Autonomic Response in Depersonalization Disorder

of 6
-
Upload
yochaiataria -
Category
Documents
-
view
216 -
download
0
Transcript of Autonomic Response in Depersonalization Disorder
-
8/13/2019 Autonomic Response in Depersonalization Disorder
1/6
Autonomic Response in Depersonalization DisorderMauricio Sierra, MD, PhD; Carl Senior, PhD; Jeffrey Dalton, MSc; Michael McDonough, MD; Alison Bond, MD; Mary L. Phillips, MD; Anne M. ODwyer, MD; Anthony S. David, MD
Background: Emotional-processing inhibition has beensuggested as a mechanism underlying some of the clini-cal features of depersonalization and/or derealization. Inthis study, we tested the prediction that autonomic re-sponse to emotional stimuli would be reduced in pa-tients with depersonalization disorder.
Methods: The skin conductance responses of 15 pa-tients with chronic depersonalization disorder accord-ing to DSM-IV , 15 controls, and 11 individuals with anxi-ety disorders according to DSM-IV, were recorded inresponse to nonspecific elicitors (an unexpectedclapandtaking a sigh) and in response to 15 randomized pic-tures with different emotional valences: 5 unpleasant, 5pleasant, and 5 neutral.
Results: The skin conductance response to unpleasantpictures was significantly reduced in patients with de-personalization disorder (magnitude of 0.017 siemens
in controls and 0.103 siemens in patients with anxietydisorders; P=.01). Also, the latency of response to thesestimuli was significantly prolongedin the group with de-personalization disorder (3.01 seconds compared with2.5 and 2.1 seconds in the control and anxiety groups,respectively; P=.02). In contrast, latency to nonspecificstimuli (clap and sigh) was significantly shorter in the
depersonalization and anxiety groups (1.6 seconds) thanin controls (2.3 seconds) ( P=.03).
Conclusions: In depersonalization disorder, auto-nomic response to unpleasant stimuli is reduced. Thefactthatpatients with depersonalization disorder respond ear-lier to a startling noise suggests that they are in a height-ened state of alertness and that the reduced response tounpleasant stimuli is caused by a selective inhibitorymechanism on emotional processing.
Arch Gen Psychiatry. 2002;59:833-838
DEPERSONALIZATION disor-der is characterized bypersistent or recurrentepisodes of detachmentor estrangement from
ones self.1 The individual may feel likean automaton, or there may be the sensa-tion of being an outside observer of onesown mental processes. 1 Manypatientshavea subjective absence of emotional feel-ings despite apparently normal emotionalexpression. 2
In contrast to the subjective natureof depersonalization, some early work 3
suggested that patients with depersonal-ization may have an underactive sympa-thetic nervous system. For example, whilemeasuring the skin conductance (SC) of a patient with anxiety, Lader and Wing 4reported a dramatic change in theSC trac-ing from the typical low-resistance, fluc-tuating pattern usually associated withanxiety to a high-resistance, nonfluctuat-ing pattern at the onset of a depersonal-ization episode. These changes were also
accompanied by a decline in pulse rate.4
A similar pattern was later reported byLader 5 in a second patient with ongoingdepersonalization. When the patient re-verted to her previous anxious state, theSC changed to extreme activity.
Using forearm blood flow as an indexof sympathetic autonomic function, Kellyand Walter 6 found that 8 depersonalizedpatients had the lowest basal recordingscomparedwith patients with a rangeof psy-chiatric disorders and controls. The find-ing that a high proportion of patients withdepersonalization disorder have high lev-
els of anxiety7
renders the previous studiescounterintuitive.Otherconditions accom-panied by high levels of anxiety, such asposttraumatic stress disorder, panic disor-der, and obsessive-compulsive disorder(OCD), have hyperactive skin conduc-tance responses (SCRs). 8-11
A recent model of depersonalizationproposed that emotional numbing andre-duced autonomic responses might be ac-counted for by inhibition of the amyg-
ORIGINAL ARTICLE
From the Institue of Psychiatry,Kings College, LondonUniversity, London, England.Dr Senior is now with theNational Institute of MentalHealth, Bethesda, Md.
(REPRINTED) ARCH GEN PSYCHIATRY/VOL 59, SEP 2002 WWW.ARCHGENPSYCHIATRY.COM833
2002 American Medical Association. All rights reserved. at Hebrew University of Jerusalem, on September 16, 2011www.archgenpsychiatry.comDownloaded from
http://www.archgenpsychiatry.com/http://www.archgenpsychiatry.com/http://www.archgenpsychiatry.com/http://www.archgenpsychiatry.com/ -
8/13/2019 Autonomic Response in Depersonalization Disorder
2/6
dala andrelated limbicstructuresby theprefrontal cortex. 2This putative inhibitory mechanism could be a compo-nent of a hard-wired protective response in thebrain.Theevolutionary benefits of such a mechanism would be toenhance chances of survivalduring life-threatening situ-ations by suppressing disorganizing levels of fear whilemaintaining vigilant alertness. 2,12 A prediction stem-ming from this model is that peoplewith depersonaliza-tion disorder will have attenuated SCRs to emotionally
unpleasant stimuli. This model also predicts that the stateof heightened alertness will generate normal or height-ened SCRs to nonspecific stimuli ( physical stimuli ) inpatients with depersonalization disorder.
