Practical Guide: Autism and Other Pervasive Developmental ...
SW 644: ISSUES IN DEVELOPMENTAL DISABILITIES
AUTISM AND PERVASIVE DEVELOPMENTAL DISORDERS
Christine Iyama, M.D.
Unit 1 – Overview
Issues in Developmental Disabilities: Important Things I’ve learned about Autism in 30 Years(Slide 1)
Tina Iyama-Kurtycz:’ Hi. My name is Tina Iyama-Kurtycz and I’m a developmental pediatrician at the University of Wisconsin in Madison. I am delighted to be able to share with you today some of the things I’ve learned about autism over the past 30 years ‘ from working with children with autism and their families. Each child has a unique story to tell and I’ve learned so much about autism from them and it shaped my understanding of what autism was 30 years ago and what it has become today.
Overview(Slide 2)
I wanted to start this hour by sharing with you some art of a former patient of mine named Jin Murakami.’ He has autism and moderate mental retardation but he’s an artist and I want to tell you it’s not because he’s representative of all children with autism, but many children with autism have unique strengths and abilities if we can recognize them and appreciate them.
Overview(Slide 3)
And so I want you to go to his website and buy his art which is shown on the slide. But I also wanted to share with you just some of the incredible, tiny miniature animals that he creates out of air-dry clay.
Overview(Slide 4)
There’s a ruler in this one to show you how tiny they really are.
Overview(Slide 5 & 6)
It’s really quite amazing.
Overview(Slide 7)
The overview of this talk is that we’re going to start with talking about the idea of autism, and I’ll explain that. I’m going to spend some time on the state-of-the-art of early diagnosis and early intervention, because that’s really a hot topic in autism right now. We’re going to talk

about what we know about causes, what we know about effective treatment, and what little is known about actual outcome.
Overview(Slide 8)
So the first principle I want to share with you is that autism is a construct. It’s an idea. It’s a way of describing a certain pattern of development. There isn’t any absolute truth. Autism isn’t something you either have or you don’t have. It’s not that clear. Autism describes a certain pattern of strengths and weaknesses. Strengths, say in memory or visual perception, in weaknesses, in language, in social communication that may be present to a disabling degree. It’s really an important idea, though, because if you and I don’t share the same idea of autism, then we won’t agree about who has it and who doesn’t.
Overview(Slide 9)
This slide, called the current concept of pervasive developmental disorders gives you the broad overview of what the autism spectrum is. This hasn’t changed for about 10 years now. It will change when the new edition of the diagnostic and statistical manual for American Psychiatric Association comes out, but right now this is still our conceptualization of the autism spectrum. The psychiatrist termed autism by pervasive developmental disorder and that’s the umbrella for the entire spectrum. And under that umbrella, there are five conditions.
On the lower left-hand side of the slide, you’ll see CDD which stands for Childhood Disintegrative Disorder and a condition called Rhett Syndrome. This describes the more severe disabling end of the spectrum. These children have very significant neurodevelopment disabilities. In the center you have the idea that autism disorder, autistic disorder, autism ‘ they’re all the same name ‘ and those are the kids who meet criteria for autism. And then in the upper right-hand corner, you have children who are more mildly affected by something called Asperger Syndrome. These are usually children with average intelligence who have difficulty with making and keeping friends.
Everything outside those circles is called pervasive developmental disorder ‘ not otherwise specified, which is a hard thing to explain to a family that their child has; but it’s how our diagnostic constructs are arranged. So that means that if you have some characteristics similar to children with autism but not enough to use one of those other four diagnoses, then you use the term PDD-NOS.’ The confusing thing, of course, is that sometimes PDD-NOS is shortened to PDD which is just merely confusing. The other thing to take away from this line is that these aren’t really black and white circles.
Think of them as clouds. Clouds have fuzzy edges. If you’re in the center of the cloud you know you’re in a cloud; but when you get to the edge, it’s really kind of harder to tell. And that’s a good idea to take away with you about these diagnostic conditions.
Unit 2 – The Clinical Diagnosis of Autism
The Clinical Diagnosis of Autism(Slide 10)
This slide shows the diagnostic and statistical manual of the American Psychiatric Association. This is sort of our diagnostic bible that we use to determine whether a person has a behaviorally defined condition or not. And there are 12 characteristics ‘ 4 social, 4 communication, 4 behavioral ‘ for a total of 12.

