Autologous Chondrocyte Implantation in the Talus - American
17
OrthopaedicsOne Articles Page of 99 372 16 Charcot foot Contents Introduction Pathophysiology Impact on Health Related Quality of Life Clinical Presentation Diagnosis Treatment Conclusions Other Images References 16.1 Introduction In spite of the massive amount of health system resource consumption directly attributed to diabetic foot morbidity, a 1999 editorial noted that only 3% of 6,661 clinical trials on diabetes-related Diabetic Medicine issues were concerned with diabetic foot morbidity.<1,2> The goal of this review is to provide the reader a summary of our current understanding of the disease process named after the famous French neurologist, Jean Martin Charcot, and provide evidence-supported guidance for clinical management. In 1868, Jean-Martin Charcot provided the first in-depth description of a destructive hypertrophic osteoarthropathy that affected joints of patients with tertiary syphilis.<3,4,5> Penicillin has virtually eradicated tertiary syphilis, while insulin has allowed patients with diabetes to survive and develop the longstanding peripheral neuropathy that appears to be the precursor for the development of a neuropathic (Charcot) osteoarthropathy. Our modern understanding of neuropathic (Charcot) arthopathy is based on a benchmark monograph published by Eichenholtz in 1966. He summarized the available literature and cataloged clinical, radiographic, and pathologic data in 68 consecutive patients. His light microscopy photographs demonstrate the pronounced osteoclastic activity that provides the basis of recent bone turnover and electron microscopy investigations.<6> Based on his clinical and pathologic observations, Eichenholtz proposed a timeline of the disease that was divided into three stages: , initiation of the process Stage I (Stage of Development) , the active period of the disease process when bony destruction Stage II (Stage of Coalescence) and deformity occur , commencing when the destructive process “burns out” and the Stage III (Stage of Reconstruction) bone consolidates (heals) with the resulting deformity, making the patient prone for the development of tissue failure, deep infection and the frequent necessity for lower extremity amputation
Transcript of Autologous Chondrocyte Implantation in the Talus - American
OrthopaedicsOne Articles
Page of 99 372
16 Charcot foot
Contents
Introduction
Pathophysiology
Impact on Health Related Quality of Life
Clinical Presentation
Diagnosis
Treatment
Conclusions
Other Images
References
16.1 Introduction
In spite of the massive amount of health system resource consumption directly attributed to diabetic foot
morbidity, a 1999 editorial noted that only 3% of 6,661 clinical trials on diabetes-relatedDiabetic Medicine
issues were concerned with diabetic foot morbidity.<1,2> The goal of this review is to provide the reader a
summary of our current understanding of the disease process named after the famous French neurologist,
Jean Martin Charcot, and provide evidence-supported guidance for clinical management.
In 1868, Jean-Martin Charcot provided the first in-depth description of a destructive hypertrophic
osteoarthropathy that affected joints of patients with tertiary syphilis.<3,4,5> Penicillin has virtually
eradicated tertiary syphilis, while insulin has allowed patients with diabetes to survive and develop the
longstanding peripheral neuropathy that appears to be the precursor for the development of a neuropathic
(Charcot) osteoarthropathy.
Our modern understanding of neuropathic (Charcot) arthopathy is based on a benchmark monograph
published by Eichenholtz in 1966. He summarized the available literature and cataloged clinical,
radiographic, and pathologic data in 68 consecutive patients. His light microscopy photographs demonstrate
the pronounced osteoclastic activity that provides the basis of recent bone turnover and electron microscopy
investigations.<6> Based on his clinical and pathologic observations, Eichenholtz proposed a timeline of the
disease that was divided into three stages:
, initiation of the processStage I (Stage of Development)
, the active period of the disease process when bony destructionStage II (Stage of Coalescence)
and deformity occur
, commencing when the destructive process “burns out” and theStage III (Stage of Reconstruction)
bone consolidates (heals) with the resulting deformity, making the patient prone for the development
of tissue failure, deep infection and the frequent necessity for lower extremity amputation
OrthopaedicsOne Articles
Page of 100 372
16.2 Pathophysiology
The development of peripheral neuropathy in individuals with diabetes is attributed to a complex interaction
of glycosylated hemoglobin with arterioles of both central and peripheral nerves. The resultant progressive
loss of function is first appreciated in the smallest nerve fibers, leading to conduction defects in sensory,
motor, and autonomic nerves. Precipitation of glycosylated hemoglobin at the arteriolar level is likely
responsible for many of the co-morbidities associated with diabetes.<7,8>
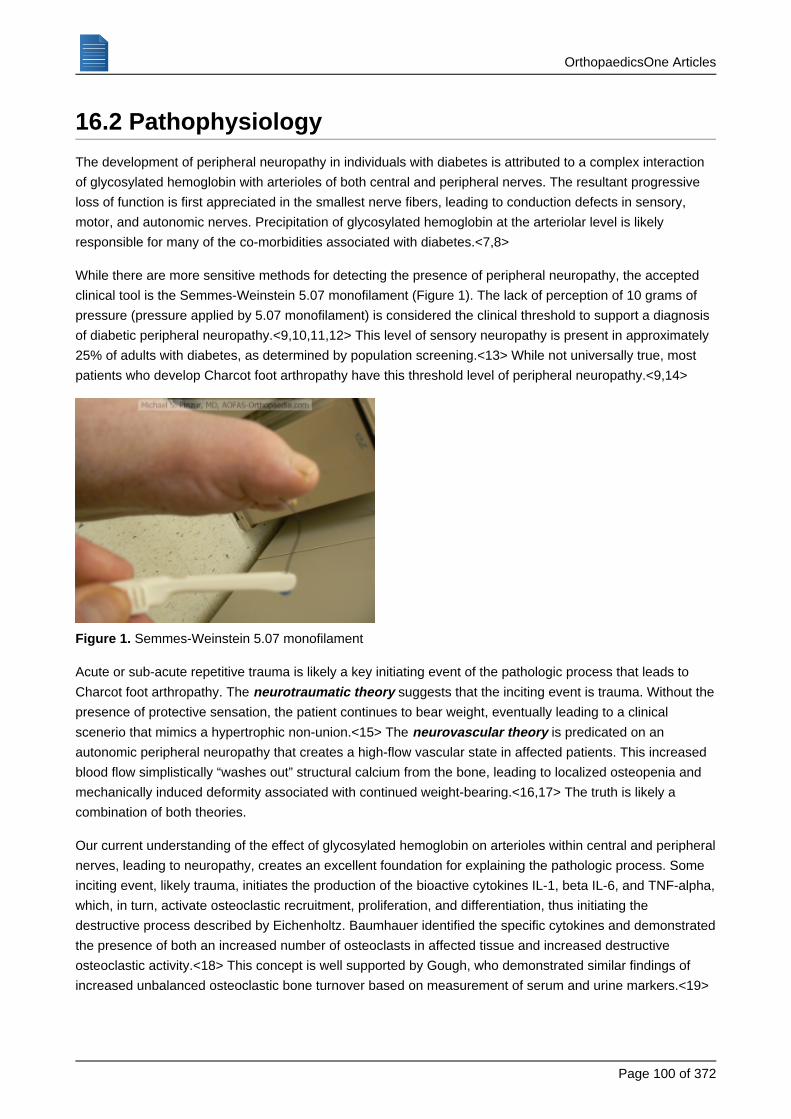
While there are more sensitive methods for detecting the presence of peripheral neuropathy, the accepted
clinical tool is the Semmes-Weinstein 5.07 monofilament (Figure 1). The lack of perception of 10 grams of
pressure (pressure applied by 5.07 monofilament) is considered the clinical threshold to support a diagnosis
of diabetic peripheral neuropathy.<9,10,11,12> This level of sensory neuropathy is present in approximately
25% of adults with diabetes, as determined by population screening.<13> While not universally true, most
patients who develop Charcot foot arthropathy have this threshold level of peripheral neuropathy.<9,14>
Semmes-Weinstein 5.07 monofilamentFigure 1.
