Autoimmune Encephalopathies and Dementias Continuum 2016

of 21
-
Upload
habib-g-moutran-barroso -
Category
Documents
-
view
220 -
download
2
Transcript of Autoimmune Encephalopathies and Dementias Continuum 2016
-
8/17/2019 Autoimmune Encephalopathies and Dementias Continuum 2016
1/21
AutoimmuneEncephalopathies andDementias
Andrew McKeon, MD
ABSTRACTPurpose of Review: This article describes the methods of diagnosis and manage-ment of autoimmune encephalopathies and dementias. The expedited distinction ofautoimmune encephalopathies and dementias from neurodegenerative disorders isimportant because treatment is most effective at the early stage of illness.
Recent Findings: The spectrum of antibody biomarkers of treatable autoimmuneencephalopathies continues to broaden and now includes antibodies targeting glu-tamate receptors ( N -methyl- D-aspartate [NMDA] and ! -amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid [AMPA]), + -aminobutyric acid A and B (GABA-A and GABA-B)receptors, glycine receptors, potassium channel complexes (Kv1, which includesleucine-rich, glioma inactivated 1 [LgI1], contactin-associated proteinlike 2 [CASPR2],and unknown specificity, and Kv4.2, which includes dipeptidyl-peptidase 6 [DPPX]),and glutamic acid decarboxylase 65 (GAD65). Early treatment of certain autoimmuneencephalopathies with rituximab or cyclophosphamide improves outcome when cor-ticosteroids, IV immunoglobulin (IVIg), and plasma exchange have proven ineffective.Summary: Despite the progress made in diagnostics, in many instances, patients withimmunotherapy-responsive encephalopathies and dementias are seronegative forencephalitis-specific antibodies. Other clues to an autoimmune cause include a
subacute symptom onset, rapid progression, personal history of autoimmunity orcancer,an inflammatory CSF,non-neural antibodies detected in serum, and a responseto immunotherapy.
Continuum (Minneap Minn) 2016;22(2):538 Y 558.
INTRODUCTION An autoimmune cause for cognitiveimpairment is frequently consideredby neurologists because of the potentialfor reversibility with immunotherapy.Classic limbic encephalitis is usually ac-
companied by an altered sensorium,rapid cognitive decline, altered moodand personality, and seizures. Becauseof the classic presentation and typicalmesial temporal T2 findings, limbicencephalitis is usually recognized by neurologists. Once infection has beenexcluded from consideration, a well-characterized and diagnostic neuralantibody may be detected in serum or
CSF (eg, leucine-rich, glioma inactivated1 [LgI1] antibody, a subtype of voltage-gated potassium channel [VGKC] com-plex antibodies) ( Case 8-1 ). In other instances, patients may present withrapid cognitive decline only, without de-lirium or seizures, and a rapidly progres-sive neurodegenerative dementia, suchas Jakob-Creutzfeldt disease, as well asan autoimmune cause, may enter thedifferential diagnosis. One or more of the following may serve as diagnosticclues for an autoimmune cause in thatcontext: a rapidly progressive or fluctu-ating course, a clinical history of
Address correspondence toDr Andrew McKeon,Neuro immunology Laboratory,Mayo Clinic, 200 1st St SW,Rochester, MN 55905,[email protected] .Relationship Disclosure:Dr McKeon receives researchfunding from MedImmune.Unlabeled Use of Products/Investigational Use Disclosure:Dr McKeon discusses theunlabeled/investigationaltreatments for autoimmuneencephalopathies anddementias, none of whichhave been approved by the US Food and Drug Administration for these indications.* 2016 American Academy of Neurology.
538 www.ContinuumJournal.com April 2016
Review Article
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/17/2019 Autoimmune Encephalopathies and Dementias Continuum 2016
2/21
coexisting autoimmunity, the presenceof inflammatory markers in the CSF,and detection of autoantibodies inserum or CSF. Sometimes, uncertainty
may persist at the end of testing and atrial of immunotherapy may provediagnostic, one way or the other. Autoimmune cognitive disorders are
Case 8-1A 57-year-oldman presented with left arm tingling that he experienced every10 minutes. Oral corticosteroids were prescribed by his primary physician forwhat was thought to be a cervical radiculopathy, and his symptoms resolved.One month later, he developed a subacute onset of episodic dysphasia andrapidly progressive memory difficulties. He underwent neurologic evaluation.Neuropsychometric testing demonstrated an amnestic profile. Brain MRIshowed mesial temporal T2 signal abnormality more prominent on the leftthan the right. His EEG demonstrated left temporal sharp waves and temporalintermittent rhythmic delta activity. Voltage-gated potassium channelcomplex (VGKC) antibodies were detected at a value of 1.00 nmol/L andwere determined to specifically target leucine-rich, glioma inactivated 1 (LgI1).Initial treatment consisted of levetiracetam 1000 mg 2 times a day, and IVmethylprednisolone 1000 mg/d for 5 days followed by weekly infusions.Although initial improvements occurred, the patient began to relapse withweekly treatments. His memory was worse, he had also developed a newmood disorder, and the abnormality in the right hippocampus on MRIappeared more prominent. Plasma exchange was started (five treatments,every other day, for 10 days) followed by prednisone 60 mg/d for 3 months,followed by tapering the daily dose each subsequent month by 10 mg, untilthe dose of 10 mg/d was reached, which was then tapered by 1 mg eachsubsequent month until the prednisone was discontinued.
He developed a cushingoid physical appearance, which resolved ondiscontinuation of prednisone. Prophylaxis with calcium, vitamin D, andtrimethoprim/sulfamethoxazole was used until prednisone was discontinued.Despite this, he developed osteoporosis, and bisphosphonate therapy wasstarted. Because of his initial relapsing course, azathioprine was started with theintention of the patient receiving 2.5 mg/kg/d for 5 years of treatment.
However, his thiopurine methyltransferase value was mildly low (16.6 units/mL,where greater than 17.0 units/mL is normal), indicating that he might notmetabolize azathioprine well and be prone to drug toxicity. The patient hadsteady improvements in cognitive function, regaining normal function overthe course of 1 year. His mood disorder did not improve with immunotherapy,nor with tapering and discontinuing levetiracetam. Citalopram was started,and his mood improved. The patient developed elevated liver transaminaseenzyme levels, which were attributed to azathioprine (thiopurinemetabolites were elevated in serum). Mycophenolate mofetil was used inthe place of azathioprine for remission maintenance for 3 years.
Comment. This case demonstrates a number of important points,including the possibility for complete remission with sustained, multimodalimmunotherapy; the complications that can arise with corticosteroid therapy;
the importance of prophylaxis for the bone demineralizing and opportunisticinfectious effects of steroids; the high probability of developing sideeffects from azathioprine if the thiopurine methyltransferase is low; andthe complementary role for symptom-based treatments (antiepilepticsand antidepressants).
539Continuum (Minneap Minn) 2016;22(2):538 Y 558 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/17/2019 Autoimmune Encephalopathies and Dementias Continuum 2016
3/21
phenotypically and immunologically diverse. Ordinarily, the terms enceph-
alopathy or encephalitis imply thepresence of an altered sensorium or consciousness, while the term demen-tia does not. For brevity, this article will refer to these disorders as autoim-mune encephalopathies.
EPIDEMIOLOGYPrecise frequency data for autoimmuneencephalopathies, dementias, and epi-lepsies are not available. These disor-ders are clearly underrecognized. A
review of over 1000 brain autopsy casesreferred to the US National Prion Dis-ease Pathology Surveillance Center as Jakob-Creutzfeldt disease demonstratedan undiagnosed, treatable cause for dementia in 7% of cases, most preva-lent of which were autoimmune disor-ders. 1 Among Mayo Clinic patientsdiagnosed with and treated for an au-toimmune encephalopathy or demen-tia, 35% had been diagnosed with aneurodegenerative disorder. 2
DIAGNOSTIC CLUESThe following diagnostic clues are worth considering when an autoim-mune etiology is suspected for a patientpresenting with a new-onset cognitivedisorder ( Table 8-1 3 ).
Clinical ManifestationsThe clinical manifestations of neuro-logic autoimmunity are diverse andoften multifocal. While certain disor-ders have been syndromically associ-ated with certain autoantibody markers(eg, limbic encephalitis and LgI1 auto-antibodies), 4 a spectrum often emergesover time through individual case re-ports or by systematic serologic evalu-ation of large numbers of patients notselected by neurologic syndrome. 5 For example, VGKC complex antibodies were initially considered to be specificfor autoimmune limbic encephalitisor disorders of peripheral nervoushyperexcitability, but, over time, other presentations have been reported, in-cluding a rapidly progressive coursemimicking Jakob-Creutzfeldt disease. 6
KEY POINTSh The clinical
manifestations ofneurologic autoimmunityare diverse (includingencephalopathy) and areoften multifocal.
h In the absence ofdetection of anencephalitis-specificantibody(eg, leucine-rich,glioma inactivated 1 orN -methyl- D-aspartatereceptor antibody), ahistory of autoimmunedisease or seropositivityfor other autoantibodies(organ-specific ornon Y organ-specificautoantibodies) are riskfactors for anautoimmuneencephalopathy.