To have a diagnosis of autism, you really only need six of them. So you don’t need all these characteristics. Parents think, ‘Well, they have some of these characteristics, but not all of them.’ And that still could be a diagnosis of autism. You need at least two social characteristics, one communication and one behavior, and at least six altogether to use the term autism. If you have four or five, you can use that term that I mentioned before, PDD-NOS. And I want to go over each of the kinds of characteristics that we’re looking for.
The Clinical Diagnosis of Autism(Slide 11)
So under social ‘ there are four social characteristics. The first one has to do with impaired non-verbal communication. So this is where the child who doesn’t make eye contact or the child who doesn’t wave or that child who doesn’t gesture, that’s where that comes in. Impaired peer interactions ‘ that is children have difficulty where they may lack interest in other children. Yesterday I had a father tell me that his child saw other children as an impediment to getting toys. So you know they just don’t have the same social interest in other children as other children their age. That is compared to their developmental level and that is an idea that we have to put in right here.
And that is if you have a 4-year-old child who is developmentally only a 2-year-old, you can’t expect a lot of 2-year-old social interactions. I mean we don’t have very many expectations for peer play in 2. So you have to know the child’s developmental level before you can apply any of these criteria. The third social characteristic is lack of sharing of experiences, discoveries or achievements with others. This is the child who really just doesn’t point out and say, ‘Look, mommy’ and/or ‘Look at this’ or ‘See what I did’ like almost all 18 months to 2-year olds are always kind of in your face showing new stuff.
These are kids who really don’t share those experiences as easily. And the fourth social criteria is lack of give and take in social relationships. These are children whose parents feel like it’s always his way or the highway. And in case you’re wondering why I use his and him a lot is because four to five times as many boys have autism as girls. So statistically, it’s more likely to be a boy. So I may refer to most of the kids as boys because they mostly are. But these kids don’t give and take. There’s not a back and forth relationship to it. It’s parents following the child whatever the child wants to do and the child is very self-directed in their play.
The Clinical Diagnosis of Autism(Slide 12)
In the fourth communication characteristics, we use delay in development of spoken language without adequate compensation. For example, the child who’s deaf but learned sign language doesn’t have a delay in communication. And so that wouldn’t fit a child who’s deaf. But these are kids who don’t have communication and they don’t figure out any other way to communicate. They may pull their parents to what they want and put their parents’ hands on the thing that they want, but they really don’t do anything themselves to request. In children who have a lot of words and sentences, they may have impaired conversation.
And conversation is a give and take thing where I say something like, ‘I like vanilla ice cream,’ then the other kid goes, ‘Oh, I really like cookie dough ice cream,’ and you go back and forth. Children with autism may answer questions, but you have to keep supplying the questions. Children with autism often have echolalia or atypical or stereotyped verbalizations. These may be kids whose only full sentences come from videos or stories that they’ve read. They may repeat exactly what you’ve said to them and not answer a question if you say, ‘Do you want me to carry you?’ They will say ‘carry you’. They won’t say ‘carry me’. And so they have trouble with the you and I pronouns.

And then they may have a lot of jargon that’s just something that babies do babble without meaning. It sounds like conversation sometimes and kids with autism may jargon. You might see that they are talking to themselves a lot rather than directing that verbalization towards an adult. And although this doesn’t really fit because it’s play, but they didn’t know where else to put it, this criteria about lack of make believe or pretend to play is important. The more a child has global cognitive delays in addition to autism, the more likely this is to be true.
The children who really just don’t understand how to use a doll or action figures or characters to create a story or care-take for something that isn’t real.
The Clinical Diagnosis of Autism(Slide 13)
And then the behavioral characteristics, there are four of these and the first one is developing a restricted range of interest in something very specific and some people call it obsessions, I like to call it passions because, really, where’s the line between passion and obsession? But I’ve had children who, for example, know everything there is to know about fire extinguishers or one child who knows where every escalator is in every building he’s ever been in.
It’s just interesting. We don’t know why certain kids like certain things, but they do, and they tend to be focused on that particular thing. There may be non-functional routines or rituals ‘ children who have many, many rules for how everything has to be. Once child made his mother say something a thousand times before she could leave him at daycare. I mean, just really non-functional necessary things that parents have to do for them. You may also see what is classically seen in autism is hand flapping or toe walking, atypical finger movements. These are just unusual and stereotype movements that children do that don’t seem to serve any particular purpose.