Acute or sub-acute repetitive trauma is likely a key initiating event of the pathologic process that leads to
Charcot foot arthropathy. The suggests that the inciting event is trauma. Without theneurotraumatic theorypresence of protective sensation, the patient continues to bear weight, eventually leading to a clinical
scenerio that mimics a hypertrophic non-union.<15> The is predicated on anneurovascular theoryautonomic peripheral neuropathy that creates a high-flow vascular state in affected patients. This increased
blood flow simplistically “washes out” structural calcium from the bone, leading to localized osteopenia and
mechanically induced deformity associated with continued weight-bearing.<16,17> The truth is likely a
combination of both theories.
Our current understanding of the effect of glycosylated hemoglobin on arterioles within central and peripheral
nerves, leading to neuropathy, creates an excellent foundation for explaining the pathologic process. Some
inciting event, likely trauma, initiates the production of the bioactive cytokines IL-1, beta IL-6, and TNF-alpha,
which, in turn, activate osteoclastic recruitment, proliferation, and differentiation, thus initiating the
destructive process described by Eichenholtz. Baumhauer identified the specific cytokines and demonstrated
the presence of both an increased number of osteoclasts in affected tissue and increased destructive
osteoclastic activity.<18> This concept is well supported by Gough, who demonstrated similar findings of
increased unbalanced osteoclastic bone turnover based on measurement of serum and urine markers.<19>
OrthopaedicsOne Articles
Page of 101 372
The motor neuropathy, which initially affects smaller nerves and muscles, leads to a motor imbalance in
which the larger and stronger foot and ankle plantar-flexor muscles overpower the smaller dorsiflexors.
Recent evidence from several authors has clearly demonstrated increased static stiffness within the Achilles
tendon and the posterior ankle ligamentous tissues. This creates an intuitive pathomechanism to explain the
initiation of the destructive process. The motor imbalance created by the motor neuropathy applies an
increased bending moment during terminal stance phase of gait that apparently overloads the structures at
the midfoot level. The resultant forces appear to be responsible for upregulating the cytokines that “turn on”
the osteoclastic activity demonstrated pathologically and clinically.<20-28>
16.3 Impact on Health Related Quality of Life
The incidence of Charcot foot appears to be approximately 0.3% per year, based on a longitudinal
observational study of 3,000 Scandinavian patients with diabetes.<29> Major complications related to the
deformity occur in 4% of patients.<29,30> One hundred patients with Charcot foot arthropathy were followed
for 3 years as the target population used in validation of the AOFAS Diabetic Foot questionnaire. This
investigation demonstrated a significant negative health related quality of life impact on affected patients.
This negative impact was sustained, and not resolved following even successful treatment.<31> Similar
observations were made from a small cohort of patients being treated in a specialty diabetic foot clinic, using
the Short Musculoskeletal Assessment questionnaire (SMFA).<32>
16.4 Clinical Presentation
Patients typically present in the sixth or seventh decade. The vast majority were diagnosed with diabetes
(both Types I and II) many years earlier. Most have clinical evidence of peripheral neuropathy, as measured
by insensitivity to the Semmes-Weinstein 5.07 (10 gm) monofilament. Occasionally, patients with neuropathy
of other etiologies, such as alcohol, chemotherapy, and heavy metal, will present for treatment. Most
patients are morbidly obese. Better than half of patients can cite a specific traumatic episode, often trivial,
that initiated the process.
Patients classically were thought to present with painless swelling of affected joints. In fact, many patients
have pain associated with the swelling and deformity. While the involved foot is warm, swollen, and
erythematous, the patient has an absence of clinical signs of sepsis, such as fever, leuccocytosis, elevated
blood sugar, or increased insulin requirement. A further clinical differentiation from infection can be made by
limb elevation. The erythema will decrease with elevation associated with arthropathy, as opposed to
infection. Patients with infection generally have some element of purulent drainage. Patients with Charcot
arthropathy have drainage only if there is secondary infection of a pressure ulcer.<6,7,8,9,14,29,30,33>
16.5 Diagnosis
OrthopaedicsOne Articles
Page of 102 372
While multiple imaging techniques have been studied, the diagnosis is generally made clinically, and
supported with plain radiographs. The initial presentation is often confused with deep infection because
affected patients are generally poor hosts.<34> While several diagnostic imaging techniques have shown
promise in differentiating acute neuropathic arthropathy from infection, none has been sufficiently specific to
warrant routine use.<35> Most patients are morbidly obese, have had diabetes for more than 10 years, and
have evidence of peripheral neuropathy as measured by insensitivity to the Semmes-Weinstein 5.07 (10 gm)
monofilament.<14> Several radiographic classifications have been developed based on anatomic location
and deformity; however, most experts use the original time-line advocated by Eichenholtz.<6,37-40>
16.6 Treatment
Based on the notion that increased osteoclastic/bone turnover is the root cause of the disease process, the
parenteral bisphosphonate pamidronate has been demonstrated to decrease bone turnover and clinical
symptoms for a limited study period.<36> While many clinicians have used oral bisphosphonates with
unpublished anecdotal success, this form of treatment has not been approved for use by the US Food and
Drug Administration.
16.6.1 Eichenholtz Stage I Disease
Total Contact Cast vs. Early Arthrodesis
Up until the mid 1990s, Charcot arthropathy was thought to be a rare condition associated with any loss of
protective sensation. Experts recognized it as a destructive process, and advised immobilization and the
avoidance of further trauma by avoiding weight-bearing until the acute process resolved.<41,42>
The non-weight-bearing total contact cast, which had become popular as a treatment for diabetic foot ulcers,
was the accepted treatment standard for acute Charcot foot arthropathy. This approach was supported by
several uncontrolled retrospective case series.<9,42> There is approximately a 3% risk for the development
of iatrogenic cast-associated ulcers, which generally resolve with local wound care and cast change.<44,45>
The “gold standard” treatment of immobilization of the foot with a non-weight-bearing total contact cast until
the foot was sufficiently “stable” to afford longitudinal management with accommodative bracing, was based
on expert opinion and confirmed by retrospective case series that had no historical or benchmark standards
or a recognized description of a favorable outcome. Two retrospective case series demonstrated similar
results when patients were treated with a weight-bearing total contact cast, changed at 2-week
intervals.<46,47> Several retrospective case series supported the role of surgery for deep infection with
sepsis, osteomyelitis, or when the resultant deformities subjectively could not be managed with
accommodative bracing.<14,48-51>
Based on clinical observations that agreed with the more recently reported health-related quality of life
outcomes questionnaires, several investigators began to advise early surgical stabilization/arthrodesis with
rigid internal fixation to avoid late deformity and/or the need for cumbersome accommodative bracing.
Successful results were based on successful arthrodesis and limb salvage. No mention was made of
health-related quality of life or functional impact of disease.<23,37,48,52-59>
OrthopaedicsOne Articles
Page of 103 372
A retrospective review of patients managed in a Diabetic Foot clinic revealed that patients with a non-linear
lateral talar--first metatarsal axis, as determined from weight bearing AP radiographs, were more likely to
develop late foot ulcers than those patients with a co-linear hindfoot-forefoot axis.<60> When this
radiographic measure was combined with a clinical assessment of plantigrade vs. non-plantigrade weight
bearing, it was retrospectively demonstrated that patients who were clinically plantigrade and possessed a
colinear hindfoot-forefoot axis on weight bearing radiographs, could achieve the specific outcome of
maintaining walking independence with longitudinal management with commercially-available depth-inlay
shoes and custom accommodative foot orthoses.<61>
16.6.2 Eichenholtz Stage II and III Disease
Accommodative Bracing vs. Correction of Deformity
Currently, we do not have universally accepted definition of a "favorable outcome" that would allow
comparison between accommodative bracing and correction of deformity.