TABLE 8-1 Key Features of Autoimmune Encephalopathy or Dementiaa
b Subacute onset
b Fluctuating course
b Tremor
b Headache
b Personal or family history (first-degree relative) of autoimmunity
b History of recent or past neoplasia
b Evidence of central nervous system inflammation on CSF (elevated protein,
pleocytosis, oligoclonal bands, elevated CSF index)b Evidence of central nervous system inflammation on MRI (mesial temporal
or other regional T2 hyperintensity)
b Hypometabolism on functional imaging
b Detection of neural autoantibody
CSF = cerebrospinal fluid; MRI = magnetic resonance imaging.a Data from McKeon A, et al, Continuum (Minneap, Minn). 3 journals.lww.com/continuum/
Fulltext/2010/04000/IMMUNOTHERAPY_RESPONSIVE_DEMENTIAS_AND.8.aspx .
540 www.ContinuumJournal.com April 2016
Autoimmune Encephalopathies
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
http://journals.lww.com/continuum/Fulltext/2010/04000/IMMUNOTHERAPY_RESPONSIVE_DEMENTIAS_AND.8.aspxhttp://journals.lww.com/continuum/Fulltext/2010/04000/IMMUNOTHERAPY_RESPONSIVE_DEMENTIAS_AND.8.aspxhttp://journals.lww.com/continuum/Fulltext/2010/04000/IMMUNOTHERAPY_RESPONSIVE_DEMENTIAS_AND.8.aspx
-
8/17/2019 Autoimmune Encephalopathies and Dementias Continuum 2016
4/21
Morvan syndrome is a rare multifocalmanifestation of VGKC complex auto-
immunity that includes features of limbic encephalitis, sleep disturbance,and peripheral nerve hyperexcitability. 4
Risk FactorsIn the absence of detection of anencephalitis-specific antibody (eg,LgI1 or N -methyl- D-aspartate [NMDA]receptor antibody), a history of auto-immune disease or seropositivity for othe r autoantibodies (organ-specificor non Y organ-specific autoantibodies)are risk factors for an autoimmuneencephalopathy.
Multiple autoimmune disorders may occur in the same patient, and individ-uals with an autoimmune disease areat higher risk of developing a secondautoimmune disorder. For example,just as systemic lupus erythematous may develop in a patient with type 1 diabetesmellitus, autoimmune thyroiditis (a very common form of autoimmunity)and an autoimmune encephalopathy (a relatively uncommon form of auto-
immunity) also may occur in the samepatient. Thus, the presence of autoim-mune thyroiditis reflects a risk for de- veloping other autoimmune diseases,including an autoimmune encephalop-athy. However, the detection of thy-roid, systemic lupus erythematous, or Sjögren syndrome antibodies in a pa-tient with an autoimmune encepha-lopathy does not imply neurologicpathogenicity of the antibodies de-tected. Also, some connective tissuedisease antibodies are commonly de-
tected in the general healthy popula-tion and should be interpreted withcaution in the context of a cogni-tive disorder.
Identifying Neural-SpecificAutoantibodiesDetection of a neural-specific autoan-tibody serves as a marker of neurologicautoimmunity. Antibodies directed at
cell-surface antigens (eg, LgI1) may bepathogenic, while antibodies directed
at an intracellular antigen (eg, antineu-ronal nuclear antibody type 1 [ANNA-1],also known as anti-Hu) are more likely markers of a T-cell Y mediated disease. 7
Identifying a ParaneoplasticDisorder A profile of neural-specific autoanti-bodies may aid in the identification of a paraneoplastic disorder. 7
Antibodies with neural specificity have varying degrees of paraneoplasticsignificance ( Table 8-2 and Table 8-3 ).
Improvement AfterImmunotherapyNeurologic improvement after immu-notherapy may be diagnostically infor-mative. In many instances, the diagnosisof autoimmune encephalopathy is basedon clinical improvements obtained withimmunotherapy. Therefore, baselineobjective clinical, electrophysiologic,radiologic, and neuropsychologicaltesting provides reference points for
evaluating clinical improvement withimmunotherapies.
Personal or Family History ofAutoimmunityPatients with an autoimmune neuro-logic disorder may have a backgroundof having a relatively common sys-temic autoimmune disease or may haveseveral first-degree relatives affected( Case 8-2 ).
These autoimmune disorders may be organ specific (including thyroid dis-ease, diabetes mellitus, pernicious ane-mia, Sjögren syndrome, rheumatoidarthritis, alopecia, vitiligo, and Addisondisease) or non Y organ specific (sys-temic lupus erythematous, systemicsclerosis, and mixed connective tissuedisease). A personal history of cancer or smoking may also serve as cluesto a paraneoplastic cause. A review of systems for symptoms consistent with
KEY POINTSh Detection of a neural-
specific autoantibodyserves as a marker ofneurologic autoimmunity.
h A profile of neural-specific autoantibodiesmay aid the identificationof a paraneoplasticencephalopathic disorder.
h Neurologic improvementafter immunotherapymay be diagnosticallyinformative ofautoimmuneencephalopathy.
h In many instances, thediagnosis of autoimmuneencephalopathy is basedon clinical improvementsobtained withimmunotherapy.Therefore, baselineobjective clinical,electrophysiologic,radiologic, andneuropsychologicaltesting providesreference points forevaluating clinicalimprovement withimmunotherapies.
h Patients with anautoimmune neurologicdisorder may have abackground of havinga relatively commonsystemic autoimmunedisease or may haveseveral first-degreerelatives affected bycommon systemicautoimmune diseases.
541Continuum (Minneap Minn) 2016;22(2):538 Y 558 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/17/2019 Autoimmune Encephalopathies and Dementias Continuum 2016
5/21
an underlying malignancy, including weight loss, night sweats, and alteredbowel habit, should be undertaken.
CLINICAL AND SEROLOGICSPECTRUMSymptoms of autoimmune encephalop-athy and dementia are almost always of
subacute onset (ie, evolving over daysto weeks).
Limbic EncephalitisLimbic encephalitis classically presents with altered mood, memory, and per-sonality as well as delirium and focal sei-zures of mesial temporal origin, with or
KEY POINTh Autoimmune
encephalopathicsymptoms are almostalways of subacuteonset (ie, evolving overdays to weeks).
TABLE 8-2 Neuronal Nuclear, Cytoplasmic, and Nucleolar Antibodies
Antibody Cognitive Disorders Other Neurologic Manifestations Cancer AssociationANNA-1 (Hu) Limbic or
extralimbicencephalitis
Peripheral neuropathy (mostcommonly sensory), cerebellarsyndrome, cranial neuropathy
Small cell carcinoma; a
thymoma; neuroblastoma(children)
ANNA-2 (Ri) Dementia, limbicencephalitis,encephalopathy
Brainstem encephalitis, cerebellardisorder, myelopathy, peripheralneuropathy
Breast adenocarcinoma,small cell carcinoma a
ANNA-3 Limbic encephalitis Peripheral neuropathy (sensory/ sensorimotor), cerebellar ataxia,brainstem encephalitis,myelopathy
Small cell carcinoma, a
adenocarcinoma (lungor esophagus)
PCA-2 Limbic encephalitis Brainstem encephalitis, cerebellar
disorder, Lambert-Eatonmyasthenic syndrome, peripheraland autonomic neuropathies
Small cell carcinoma a
AmphiphysinIgG
Cognitive dysfunction,encephalopathy,limbic encephalitis
Neuropathy, myelopathy, stiffperson syndrome, Lambert-Eatonmyasthenic syndrome
Small cell carcinoma, a
breast adenocarcinoma
CRMP-5 IgG Subacute dementia,personality change
Seizures, chorea, ataxia, psychiatricsymptoms, cranial neuropathy(optic neuropathy, abnormalolfaction/taste), myelopathy,radiculopathy, neuropathy,Lambert-Eaton myasthenic syndrome
Small cell carcinoma, a
thymoma
Ma1, Ma2
antibodies
Memory impairment,
dementia, limbicencephalitis
Brainstem encephalitis, cerebellar
syndrome, hypothalamic disorder,psychiatric symptoms
Testicular germ cell
tumors (Ma2); lung cancer,gastrointestinal cancer,non-Hodgkin lymphoma,breast cancer (Ma1, Ma2)
GAD65 IgG Limbic encephalitis Seizures, cerebellar ataxia,brainstem encephalitis, stiff personsyndrome, extrapyramidalsigns, myelopathy
Thymoma, renal cell,adenocarcinoma (breast orcolon) are rarely reported
AGNA (SOX1) Limbic encephalitis Lambert-Eaton myasthenicsyndrome, cerebellar dysfunction
Small cell carcinoma a
AGNA = antiglial/neuronal nuclear antibody; ANNA-1 = antineuronal nuclear antibody type 1; ANNA-2 = antineuronal nuclear antibodytype 2; ANNA-3 = antineuronal nuclear antibody type 3; CRMP-5 = collapsin response mediator protein-5; GAD65 = glutamic aciddecarboxylase 65; IgG = immunoglobulin G; PCA-2 = Purkinje cell cytoplasmic antibody type 2; SOX1 = sex-determining region Y box 1.a Small cell carcinoma can be pulmonary or extrapulmonary.