To test these predictions,we compared SCRs to neu-tral and emotional visual stimuli in 15 patients withchronic depersonalization disorder, 15 controls, and 11patients with anxiety disorders. The study was ap-proved by the ethics committee of the Institute of Psy-chiatry and Maudsley Hospital, London, England.
PARTICIPANTS AND METHODS
PARTICIPANTSFifteen patients with a DSM-IV diagnosis of depersonalizationdisorder were recruited from the Depersonalization DisorderClinic at MaudsleyHospital. 13 The diagnosis of depersonaliza-tion disorder was ascertainedby means of a semistructured in-terview using the Present State Examination 14 by an experi-enced psychiatrist (M.S.) and by scores above the cutoff pointof 70 on the Cambridge Depersonalization Scale. 15 All patientshad chronic and continuous (as opposed to intermittent) de-personalization disorder of durationsrangingfrom 2 to 15 years.No patients were takingany medication at thetime of thestudy,and they were all medication free for 2 months or longer. Pa-tients with comorbid psychiatric or neurologic conditions orsubstance or alcohol abuse were excluded by means of a thor-ough standard psychiatric interview.
Eleven patients meeting DSM-IV criteria for anxiety disor-ders (5 with OCD; 6 with panic disorder with agoraphobia) wererecruited from the Behavioral Psychotherapy Unit at MaudsleyHospital. Patients were diagnosed by experienced clinicians bymeans of a thorough standard clinical interview. In addition tothe exclusion criteria applied to patients with depersonalizationdisorder,care was taken toexclude washers in theOCDsample,as frequent washing could affect SCRs. Two patients with OCDwere receiving medication (40 mg of fluoxetine hydrochlorideand 50 mg of sertraline hydrochloride). These 2 were not outli-ers on any of the psychophysiologic measurements and, hence,were retained for the data analysis.
Fifteen controls were selected from staffmembers andstu-dents at the Institute of Psychiatry, King s College. All controlsdenied a personal history of mentalillness andscored below the
cutoff points on the administered scales. No controls were tak-ing any medication.
The 3 groups were matched for sex and age because these2 variables affect electrodermalactivity. 16 All participants werepaid for their participation in the study and provided writteninformed consent.
STIMULI
Fifteen pictures selected from the International Affective Pic-tureSystem(IAPS) 17 were used. Three groups of 5 pictureswereselected by valence: neutral (IAPS numbers 1670, 7160, 7150,
7100, and7830)pleasant (IAPS numbers1463,1610, 1710, 1352,and 2530), and unpleasant (IAPS numbers 3060, 9320, 6570,6370, and 1930).
The pictures were randomized and arranged in counter-balanced order in 2 blocks. Each block was allocated ran-domly to roughly half of each group. Pictures were presentedon a color television placed 1.5 m from the participant. Eachpicture was shown for 30 seconds, followed by a 30-secondinterstimulus interval when the monitor screen was blank.Before presentation of the stimuli, 2 neutral pictures (IAPS
numbers 7170 and 7050) were presented to facilitate habitua-tion to the projection system.During the 30-second interval between pictures, partici-
pants were asked to rate the picture they hadjust seen on the di-mensions of valence (positive to negative) and arousal (excitedto calm) using the Self-Assessment Manikin, an affective ratingsystem devised by Lang. 18 Ratings of valence on the Self-Assessment Manikinare indicated by 5 graphic depictionsof themanikinwithfacialexpressionsranging froma severefrown (mostnegative) to a broad smile (most positive). Forarousal,the mani-kin varies from a state of low to high agitation. The participantcan select any of the 5 figures, or boxes in between, on a 9-pointrating scale for each dimension. Ratings are scored such that 9represents a high rating on each dimension (ie, high pleasure orhigharousal)and 1 represents a low rating on each dimension. 18
PROCEDURE
Skinconductance wasrecordedusingstandardsilver silver chlo-ride electrodes 0.5 cm in diameter. Electrodes were attached tothedistal phalangesof thefirstandsecond digitsof thenondomi-nanthand. Skinconductancewasmeasuredusing a constantvolt-age(0.6 V)SCmodule(SC4;ContactPrecisionInstruments,Cam-bridge,Mass) attachedto a personalcomputer. Water soluble jelly(KY Jelly; Johnson & Johnson, Slough, England) was used as anelectrolyte.The SC signal was sampled at 100-millisecondinter-vals. Only deflectionsgreater than or equal to 0.04 siemenswerecomputed. The timing of the stimuli presentation was synchro-nized to the SC recording program.