,Experts who advocate longitudinal management with accommodative bracing techniquessuch as custom-fabricated therapeutic footwear, accommodative ankle foot orthoses (AFO), or the
custom-fabricated Charcot Restraint Orthotic Walker (CROW), define favorable outcomes simply
based on limb preservation and the avoidance new ulcers or infections. As such, the reports are
retrospective case series without benchmark controls.<9,14,43,51,55,62,63,64>
advocate early arthrodesis forExperts who wish to avoid the use of accommodative orthosesacute (Stage I) disease and correction of deformity for later (Stage II and III) disease. They perceive
the accommodative orthoses as cumbersome and not well tolerated by their patients. They suggest
that correction of deformity and the provision of a stable foot allows the use of commercially available
therapeutic footwear. Without benchmark controls, they define their surgical outcomes based on
successful arthrodesis or correction of deformity. Their case series also fail to report on the perceived
positive impact on health related quality of life.<48,52,53,55-58,65>
It is well accepted that patients with long-standing diabetes who have peripheral neuropathy, morbid obesity,
and, often, severe localized osteoporosis are frequently poor surgical candidates. These characteristics put
them at high risk for mechanical loss of fixation with attempted surgical correction, as well as wound infection
or failure with extensive dissection. These observations have led many investigators to report on
non-controlled case series of patients treated surgically with correction of deformity and the maintenance
with fine wire ring external fixation in those patients arbitrarily defined as high risk for infection or mechanical
failure.<53,59,66-68>
Partial foot and Syme’s ankle disarticulation amputations have been discussed in retrospective case series
as a functional alternative to other forms of treatment.<54,69,70>
16.6.3 Ankle Fracture in Diabetics with Peripheral Neuropathy
OrthopaedicsOne Articles
Page of 104 372
Connolly was the first to report on a series of patients with diabetes who developed limb-threatening
deformity or infection following failure of internal fixation of seemingly simple ankle fractures.<71> Several
authors have reported on high complication rates associated with ankle fracture in the population of patients
with diabetes, especially those with evidence of peripheral neuropathy.<34> Several authors have
advocated augmented internal fixation combined with prolonged non-weight-bearing until radiographic
evidence of bony healing, based on case-controlled series.<13,72,73> Many patients who present with
Charcot arthropathy of the ankle initiated their disease process with an ankle fracture, often trivial and
non-displaced.
16.6.4 Charcot Ankle