542 www.ContinuumJournal.com April 2016
Autoimmune Encephalopathies
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/17/2019 Autoimmune Encephalopathies and Dementias Continuum 2016
6/21
without secondary generalization. BrainMRI usually reveals T2 signal abnor-mality in one or both hippocampalregions. EEG may reveal unilateral or
bilateral temporal slowing or epilepti-form discharges. The main differentialdiagnosis is herpes encephalitis. Auto-immune encephalitis may also have an
TABLE 8-3 Antibodies Targeting Neural Ion Channels and Receptors
Antibody Cognitive DisordersOther NeurologicManifestations Cancer Association
VGKC complexantibody (antigenictargets may be LgI1or CASPR2)
Limbic encephalitis, amnesia,executive dysfunction,dementia (includingfrontotemporaldementia Y like syndromeand Jakob-Creutzfeldt Y like disease)
Seizures, psychiatric symptoms,insomnia, extrapyramidaldisorder, myoclonus,hypothalamic disorder,autonomic disorders, peripheralhyperexcitability
Small cell lung cancer,thymoma, prostateadenocarcinoma,breast adenocarcinoma
NMDA receptorantibody
Memory impairment,depression, psychosis,agitation, behavioralchange
Characteristic multistagesyndrome of prodrome,psychiatric symptoms, seizures,abnormal movements (including
orofacial dyskinesia), followedby decreased responsiveness,hypoventilation, and autonomicinstability
Ovarian teratoma
GABA-A and GABA-Breceptor antibodies
Limbic encephalitis,sometimes seizurepredominant, otherencephalitides
Seizures (limbic encephalitis),visual hallucinations, aphasia,orolingual movements,cerebellar ataxia
Small cell lungcarcinoma,neuroendocrineneoplasia
AMPA receptorantibody
Memory loss, disorientation,psychiatric symptoms,behavioral change, agitation(limbic encephalitis)
Seizures (limbic encephalitis),nystagmus, hypersomnia,progressive unresponsiveness,dysdiadochokinesia, hallucinations
Breast cancer, lungcancer, thymus cancer
DPPX antibody Cognitive impairment Seizures, myoclonus, sleep
disorders, eye movementdisorders, ataxia,gastrointestinal dysmotility
B-cell neoplasms
Ganglionicacetylcholine receptorantibody
Cognitive impairment,executive dysfunction,frontotemporal syndrome,encephalopathy
Dysautonomia, peripheralneuropathy
Adenocarcinoma,renal cell carcinoma,lymphoid cancers
mGluR5 antibody Limbic encephalitis None Hodgkin lymphoma
Glycine receptor Progressive encephalomyelitiswith rigidity and myoclonus(PERM)
Stiff person syndrome B-cell neoplasms,thymoma
IgLON5 Cognitive decline Chorea, ataxia, dysarthria,dysphagia, sleep apnea,dream enactment
None reported
AMPA = ! -amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid; CASPR2 = contactin-associated proteinlike 2; DPPX = dipeptidyl-peptidase6; GABA-A = + -aminobutyric acid A; GABA-B = + -aminobutyric acid B; IgLON5 = IgLON family member 5; LgI1 = leucine-rich, gliomainactivated 1; mGlurR5 = metabotropic glutamate receptor 5; NMDA = N -methyl- D-aspartate; VGKC = voltage-gated potassium channel.
543Continuum (Minneap Minn) 2016;22(2):538 Y 558 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/17/2019 Autoimmune Encephalopathies and Dementias Continuum 2016
7/21
extratemporal localization, affectingone or more of frontal, parietal, andoccipital regions. 8
Neural autoantibody and cancer as-
sociations are protean, and thus acomprehensive serologic and CSF anti-body evaluation is required ( Table 8-2and Table 8-3 ).8 Information regardingcancer type and likely treatment re-sponsiveness can be obtained from aserologic or CSF diagnosis. For exam-ple, a patient with ANNA-1 detected would likely have small cell carcinoma(90% of patients) usually of lung, 9 butimprovements with immunotherapy would be unlikely to occur.
In contrast, a patient with VGKC com-plex antibody would be unlikely to havecancer detected (less than 20% of pa-tients), but would likely have very largeimprovements in cognitive function (or even full recovery) if treated early (andcomprehensively) with immunotherapy. 5
Autoimmune Dementia Autoimmune dementia phenotypesmay resemble Jakob-Creutzfeldt dis-
ease, which, classically, is a rapidly progressive neurodegenerative disor-der accompanied by ataxia and myoc-lonus. 6 Rapidly progressive forms of
Alzheimer disease and dementia withLewy bodies also are difficult to dis-tinguish clinically from an auto-immune dementia. Tremulousness andheadache at presentation, marked fluc-tuations in the clinical course, andspontaneous remission suggest an au-toimmune cause. 2
N -Methyl- D-aspartate ReceptorEncephalitisIn some instances, autoimmune neu-rologic disorders can be named withreference to an autoantibody with highspecificity for encephalitis, detected inserum, CSF, or both. Examples includeanti-NMDA receptor encephalitis andLgI1 encephalitis. 10,11 Patients withNMDA receptor antibody (targeting theGluN1 [NR1] subunit) have a stereo-typed neurologic disorder that oftenevolves in stages, as described by Dalmau
KEY POINTSh Limbic encephalitis
classically presents withaltered mood, memory,and personality as wellas delirium and focalseizures of mesialtemporal origin, with orwithout secondarygeneralization.
h Autoimmunedementia phenotypesmay resembleJakob-Creutzfeldtdisease, which, classically,is a rapidly progressiveneurodegenerativedisorder accompanied byataxia and myoclonus.
h Central nervous systeminfection and otherinflammatory centralnervous system disordersare major differentialdiagnostic considerationswhen evaluating patientswith rapidly progressivecognitive decline and aninflammatory spinal fluid.
Case 8-2A 65-year-old man presented with an abrupt onset and fluctuating courseof memory loss that began 3 months prior to neurologic evaluation. Hissymptoms were characterized by inability to recall recent events andconversations. The patient’s personal history was remarkable for perniciousanemia. The patient’s sister had Hashimoto thyroid disease. The KokmenShort Test of Mental Status revealed a score of 36 out of 38 (losing 2 of 4 forrecall). His MRI brain scan demonstrated nonspecific white matter change,and his EEG showed moderate generalized slowing. Neuropsychologicalevaluation revealed learning and memory impairments consistent with theamnestic variant of mild cognitive impairment. Serum and CSF testing forneural and non-neural autoantibodies was negative. Because of the abruptonset of symptoms, and the presence of both personal and family histories ofautoimmunity, a course of IV methylprednisolone was undertaken (1000 mg/dfor 3 consecutive days, followed by 1000 mg/wk for 5 weeks). The patientreported dramatic improvement of cognition, and learning and memorywere significantly improved on neuropsychometric reevaluation.
Comment. This case demonstrates an autoimmune cognitive disorder limitedto mild cognitive impairment. Personal and family histories of autoimmunitywere key diagnostic clues, despite the absence of neural autoantibodies in theserum and CSF. Neuropsychological evaluations performed before and afterimmunotherapy allowed objective assessment of the response to treatment.
544 www.ContinuumJournal.com April 2016
Autoimmune Encephalopathies
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/17/2019 Autoimmune Encephalopathies and Dementias Continuum 2016
8/21
and colleagues. 11 Initial symptoms may include headache, fever, nausea, andprominent psychiatric symptoms. Themajority of patients initially come tothe attention of psychiatrists. Depres-sion, anxiety, insomnia, fear, delusions,mania, and paranoia frequently occur.Other behavioral changes include so-cial withdrawal and stereotyped behav-ior. Amnesia and an unusual languagedisorder ensue. In children, behav-ioral change is a common presentingsymptom (such as temper tantrums andhyperactivity), which is followed by neurologic disorders including seizuresand dyskinesia, which may also be thepresenting symptoms in children. After these initial symptoms, decreased re-sponsiveness ensues in both adults andchildren. Movement disorders are di- verse and include oro-lingual-facial dys-kinesia, generalized limb and truncaldyskinesia, oculogyric crisis, dystonia,and rigidity. Central autonomic mani-festations, including hyperthermia,tachycardia, and hypertension, may besevere and necessitate intensive careunit management. Hypoventilation may occur, necessitating prolonged ventila-tory support (often months).