Before the galvanic skin resistance (response) measure-ments, all participantscompleted the followingself-ratingscales:the Beck Depression Inventory, 19 the Spielberger trait and statescales,20 and the Cambridge Depersonalization Scale. 15
To standardize the dermo-gel-electrode interface, partici-pants were requested to wash their hands using a nonabrasivesoap (Ivory soap) as recommended by Cacioppo and Tassi-nary. 21 Participants were then led into the testing room (adja-cent) and sat on a comfortable chair. After the electrodes hadbeenplacedtherewasa 5-minute habituationperiodduringwhichparticipants were asked to sit quietly, relax, and move as littleaspossible.Twominutes of baseline SC were then recorded,dur-ing which there were no stimuli and participants were in-structed not to move or talk.
Two nonspecific elicitors of SCR, a hand clap (deliveredabout 30 cm from the participant s left ear without warning)and a deep inhalation by the participant, were used to assess
the integrity of thedermoelectrical system.These 2 stimuli weredelivered 30 and 45 seconds (clap followed by sigh) after a2-minute baseline recording. These stimuli have been shownto reliably elicit SCRs from healthy individuals. 21,22 Partici-pants were then told that a seriesof slideswas goingto be shownon the television screenand they were instructed to look at eachof them carefully. During each interstimulus interval, partici-pants were asked toprovide verbal ratings onvalence (how pleas-ant the picturewas) and arousal (how agitated or moved theparticipant felt by the picture). For reference purposes, an en-larged Self-Assessment Manikin was placed below the televi-sion screen. All testing was restricted to afternoon hours
(REPRINTED) ARCH GEN PSYCHIATRY/VOL 59, SEP 2002 WWW.ARCHGENPSYCHIATRY.COM834
2002 American Medical Association. All rights reserved. at Hebrew University of Jerusalem, on September 16, 2011www.archgenpsychiatry.comDownloaded from
http://www.archgenpsychiatry.com/http://www.archgenpsychiatry.com/http://www.archgenpsychiatry.com/http://www.archgenpsychiatry.com/ -
8/13/2019 Autonomic Response in Depersonalization Disorder
3/6
(2 PM5 PM), as time of testing can be a source of confoundingeffects.16
DATA ANALYSES
Skin conductance levels and nonspecific fluctuations exceed-ing0.04 siemenswere counted during a 2-minute baseline re-cording. Amplitude was defined as the highest deflection (pha-sicincreasein conductance) from baseline initiated1 to4 secondsafter slide onset andexceeding 0.04siemens. For stimulus pre-
sentation, SCR magnitude (mean value of amplitude computedacrossall stimuluspresentations, includingthose without a mea-surable response) was obtained. A log transformation(log[SCR+1]) was used to normalize the magnitude data. Be-cause magnitude has the potential disadvantage of confound-ing frequency and amplitude, which do not always covary, anSCR probability was computed as a measure of response fre-quency above a threshold regardless of amplitude (number of responses above 0.04 siemens per total number of presentations). 23 Response latencies (temporal interval be-tweenstimulusonset andSCR initiation)were computedfor allresponses occurring 1 to 4 seconds after onset of the stimulus.In addition to the previous measurements, baseline mean con-ductance level (during theinitial 2 minutes) andnumberofnon-specific responses (ie, deflections occurring 4 seconds afterstimulus onset) during each epoch were counted.
Statistical analysis was performed using a software pro-gram (SPSS version 8; SPSS Inc, Chicago, Ill). Analysisof vari-
ance was used throughout, accompanied by post-hoc analysis(Scheffe test). An .05 was considered statistically signifi-cant, and all significance tests were 2-tailed. For the purposeofhypothesistesting,comparisonof magnitudes to stimuli acrossgroups and response latency ( Figure ) constituted the pri-mary outcome variables. All other analyses were regarded asexploratory.
RESULTS
The3 groups did not differ significantlyby age (F 2,33 =0.11;P=.89) or sex (F 2,33 =0.035; P=.96). Mean global scoreson the Beck Depression Inventory and the Spielbergerscales (state and trait) did not differ significantly be-tween individuals with depersonalization disorder andthose with anxiety disorders; controls had significantlylower scores on these scales. Global scores on the Cam-bridge Depersonalization Scale were significantlyhigherforpatients with depersonalization disorder than forcon-trols and those with anxiety disorders ( Table 1 ).
No difference was found in the ratings for valencebetween patients with depersonalization disorder andtheother 2 groups. However, 1-way analysis of variance re-
vealedsignificant differences in the arousal ratingsacrossgroups (F 2=4.9; P=.01), with depersonalized patientsre-vealing lower scores for theunpleasant pictures than theother 2 groups (Scheffe, P .05).