Most experts currently agree that when the destructive Charcot process involves the ankle joint, the resultant
deformity is so difficult to accommodate with orthotic means that amputation becomes inevitable when
stability/joint integrity is lost. Once the joint has been irreversibly damaged, early ankle or tibiocalcaneal
arthrodesis are advised. Biomechanical evidence suggests that internal fixation with a retrograde locked
intramedullary nail affords the most stable mechanical construct.<74,75> While various applications of
blade-plating have been used to achieve ankle fusion in this complex patient population, it appears that
ankle fusion with retrograde intramedullary nailing is currently the most popular technique to achieve ankle
arthrodesis.<76-80> This technique is complicated by both early and late intramedullary infection that
requires creative methods for successful resolution.
Stress fracture of the distal tibial metaphysis is a known complication following successful ankle fusion,
regardless of the method of fixation.<13,81,82> This can be avoided by extending the ankle fusion nail to the
proximal tibial metaphysis.<75,80>
16.7 Conclusions
Charcot foot is becoming a larger clinical problem due to the increased incidence of diabetes and morbid
obesity and the improved longevity of affected patients. As the problem has become more apparent, the
interest of the orthopaedic device industry has provided improved implants for the surgical treatment of this
disorder. Increasing incidence and awareness, combined with increased interest by orthopaedic foot and
ankle surgeons and improved implants appears to predict a more favorable future for this very complex
patient population.
16.8 Other Images
OrthopaedicsOne Articles
Page of 105 372
Figure 2a.
Figure 2b.
Figure 2c.
OrthopaedicsOne Articles
Page of 106 372
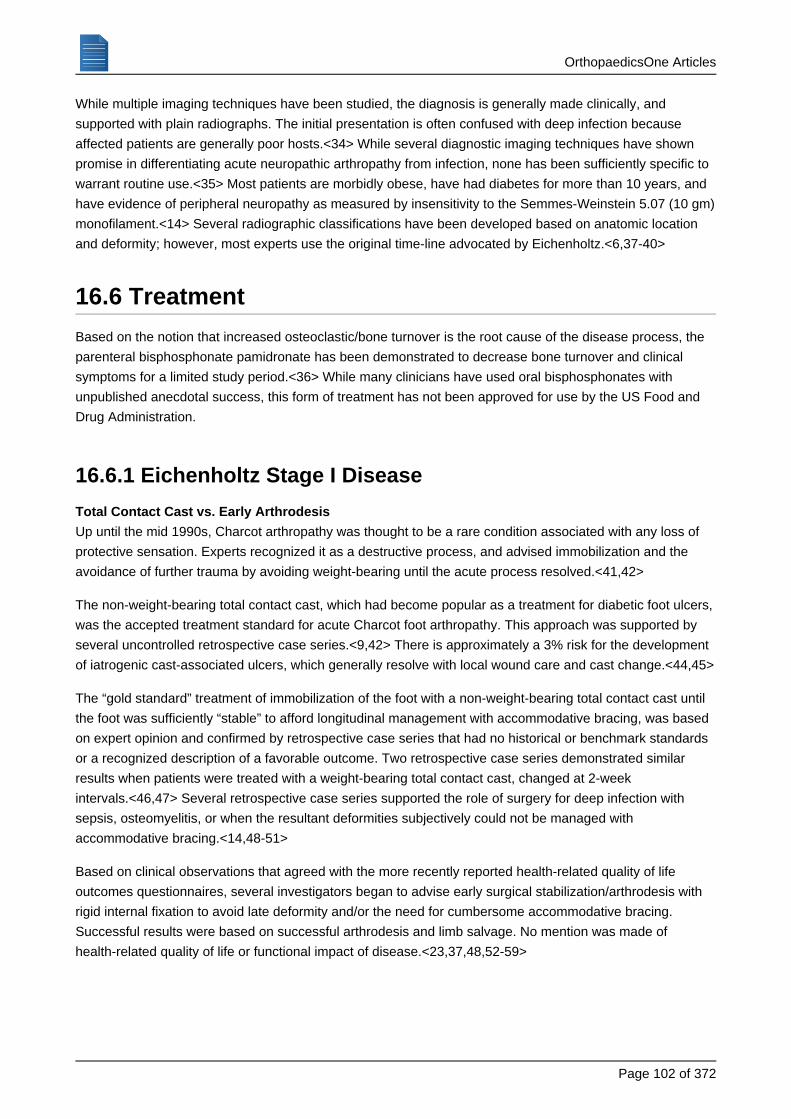
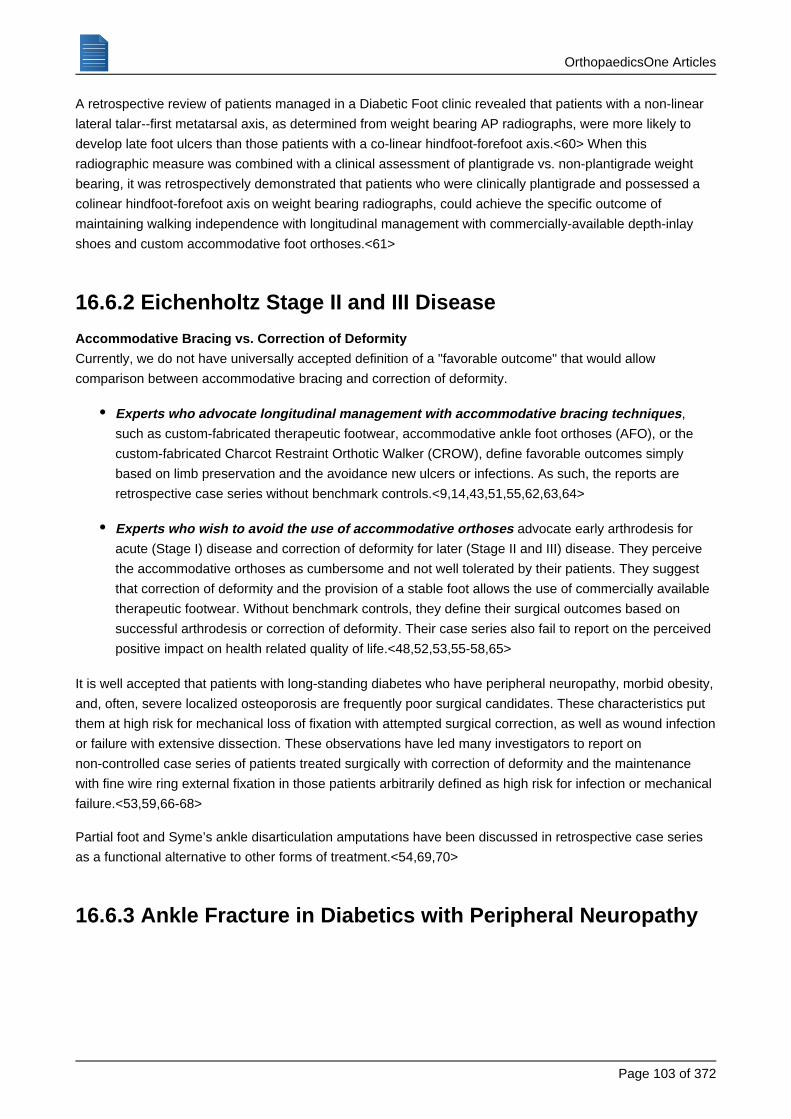
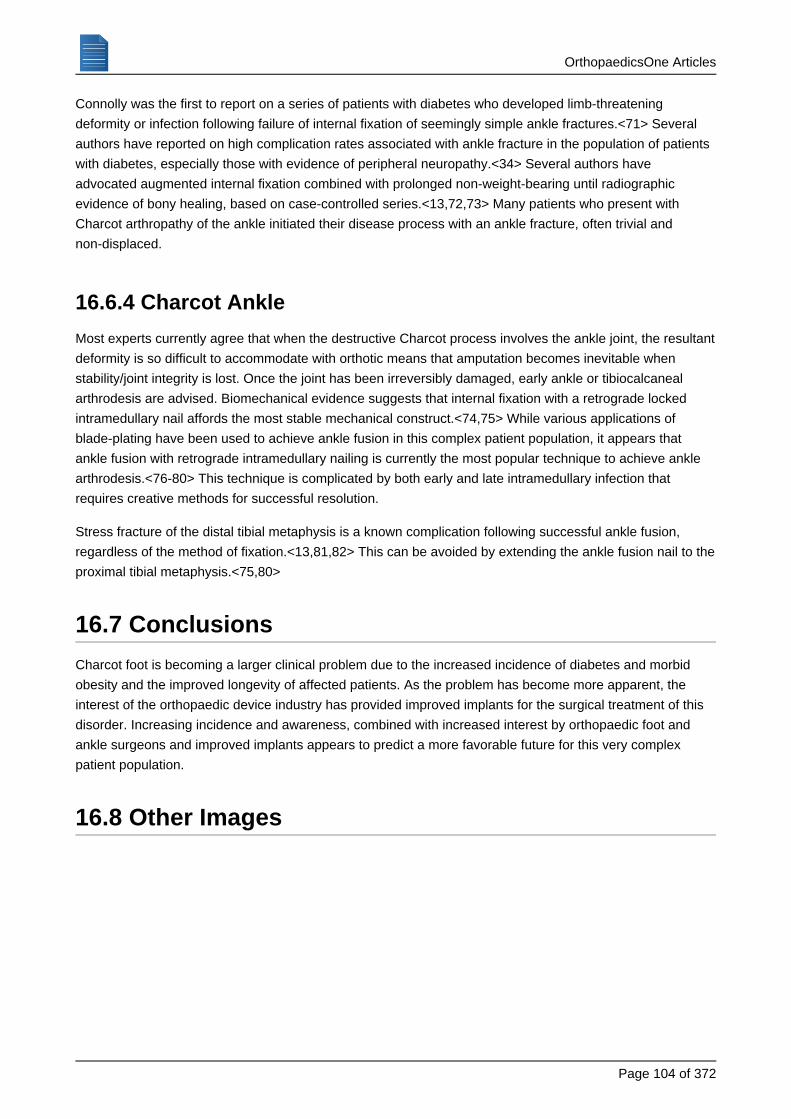
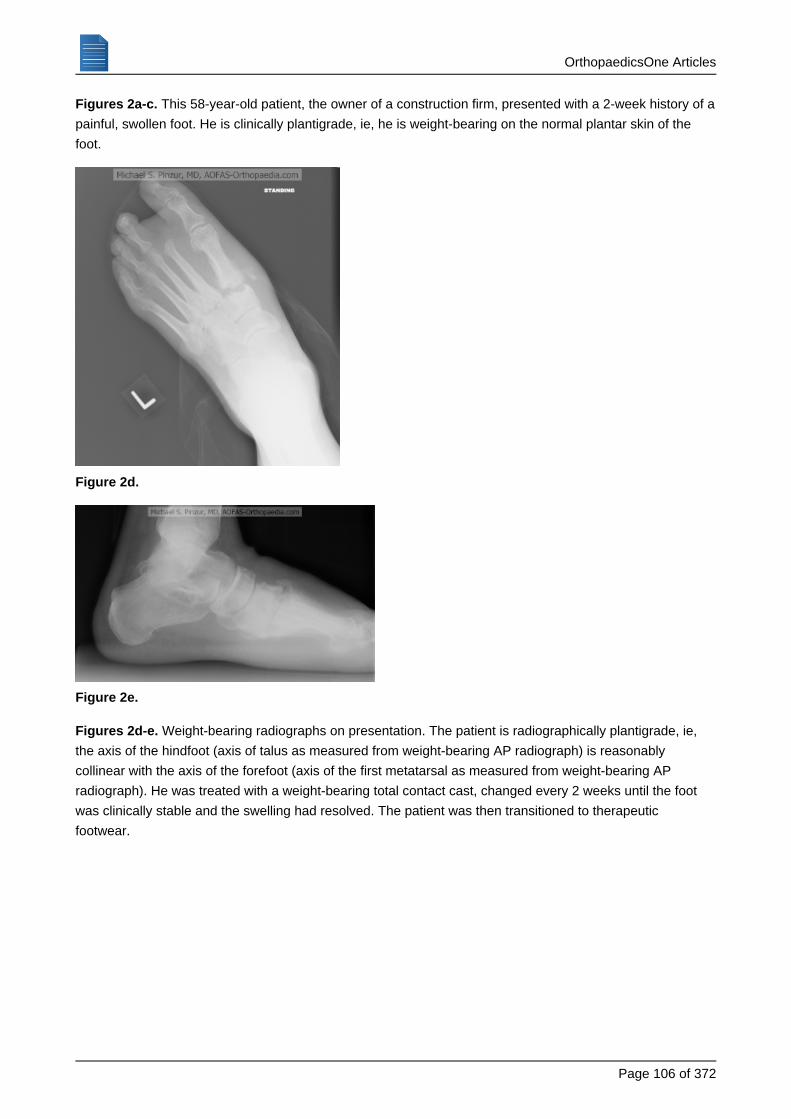
This 58-year-old patient, the owner of a construction firm, presented with a 2-week history of aFigures 2a-c.
painful, swollen foot. He is clinically plantigrade, ie, he is weight-bearing on the normal plantar skin of the
foot.
Figure 2d.
Figure 2e.
Weight-bearing radiographs on presentation. The patient is radiographically plantigrade, ie,Figures 2d-e.
the axis of the hindfoot (axis of talus as measured from weight-bearing AP radiograph) is reasonably
collinear with the axis of the forefoot (axis of the first metatarsal as measured from weight-bearing AP
radiograph). He was treated with a weight-bearing total contact cast, changed every 2 weeks until the foot
was clinically stable and the swelling had resolved. The patient was then transitioned to therapeutic
footwear.
OrthopaedicsOne Articles
Page of 107 372
Figure 2f.
Figure 2g.