And then the last behavioral characteristic has to do with a preoccupation with a part of an object. So a child may like things for how they line up or they may like a toy for how spinny the wheels are so they’ll take a train and turn it upside down and spin the wheels instead of using it like a train. There are kids who like to open and close doors or turn on and off light switches. So something that they’re liking it not for the real function of the object but for something that’s satisfying to them.
The Clinical Diagnosis of Autism(Slide 14)
This slide states that these characteristics have to have a functional impact on the life of the child and that is essential. You can have a little bit of anxiety and not have an anxiety disorder if it doesn’t affect how you function. So just like anxiety, kids with autism can have a little bit and if they’re not having difficulty in either their home or their school, then a diagnosis isn’t needed. So we want to know that this is actually impairing a child in some disabling degree.
The Clinical Diagnosis of Autism(Slide 15)
These symptoms need to be recognized before three years of age. They have to have an onset before three years of age.
Actually, some parents don’t recognize these characteristics before three. They may just value eccentricity or they might be in denial that there’s a problem, but whatever. Parents may not recognize it, but to make a diagnosis of autism, those MDs should be able to elicit a history that this started before three.

The Clinical Diagnosis of Autism(Slide 16)
OK now, so here’s a slide of my ideal world. You’ll see two curbs ‘ one in which all children who are not autistic would stand and then another section of the curb where all the children with autism would stand and it would be very clear and I would be able to do something else with my professional life because it would be easy and everyone would agree. That would be really nice.
And if you know any physicians in your life you know that we like clarity. We like things to be black and white and clear.
The Clinical Diagnosis of Autism(Slide 17)
And unfortunately, our real world, the real world slide involves a lot of overlap between non-autistic and autistic. It’s just life. If you have classic characteristics and you fall solidly underneath the curb that is for autism, it will all agree. We’ll mostly agree that this child has autism. Most children who are not typically developing will fall under the non-autistic curb very nicely. But there are kids who stand in the middle there and is this a kid who has a couple of autistic characteristics who will be normal or is this a kid with a couple of autistic characteristics who really has more greater disability than that.
So it’s hard to tell when kids are 2 or 3, which way that’s going to go. And it makes it difficult for us to be clear with families about, ‘Oh yes, your child definitely is this or that.’ It’s just not that clear and this kind of curb exists for every characteristic you look at in autism. So look at hand flapping. Not every kid who flaps their hands has autism. Speech and language. Some kids are more impaired in speech and language. Some kids are more sociable. So it’s any characteristic you look at has a curb with an overlap into the typical population.
The Clinical Diagnosis of Autism(Slide 18)
So another principle is represented by this cardboard box, and that children are more complex than the diagnostic boxes we have to use. You may have noticed that occupational therapist will use the term sensory processing disorder to describe children who have an autistic spectrum disorder that physical therapist often see motor planning issues in the child’s movement. A speech and language person might see auditory processing problems in the child who has autism.
A child psychiatrist often see ADHD or anxiety disorder. Developmental pediatricians tend to see autistic spectrum disorders, but we all kind of see the things we were trained to see and use the boxes we were trained to use. That explains why children often have many diagnoses from different kinds of professionals.
The Clinical Diagnosis of Autism(Slide 19)
The other important thing, there are lots of important things, I’m sorry about that, but one of the things to recognize is that autism itself is just one aspect of complex central nervous system dysfunction. It’s not this entity that exists outside of other kinds of disabilities.
So if you look at this list, if you take all the premature infants that graduate from a nursery and

you do an autism screener on them, 25% fail the screener. If you actually look at kids who have cerebral palsy, about 15% of those kids have autism. If you look at all the children with mental retardation or a cognitive disability, somewhere between 10% and 18% will have an autistic spectrum disorder and that is compared to the population which is at or just slightly below 1%. So it’s elevated in every disability group.
We don’t have numbers for ADHD, learning disabilities and epilepsy; but those numbers would be higher than 1%. So it’s the social and communicative aspect of complex central nervous system dysfunction. Child psychiatrists actually give us a very good technique for using these different terms and that is of comorbidity. So you can have both epilepsy and autism. You can have cerebral palsy and autism. You don’t have to have one or the other. Comorbidity allows us to describe the things that are most disabling and most important to address in a child’s life.