There was a difference in themean [SD] resting base-line level of SC across groups (F 2 =6.468; P=.004)(Table 2 ). The greatest difference (Scheffe, P .05) wasfound between patients with depersonalization disorder(1.8 [0.89] siemens)andthosewith anxiety disorders(4.1[1.8] siemens). Controls had an SC intermediate to thatin theother2 groups(2.65[1.8]siemens). Themean (SD)number of nonspecific deflections during the 2-minutebaselinerecordingshowed a similar pattern, with the low-estnumber in thedepersonalization group (1.3 [1.8]) fol-
lowed by the control (1.5 [2.8]) and anxiety (4.0 [3.1])groups. However, these differences did not reach statisti-cal significance (F 2=2.4; P=.10).
SKIN CONDUCTANCE RESPONSE
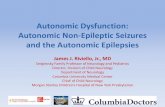
Themagnitudes of SCRs to theunpleasant, pleasant, andneutral pictures for each of the 3 groups are shown inthe Figure. Because responses to the startle noise (hand
0.30
0.25
0.20
0.15
0.10
0.05
0Depersonalization
DisorderControl s Anxie ty Disorders
Group
P r o p o r t
i o n o
f L a r g e s t
R e s p o n s e
Unpleasant StimuliPleasant StimuliNeutral Stimuli
Skin conductance response (SCR) magnitude to stimuli across groups.Because the range of SCR amplitudes can vary across participants,responses are standardized as range-corrected scores (for each participant,SCR magnitudes were computed as a proportion of that participants largestresponse).
Table 1. Global Scores on Administered Scales and Demographic Data *
Variable
DepersonalizationDisorder (D)
(n = 15)Controls (C)
(n = 15)
AnxietyDisorders (A)
(n = 11)Post Hoc Analysis(Scheff, P .05) 1-Way ANOVA
Age, y 33.8 (8.7) 34.3 (8.7) 35.6 (9.6) NS F2,33 = 0.11; P = .89Sex, F/M No. (%) 7 (49)/8 (51) 7 (49)/8 (51) 5 (49)/6 (51) NS F2,33 = 0.035; P = .96CDS score 141.7 (51.5) 19 (15.5) 46.42 (56.5) D vs C, A F2,31 = 29.7; P .001BDI score 17.57 (5.3) 2.5 (3.8) 24.2 (13.1) D, A vs C F2,30 = 25.8; P .001Spielberger scale score
State 47.4 (15.2) 29.3 (10.7) 51.78 (17.88) D, A vs C F2,32 = 7.6; P .001Trait 53 (6.2) 35 (4.7) 57 (12.7) C vs D, A F2,33 = 26; P .001
BAI score 20.5 (15.8) 10.5 (16.6) 24.3 (19.1) NS F2,29 = 1.6; P = .28
* Data are given as mean (SD) except where indicated otherwise. ANOVA indicates analysis of variance; NS, nonsignificant; CDS, Cambridge DepersonalizationScale; BDI, Beck Depression Inventory; and BAI, Beck Anxiety Inventory.
(REPRINTED) ARCH GEN PSYCHIATRY/VOL 59, SEP 2002 WWW.ARCHGENPSYCHIATRY.COM835
2002 American Medical Association. All rights reserved. at Hebrew University of Jerusalem, on September 16, 2011www.archgenpsychiatry.comDownloaded from
http://www.archgenpsychiatry.com/http://www.archgenpsychiatry.com/http://www.archgenpsychiatry.com/http://www.archgenpsychiatry.com/ -
8/13/2019 Autonomic Response in Depersonalization Disorder
4/6
clap) did not differ significantly from those to the sigh
(F2,32 =0.33; P=.76), both were collapsed into a singlevari-able (physical stimulus). There were no significant dif-ferences in the responses to the physical stimuli acrossgroups (F 2,33 =1.5; P=.36).
Because we predicted an interaction between typeof emotional stimuli and participant group (ie, a dispro-portionately lower response to unpleasant stimuli in de-personalized patients), a mixed2-factor analysis of vari-ance was used. It revealed a main effect for group(F 1,32 =14.6; P=.001) and a main effect for valence(F 2,31 =8.49; P=.001). There was also a significant group
valence interaction (F 2,32 =3.8; P=.03). Simple effectsanalyses showed that the 3 groups differed significantlyin theirSCRstounpleasant stimuli (F 2=4.13; P=.02),with
patients with depersonalization disorder having signifi-cantly lower SCRs than controls and those with anxietydisorders (Scheffe, P .05).
The group with depersonalization disorder alsohada significantly lower probability of response to the un-pleasant stimuli (F 2=7.4; P=.002), the differences beingsignificant with controls and theanxiety group (Scheffe ,P .05). Although amplitudeand SCRprobability seemedto be lower for the pleasant and neutral pictures in thedepersonalization group, the differencedidnot reach sta-tistical significance (F 2=0.03; P=.95).