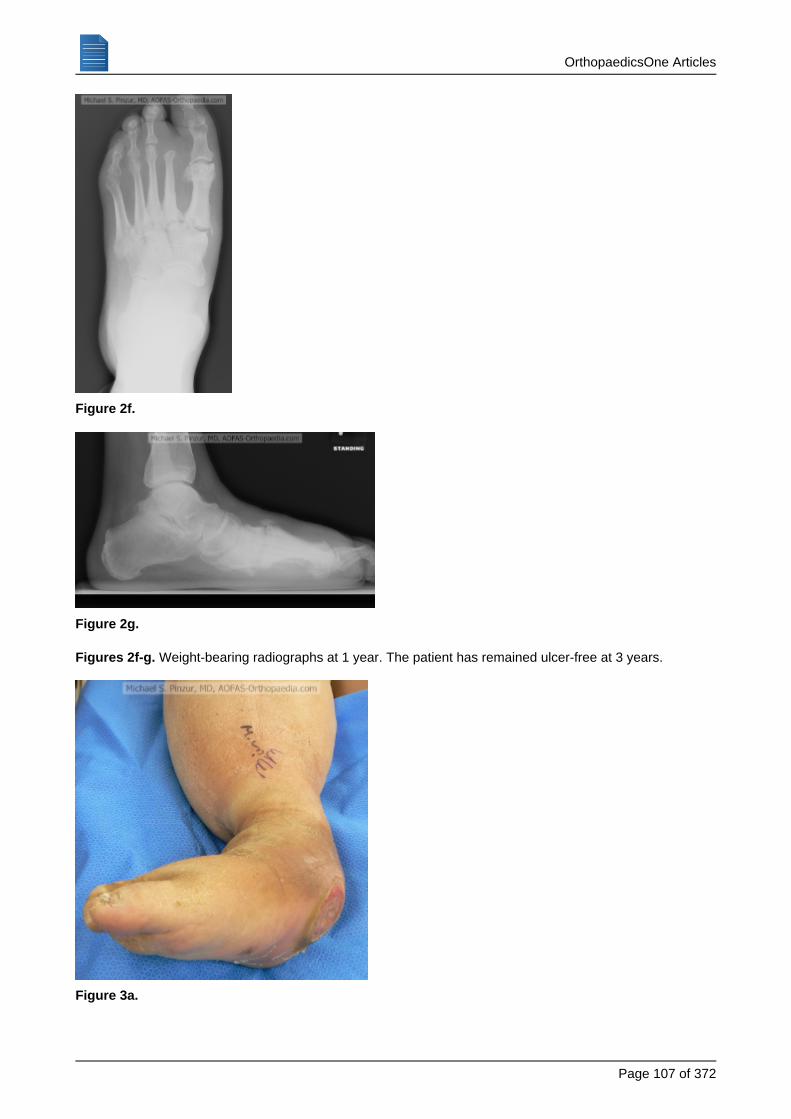
Weight-bearing radiographs at 1 year. The patient has remained ulcer-free at 3 years.Figures 2f-g.
Figure 3a.
OrthopaedicsOne Articles
Page of 108 372
Figure 3b.
Figure 3c.
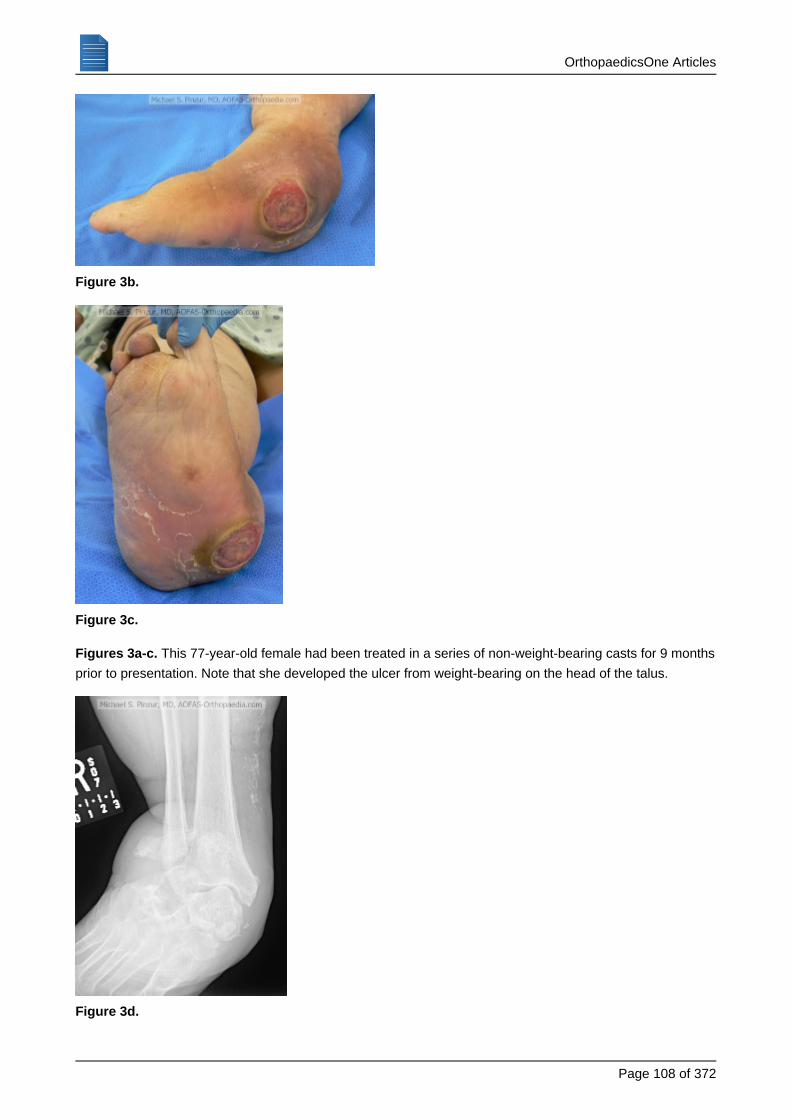
This 77-year-old female had been treated in a series of non-weight-bearing casts for 9 monthsFigures 3a-c.
prior to presentation. Note that she developed the ulcer from weight-bearing on the head of the talus.
Figure 3d.
OrthopaedicsOne Articles
Page of 109 372
Figure 3e.
Figure 3f.
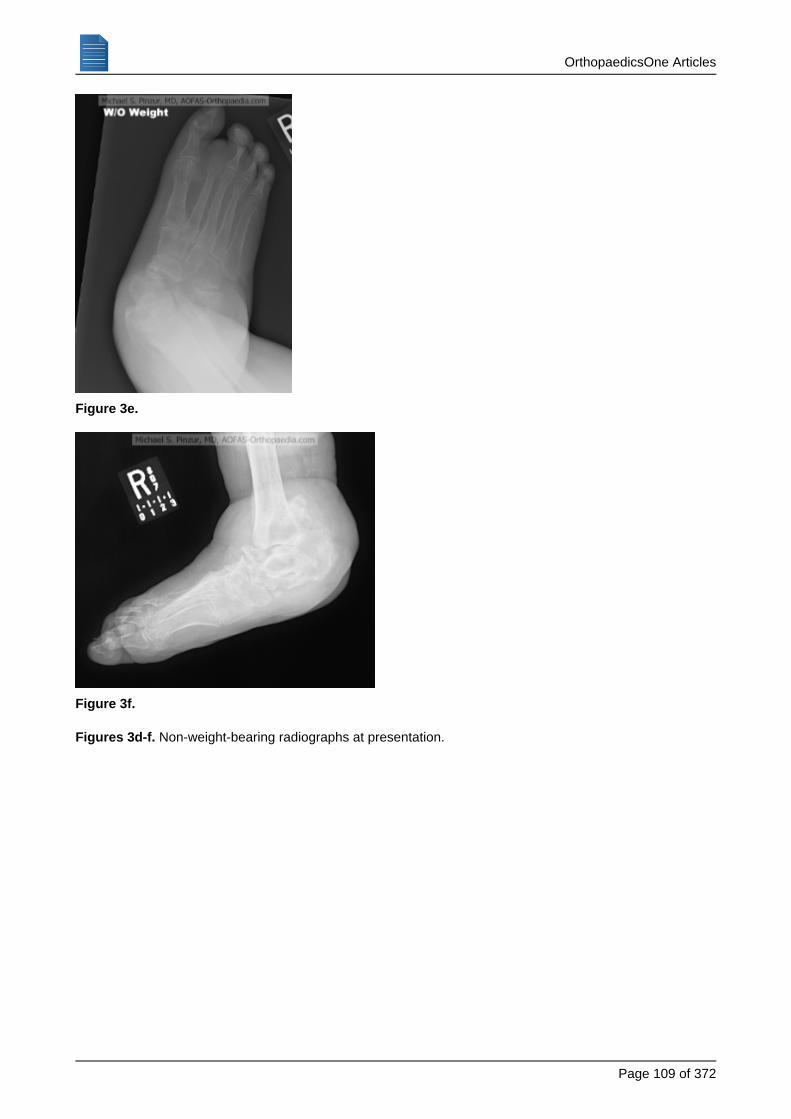
Non-weight-bearing radiographs at presentation.Figures 3d-f.

OrthopaedicsOne Articles
Page of 110 372
Figure 3g.
Figure 3h.
||
Figure 3i.