Brainstem EncephalitisPresenting symptoms of brainstemencephalitis include eye movementdisorders, other cranial neuropathies,nausea, vertigo, postural instability,and parkinsonism. 12 These are com-mon presentations for patients with
Ma2 antibodies (anti-Ta, which usually occurs in young men with testicular carcinoma) or both Ma1 and Ma2 anti-bodies (anti-Ma, which occurs in bothmen and women with a variety of cancer types). 12 Jaw dystonia is an un-usual manifestation of brainstem en-cephalitis reported in antineuronalnuclear antibody type 2 (ANNA-2) sero-positive patients. 13
Other AutoimmuneEncephalopathiesSometimes encephalopathy is but onemanifestation of an immunologically well-characterized disorder, examplesof which include dipeptidyl-peptidase6 (DPPX) encephalitis, a multifocal cen-tral nervous system (CNS) and auto-nomic disorder in which patients may experience seizures, sleep disorders,myelopathy, and gastrointestinal dis-orders (Case 8-3) .14,15 Patients withDPPXor glycine receptor autoimmunity may have a multifocal phenotype known
as progressive encephalomyelitis withrigidity and myoclonus (PERM). 16
In other instances, the more genericterm of autoimmune encephalopathy without reference to a specific neuralantibody is appropriate. This is becausethe neural antibody detected has lessspecificity for encephalitis (eg, ! -3ganglionic acetylcholine receptor), or no neural antibody has been detecteddespite comprehensive evaluation, butother clues for an autoimmune diag-nosis have emerged. These clues couldinclude one or more of a history of co-existing autoimmune diseases (eg,thyroid disease), the detection of non-neural autoantibodies (such as thyroidautoantibodies) in serum, or an inflam-matory spinal fluid, an encephalitic-appearing head MRI, and a responseto immunotherapy. 2
Both Hashimoto encephalopathy and steroid-responsive encephalopathy associated with autoimmune thyroiditis(SREAT) refer to a triad of encepha-
lopathy, thyroid autoimmunity, andclinical improvements with immuno-therapy. 17 Because both thyroid auto-antibodies and cognitive symptoms arecommon in the general population, thisexample serves to underline the im-portance of objectifying cognitive im-provements with immunotherapy.Corticosteroids have nonspecific acti- vating effects (eg, improved mood,
KEY POINTSh N -Methyl-D-aspartate
receptor encephalitisoften has a stereotypedcourse evolving from apsychiatric-predominantphenotype toencephalopathy, seizures,and hyperkineticmovement disorders.
h Presenting symptoms ofbrainstem encephalitisinclude eye movementdisorders, other cranialneuropathies, nausea,vertigo, posturalinstability, andparkinsonism.
545Continuum (Minneap Minn) 2016;22(2):538 Y 558 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/17/2019 Autoimmune Encephalopathies and Dementias Continuum 2016
9/21
wakefulness, and energy) as well asan immunosuppressive capacity. Inthe author’s experience, true SREATis a rare entity, while patients withnonspecifically elevated thyroid anti-
bodies and subjective cognitive symp-toms occurring in the context of untreated sleep disorders, depression,and narcotic pain medication use arecommonly encountered.
In some disorders, characteristicnoncognitive symptoms may assist inmaking an autoimmune diagnosis. For instance, in patients with rapid cogni-tive decline (often accompanied by
headache and psychiatric disturbance)and one or more of branch retinal artery occlusions and sudden hearing loss,Susac syndrome shouldbe considered. 18
DIFFERENTIAL DIAGNOSISOther causes of cognitive declineshould be considered and excluded asnecessary. In particular, one needs toexclude other potentially treatablecauses of dementia ( Table 8-4 ). Other inflammatory disorders that can causea dementia phenotype, but are of unknown cause, include CNS vasculitis,sarcoidosis, and multiple sclerosis.
KEY POINTSh Caution is advised
regarding making adiagnosis of Hashimotoencephalopathy(also known assteroid-responsiveencephalopathyassociated withautoimmune thyroiditis)in patients withcognitive symptoms(without objectiveabnormalities) andthyroid autoimmunity,which is common in
the general population.h Other inflammatory
disorders that can causea dementia phenotype,but are of unknowncause, include centralnervous system vasculitis,sarcoidosis, andmultiple sclerosis.
Case 8-3A 27-year-old man presented with cognitive impairment, incoordination,and vision disturbance that began 1 year prior to neurologic evaluation.His neurologic symptoms were preceded by a 3-year history of weight lossand irritability. Examination revealed an amnestic syndrome, multifocalmyoclonus, diffuse hyperreflexia, ataxia, and nystagmus. Gastrointestinalmotility studies documented gastroparesis and bowel hypomotility, andautonomic reflex testing demonstrated cardiovagal and vasomotordysfunction. A sleep study demonstrated obstructive sleep apnea andambiguous sleep (where rapid eye movement [REM] sleep and non-REMsleep are difficult to distinguish during polysomnography). Video EEGdemonstrated continuous tremulousness without epileptiform correlate,which was confirmed by surface EMG to be myoclonus. Dipeptidyl-peptidase6 (DPPX) antibody was detected in the serum and CSF. His symptomsimproved after treatment with IV methylprednisolone. Oral prednisone anda steroid-sparing immunosuppressant (mycophenolate mofetil) were added.His weight, cognition, and balance improved but did not normalize. Fivemonths after the initial neurologic presentation and after discontinuingcorticosteroid therapy, visual hallucinations developed and wereaccompaniedby profound diaphoresis and hypothermia. Cardiac arrest ensued; aftersuccessful resuscitation, fluctuating blood pressure and body temperaturenecessitated extended intensive care. Diaphoresis, blood pressure, andtemperature normalized following IV methylprednisolone treatment.Dysautonomicsigns improved greatly following plasma exchange, rituximab,and slowly tapered prednisone therapy. The patient had remitted from hisencephalitic illness 2 years after initial presentation, with rituximab dosesadministered every 6 months used as maintenance therapy. However, he hadmild residual ataxia and cognitive impairment, but was still much troubled
by his sleep disorder.Comment . This case is illustrative of multifocality (central nervoussystem and autonomic disorders) occurring in a patient with autoimmuneencephalopathy, the need for aggressive, sustained immunotherapy insome patients, and the possibility of residual neurologic problems despitemaximal treatment.
546 www.ContinuumJournal.com April 2016
Autoimmune Encephalopathies
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/17/2019 Autoimmune Encephalopathies and Dementias Continuum 2016
10/21
CLINICAL EXAMINATION ANDCOGNITIVE TESTINGBedside tests include the Mini-MentalState Examination (MMSE), the KokmenShort Test of Mental Status, and theMontreal Cognitive Assessment (MoCA). Autoimmune neurologic disorders areoften multifocal; thus, it is important tonote neurologic symptoms and signsaccompanying cognitive impairmentor seizures. These signs may includeataxia, brainstem abnormalities, parkin-sonism, myoclonus, tremor,myelopathy,or a peripheral nervous system disor-der. These evaluations enable documen-tation of the specific cognitive deficitsand serve as a baseline to which the
posttreatment cognitive profile may be compared. Where possible, a moredetailed neuropsychological profileshould be obtained to document mildabnormalities not detectable by bed-side testing and to exclude potentialconfounders (such as mood disordersand the side effects of psychoactivemedications).
IMAGINGImaging of the brain can provide bothstructural and functional clues to anautoimmune cause for encephalopathy.
Magnetic Resonance ImagingMesial temporal hyperintensities, ei-ther unilateral or bilateral with or
KEY POINTSh Where possible, a
more detailedneuropsychologicalprofile should beobtained to documentmild abnormalities notdetectable by bedsidetesting and to excludepotential confounders(such as mooddisorders and the sideeffects of psychoactivemedications).
h Imaging of the braincan provide bothstructural and functionalclues to an autoimmunecausefor encephalopathy.
TABLE 8-4 Differential Diagnostic Considerations for Patients With Cognitive Impairmenta
Potentially Treatable Causesof Cognitive Impairment ExamplesAutoimmune encephalopathiesand dementias
Immunotherapy-responsive disorders of presumed autoimmuneetiology; some patients have an associated neural-specific antibody(see Table 8-2 and Table 8-3 )
Other inflammatory centralnervous system (CNS) disorders
Multiple sclerosis, acute disseminated encephalomyelitis,neurosarcoidosis
Vasculopathies CNS vasculitis, posterior reversible encephalopathy syndrome (PRES),subdural hematoma
Neoplastic Primary CNS lymphoma (including intravascular and meningeal presentations)
Seizure disorders Nonconvulsive status epilepticus
Iatrogenic Benzodiazepines, antidepressants, antipsychotics, antiepileptics,anticholinergics, analgesics
Toxic Alcohol, opiates, cocaine, amphetamines, organic solvents
Nutritional deficiency Vitamin B 12 , thiamine, folic acid
Psychiatric illness Anxiety, depression, psychosis
CNS infection Herpes simplex virus, human herpesvirus 6, human immunodeficiency virus,fungal (eg, cryptococcus), mycobacterial, Whipple disease, neurosyphilis
Metabolic Respiratory, renal, or liver failure; obstructive sleep apnea syndrome;mitochondrial disorders (eg, mitochondrial myopathy, encephalopathy,lactic acidosis, and strokelike episodes syndrome [MELAS])
Endocrine Disturbances in pituitary, thyroid, para thyroid, endocrine, pancreatic, or
adrenal functiona Reprinted with permission from McKeon A, et al, Continuum (Minneap Minn). 3 journals.lww.com/continuum/Fulltext/2010/04000/ IMMUNOTHERAPY_RESPONSIVE_DEMENTIAS_AND.8.aspx. B 2010 American Academy of Neurology.