Although our findings are consistent with the pre-
dicted lackofanSCR tounpleasant stimuli, they alsoshowa trend suggesting generalized hyporesponsiveness. TheSCRs to pleasant andneutral stimuli didnot differ signifi-cantlyacrossgroups, but there wasa significant main effectof group, that is, lower responses from patients with de-personalization disorder. Potentially, therefore, the inter-pretation of a specific effect for unpleasant stimuli mightbe contaminatedby a floor effectarising from the reducedresponses of the depersonalization group overall. Conse-quently, we carried out a supplementary analysis usingrange-corrected scores as suggested by Lykken and Ven-ables 24; it expresses each SCR as a proportion of that par-ticipant s largest response.Theserange-corrected means areshown in the Figure. With this transform, genuine differ-
ences betweenSCRs tounpleasant andneutralpictureswerestill evident as a group valence interaction (F 2,32 =3.7;P=.046). A valence main effect (F 2,64 =14.03; P .001) anda group main effect (F 2,32 =3.73; P=.043) were still found.This shows that even when the range of responses is cor-rected, patients withdepersonalization disorderstillshowa marked reduction in their SCRs to unpleasant stimuli.
The fact that in our set of pictures those with nega-tive valence also had the highest arousabilitymakes it dif-ficult to know whether the reduced responses seen in thedepersonalization group were arousal or valence deter-
Table 2. Skin Conductance Responses (SCRs), Latencies, and Subjective Ratings to Administered Stimuli *
Stimulus
DepersonalizationDisorder (D)
(n = 15)Controls (C)
(n = 15)
AnxietyDisorders (A)
(n = 11)Post Hoc Analysis(Scheff, P .05) ANOVA
Skin conductanceat baseline, siemens
1.8 (0.89) 2.65 (1.8) 4.1 (1.8) D vs A F2,22 = 6.4; P = .004
SCR Amplitude to Stimuli, siemensUnpleasant 0.017 (0.012) 0.074 (0.062) 0.103 (0.085) D vs C, A F2,33 = 4.13; P = .002
Pleasant 0.017 (0.02) 0.051 (0.032) 0.056 (0.054) NS F2,33 = 0.98; P = .38Pictures 0.009 (0.018) 0.032 (0.028) 0.038 (0.042) NS F2,33 = 1.1; P = .34Physical 0.261 (0.28) 0.24 (0.22) 0.35 (0.35) NS F2,33 = 0.21; P = .80
Corrected SCR Amplitude to Stimuli, siemensUnpleasant 0.07 (0.01) 0.26 (0.07) 0.27 (0.79) D vs C, A F2,26 = 5.1; P = .01Pleasant 0.07 (0.1) 0.16 (0.25) 0.19 (0.15) NS F2,26 = 1.5; P = .23Neutral 0.03 (0.05) 0.08 (0.1) 0.08 (0.07) NS F2,26 = 1.7; P = .18
Probability of SCRUnpleasant 0.2 (0.26) 0.52 (0.37) 0.71 (0.28) D vs C, A F2,33 = 7.4; P = .002Pleasant 0.15 (0.24) 0.31 (0.35) 0.41 (0.36) NS F2,33 = 1.9; P = .16Neutral 0.14 (0.22) 0.18 (0.38) 0.24 (0.19) NS F2,33 = 0.45; P = .63Physical 0.20 (0.28) 0.21 (0.42) 0.27 (0.35) NS F2,33 = 0.52; P = .57
Latency of SCR, sUnpleasant 3.01 (0.76) 2.5 (1.1) 2.1 (0.26) D vs A F2,21 = 5.2; P = .02Pleasant 2.1 (0.6) 2.4 (0.53) 1.7 (0.51) NS F2,21 = 1.7; P = .19Neutral 2.04 (0.5) 1.9 (0.6) 2.2 (0.24) NS F2,21 = 1.5; P = .21Physical 1.6 (0.5) 2.3 (0.35) 1.6 (0.89) D, A vs C F2,21 = 4.6; P = .03
Valence RatingUnpleasant 7.2 (0.96) 7.8 (0.71) 7.7 (0.76) NS F2,33 = 1.8; P = .17Pleasant 3.6 (1.3) 2.9 (0.47) 3.4 (1.10) NS F2,33 = 1.7; P = .19Neutral 4.5 (0.58) 4.5 (0.34) 4.9 (0.27) NS F2,33 = 2.9; P = .08
Arousal RatingUnpleasant 3.2 (2.01) 5.8 (2.2) 7.4 (1.47) D vs C, A F2,33 = 4.9; P = .01Pleasant 4.9 (1.6) 4.9 (1.7) 5.4 (2.1) NS F2,33 = 0.24; P = .78Neutral 4.1 (1.3) 3.6 (1.4) 3 (1.4) NS F2,33 = 0.43; P = .65
* Data are given as mean (SD). ANOVA indicates analysis of variance; NS, not significant.