OrthopaedicsOne Articles
Page of 111 372
1.
2.
3.
4.
5.
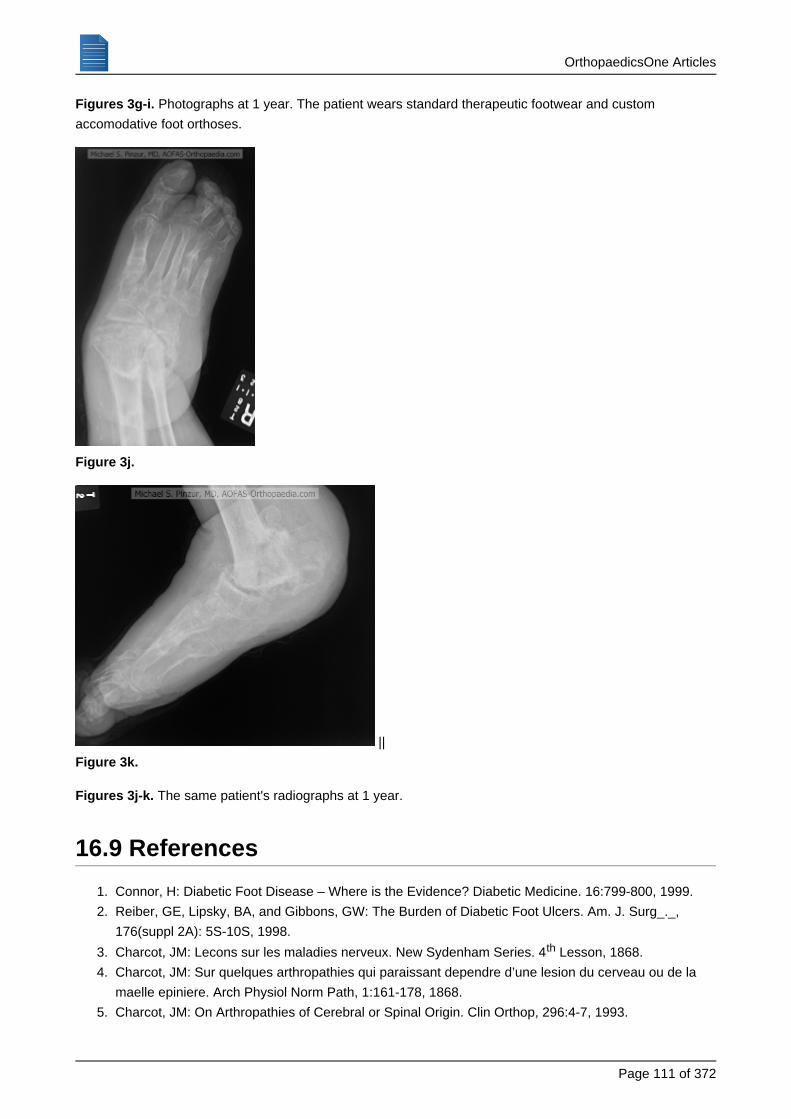
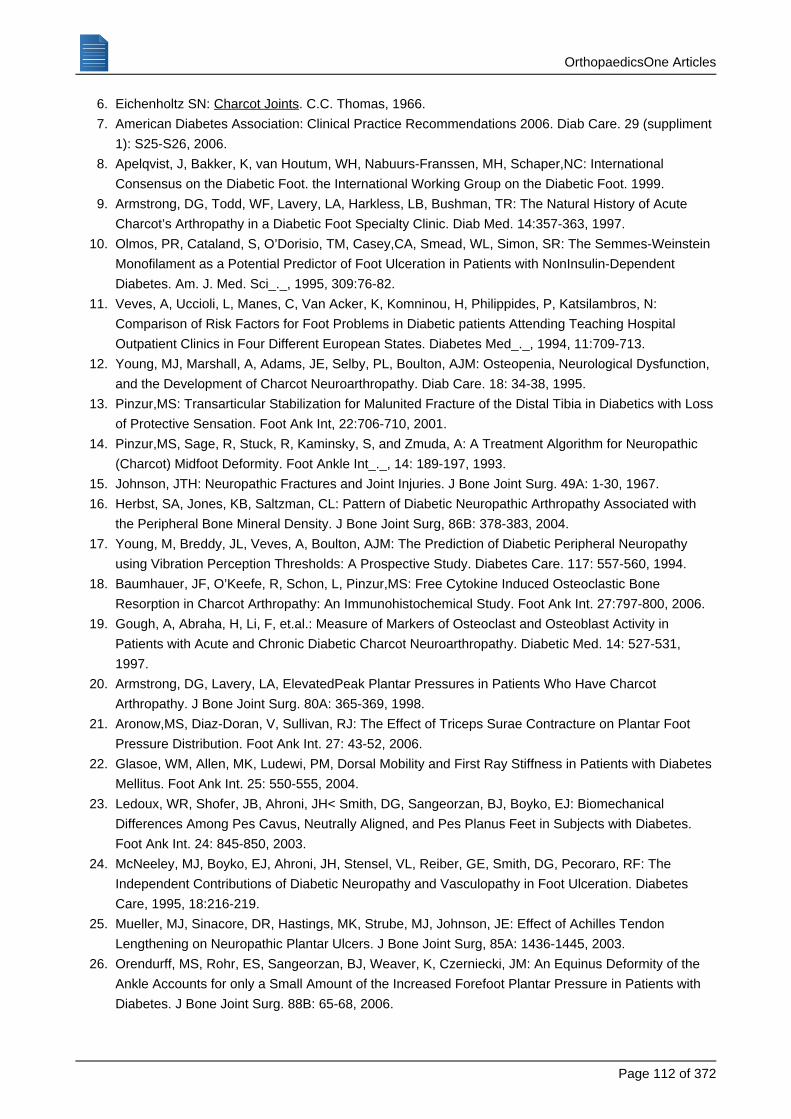
Photographs at 1 year. The patient wears standard therapeutic footwear and customFigures 3g-i.
accomodative foot orthoses.
Figure 3j.
||
Figure 3k.
The same patient's radiographs at 1 year.Figures 3j-k.
16.9 References
Connor, H: Diabetic Foot Disease – Where is the Evidence? Diabetic Medicine. 16:799-800, 1999.
Reiber, GE, Lipsky, BA, and Gibbons, GW: The Burden of Diabetic Foot Ulcers. Am. J. Surg_._,
176(suppl 2A): 5S-10S, 1998.
Charcot, JM: Lecons sur les maladies nerveux. New Sydenham Series. 4 Lesson, 1868.th
Charcot, JM: Sur quelques arthropathies qui paraissant dependre d’une lesion du cerveau ou de la
maelle epiniere. Arch Physiol Norm Path, 1:161-178, 1868.
Charcot, JM: On Arthropathies of Cerebral or Spinal Origin. Clin Orthop, 296:4-7, 1993.
OrthopaedicsOne Articles
Page of 112 372
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
20.
21.
22.
23.
24.
25.
26.
Eichenholtz SN: . C.C. Thomas, 1966.Charcot Joints
American Diabetes Association: Clinical Practice Recommendations 2006. Diab Care. 29 (suppliment
1): S25-S26, 2006.
Apelqvist, J, Bakker, K, van Houtum, WH, Nabuurs-Franssen, MH, Schaper,NC: International
Consensus on the Diabetic Foot. the International Working Group on the Diabetic Foot. 1999.
Armstrong, DG, Todd, WF, Lavery, LA, Harkless, LB, Bushman, TR: The Natural History of Acute
Charcot’s Arthropathy in a Diabetic Foot Specialty Clinic. Diab Med. 14:357-363, 1997.
Olmos, PR, Cataland, S, O’Dorisio, TM, Casey,CA, Smead, WL, Simon, SR: The Semmes-Weinstein
Monofilament as a Potential Predictor of Foot Ulceration in Patients with NonInsulin-Dependent
Diabetes. Am. J. Med. Sci_._, 1995, 309:76-82.
Veves, A, Uccioli, L, Manes, C, Van Acker, K, Komninou, H, Philippides, P, Katsilambros, N:
Comparison of Risk Factors for Foot Problems in Diabetic patients Attending Teaching Hospital
Outpatient Clinics in Four Different European States. Diabetes Med_._, 1994, 11:709-713.