The Clinical Diagnosis of Autism(Slide 20)
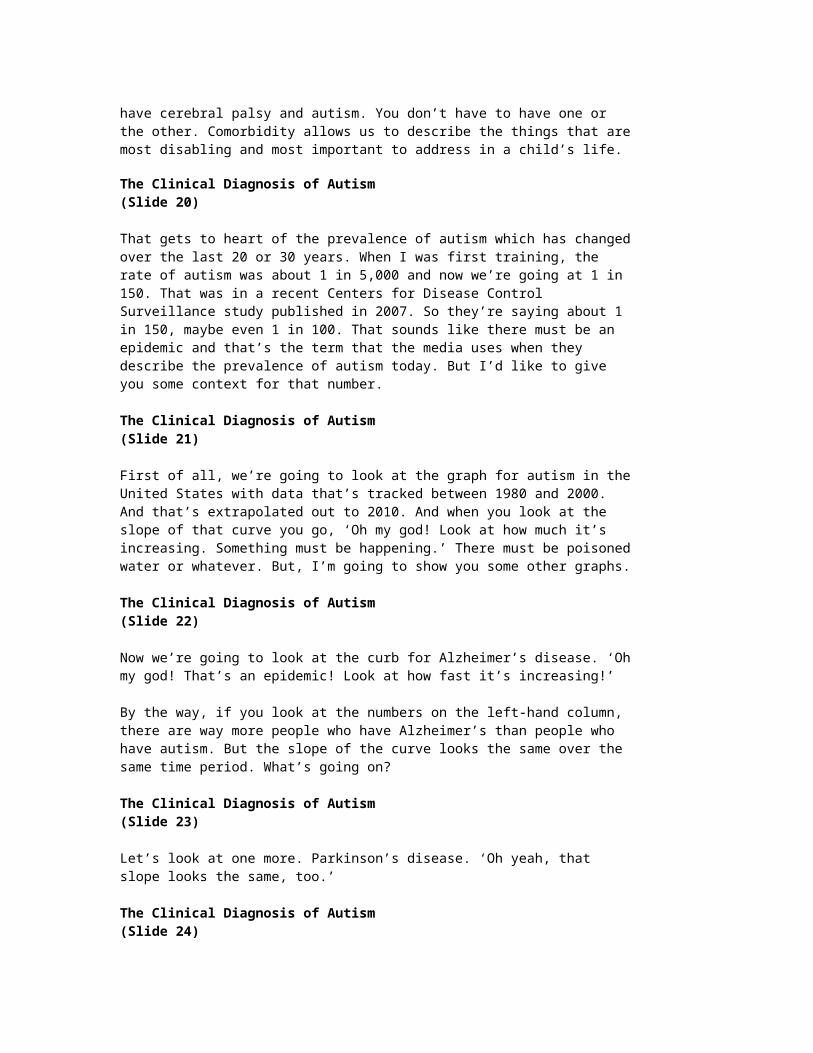
That gets to heart of the prevalence of autism which has changed over the last 20 or 30 years. When I was first training, the rate of autism was about 1 in 5,000 and now we’re going at 1 in 150. That was in a recent Centers for Disease Control Surveillance study published in 2007. So they’re saying about 1 in 150, maybe even 1 in 100. That sounds like there must be an epidemic and that’s the term that the media uses when they describe the prevalence of autism today. But I’d like to give you some context for that number.
The Clinical Diagnosis of Autism(Slide 21)
First of all, we’re going to look at the graph for autism in the United States with data that’s tracked between 1980 and 2000. And that’s extrapolated out to 2010. And when you look at the slope of that curve you go, ‘Oh my god! Look at how much it’s increasing. Something must be happening.’ There must be poisoned water or whatever. But, I’m going to show you some other graphs.
The Clinical Diagnosis of Autism(Slide 22)
Now we’re going to look at the curb for Alzheimer’s disease. ‘Oh my god! That’s an epidemic! Look at how fast it’s increasing!’
By the way, if you look at the numbers on the left-hand column, there are way more people who have Alzheimer’s than people who have autism. But the slope of the curve looks the same over the same time period. What’s going on?
The Clinical Diagnosis of Autism(Slide 23)
Let’s look at one more. Parkinson’s disease. ‘Oh yeah, that slope looks the same, too.’
The Clinical Diagnosis of Autism(Slide 24)
And, finally my favorite because it’s so unexpected is traumatic brain injury. That slope is as steep as any of the others and what’s happened in all of these conditions is that the more we study something, the broader we make our understanding of it and the more mildly affected people we include.