547Continuum (Minneap Minn) 2016;22(2):538 Y 558 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
http://journals.lww.com/continuum/Fulltext/2010/04000/IMMUNOTHERAPY_RESPONSIVE_DEMENTIAS_AND.8.aspxhttp://journals.lww.com/continuum/Fulltext/2010/04000/IMMUNOTHERAPY_RESPONSIVE_DEMENTIAS_AND.8.aspxhttp://journals.lww.com/continuum/Fulltext/2010/04000/IMMUNOTHERAPY_RESPONSIVE_DEMENTIAS_AND.8.aspxhttp://journals.lww.com/continuum/Fulltext/2010/04000/IMMUNOTHERAPY_RESPONSIVE_DEMENTIAS_AND.8.aspx
-
8/17/2019 Autoimmune Encephalopathies and Dementias Continuum 2016
11/21
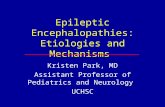
without enhancement after gadoliniumadministration, are classic autoim-
mune limbic encephalitis findings( Figure 8-1 ). Normal imaging is com-mon, particularly in the early illnessstages, and is the norm in patients with anti-NMDA receptor encephali-tis.11 Extratemporal abnormalities aresometimes observed. If lesions are notin a typical distribution or have avid en-hancement, other inflammatory (eg,neurosarcoidosis) or oncologic (eg,lymphoma) diagnoses should be con-sidered. Patients with Susac syndromeusually have multiple hemispheric
white matter lesions involving the cor-pus callosum, somewhat mimicking
multiple sclerosis, but with prominent,extensive leptomeningeal enhancement.Rapidly resolving large hemisphericT2 abnormalities should raise concernfor a mitochondrial disorder, such asmitochondrial myopathy, enceph-alopathy, lactic acidosis, and stroke-like episodes syndrome (MELAS).Nonenhancing posterior predominant whi te matter lesions should raiseconcern for progressive multifocalleukoencephalopathy. Cortical ribbonhyperintensities can be observed in
FIGURE 8-1 MRI findings in autoimmune encephalopathy, including unusual extratemporal disorders. MRI images includeT2 fluid-attenuated inversion recovery (FLAIR) coronal ( A, B, D, E ), axial (C ), and turbo spin echo axial ( F ). A, Classic limbic encephalitis (arrows ). B, image also shows limbic encephalitis, but bilateral T2 signal change
is more subtle ( arrows ). C , Normal MRI in patient with anti- N -methyl- D-aspartate (NMDA) receptor encephalitis. D, F , Imagesfrom two patients demonstrate unilateral frontal abnormalities ( arrows ). Panel D shows a patient with antineuronal nuclearantibody type 1 (ANNA-1) (anti-Hu antibody), which is more commonly associated with limbic encephalitis. Panel F shows apatient with a syndrome mimicking corticobasal degeneration, but occurred on a paraneoplastic basis in patient with breastcancer. E , Image shows bilateral frontoparietal T2 hyperintensities ( arrows ) in a patient with seronegative autoimmune encephalitis.
548 www.ContinuumJournal.com April 2016
Autoimmune Encephalopathies
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/17/2019 Autoimmune Encephalopathies and Dementias Continuum 2016
12/21
some patients (and thus may be mis-leading for Jakob-Creutzfeldt disease). 6
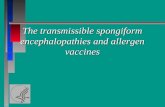
Functional ImagingGlobal hypometabolism is the mostcommon feature encountered in pa-tients with autoimmune encephalopa-thies. However, focal hypometabolismcan also be encountered ( Figure 8-2 ).2
In instances where the patient has sei-zures, hypermetabolism can occur. 19
ELECTROPHYSIOLOGYEEG is helpful for documenting func-
tional abnormalities in patients withautoimmune encephalitis. Moderateto severe generalized slowing is usual, with superimposed regional abnor-malities (eg, focal slowing or epilepti-
form discharges) also commonly occurring. Regional abnormalitiesmost commonly emanate from thetemporal lobes, although extratempo-ral abnormalities have also been re-ported. 20 Again, improvements in theseabnormalities can be reassuring regard-ing the efficacy of treatment.
ROUTINE CEREBROSPINAL FLUIDPARAMETERSFurther clues to an autoimmune eti-ology for a cognitive disorder may befound on CSF evaluation. Elevated
protein concentration (greater than100 mg/dL), elevated numbers of whiteblood cells, abnormal numbers of CSF-exclusive oligoclonal bands, and ele- vated IgG index and synthesis rate all
KEY POINTSh EEG is also helpful for
documenting functionalabnormalities in patientswith autoimmuneencephalitis.
h Objectifying thecognitive abnormalitiesthrough clinicalexamination, cognitivetesting, imaging,and EEG is criticalto the diagnosisof autoimmuneencephalopathy andprovides a baselinefor treatment.
FIGURE 8-2 Fluorodeoxyglucose positron emission tomography (FDG-PET) pretreatment ( A)and postimmunotherapy ( B), in a patient with autoimmune encephalopathy.Sagittal ( A, B, top) and coronal ( A, B, bottom ) views of brain metabolism are
demonstrated. Metabolism ranges from normal ( blue ) to increasingly abnormal ( through green , yellow , and red ). Images demons trate functional improvement after treatment ( arrows ).
Modified with permission from Flanagan EP, et al. Mayo Clin Proc.2
www.mayoclinicproceedings.org/article/ S0025-6196(11)60229-2/fulltext . B 2010 Mayo Foundation for Medical Education and Research.
549Continuum (Minneap Minn) 2016;22(2):538 Y 558 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
http://www.mayoclinicproceedings.org/article/S0025-6196(11)60229-2/fulltexthttp://www.mayoclinicproceedings.org/article/S0025-6196(11)60229-2/fulltexthttp://www.mayoclinicproceedings.org/article/S0025-6196(11)60229-2/fulltexthttp://www.mayoclinicproceedings.org/article/S0025-6196(11)60229-2/fulltexthttp://www.mayoclinicproceedings.org/article/S0025-6196(11)60229-2/fulltexthttp://www.mayoclinicproceedings.org/article/S0025-6196(11)60229-2/fulltext
-
8/17/2019 Autoimmune Encephalopathies and Dementias Continuum 2016
13/21
support an autoimmune cause. TheseCSF findings, however, are encoun-tered in many idiopathic inflammatory CNS disorders, including multiplesclerosis. Oligoclonal bands are occa-sionally detected in nonautoimmunecontexts such as pathologically provenprimary neurodegenerative disordersor Jakob-Creutzfeldt disease. 21
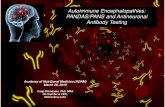
ANTIBODY TESTING An ti body pr of il es in cl ud e ne ur al( Table 8-2 , Table 8-3 , and Figure 8-3 )and non-neural IgG markers. Seroposi-
tivity for non-neural autoantibodiesdoes not confirm a diagnosis of an auto-immune CNS disorder, but does sup-port consideration of an autoimmunepathogenesis, particularly in those whohave negative testing for encephalitis-specific antibodies. Seropositivity may also trigger a trial of treatment. For example, detection of thyroid auto-
antibodies alone is not diagnostic of an autoimmune encephalopathy butgenerally supports the suspicion of autoimmunity. Also, a patient with cog-nitive symptoms who is seropositive for antinuclear and double-stranded DNA antibodies might have CNS lupus, 22
for which there is no specific antibody biomarker available.
The detection of a neural-specificantibody in serum or CSF may be di-rectly diagnostic of an autoimmuneneurologic disorder. Antibody testsperformed on serum alone might
suffice for paraneoplastic antibody testing, although overall combinedserum and CSF testing increases thediagnostic yield for classic paraneoplas-tic antibodies (such as collapsin responsemediator protein-5 [CRMP-5] IgG)somewhat. 23 However, in the case of NMDA receptor antibodies, CSF is al- ways more informative than serum. 24
FIGURE 8-3 Typical patterns of patient neural IgG antibody staining. Indirect immunofluorescence testing employscomposite of mouse brain tissues on which patient serum or CSF is applied. Panels A, B, and C showcerebellum, and panels D , E , and F show hippocampus. Dipeptidyl-peptidase 6 (DPPX) antibody ( A and D),
+ -aminobutyric acid B (GABA-B) receptor antibody ( B and E ), and N -methyl- D-aspartate (NMDA) receptor antibody ( C and F )are shown.
550 www.ContinuumJournal.com April 2016
Autoimmune Encephalopathies
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/17/2019 Autoimmune Encephalopathies and Dementias Continuum 2016
14/21
In contrast, VGKC complex anti-bodies are more readily detectable inserum than in CSF. 25 Although theseantibodies target antibodies physically related to Kv1.1, Kv1.2, and Kv1.6potassium channels, they may not tar-get the potassium channels themselves,and some target proteins physically coupled to potassium channels (LgI1and contactin-associated proteinlike 2[CASPR2]). However, in more than 50%of VGKC complex antibody Y positivecases, the LgI1 and CASPR2 antibodiesare not detected. 5 Although caution isadvised in interpreting such results, itis sometimes inaccurately stated that VGKC complex IgGs that are LgI1 or CASPR2 negative are always nonspecific.
