanent tooth roots (NB at this age the roots of the permanent teeth are still open as they have not fully developed a root apex). Gentle extraction is required of the deciduous tooth. Place a maxillary nerve or infraorbital nerve block first. Creating a small mucoperiosteal flap is often helpful in improving exposure and reducing the chance of fracturing the tooth. The socket should be curetted carefully and flushed with sterile saline before closure. Antibiotic and NSAID usage is appropriate afterwards. POTENTIAL COMPLICATIONS: The most common complication during the extraction process is fracturing the tooth, potentially leaving infected fragments behind which will sequestrate at a later time. Very gentle technique, correct instrument selection and patience are required. Radiographs will help if you are unsure if you have left any fragments. Aggressive instrumentation can result in self-trauma to the oral mucosa and yourself; in severe cases leading to oronasal fistula creation. Long term complications include infection of developing permanent teeth structures and physical trauma to the erupting teeth resulting in deformed teeth or damage to the enamel on eruption. TIP! If you don’t have dental radiographs, take an open mouth view
and angle the xray beam!

DANGEROUS DENTISTRY: keeping everyone safe.
Dr Jessamy Alexander BVSc (Hons) MANZCVS
PPE- most of us know that this is important. In a study published in 2013 (based on the responses of Australian vets at the AVA conference in 2011) the reported use of PPE was less than "adequate" in most scenarios. However, dental procedures (along with post mortem and surgery) was one of the few where we vets actually did pay attention to PPE. While this is great news, we can all get a little slack with using the protective gear available, as well as making sure our support staff as safe as well. The basic personal protective equipment needed for veterinary dentistry includes: • Masks • Gloves. • Safety glasses • Smock/ hat Gloves are an essential piece of personal protective equipment. In addition to protection from infectious agents, protection from mechanical injury also is provided by these items. They help you practice (universal) precautions and protect both you and the patient from cross contamination with bacteria. But also remember that many of the dental instruments (and teeth!) are quite sharp and a glove puncture and a hand wound could easily happen if you are not careful with those instruments. Dental procedures can be messy and the fluids inherent to the procedures make the gloves slippery, increasing the likelihood of injury. Be sure to have plenty of disposable gauze pads to wipe your gloves off as needed. If someone does get injured, then your gloves also protect you from direct exposure to human blood that may have contaminated the area or equipment.
Vet nurse ready for action – gloves, eye protection
and mask on!

In addition to the right type of glove, you must also have a glove that fits you. Too tight and your hands will fatigue and fingertips may become numb. Too loose and it may interfere with your control of instruments and dexterity. Consider using surgical gloves rather than non-sterile disposable gloves, as these will provide a better fit. I am sure that the stories of serious eye damage due to solid debris flying through the air have been heard before. These are not “veterinary urban legends”. Power equipment can project particles into the air several feet around the operatory area, so protective eyewear and masks are a must for all those present in the room- again this includes your nurse. You should wash the eyewear between use. If you find glasses too tight around your head- keep shopping till you find the right fit! Disposable masks with eye shields attached may also be more comfortable. Aerosolisation of bacteria is common during dental procedures. One common pathogen in the mouths of animals is Pasteurella multocida, and that organism has been linked to cardiac and pulmonary problems in humans and animals alike. As well as the extremely important mask, vets and nurses should also wear a smock and a cap. Anything you wear, as well as any exposed hair, will be contaminated with the bacteria. Therefore, it is advisable to wear removable coverings so you will not be carrying the bacteria around with you all day. In one study, irrigating the oral cavity with a 0.12% chlorohexadine solution significantly decreased bacterial aerosolisation- so rinse out the mouth with CLS at the start of the dental. General safety advice:
• Follow guidelines radiation care- radiation risks from dental diagnostic radiology risks are small, but cannot be ignored. When using xray, minimise staff in the room, use correct technique to avoid retakes, and always wear both apron and thyroid protection (which reduces exposure 98% and 50% respectively).
• Pay attention to ergonomics- Use ergonomic practices in positioning the patient, leaning over the table, and in hand position to prevent repetitive motion injuries.
• Do not eat (or drink your coffee/tea!) whilst in the dental room.
• Wearing gloves does not replace the need for handwashing. Personnel should wash their hands immediately before donning gloves, as well as afterwards.
Radiation safety – gown and
thyroid protector on!

• Follow anaesthetic guidelines to minimise risks with inhalational anaesthetics.
• Take appropriate care when using dental chemicals and developing xrays (if film is used). • Protective eyewear may also include UV shield for protection from retinal
damage, and magnification/ loops to prevent strain. • If you are continually using ultrasonic power scalers, it is possible for you to
sustain hearing loss over a long period of time. Consider ear protection. • Report malfunctioning equipment and unsafe working situations promptly.
Hopefully this will keep us all practising and enjoying dentistry for many
years to come!
NEWS FLASH: PPE isn’t just for small animal dentists! Power tool use in equine dentistry increases the need for eye and hearing protection. It also aerosolises fine particles of tooth which you don’t want to breathe in! Be safe in the paddock too.