The Clinical Diagnosis of Autism(Slide 25)So for traumatic brain injury, when I was training just before that data was collected, you had to pretty much be in a coma in an intensive care unit and have severe brain injury when you came out before anyone would count you. And now, if anybody in the audience has ever been knocked unconscious in a sporting event or by a kitchen cabinet, you have a traumatic brain injury and they’re counting those.
Unit 3 – Historical Perspectives and Prevalence
Historical Perspectives and Prevalence(Slide 26)
I’m going to give you a brief history about the diagnosis of autism and then give you a little insight into the things that have changed for me particularly. But if you’re a parent in 1600 in England or Ireland and you had an 18-month-old who stopped talking and began to act strangely, that’s what changelings were. You would say the fairies took them and left this changeling child in their place. That’s how people understood this. It wasn’t until 1943 and 1944 when Leo Kanner and Hans Asperger described within four months of each other the condition we understand to be autism now, that we actually knew there was a diagnosable condition.
Between the ‘40s and mid ‘70s that we were ruled by understanding behavioral disorders by Freudian psychoanalytic theory and we just didn’t have any other constructs. And so the theory at that point was that autism was caused by mothers who were ‘refrigerator mothers’. They were cold and withdrawn and therefore their child withdrew. It wasn’t until sort of the ‘70s to ‘80s that we began to understand brain development and what was really happening. We started to notice. Well, people started to notice that children with autism, 30% of them had seizures and 75% might have a co-existing mental retardation. So ‘ Oh, this is a neurodevelopmental disorder.
And so the whole shift came away from blaming mothers ‘ which was the right thing to do, move away from that ‘ to understanding autism as a neurodevelopmental problem in brain development. It wasn’t until 1980 that the term PDD was introduced and it wasn’t until 1994 that we were able to use the term Asperger syndrome as a diagnosis. In the 2000s people have been focusing more on this very subtle lack of social reciprocity that may be present in ‘ it is present in kids with autism, but it may not be present just in kids with autism.
So we don’t know that.
Historical Perspectives and Prevalence(Slide 27)
And to parallel that, when I was training in the 1970s, I was told at my fellowship that I would know of a child who had autism if I felt a chill go up my spine when I saw them and having never felt that, I never diagnosed it.’ It was really rare.’ And in the 1980s, if a child fell below 70 in an IQ score, we would say they had mental retardation yet we know that your child knows all of the states and the capitals; but that’s just a splinter skill.’ And that’s how we would say your child has mental retardation and some splinter skills. And now we would say your child has an autistic spectrum disorder.
In the ‘90s and 2003, really have begun to focus on the subtleties of social interaction with people and how children are able to have a give and take with you in a relationship and once we

started focusing on that, the numbers really started to climb.’ In Wisconsin, between 2000 and 2005, we have had something called the autism waiver program that I’ll talk about later.’ But people were coming for diagnosis, for services, and I wanted to diagnose to get these kids’ services because it seemed like the best possible option for them.’ However, now that we’re in 2009, I have so many people who know about autism that parents are coming in with all the jargon associated with autism.
‘My child doesn’t have joint attention.’ Or ‘My child doesn’t do the’’ And they are all autism characteristic, but I’m finding that more and more of those kids may have a global delay.’ They may have a language disorder.’ They may not have an autistic spectrum disorder.’ So I think we’ve kind of maxed out on the number of kids that we would diagnose.’ And now the pendulum swinging a little bit back the other way because this is how our understanding develops.’
Historical Perspectives and Prevalence(Slide 28)
The trick with all behavioral diagnoses is that you have to have a convergence of three stories at the same moment.’ So I get 60 or 90 minutes with a new family, and in that short period of time, in that slice of a child’s life, the child has to be willing or able to show certain characteristics.
The parents have to be willing or able to tell me a story that fits with that condition.’ And the clinician or diagnostician has to be willing and able to see what is in front of them and all those three things have to come together, and that ‘ How the child presents changes overtime as the child gets older. So given all those variables, there’s really not much surprise why it’s so hard to know who has autism and who doesn’t and how can we agreed and it’s really still quite an area where people in the same field don’t use the same ‘ You can’t come to the same conclusions all the time.
Historical Perspectives and Prevalence(Slide 29)
When I’m training pediatricians and pediatric residents, I really ask them to treat developmental and behavioral questions from parents as they would any other concern.’ It’s a big issue for us because development is the only area in which a parent can go into a pediatrician and say, ‘My 2-year-old isn’t talking,’ and have the pediatrician just say, ‘Oh, you know, lots of 2-year-olds don’t talk’ without really investigating it. So I’m really working to try to get pediatric residents to learn to approach this developmental question the same way they would any other question.