Examples of other antibodies thattarget neural plasma membrane an-tigens that have been described inautoimmune encephalitis include gluta-matergic ! -amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid (AMPA)receptor, 26 + -aminobutyric acid A (GABA-A) receptor, 27 + -aminobutyricacid B (GABA-B) receptors, 28 andIgLON family member 5 (IgLON5)( Table 8-3 ).29 The latter disorder ispossibly at the interface of currentknowledge between autoimmuneand neurodegenerative disorders.Described in one study to date, pa-tients seropositive for IgLON5 anti-body have obstructive sleep apnea,sleep behavior symptoms, move-ment disorders, a lack of response toimmunotherapy, and a brainstem-and hypothalamus-restricted tauo-
pathy at autopsy. Of the patientsdescribed in one study, two out of eight had cognitive impairment. 29
ONCOLOGIC SIGNIFICANCE An autoimmune encephalopathy or dementia may occur as an aberrantby-product of an immune responsedirected against a non-neurologic can-cer. A paraneoplastic autoantibody
profile may predict the cancer type insome circumstances. An algorithmic
approach to testing for autoantibody profiles is usually a more sensitivediagnostic strategy than physician-selected single antibody testing. Some-times a single antibody will be positive,but in others positivity for multiple auto-antibodies will be detected. For ex-ample, seropositivity for amphiphysinantibody predicts either small cell car-cinoma or breast adenocarcinoma, butthe presence or absence of coexistingantibodies narrows that differentialdiagnosis. Among 63 patients at theMayo Clinic with amphiphysin anti-body and cancer history, 33 had smallcell lung carcinoma; of those patients,27 had coexisting neural-specific au-toantibodies that also predicted smallcell carcinoma. In contrast, 30 patients with amphiphysin-IgG seropositivity in whom breast adenocarcinoma wasfound were otherwise seronegative. 30
Seronegativity does not exclude aparaneoplastic cause. Suspicion for aparaneoplastic cause may also be raised
by risk factors obtained from the clin-ical history, such as a smoking history or previous cancer history. A thoroughphysical examination and CT of chest,abdomen, and pelvis are commonly undertaken as primary screeningtests. Other tests may be required de-pending on age, sex, and other risk factors. Testicular ultrasound or prostate-specific antigen testing and digital rec-tal prostate examination are requiredto evaluate for testicular and prostatecarcinomas, respectively. MRI or ultra-sound (including transvaginal imaging)of the pelvis and gynecologic examina-tion are required to evaluate for ovariancarcinoma or teratoma. Mammography and breast examination are required toevaluate for breast adenocarcinoma.Endoscopic examination of the upper and lower gastrointestinal tracts should
551Continuum (Minneap Minn) 2016;22(2):538 Y 558 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/17/2019 Autoimmune Encephalopathies and Dementias Continuum 2016
15/21
also be considered where appropriate.Positron emission tomography (PET)coregistered with CT (PET/CT) imag-ing increases the diagnostic yield for cancer by 20% for patients in whomstandard evaluations have been unre- vealing for cancer. 31
TREATMENTRandomized, controlled treatment tri-als for the treatment of autoimmuneCNS disorders are lacking. Treatmentdata are derived from case reports, caseseries, and expert opinion. 32 Based on
the available literature and the author’sexperience, a therapeutic approach isoutlined. 32 The treatment protocolmust be individualized for the patient,dictated by clinical severity, types of antibodies detected, and the presenceor absence of cancer. Also, responses toshort-term treatments usually informthe approach to long-term treatment,if needed.
ImmunotherapyMost of the recommendations dis-cussed in the following sections aresupported by observational studies andthe experiences of the author and other colleagues at Mayo Clinic for managingautoimmune neurologic disorders( Table 8-5 and Figure 8-4 ).
The type of antibody identified may predict the neurologic response to im-munotherapy. Detection of antibodiestargeting intracellular antigens such asPurkinje cell cytoplasmic antibody type 1 (PCA-1) (anti-Yo) portends limi-
ted responses to immunotherapy anda poor prognosis. This may be the casebecause the immune process is medi-ated by cytotoxic T cells, leading toirreversible neuronal degeneration. 33
On the other hand, detection of anti-bodies targeting neural surface antigens(such as NMDA receptors and LgI1)usually predicts a more favorable out-come. This may be explained by the
pathogenic effects of these antibodies(impaired neuronal or glial function,
but not destruction, at least early on), which may be reversed by immuno-therapy (eg, removal by plasma ex-change) resul t ing in reversal of neurologic dysfunction. 34 The timingof immunotherapy is important. Caseseries of patients with autoimmuneCNS disorders have demonstrated thatearly immunotherapy confers a better treatment outcome than delayed ther-apy. 2,35,36 A lack of response to onemodality (eg, corticosteroids) does notexclude a response to another agent(eg, IV immunoglobulin [IVIg]).
The immunotherapy protocol hastwo components: acute therapy andchronic therapy. Before starting treat-ment, baseline neurologic and ancillary evaluations should be performed toestablish parameters for objectivetreatment-response monitoring, as de-scribed earlier. Antibody titers havelimited use as a surrogate of clinicaloutcome in the acute phase of treat-ment because values usually reduce with treatment even if therapy is notclinically beneficial. There may be a rolefor antiepileptic drug therapy in addi-tion to immunotherapy in those pa-tients who have seizures as well ascognitive dysfunction.
Acute TherapyFor acute therapy, a trial of high-dosepulse IV corticosteroid therapy isusually the first treatment. IVIg may be used in patients who are unlikely totolerate corticosteroids or are at risk for
diabetes mellitus (including patientspositive for glutamic acid decarboxylase65 [GAD65] antibodies). Typical treat-ment protocols include 1000 mg/d of IV methylprednisolone or 0.4 g/kg/dof IVIg for 5 consecutive days. Mostpatients with autoimmune encepha-litis require maintenance treatmentthereafter. In those patients with se- vere encephali tis, dai ly oral or IV
KEY POINTSh Normal results of MRI,
CSF testing, andantibody testing do notexclude an autoimmuneencephalopathydiagnosis, but normalfindings in allthree make thediagnosis unlikely.
h In a paraneoplasticcontext, theautoantibody profilemay narrow the searchfor cancer.
552 www.ContinuumJournal.com April 2016
Autoimmune Encephalopathies
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/17/2019 Autoimmune Encephalopathies and Dementias Continuum 2016
16/21
TABLE 8-5 Commonly Used Therapies for Autoimmune Encephalopathiesa
Treatment Regimen Route Common Side EffectsTherapeuticPhase
Methylprednisolone 1000 mg/d for 3 days, followedby 1000 mg/wk for 6 Y 8 weeks
IV Insomnia,psychiatricsymptoms,hyperglycemia, electrolyteimbalances, fluid retention,hypertension, peptic ulcer,Cushing syndrome, cataracts,infection and osteoporosis,avascular necrosis, addisoniancrisis on rapid withdrawal ofcorticosteroid
Acute andmaintenance(taperingdose)
IV immunoglobulin(IVIg)
0.4 g/kg/d for 5 days, followedby 0.4 g/kg/wk for 6 Y 8 weeks
IV Headache, aseptic meningitis,thromboembolic events, acute
renal failure and anaphylaxisdue to IgA deficiency (rare)
Acute andmaintenance
(taperingdose)
Plasma exchange 1 exchange every other dayfor 10 Y 14 days
IV (usuallythrougha centralline)
Hypotension, electrolyteimbalance (hypocalcemia-related perioral paresthesia)
Related to IV central line:infection, hemorrhage,thrombosis, and pneumothorax
Acute
Azathioprine Initially 1.5 mg/kg/d, target2 Y 3 mg/kg/d (guided by5-point mean corpuscularvolume increasefrom baseline)
Oral Gastrointestinal symptoms(eg, nausea, vomiting,diarrhea), hypersensitivityreactions, alopecia, cytopenia,and hepatotoxicity; rare
complications are lymphomaand infection
Maintenance
Mycophenolatemofetil
Initially 500 mg twice daily,target 1000 mg twice daily
Oral Gastrointestinal symptoms(eg, diarrhea, nausea,vomiting), hypertension,peripheral edema, infections,myelosuppression, lymphoma,and other malignancies
Maintenance
Rituximab 375 mg/m 2 /wk for 4 weeks, or1000 mg/wk for 2 weeks
IV Allergic reaction, opportunisticinfection, reactivation oftuberculosis infection orhepatitis B infection
Acute ormaintenance
Cyclophosphamide IV: 500 Y 1000 mg/m 2 /mo
for 3 Y
6 monthsOral: 1 Y 2 mg/kg/d(50 Y 100 mg/d)
IV or oral Gastrointestinal symptoms
(eg, nausea, vomiting),alopecia, mucositis,hemorrhagic cystitis(administer mesnaprophylaxis), infertility,and myelo suppression
Acute or
maintenance
IgA = immunoglobulin A; IV = intravenous.a Modified with permission from McKeon A et al, Continuum (Minneap Minn). 3 journals.lww.com/continuum/Fulltext/2010/04000/
IMMUNOTHERAPY_RESPONSIVE_DEMENTIAS_AND.8.aspx . B 2010 American Academy of Neurology.
553Continuum (Minneap Minn) 2016;22(2):538 Y 558 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
http://journals.lww.com/continuum/Fulltext/2010/04000/IMMUNOTHERAPY_RESPONSIVE_DEMENTIAS_AND.8.aspxhttp://journals.lww.com/continuum/Fulltext/2010/04000/IMMUNOTHERAPY_RESPONSIVE_DEMENTIAS_AND.8.aspxhttp://journals.lww.com/continuum/Fulltext/2010/04000/IMMUNOTHERAPY_RESPONSIVE_DEMENTIAS_AND.8.aspx
-
8/17/2019 Autoimmune Encephalopathies and Dementias Continuum 2016
17/21
steroids are usually needed. For those with milder disorders, weekly IV methylprednisolone infusions may suf-fice. In patients with limited early re-sponses to steroids, plasma exchangecan be given as every other day ex-changes (five to seven treatments) for
10 to 14 days. If IVIg is the primary treatment used, a weekly infusion of 0.4 g/kg can be used.