MEET YOUR COMMITTEE
DR Kevin Ng
This edition I asked Dr Kevin Ng a couple of quick questions. Kevin is our AVDS committee member who represents Western Australia.
1. What sort of veterinary practice do you do?
100% small animal. I have an excellent foundation in general practice and have recently begun receiving referral dentistry work.
2. How did you get inspired to be interested in veterinary dentistry? I wanted to improve myself in an area where I felt that: a. I was poor at. b. I could make a difference by offering high quality services in an area where the veterinary industry still has a lot of room for improvement.
3. If you could choose any dental procedure to do what would you perform? Root canal treatment. The demanding nature of this treatment and the technical skills required provide an exciting challenge. Plus, the patient gets to retain the function of their important teeth such as canines and cutting teeth. This is especially important as teeth serve a variety of functions during play, eating and defence.
4. Best bit about dentistry AND the worst bit about dentistry. I gain the most reward out of the ability to resolve pain, infection and disease that owners frequently do not even realise is there. Unfortunately, there is still a lot of work to be done to improve the profile of oral healthcare in the pet population.
5. What do you see as the future for veterinary dentistry in Australia? I think that in order to continue to improve services in veterinary oral healthcare, the profession needs to continue to invest in a multi-pronged approach targeted at teaching universities, research institutions, undergraduate and postgraduate veterinarians, recreational pet ownership groups and the general public. Increased awareness of preventative and maintenance care, and a greater understanding of treatment options available to our patients are needed to increased the perceived value of a healthy oral cavity for our pets.
6. When you don’t have your head inside an animal’s mouth, what do you like doing?
Skiing, diving and photography. I love being outdoors and observing and photographing Australia's native plant and animal species. I have a special passion for photographing native orchids. Their morphology and biology is unique and much like Australia itself, their rugged beauty is without equal.
Thanks Kevin!

lOOKING TO LEARN MORE IN 2015 ?
Here are some upcoming CPD events that have been noted by members of the Committee . Feel free to tell us of other events you may know about in time for our next newsletter!
• 24-28 March – Essentials of equine dentistry, Grafton NSW o www.evds.net.au
• 24-30 May 2015 – PanPac Veterinary Conference, Brisbane QLD
o www.panpac2015.com
• 9-11 July – ANZCVS Science Week, Gold Coast QLD o www.anzcvs.or.au
• 19-‐20 September – University of Melbourne dental weekend
• 24-27 September – Dental and Diving Conference, Fiji o www.k9gums.com.au

Looking for a new challenge in 2015? WANTED: Veterinarian with Advanced Dental Skills Bulimba Vet Surgery in Brisbane is seeking a veterinarian who is keen to join our 4 vet practice, and is able to offer high-‐end dental skills. Ideally, these skills would include: Bite assessments & malocclusion treatment options Full mouth extractions Height reductions Nerve blocks Stomatitis treatment options Radiological competency re dental radiographs This is a GP role with plenty of scope to develop the advanced dental aspects of our practice. The ideal candidate would likely have their Membership in Dentistry and Oral Surgery. Bulimba Vet is a part of a group of seven practices, so there is also scope to develop the dental aspects of other clinics within our group. The case load is large, and the support for dentistry is well ingrained in our practice culture. This position is available from mid-‐March 2015, due to departure of our current “dental guru” who is leaving to pursue a dental internship. Please direct all enquiries to Judy Harbison BVSc via 0419 708030, or [email protected].

Thanks for reading! Don't forget to tell us
what you think.
We encourage all members to become involved in their Special Interest Group. Let us know what conditions, techniques or instruments/equipment you would like
to learn more about. What do you like about the newsletter?
Which areas could we improve or change? What else would you like to see our SIG achieve?
PRESIDENT
Dr Rod Salter – [email protected]
PRESIDENT-ELECT
Dr Tara Cashman – [email protected] SECRETARY / TREASURER Dr Amanda Hulands-Nave – [email protected]
CONTACT US!












![Research Article Modulation of Arachidonic Acid Metabolism ...downloads.hindawi.com/archive/2014/683508.pdf · metabolism of arachidonic acid to biologically active EETs [ ]. e three](https://static.fdocuments.net/doc/165x107/606ff9bcbd5c0d69301096c4/research-article-modulation-of-arachidonic-acid-metabolism-metabolism-of-arachidonic.jpg)