For example, if a mother came in and said, ‘My child looks pale to me,’ we wouldn’t say, ‘Well, you live in Wisconsin.’ Lots of kids look pale.’ We wouldn’t do that. We would take a history.’ We do an exam. We might get some laboratory studies. We would collect data and then say, ‘You know, your child is normal.’ But we don’t that for development and it’s a work in progress to get pediatricians to recognize that this isn’t any different.
Historical Perspectives and Prevalence(Slide 30)
The American Academy of Pediatrics, which is my professional organization, is urging and has recommended that all pediatricians screen for autism at 18 and 24 months using a standardized autism screener.’ The one I’m going to mention here is the most widely known as the M Chat, which is the modified check list for autism in toddlers, 23 yes/no questions. It’s really very easy to administer. And a few offices in the area are using it. I actually think 18 and 24 months is
late, and I’ll explain why in the section on early identification.
But it turns out that only 23% of pediatric offices use any kind of developmental screener. So it’s hard to know if this recommendation is actually going to take or not.’
Historical Perspectives and Prevalence(Slide 31)
If you want to look up their reference, I’ve given you the reference for the M Chat on the next page ‘ next slide.’ If you want to look up the reference for the M Chat I’ve given you the authors on this slide. I actually think 18 and 24 months is late. I would really like to get in and provide intervention for children before that.
Historical Perspectives and Prevalence(Slide 32)
I like the Filipec criteria.’Pauline Filipec is the pediatric neurologist who headed a large consortium of professional organizations in 1999 and came up with a list of absolute indicators for an autism evaluation.
And I like her criteria because they address earlier concerns.’ So if a child doesn’t have any single meaningful word by 16 months of age, that’s a reason for referral. That means a child may say ‘mama’ but if they don’t use ‘mama’ to call their mom to come to them or say ‘mama’ when they see them, it’s not meaningful. It’s not communicative and no single meaningful word at 16 months is a reason for referral.’ No communicative gestures by 12 months.’ A 12-month-old should be able to reach their arms up to get picked up. They should be waving bye-bye. They should be pointing with an index finger to indicate interest. Those are gestures.
If a child does not have any communicative gestures by 12 months, that’s a reason for referral.’ No flexible two-word phrases by two years. And that means that thing like ‘all done’ and ‘thank you’ aren’t two words, they’re really one-word units because you never use thank without you and you never use all without done. So they may flexibly use two-word combinations such as ‘mommy outside,’ ‘more juice,’ ‘go bye-bye’.’ So they’re combining two words together flexibly. And any loss of any social or language skill at any age is important because about a third of children with autism will present with language regression.
Unit 4 – Clinical Diagnostic Practices
Clinical Diagnostic Practices(Slide 33)
One of the things if any of you are going to be clinicians in your work and you’re going to be interacting with parents and young children, there are a few techniques that I’ve learned that are very quick to do and that gives you a tremendous amount of information.’ I learned this partly through experience and partly from this test called ‘The Autism Diagnostic Observation Schedule’ or ADAS which was developed by Cathy Lord and her coworkers and is just a brilliantly designed test to elicit autistic behaviors. For example, on the ADAS you get some bubbles and you can get a bubble gun or you can get just a bubble wand and a bottle and you blow bubbles for the kids.’ 99% of kids love bubbles.
I have had kids with autism who are terrified of them and do not want them to pop them on their skin, and so ‘ a few kids, but almost all kids universally love bubbles especially around two or three. And so you’re blowing bubbles. They see you blowing bubbles and then you stop and you hold the wand and you hold the bubbles and you wait for them to request. And these

may be kids who have been taught the sign ‘more’ over and over again by Birth to Three people, or they have the word ‘more’. But when you set up a situation where they need to use the word to request, they walk away. Just like, ‘All right. I can’t any more. I’m just going to go somewhere else.’ It’s really telling.
The ADAS also taught me about conversation and how to use a statement which is what they call a conversational press, and not to facilitate the child answering. So often, like that ice cream example, ‘I like vanilla ice cream.’ Stop. Wait for the child to say something instead of what we usually do is, ‘I like vanilla ice cream. What do you like?’ And that might make that easy enough for the child with autism to answer, but if you just make a conversational statement and wait for a response, you’ll be surprised at how often kids on the spectrum just keep talking about whatever it was and ignore you completely.