After the initial trial of therapy, thepatient should be reevaluated toobjectively determine the response toimmunotherapy. If a rapid series of trials
FIGURE 8-4 A non Y evidence-based treatment algorithm for the treatment of autoimmuneencephalopathy or dementia.CSF = cerebrospinal fluid; EEG = electroencephalog ram; IV = intravenous; IVIg =
intravenousimmunoglobulin;MRI = magneticresonance imagin g; PET= positronemissiontomography.
Modified with permission from McKeon et al, Continuum (Minneap Minn). 3 journals.lww.com/continuum/Fulltext/2010/
04000/IMMUNOTHERAPY_RESPONSIVE_ DEMENTIAS_AND.8.aspx . B
2010 American Academy of Neurology.
554 www.ContinuumJournal.com April 2016
Autoimmune Encephalopathies
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
http://journals.lww.com/continuum/Fulltext/2010/04000/IMMUNOTHERAPY_RESPONSIVE_DEMENTIAS_AND.8.aspxhttp://journals.lww.com/continuum/Fulltext/2010/04000/IMMUNOTHERAPY_RESPONSIVE_DEMENTIAS_AND.8.aspxhttp://journals.lww.com/continuum/Fulltext/2010/04000/IMMUNOTHERAPY_RESPONSIVE_DEMENTIAS_AND.8.aspxhttp://journals.lww.com/continuum/Fulltext/2010/04000/IMMUNOTHERAPY_RESPONSIVE_DEMENTIAS_AND.8.aspx
-
8/17/2019 Autoimmune Encephalopathies and Dementias Continuum 2016
18/21
of immunotherapy are not beneficialin an acutely ill hospitalized patient with a well-characterized antibody-mediated encephalitis, steroid or IVIg therapy should be continued, andanother immunosuppressant (such asrituximab or cyclophosphamide)should be introduced early. 37 In addi-tion, therapeutic levels of antiepilep-tic drugs and supportive therapy for weeks to months are required. Sup-portive therapies may be required inan intensive care unit setting andinclude optimized blood pressure
control, treatment of autonomic insta-bility, deep venous thrombosis prophy-laxis, monitoring and treatment of intercurrent infections, and mainte-nance of fluid and electrolytes. Thisscenario is particularly relevant for patients with anti-NMDA receptor en-cephalitis, who frequently requiremonths of supportive care in additionto immunosuppression.
For patients with severe disorders,upon completion of the initial roundsof acute IV treatments, the author favors60 mg/d oral prednisone for 3 monthsfollowed by taper by 10 mg/mo until adose of 10 mg/d is reached, and thentaper by 1 mg/mo until discontinued.For patients with a history of difficultto treat or relapsing disorders, theauthor simultaneously starts an oralsteroid Y sparing agent.
Chronic TherapyThe most important principle is theneed for aggressive treatment in the
first 6 to 9 months when relapse is mostlikely to occur. Relapses frequently occur during rapid immunotherapy taper or discontinuation, as noted tooccur in patients with NMDA receptor, AMPA receptor, and VGKC complex antibodies. Gradual tapering doses of steroids or IVIg may suffice for mainte-nance of remission, but some patientsmay benefit from maintenance immu-
notherapy for an even longer period of time. The duration for which patientsshould be treated has not been deter-mined by clinical trials. In essence, theduration of treatment is determined by the treating clinician based on enceph-alitis severity and presence or absenceof relapses. For patients in whomrituximab therapy was employed duringthe acute illness, that may also suffice asmaintenance therapy (every 6 monthsor when the B-lymphocyte marker CD20 becomes detectable).
Azathioprine or mycophenolate
mofetil could be used as an oral main-tenance immunosuppressive agent inthose patients in whom it is desirable totransition from corticosteroid or cyclo-phosphamide treatment. The initiationof a chronic oral immunosuppressiveagent should overlap with gradual taper of oral corticosteroids and/or IVIginfusions over that time frame. Thisapproach facilitates the oral immuno-suppressants taking effect before thesteroids or IVIg treatments are com-pleted. Some patients relapse despitethis approach and are corticosteroiddependent. In these patients, a low oralprednisone dose (10 mg/d to 20 mg/dor alternate day) may be needed.
Careful monitoring for side effectsof long-term immunotherapy is criti-cal. Surveillance includes monitoringof blood counts and tests of liver andrenal function. Before using azathio-prine, thiopurine methyltransferase(TPMT) deficiency needs to be excludedby establishing the TPMT genotype
or measuring the TPMT enzyme level(both are blood tests). Among patients with neuromyelitis optica, a rise of mean corpuscular volume of at least 5points from baseline is indicative of efficacy. 38 For those treated withmycophenolate mofetil, the drug levelcan be measured to avoid undertreat-ment or toxicity. The level of mycophe-nolic glucuronide (an enzyme that
KEY POINTh In patients in
whom a responseto immunotherapyis documented,maintenance treatmentfor 6 to 9 months(depending on severity)is usually required.
555Continuum (Minneap Minn) 2016;22(2):538 Y 558 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/17/2019 Autoimmune Encephalopathies and Dementias Continuum 2016
19/21
metabolizes mycophenolate) may beindicative of risk for drug toxicity (if the level is low) or a subtherapeuticdrug level (if the level is high).
Patients taking glucocorticoids mustalso take elemental calcium, at least1500 mg/d and vitamin D 1000 IU/d,either through diet or supplements, asdeterioration of bone mineral density may occur soon after starting steroiduse. Baseline and follow-up bone den-sitometry and bisphosphonate treat-ment should be considered in patientsrequiring more than 3 months of gluco-
corticoid treatment. Pneumocystis jiroveci pneumonia prophylaxis shouldconsist of 1 trimethoprim/sulfamethox-azole double-strength tablet 3 times per week for patients on chronic cortico-steroids. Alternatives for sulfa-allergicpatients include daily oral dapsone or monthly inhaled pentamidine. A protonpump inhibitor could be considered inpatients with upper gastrointestinalsymptoms or history of ulceration.Monitoring for hyperglycemia and hy-pertension should be routine.
Cancer TreatmentFor patients with paraneoplastic disor-ders, treatment of cancer may alsopermit stabilization or improvement of the neurologic symptoms. Occasionally,tumor treatment alone is very effective(eg, teratoma removal in patients withNMDA receptor encephalitis), but rarely suffices alone as treatment for neuro-logic symptoms. 37 For other patients,cancer treatment may (at best) bring
about stabilization (eg, small cell carci-noma treatment in a patient with ANNA-1). Neurologic therapeutic ben-efit may also occur because of chemo-therapy’s immunosuppressant effects.
For patients with classic paraneo-plastic encephalitis, improvements arerarely dramatic. Plasma exchange and IV corticosteroids may bring about neuro-logic stability. If neurologic symptoms
are severe despite cancer treatment,cyclophosphamide (given as 6 monthly
IV pulses or daily oral therapy for 6 to12 months) may be of utility in thosepatients with limited-stage cancer, com-plete cancer remission, short durationof neurologic symptoms, and a goodoncologic performance status. 39
CONCLUSION Autoimmune encephalopathies anddementias are important to recognizebecause they are potentially treatable.The comprehensive evaluation consistsof detailed clinical history (includingautoimmune), imaging, electrophysio-logic, and immunologic studies. Early treatment with immunotherapy is crit-ical to optimize outcomes.
REFERENCES1. Chitravas N, Jung RS, Kofskey DM, et al.
Treatable neurological disordersmisdiagnosed as Creutzfeldt-Jakob disease.Ann Neurol 2011;70(3):437 Y 444.doi:10.1002/ana.22454.
2. Flanagan EP, McKeon A, Lennon VA, et al.Autoimmune dementia: clinical course andpredictors of immunotherapy response.Mayo Clin Proc 2010;85(10):881 Y 897.doi:10.4065/mcp.2010.0326.
3. McKeon A, Lennon VA, Pittock SJ.Immunotherapy-responsive dementiasand encephalopathies. Continuum(Minneap Minn) 2010;16(2 Dementia):80 Y 101. doi:10.1212/01.CON.0000368213.63964.34
4. Irani SR, Alexander S, Waters P, et al.Antibodies to Kv1 potassiumchannel-complex proteins leucine-rich,glioma inactivated 1 protein andcontactin-associated protein-2 in limbicencephalitis, Morvan’s syndrome andacquired neuromyotonia. Brain 2010;133(9):2734 Y 2748. doi:10.1093/brain/awq213.
5. Klein CJ, Lennon VA, Aston PA, et al. Insightsfrom LGI1 and CASPR2 potassium channelcomplex autoantibody subtyping. JAMANeurol 2013;70(2):229 Y 234. doi:10.1001/ jamaneurol.2013.592.
6. Geschwind MD, Tan KM, Lennon VA, et al.Voltage-gated potassium channel autoimmunitymimicking Creutzfeldt-Jakob disease. ArchNeurol 2008;65(10):1341 Y 1346. doi:10.1001/ archneur.65.10.1341.
KEY POINTh Prophylaxis against
opportunistic infectionand osteoporosis andmonitoring forhypertension anddiabetesmellitus should beundertaken in patientstaking corticosteroids.