(REPRINTED) ARCH GEN PSYCHIATRY/VOL 59, SEP 2002 WWW.ARCHGENPSYCHIATRY.COM836
2002 American Medical Association. All rights reserved. at Hebrew University of Jerusalem, on September 16, 2011www.archgenpsychiatry.comDownloaded from
http://www.archgenpsychiatry.com/http://www.archgenpsychiatry.com/http://www.archgenpsychiatry.com/http://www.archgenpsychiatry.com/ -
8/13/2019 Autonomic Response in Depersonalization Disorder
5/6
mined. To address this problem, we compared a subset of 2 pleasant pictures (IAPS numbers 1463 and 2352) and 2unpleasant pictures (IAPS numbers 9330 and 6570) withequivalent arousal ratings. The greatest difference be-tweengroupswaswith theunpleasant pictures, but thedif-ferencedidnotreachstatisticalsignificance (F 2=1.8; P=.09).
LATENCY OF SCR
Analysis of variance for latency of SCR onset to type of stimuli revealed a main effect for type of stimuli (physi-cal and emotional: F 1,21 =18.14; P=.001) and for group(F 1,21 =5.5; P=.001). There was also an interaction be-tween type of stimuli (physical stimuli included) andgroup (F 2,21 =4.3; P=.03). Post hoc analysesrevealed thatdepersonalizedpatients hada longer latency to unpleas-ant pictures than did patients with anxiety disorders(Scheffe, P .05). Also, depersonalized patients andthosewith anxiety disorders had a significantly shorter la-tency to physical stimuli than controls (Scheffe , P .05).
COMMENT
Toour knowledge, this is thefirststudytoexploreSCRstoemotionalstimuliindepersonalizationdisorder. Thestudyhasseveral limitations, includingthe relativelysmall samplesizes (inparticular that of the anxiety group). In addition,theanxiety group was not ideal in that it includedpatientswith 2 different disorders (panic disorder and OCD) thatmay differ in physiologic response. However, because theaim of the study was to compare patients with deperson-alization disorder, controls, and patients with high levelsofanxiety regardlessof nosologicstatus, thismightnotcon-stitutea seriousdrawback. Another limitation comes fromthe fact that the loudness of the clap and the depth of thesigh (physical stimuli)werenotrigorouslycontrolled, and,hence, these measures might have introduced a greater
source of error than the pictures.Ourfindingsshowthat, aspredictedbySierraandBer-rios, 2 depersonalization disorderseems tobeassociatedwithreducedautonomic respondingto aversivestimuli. In fact,there is no differential responding by patients with deper-sonalizationdisorder tounpleasant picturescomparedwithpleasant and neutral pictures. The absence of any differ-ential SCR to these types of emotional stimuli is striking;higher amplitude SCRs to unpleasant stimuli were foundin controls and those with anxiety disorders.
Standardizing the data to an index of response (asopposed to raw amplitude measurements) did not abol-ish the findings, suggesting that these are not due to afloor effect caused by a generalized dampening of SCRs.
Rather, our findings suggest that the SCR abnormalitiesin depersonalization disorder have tonic andphasiccom-ponents. Thus, the reduced baseline SC and fewer non-specific fluctuations suggest the presence of an inhibi-tory mechanism, which tonically inhibits sympatheticoutflow.This finding is in linewith that reported byKellyand Walter, 6 who found marked low baseline forearmblood flow in depersonalized patients.
However, the fact that patients with depersonaliza-tion disorder showed differential responses to the un-pleasant stimuli suggests that phasic inhibitory mecha-
nisms are also at play. Patients with depersonalizationdisordernotonly had fewer measurable responses to theunpleasant pictures, but when they showed a response,it had significantly lower amplitude. Also in favor of aselective inhibitory mechanism is the finding that pa-tients with depersonalization disorder had a longer SCR latency to unpleasant stimuli but not to pleasant, neu-tral, or physical stimuli. That these findings were selec-tive to theunpleasantpictures (an effect that was still ob-
servable after controlling for arousability) implies thatan adequate appraisal of valence is taking place. Indeed,subjective ratings forvalence didnotdiffer acrossgroups;therefore, the ability to judge the emotional meaning of complex scenes is preserved in depersonalization disor-der. However, these patients rated the unpleasant pic-tures as less arousing, thus paralleling the psychophysi-ologicdata. In this regard, studies 25 with healthysubjects(using IAPS pictures and the Self-Assessment Manikin)have found that SCRs mainly correlate with subjectivearousal as opposed to valence.
Thefact that there were no differences acrossgroupsto thephysical stimuli further suggests that SCRs arenotindiscriminately reduced in depersonalization disorder.
Moreover, patients with depersonalization disorder andthose with anxiety disorders had quicker responses(shorter latency) to the nonspecific stimuli than con-trols. The SCR to an unwarned stimulus, such as a clap,is a component of the startle response, which is in-creased in anxiety disorders and posttraumatic stressdisorder and probably reflectsa heightened state of alert-ness. 26 Indeed, levels of anxiety as measured by self-rating scales were raised in patients with depersonaliza-tion disorder and in those with anxiety disorders.