Young, MJ, Marshall, A, Adams, JE, Selby, PL, Boulton, AJM: Osteopenia, Neurological Dysfunction,
and the Development of Charcot Neuroarthropathy. Diab Care. 18: 34-38, 1995.
Pinzur,MS: Transarticular Stabilization for Malunited Fracture of the Distal Tibia in Diabetics with Loss
of Protective Sensation. Foot Ank Int, 22:706-710, 2001.
Pinzur,MS, Sage, R, Stuck, R, Kaminsky, S, and Zmuda, A: A Treatment Algorithm for Neuropathic
(Charcot) Midfoot Deformity. Foot Ankle Int_._, 14: 189-197, 1993.
Johnson, JTH: Neuropathic Fractures and Joint Injuries. J Bone Joint Surg. 49A: 1-30, 1967.
Herbst, SA, Jones, KB, Saltzman, CL: Pattern of Diabetic Neuropathic Arthropathy Associated with
the Peripheral Bone Mineral Density. J Bone Joint Surg, 86B: 378-383, 2004.
Young, M, Breddy, JL, Veves, A, Boulton, AJM: The Prediction of Diabetic Peripheral Neuropathy
using Vibration Perception Thresholds: A Prospective Study. Diabetes Care. 117: 557-560, 1994.
Baumhauer, JF, O’Keefe, R, Schon, L, Pinzur,MS: Free Cytokine Induced Osteoclastic Bone
Resorption in Charcot Arthropathy: An Immunohistochemical Study. Foot Ank Int. 27:797-800, 2006.
Gough, A, Abraha, H, Li, F, et.al.: Measure of Markers of Osteoclast and Osteoblast Activity in
Patients with Acute and Chronic Diabetic Charcot Neuroarthropathy. Diabetic Med. 14: 527-531,
1997.
Armstrong, DG, Lavery, LA, ElevatedPeak Plantar Pressures in Patients Who Have Charcot
Arthropathy. J Bone Joint Surg. 80A: 365-369, 1998.
Aronow,MS, Diaz-Doran, V, Sullivan, RJ: The Effect of Triceps Surae Contracture on Plantar Foot
Pressure Distribution. Foot Ank Int. 27: 43-52, 2006.
Glasoe, WM, Allen, MK, Ludewi, PM, Dorsal Mobility and First Ray Stiffness in Patients with Diabetes
Mellitus. Foot Ank Int. 25: 550-555, 2004.
Ledoux, WR, Shofer, JB, Ahroni, JH< Smith, DG, Sangeorzan, BJ, Boyko, EJ: Biomechanical
Differences Among Pes Cavus, Neutrally Aligned, and Pes Planus Feet in Subjects with Diabetes.
Foot Ank Int. 24: 845-850, 2003.
McNeeley, MJ, Boyko, EJ, Ahroni, JH, Stensel, VL, Reiber, GE, Smith, DG, Pecoraro, RF: The
Independent Contributions of Diabetic Neuropathy and Vasculopathy in Foot Ulceration. Diabetes
Care, 1995, 18:216-219.
Mueller, MJ, Sinacore, DR, Hastings, MK, Strube, MJ, Johnson, JE: Effect of Achilles Tendon
Lengthening on Neuropathic Plantar Ulcers. J Bone Joint Surg, 85A: 1436-1445, 2003.
Orendurff, MS, Rohr, ES, Sangeorzan, BJ, Weaver, K, Czerniecki, JM: An Equinus Deformity of the
Ankle Accounts for only a Small Amount of the Increased Forefoot Plantar Pressure in Patients with
Diabetes. J Bone Joint Surg. 88B: 65-68, 2006.
OrthopaedicsOne Articles
Page of 113 372
27.
28.
29.
30.
31.
32.
33.
34.
35.
36.
37.
38.
39.
40.
41.
42.
43.
44.
45.
46.
47.
48.
Rao, SR, Saltzman, CL, Wilken, J, Yak, J: Increased Passive Ankle Stiffness and Reduced
Dorsiflexion Tange of Motion in Individuals with Diabetes Mellitus. Foot Ank Int. 27: 617-622, 2006.
Trevino, SG, Buford, WL, Nakamura, T, Wright, AJ, Patterson, RM: Use of a Torque-Range-of-Motion
Device for Objective Differentiation of Diabetic from Normal Feet in Adults. Foot Ank Int. 25: 561-567,
2004.
Fabrin, J, Larsen, K, Holstein,PE: Long-Term Follow-up in Diabetic Charcot Feet with Spontaneous
Onset. Diabetes Care, 23:796-800, 2000.
Klenerman, L: The Charcot Neuroarthropathy Joint in Diabetes Mellitus. Diab Med. 13:S52-S54,
1996.
Dhawan, V, Spratt, KF, Pinzur,MS, Baumhauer, J, Rudicel, S, Saltzman, CL: Reliability of AOFAS
Diabetic Foot Questionnaire in Charcot Arthropathy: Stability, Internal consistency and measurable
difference. Foot Ank Int. 26: 717-731, 2005.
Pinzur,MS, Evans, A: Health Related Quality of Life in Patients with Charcot Foot. Amer J Ortho.
32:492-496, 2003.
Pinzur,MS, Freeland, R, Juknelis, D: The Association between Body Mass Index and Diabetic Foot
Disorders. Foot Ank Int. 26: 375-377, 2005.
Bibbo, C, Lin, SS, Beam, HA, Behrens, FF: Complications of Ankle Fractures in Diabetic Patients.
Ortho Clin N Amer. Volume 32, 2001.
Chantelau, E: The Perils of Procrastinatio: The Effect of Early vs. Delayed Detection and Treatment of
Incipient Charcot Fracture. Diab Med. 22: 1707-1712, 2005.
Jude, EB, Selby, PL, Burgess, J, et.al.: Bisphosphonates in the Treatment of Charcot
Neuroarthropathy. A Double Blind Randomized Controlled Trial. Diabetologia. 44: 2032-2037, 2001.
Schon, LC, Easley,ME, Seinfeld, SB: Charcot Neuroarthropathy of the Foot and Ankle. Clin Orthop.
349: 116-131, 1998.
Schon, LC, Weinfgeld, SB, Horton,GA, Resch, S: Radiographic and Clinical Classification of Acquired
MidTarsus Deformities. Foot Ank Int. 19: 394-404, 1998.
Sanders, LJ, Mrdjenovich, D: Anatomic Patterns of Bone and Joint Destruction in Neuropathic
Diabetics. Diabetes. 40 (suppl 1):529A, 1991.
Thompson, RC, Clohisy, DR: Deformity following Fracture in Diabetic Neuropathic Osteoarthropathy.
J Bone Joint Surg. 75A: 1765-1773, 1993.
Brodsky, JW: The Diabetic Foot. In Coughlin, MJ, and Mann, RA: .Surgery of the Foot and Ankle
Mosby, Inc., St. Louis, 1999, pages 895-969.
Sanders, LJ, Frykberg, RG: Charcot Neuroarthropathy of the Foot. In Bowker, JH, Pfeifer,MA: The
. Mosby, St. Louis, pages 439-466, 2001.Diabetic Foot
Boninger, ML, Leonard Jr, JA: Use of Bi-Valved Ankle-Foot Orthosis in Neuropathic Foot and Ankle
Lesions. J Rehab Res Dev. 33: 16-22, 1996.
Guyton, GP: An Analysis of Iatrogenic Complications from the Total Contact Cast. Foot Ank Int. 26:
903-907, 2005.
Wukich, DK, Motko, J: Safety of Total Contact Casting in High Risk Patients with Neuropathic Foot
Ulcers. Foot Ank Int. 25: 556-560, 2004.
Pinzur,MS, Lio, T, Posner, M: Treatment of Eichenholtz Stage I Charcot Foot Arthropathy with a
Weight Bearing Total Contact Cast. Foot Ank Int. 27: 324-329, 2006.
deSouza, L: Charcot Arthropathy and Immobilization in a Weight-Bearing Total Contact Cast. J Bone
. 90A: 754-759, 2008.Joint Surg
Bono, JV, Roger, DJ, Jacobs, RL: Surgical Arthrodesis of the Neuropathic Foot. Clin Orthop. 296:
14-20, 1993.
OrthopaedicsOne Articles
Page of 114 372
49.