556 www.ContinuumJournal.com April 2016
Autoimmune Encephalopathies
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/17/2019 Autoimmune Encephalopathies and Dementias Continuum 2016
20/21
7. McKeon A, Pittock SJ. Paraneoplasticencephalomyelopathies: pathology andmechanisms. Acta Neuropathol2011;122(4):381 Y 400. doi:10.10007/ s00401-011-0876-1.
8. McKeon A, Ahlskog JE, Britton JW, et al.Reversible extralimbic paraneoplasticencephalopathies with large abnormalitieson magnetic resonance images. Arch Neurol2009;66(2):268 Y 271. doi:10.1001/ archneurol.2008.556.
9. Lucchinetti CF, Kimmel DW, Lennon VA.Paraneoplastic and oncologic profiles ofpatients seropositive for type 1 antineuronalnuclear autoantibodies. Neurology1998;50(3):652 Y 657. doi:10.1212/ WNL.50.3.652.
10. Irani SR, Michell AW, Lang B, et al.Faciobrachial dystonic seizures precede Lgi1antibody limbic encephalitis. Ann Neurol2011;69(5):892 Y 900. doi:10.1002/ana.22307.
11. Dalmau J, Gleichman AJ, Hughes EG, et al.Anti-NMDA-receptor encephalitis: caseseries and analysis of the effects of antibodies.Lancet Neurol 2008;7(12):1091 Y 1098.doi:10.1016/S1474-4422(08)70224-2.
12. Dalmau J, Graus F, Villarejo A, et al. Clinicalanalysis of anti-Ma2-associated encephalitis.Brain 2004;127(pt 8):1831 Y 1844.doi:10.1093/brain/awh203.
13. Pittock SJ, Parisi JE, McKeon A, et al.Paraneoplastic jaw dystonia and laryngospasm
with antineuronal nuclear autoantibody type 2(anti-Ri). Arch Neurol 2010;67(9):1109 Y 1115.doi:10.1001/archneurol.2010.209.
14. Boronat A, Gelfand JM, Gresa-Arribas N, et al.Encephalitis and antibodies todipeptidyl-peptidase-like protein-6, a subunitof Kv4.2 potassium channels. Ann Neurol2013;73(1):120 Y 128. doi:10.1002/ana.23756.
15. Tobin WO, Lennon VA, Komorowski L, et al.DPPX potassium channel antibody:frequency, clinical accompaniments, andoutcomes in 20 patients. Neurology2014;83(20):1797 Y 1803. doi:10.1212/ WNL.0000000000000991.
16. Carvajal-Gonzalez A, Leite MI, Waters P, et al.Glycine receptor antibodies in PERM andrelated syndromes: characteristics, clinicalfeatures and outcomes. Brain 2014;137(pt 8):2178 Y 2192. doi:10.1093/brain/awu142.
17. Castillo P, Woodruff B, Caselli R, et al.Steroid-responsiveencephalopathy associatedwith autoimmune thyroiditis. Arch Neurol2006;63(2):197 Y 202. doi:10.1001/ archneur.63.2.197.
18. Susac JO, EganRA, Rennebohm RM,Lubow M.Susac’s syndrome: 1975-2005 microangiopathy/
autoimmune endotheliopathy. J Neurol Sci2007;257(1 Y 2):270 Y 272. doi:10.1016/ j.jns.2007.01.036.
19. Fauser S, Talazko J, Wagner K, et al.FDG-PET and MRI in potassium channelantibody-associated non-paraneoplasticlimbic encephalitis: correlation with clinicalcourse and neuropsychology. Acta NeurolScand 2005;111(5):338 Y 343. doi:10.1111/ j.1600-0404.2005.00406.x.
20. Rudzinski LA, Pittock SJ, McKeon A, et al.Extratemporal EEG and MRI findings inANNA-1 (anti-Hu) encephalitis. Epilepsy Res2011;95(3):255 Y 262. doi:10.1016/ j.eplepsyres.2011.04.006.
21. Janssen JC, Godbolt AK, Ioannidis P, et al.The prevalence of oligoclonal bands in the
CSF of patients with primaryneurodegenerativedementia. J Neurol 2004;251(2):184 Y 188.doi:10.1007/s00415-004-0296-4.
22. Joseph FG, Lammie GA, Scolding NJ. CNSlupus: a study of 41 patients. Neurology2007;69(7):644 Y 654. doi:10.1212/ 01.wnl.0000267320.48939.d0.
23. McKeon A, Pittock SJ, Lennon VA. CSFcomplements serum for evaluatingparaneoplastic antibodies and NMO-IgG.Neurology 2011;76(12):1108 Y 1110.doi:10.1212/WNL.0b013e318211c379.
24. Gresa-Arribas N, Titulaer MJ, Torrents A, et al.Antibody titres at diagnosis and duringfollow-up of anti-NMDA receptorencephalitis: a retrospective study. LancetNeurol 2014;13(2):167 Y 177. doi:10.1016/ S1474-4422(13)70282-5.
25. Vincent A, Buckley C, Schott JM, et al.Potassium channel antibody-associatedencephalopathy: a potentiallyimmunotherapy-responsive form of limbicencephalitis. Brain 2004;127(pt 3):701 Y 712.doi:10.1093/brain/awh077.
26. Lai M, Hughes EG, Peng X, et al. AMPAreceptor antibodies in limbic encephalitisalter synaptic receptor location. Ann Neurol2009;65(4):424 Y 434. doi:10.1002/ana.21589.
27. Petit-Pedrol M, Armangue T, Peng X, et al.
Encephalitis with refractory seizures, statusepilepticus, and antibodies to the GABAAreceptor: a case series, characterisation of theantigen, and analysis of the effects ofantibodies. Lancet Neurol 2014;13(3):276 Y 286.doi:10.1016/S1474-4422(13)70299-0.
28. Lancaster E, Lai M, Peng X, et al.Antibodies to the GABA(B) receptor inlimbic encephalitis with seizures: caseseries and characterisation of the antigen.Lancet Neurol 2010;9(1):67 Y 76. doi:10.1016/ S1474-4422(09)70324-2.
557Continuum (Minneap Minn) 2016;22(2):538 Y 558 www.ContinuumJournal.com
Copyright © American Academy of Neurology. Unauthorized reproduction of this article is prohibited.
-
8/17/2019 Autoimmune Encephalopathies and Dementias Continuum 2016
21/21
29. Sabater L, Gaig C, Gelpi E, et al. Anovel non-rapid-eye movement andrapid-eye-movement parasomnia with sleepbreathing disorder associated with antibodiesto IgLON5: a case series, characterisation ofthe antigen, and post-mortem study. LancetNeurol 2014;13(6):575 Y 586. doi:10.1016/ S1474-4422(14)70051-1.
30. McKeon A, Pittock SJ, Lennon VA.Stiff-person syndrome with amphiphysinantibodies: distinctive features of a raredisease. Neurology 2009;73(24):2132.doi:10.1212/WNL.0b013e3181bd6a72.
31. McKeon A, Apiwattanakul M,Lachance DH, et al. Positron emissiontomography-computed tomography inparaneoplastic neurologic disorders:systematic analysis and review. Arch Neurol2010;67(3):322 Y 329. doi:10.1001/ archneurol.2009.336.
32. McKeon A. Immunotherapeutics forautoimmune encephalopathies anddementias. Curr Treat Options Neurol2013;15(6):723 Y 737. doi:10.1007/ s11940-013-0251-8.
33. Albert ML, Austin LM, Darnell RB. Detectionand treatment of activated T cells in thecerebrospinal fluid of patients withparaneoplastic cerebellar degeneration.Ann Neurol 2000;47(1):9 Y 17. doi:10.1002/ 1531-8249(200001)47.
34. Hughes EG, Peng X, Gleichman AJ, et al.Cellular and synaptic mechanisms ofanti-NMDA receptor encephalitis. J Neurosci2010;30(17):5866 Y 5875. doi:10.1523/ JNEUROSCI.0167-10.2010.
35. Pittock SJ, Yoshikawa H, Ahlskog JE, et al.Glutamic acid decarboxylase autoimmunitywith brainstem, extrapyramidal, and spinalcord dysfunction. Mayo Clin Proc 2006;81(9):1207 Y 1214. doi:10.4065/81.9.1207.
36. Quek AM, Britton JW, McKeon A, et al.Autoimmune epilepsy: clinical characteristicsand response to immunotherapy. ArchNeurol 2012;69(5):582 Y 593. doi:10.1001/ archneurol.2011.2985.
37. Titulaer MJ, McCracken L, Gabilondo I, et al.Treatment and prognostic factors forlong-term outcome in patients with anti-NMDAreceptor encephalitis: an observational cohortstudy. Lancet Neurol 2013;12(2):157 Y 165.doi:10.1016/S1474-4422(12)70310-1.
38. Costanzi C, Matiello M, Lucchinetti CF, et al.Azathioprine: tolerability, efficacy, andpredictors of benefit in neuromyelitis optica.Neurology 2011;77(7):659 Y 666. doi:10.1212/ WNL.0b013e31822a2780.
39. Vernino S, O’Neill BP, Marks RS, et al.Immunomodulatory treatment trial forparaneoplastic neurological disorders.Neuro Oncol 2004;6(1):55 Y 62. doi:10.1215/ S1152851703000395.
558 www.ContinuumJournal.com April 2016
Autoimmune Encephalopathies