Taken as a whole, these results suggest the simul-taneous existence of inhibitory and facilitatory mecha-nismson specific componentsofautonomicactivity.Thus,patients withdepersonalization disorder in common with
those with anxiety disorders have similarlyhigh anxietyratings and SCRs (shorter latency of response) to non-specific stimuli,suggestiveofa state of heightenedarousal.However, only patients with depersonalization disordershow a marked diminution and delay in response to un-pleasant pictures. These findings are compatiblewith themodel proposed by Sierra and Berrios, 2 which postu-lates the simultaneousexistenceof an inhibitory mecha-nism on emotional response and an excitatory mecha-nism leading to a state of heightened alertness.
In the face of increased arousal (as suggested by theamplitude and latency responses to the physical stimuli),a reduction in SCR amplitude andincreased response la-tency to the unpleasant pictures lends empirical sup-
port to the notion that depersonalization is the manifes-tation of a protective, functional response of thenervoussystem intended to deal with life-threatening situations.However, the emergence and persistence of this re-sponse in a nonthreatening situation would result in anextremely strange experience, namely, the sudden on-set of lack of emotional feelings, things looking devoidof emotional coloring but with improved sensory defi-nition. Moreover, it is suggested that a state of height-ened alertness in theabsence of autonomic arousalmightbe conducive to a state of heightened self-observation,
(REPRINTED) ARCH GEN PSYCHIATRY/VOL 59, SEP 2002 WWW.ARCHGENPSYCHIATRY.COM837
2002 American Medical Association. All rights reserved. at Hebrew University of Jerusalem, on September 16, 2011www.archgenpsychiatry.comDownloaded from
http://www.archgenpsychiatry.com/http://www.archgenpsychiatry.com/http://www.archgenpsychiatry.com/http://www.archgenpsychiatry.com/ -
8/13/2019 Autonomic Response in Depersonalization Disorder
6/6
which is a common feature of depersonalization disor-der. From a nosologic standpoint, the marked psycho-physiologic differences between patients withdeperson-alization disorder and those with anxiety disorders lendsupport to the view that depersonalization disorder is avalid entity in its own right. This notwithstanding, it isinteresting that alexithymia andantisocial personality dis-order (conditions thought to be unrelated to deperson-alization) have recently been found to have similar psy-
chophysiologic featuresas those found in thisstudy. Thus,subjects with high scores on the Toronto AlexithymiaScale produce fewer specific SCRs to emotional visualstimuli regardless ofcategory. 23 Similarfindingshavebeenreported in individuals with developmental antisocialpersonality disorder. 27 Although alexithymia and anti-social personality disorder seem to share with deperson-alization disorder abnormalities in the experiencing of emotions, thereareclear phenomenologicdifferences.Forexample,patients with sociopathic behavior seem to havea selectivedeficit in theexperiencing of empathy andfailto react autonomically to picturesconveying distressbutnot to fearful or otherwise unpleasant pictures. 27 More-over, unlike patients with depersonalization disorder,
those with antisocial personality disorder have high lev-els of impulsivity and make overt displays of lack of em-pathy. 28 Patientswith depersonalization disorder, in con-trast, complain of subjective emotional deficits despitenormal behavioral expression. 2 Patients with alexi-thymia seem to have difficulty differentiating and ex-pressing emotionsverbally,which is thought to give riseto physiologic arousal anda negative subjective state.Un-like patients with depersonalization disorder, alexithy-mic patients have greater tonic electrodermal activityand report more arousal and displeasure in general thancontrols. 29
In conclusion, our findings support theview that de-personalization disorder is characterizedby reduced emo-
tionalreactivity toemotionalstimuli. Further work in thisarea should help in understanding this distressing disor-der and the interplay between affect and cognition.
Submitted for publication December 7, 2000; final revisionreceived September 17, 2001; accepted October 12, 2001.
This study was supported by the Col WW PilkingtonWill, Cecil Pilkington, and AP Pilkington Pilozzo Chari-table Trusts, United Kingdom.
Corresponding author and reprints: Mauricio Sierra,MD, PhD, Institute of Psychiatry, 103 Denmark Hill,London SE5 8AZ, England (e-mail: [email protected]).
REFERENCES
1. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition. Washington, DC: American Psychiatric Press; 1994.
2. Sierra M, Berrios GE. Depersonalization. Biol Psychiatry . 1998;44:898-908.3. Roth M, Argyle N. Anxiety panic and phobic disorder: an overview. J Psychiatr
Res. 1988;22(suppl 1):33-54.4. Lader MH, Wing L. Physiological Measures, Sedative Drugs and Morbid Anxiety.