50.
51.
52.
53.
54.
55.
56.
57.
58.
59.
60.
61.
62.
63.
64.
65.
66.
67.
68.
69.
Brodsky, JW, Rouse, AM: Exostectomy for Symptomatic Bony Prominences in Diabetic Charcot Feet.
Clin Orthop. 296: 21-26, 1993.
Catanzariti,AR, Mendicino, R, Haverstock, B: Ostectomy for Diabetic Neuroarthropathy Involving the
Midfoot. J Foot & Ank Surg. 39: 291-300, 2000.
Pinzur,MS: Benchmark Analysis of Diabetic Patients with Neuropathic (Charcot) Foot Deformity. Foot
Ankle Int_._ 20: 564-567, 1999.
Early, J.S., and Hansen, S.T.: Surgical Reconstruction of the Diabetic Foot. Foot & Ankle Int_._,
17:325-330, 1996.
Farber,DC, Juliano, PJ, Cavanagh, PR, Ulbrecht, J, Caputo, G: Single Stage Correction with External
Fixation of the Ulcerated Foot in Individuals with Charcot Neuroarthropathy. Foot Ank Int. 23:
130-134, 2002.
Koller, A, Wetz, HH: Link-Witzel Operation for Diabetics. Orthopade. 32: 231-235, 2003.
Myerson, MS, Henderson, MR, Saxby, T, Short, KW: Management of Midfoot Diabetic
Neuroarthropathy. Foot Ank Int. 15: 233-241, 1994.
Papa, J, Myerson, M, Girard, P: Salvage, with Arthrodesis, in Intractable Diabetic Neuropathic
Arthropathy of the Foot and Ankle. J Bone Joint Surg. 75A:1056-1066, 1993.
Sammarco, GJ, Conti, SF: Surgical Treatment of Neuropathic Foot Deformity. Foot Ank Int. 19:
102-109, 1998.
Simon, SR, Tejwani, SG, Wilson, DL, Santner, TJ, Denniston, NL: Arthrodesis as an Early Alternative
to Nonoperative Management of Charcot Arthropathy of the Diabetic Foot. J. Bone Joint Surg_._,
82A: 939-950, 2000.
Zarutsky, E, Rush, SM, Schuberth, JM: The Use of Circular Wire External Fixation in the Treatment of
Salvage Ankle Arthrodesis. J Foot & Ank Surg. 44: 22-31, 2005.
Bevan, WP, Tomlinson, MP: Radiographic Measure as a Predictor of Ulcer Formation in Diabetic
Charcot Midfoot. Foot Ank Int. 29:568-573, 2008.
Pinzur,MS: Surgical vs. Accommodative Treatment for Charcot Arthropathy of the Midfoot. Foot Ank
Int. 25: 545-549, 2004.
Mehta, JA, Brown, C, Sargeant, N: Charcot Restraint Orthotic Walker. Foot Ank Int. 19: 619-623,
1998.
Morgan, JM, Biehl III, WC, and Wagner, FWW Jr.: Management of Neuropathic Arthropathy with the
Charcot Restraint Orthotic Walker. Clin. Orthop_._ 296:58-63, 1993.
Trepman, E, Donnelly, P: Patellar Tendon-Bearin, Patten-Bottom Caliper Suspension Orthosis in
Active Charcot Arthropathy: Crutch-Free Ambulation with no Weight Bearing in the Foot. Foot Ank Int.
23: 335-339, 2002.
Sammarco, VJ, Sammarco, GJ, Walker, EW, Guiao, RP: Midtarsal Arthrodesis in Treatment of
Charcot Midfoot Arthropathy. J Bone Joint Surg. 91A: 80-91, 2009.
Koller, A, Fiedler, R, Wetz, HH: External Fixator for Reconstruction of Foot Statics in Neurogenic
Osteoarthropathies. Orthopade. 30: 218-225, 2001.
Wukich, DK, Lowery, NJ, McMillen, RL, Frykberg, RG: Postoperative Infection Rates in Foot and
Ankle Surgery: A Comparison of Patients with and without Diabetes Mellitus. J Bone Joint Surg. 92A:
287-295, 2010.
Wukich, D, Belczyk, RJ, Burns, PR, Frykberg, RG: Complications Encountered with Circular Ring
Fixation in Persons with Diabetes Mellitus. Foot Ank Int. 29: 994-1000, 2008.
Eckardt, A, Schollner, C, Decking, J, Ritter, S, Schadmand-Fischer, S, Kraus, O, Kustner, E: The
Impact of Syme Amputation in Surgical Treatment of Patients with Diabetic Foot Syndrome and
Charcot-Neuro-Osteoarthropathy. Arch Orthop Trauma Surg. 124: 145-150, 2004.
OrthopaedicsOne Articles
Page of 115 372
70.
71.
72.
73.
74.
75.
76.
77.
78.
79.
80.
81.
82.
83.
Pinzur,MS, Stuck, R, Sage, R, Hunt, N, Rabinovich, Z: Syme’s Ankle Disarticulation in Patients with
Diabetes. J Bone Joint Surg. 85A:1667-1672, 2003.
Connolly, JF, Csencsitz, TA: Limb Threatening Neuropathic Complications from Ankle Fractures in
Patients with Diabetes. Clin. Orthop_._, 348: 212-219, 1998.
Perry, MD, Taranow, WS, Manoli, A, Carr, JB: Salvage of Failed Neuropathic Ankle Fractures: Use of
Large Fragment Fibular Plating and Multiple Syndesmodic Screws. J Surg Orthop Adv. 14: 85-91,
2005.
Jani, MM, Ricci, WM, Borrelli Jr, J, Barrett, SE, Johnson, JE: A Protocol for Treatment of Unstable
Ankle Fractures Using Transarticular Fixation in Patients with Diabetes Mellitus and Loss of Protective
Sensation. Foot Ank Int. 24: 838-844, 2003.
Mueckley, TM, Eichorn, S, von Oldenburg, G, Speitling, A, DiCicco, JD, Hofmann, GO, Buhren, V:
Biomechanical Evaluation of Primary Stiffness of Tibiotalar Arthrodesis with an Intramedullary
Compression Nail and Four Other Fixation Devices. Foot Ank Int. 27: 814-820, 2006.
Noonan, T, Pinzur,MS, Paxinos, O, Havey, RM, Patwardhan, AG: Tibiotalocalcaneal Arthrodesis with
a Retrograde Intramedullary Nail: A Biomechanical Analysis of the Effect of Nail Length. Foot Ank Int,
26: 304-308, 2005.
Alvarez, RG, Barbour, TM, Perkins, TD: Tibiocalcaneal Arthrodesis for NonBraceable Neuropathic
Ankle Deformity. Foot Ank Int. 15: 354-359, 1994.
Kile, TA, Donnelly, RE, Gehrke, JC, Werner,ME, and Johnson, KA: Tibiotalocalcaneal arthrodesis
with an Intramedullary Device. Foot Ankle Int_._, 15: 669-673, 1994.
Moore, TJ, Prince, R, Pochatko, D, and Smith JW: Retrograde Intramedullary Nailing for Ankle
Arthrodesis. Foot Ankle Int_._, 16:433-436, 1995.
Pinzur, M.S., Kelikian, A.: Charcot Ankle Fusion with a Retrograde Locked Intramedullary Nail. Foot &
Ankle Int_._ 18:699-704, 1997.
Pinzur,MS, Noonan, T: Ankle Arthrodesis with a Retrograde Femoral Nail for Charcot Ankle
Arthropathy. Foot Ank Int, 26: 545-549, 2005.
Lidor C., Ferris LR., Hall R., Alexander IJ, Nunley JA II. Stress Fracture of the Tibia After Arthrodesis
of the Ankle or the Hindfoot. J Bone Joint Surg, 79:558-564, 1997.
Thordarson, DB, and Chang, D: Stress Fractures and Tibial Cortical Hypertrophy After
Tibiotalocalcaneal Arthrodesis with an Intramedullary Nail. Foot Ankle Int_._, 20: 497-500, 1999.
The Semmes-Weinstein 5.07 monofilament. The 5.07 monofilament applies ten grams of pressure
when deformed. This appears to be the clinical threshold of peripheral neuropathy that places diabetic
patients for diabetes-associated foot-specific morbidity.at risk