London, England: Oxford University Press; 1966. Maudsley Monographs No. 14.5. Lader MH. The Psychophysiology of Mental Illness . London, England: Rout-
ledge & Kegan Paul; 1975.6. Kelly DHW,Walter CJS.The relationship between clinicaldiagnosisand anxiety,
assessedby forearm blood flowand othermeasurements. Br J Psychiatry.1968;114:611-626.
7. Simeon D, Gross S, Guralnik O, Stein DJ, Schmeidler J, Hollander E. Feeling un-real. Am J Psychiatry . 1997;154:1107-1113.
8. Pitman RK, Orr SP, Shalev AY, Metzger LJ, Mellman TA. Psychophysiologicalalterations in post-traumatic stressdisorder. Semin Clin Neuropsychiatry.1999;4:234-241.
9. McFall ME, Murburg MM, Ko GN, Veith RC. Autonomic responses to stress inVietnam combat veterans with posttraumatic stress disorder. Biol Psychiatry.1990;15:1165-1175.
10. Roth WT,WilhelmFH, Trabert W. Autonomicinstabilityduringrelaxationin panicdisorder. Psychiatry Res. 1998;80:155-164.
11. Hoehn-Saric R, McLeod DR, Zimmerli WD, Hipsley PA. Symptoms and physi-ologic manifestations in obsessive compulsive patients before and after treat-ment with clomipramine. J Clin Psychiatry. 1993;54:272-276.
12. Noyes R, Kletti R. Depersonalization in response to life-threatening danger.Compr Psychiatry. 1977;8:375-384.
13. Phillips ML, Sierra M, Hunter E, Lambert MV, Medford N, Senior C, David AS.A depersonalisation research unit: progress report. Psychiatr Bull. 2001;25:105-108.
14. Wing JK,Cooper JE,Sartorius NT.The Descriptionand Classification of Psychi- atricSymptoms: An InstructionManualfor the PSEand CATEGO Program.Cam-bridge, England: Cambridge University Press; 1974.
15. Sierra M, Berrios GE. The Cambridge Depersonalization Scale: a new instrumentfor the measurement of depersonalization. Psychiatry Res . 2000;93:153-164.
16. Venables PH, Mitchell DA. The effects of age, sex and time of testing on skinconductance activity. Biol Psychol. 1996;43:87-101.
17. Lang PJ,Bradley MM,Cuthbert BN.International AffectivePicture System(IAPS): Instruction Manual andAffective Ratings:TechnicalReport A-4.Gainesville: Cen-ter for Research in Psychophysiology, University of Florida; 1999.
18. Lang PJ. Behavioral treatment and bio-behavioral assessment: computer appli-cations. In: Sidowski JB, Johnson KH, Williams EA, eds. Technology in Mental Health Care Delivery Systems. Norwood, NJ: Ablex; 1980:119-137.
19. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measur-ing depression. Arch Gen Psychiatry. 1961;4:561-571.
20. Spielberger CD,GorsuckR, Lushene RE.TheState-Trait Anxiety Inventory-YForm.Palo Alto, Calif: Consultants Psychologists Press; 1977.
21. CacioppoJT, Tassinary LG,eds.Principlesof Psychophysiology . Cambridge, En-gland: Cambridge University Press; 1991.
22. Schneider RE, Fowles DC. A convenient, non-hydrating measurement of elec-trodermal activity. Psychophysiology. 1978;15:483-486.
23. Roedema TM, Simons RF. Emotion-processing deficit in alexithymia. Psycho- physiology. 1999;36:379-387.
24. Lykken DT, Venables PH. Direct measurement of skin conductance: a proposalfor standardization. Psychophysiology. 1971;8:656-672.
25. Lang PJ, Greenwald MK, Bradley MM, Hamm AO. Looking at pictures: affective,facial, visceral, and behavioral reactions. Psychophysiology. 1993;30:261-273.
26. HowardR, FordR. From thejumping Frenchmenof Maine to post-traumaticstressdisorder: the startleresponse in neuropsychiatry. PsycholMed.1992;22:695-707.
27. Blair RJ, Jones L, Clark F, Smith M. The psychopathic individual: a lack of re-sponsiveness to distress cues? Psychophysiology. 1997;34:192-198.
28. Blair RJ. A cognitive developmental approach to morality: investigating the psy-chopath. Cognition. 1995;57:1-29.
29. Friedlander L, Lumley MA, FarchioneT, Doyal G. Testing the alexithymia hypoth-esis. J Nerv Ment Dis. 1997;185:233-239.
(REPRINTED) ARCH GEN PSYCHIATRY/VOL 59, SEP 2002 WWW.ARCHGENPSYCHIATRY.COM838
2002 American Medical Association. All rights reserved. at Hebrew University of Jerusalem, on September 16, 2011www.archgenpsychiatry.comDownloaded from
http://www.archgenpsychiatry.com/http://www.archgenpsychiatry.com/http://www.archgenpsychiatry.com/http://www.archgenpsychiatry.com/