The ADAS also uses picture books. Books without words to see how a child can tell a story from pictures and this is an ability that kicks in more around three for typically developing children. So I keep one simple picture book like ‘Brown Bear, Brown Bear’ and one more complicated picture book depending on where the child’s language skills are. But you can collect any tremendous language sample from kid by showing them pictures and trying to get them to tell you a story.
I’ll show you the puzzle on the next slide but I also want to mention the draw person test has been around forever since the time it was called the ‘draw a man’ test and then became politically incorrect. Good enough in Harris' Draw A Person test is you give a kid between three and eight years of age a blank piece of paper, a pencil, and you go, ‘Draw a person for me. Draw me a whole person,’ and just let them go. You don’t prompt them, you don’t do anything. You can score that and it gives you a beautiful snapshot of development that you can use to help understand whether some of those other characteristics are developmentally appropriate or not.
Clinical Diagnostic Practices(Slide 34)
Here’s the picture of the puzzle. One of the things I learned from getting this picture was that if you turn a puzzle upside down and scatter all the pieces will fall out. So this is just the empty puzzle. But what I do is instead of asking kids the labels for the puzzle ‘ Because kids with autism are very good with labels. They can go apple and train and trends. I ask them, which one do you eat? And you’d be surprised ‘ I mean, kids around 2-1/2 starts to be able to answer those simple function questions and by 3 they’ve got them. Which one do you eat is not a question they understood and it really gets the heart of the impairment in receptive language that many children with autism have.
Which one do you live in? Which one do you color with? Which one flies? They may not have that kind of language that their parents really think they have.’
Clinical Diagnostic Practices(Slide 35)
Another principle of interacting with children is that you can’t tell how a child is going to interact with you until your try. Oh sure ‘ Sometimes I walk in a room and the child is screaming and flapping and lining up all their toys and you go, ‘Oh yeah, I know what they have’ and it takes about one second. But a lot of times, I go in, the kids playing with toys, I talk to the parents and the kid looks fine in the corner until I go and sit down next to them and try to play with them.

And recently, I’ve had kids just scream at me. They were fine. I sit down next to them, they go, ‘Go away. Don’t touch me.’ Screaming.’ One girl sort of tried to bite me and just lunged at me.’ She was fine until I went to sit next to her. So another way that kids might react to have autism is that you come just next to them, you ask them a few questions. I’ve had kids pick up all the toys they were playing and just turned away from me so they didn’t have to deal with me. Kids with autism are not as interested in people as play partners. They are interested in doing what they want to do and are generally not so interested in adults who might want to play with them.
Oftentimes parents will say, ‘My child’s just shy.’ And I’ll say, ‘You know, shy looks really different.’ When I walk into a room with a shy kid, that shy kid gets up, they walk over to their parents, they run over to their parents, climb up on them and hide. And shy children look very different than autistic children.
Clinical Diagnostic Practices(Slide 36)
So to just summarize what are the parts of an autism diagnosis? What I tried to get done in my little bit of time is a careful developmental history. I will review any program information that I get and sometimes I don’t get it so I work with what I have, but I would like to review program information.
I observe the child while I’m talking to the parents. I try to interact with them with variable results. I go through the DSM IV criteria and administer a test like the ADAS and that is everything that goes into deciding whether a child has autism, PDD-NOS or Asperger syndrome. The other thing I try to do at the same time, which is really sometimes tricky, is to try to look for clues in the physical exam and the neurologic exam as to why a child might have autism. And sometimes I can find. You know, you have characteristics of this genetic syndrome or that syndrome or you have short stature or you have microcephaly. The other clues that might help us understand this.
And then I try to explain that process to the family and then I write a way too lengthy report that summarizes my thought processes because people need to know how you came to that conclusion. You can’t just walk into a room and say, ‘Well, your child has autism.’ But that doesn’t help anybody. Parents need to have been able to tell their story, be sure that somebody listen to them and appreciated their concerns and then explained what the next step will be.
Clinical Diagnostic Practices(Slide 37)
Unit 5 – Issues in Early Identification
Issues in Early Identification(Slide 38)
So now we’d like to talk about early diagnosis and I’m going to spend a fair amount of time because this is really the cutting edge of autism diagnostics and we are arguing amongst ourselves about how early is too early. Some people would like to move autism diagnostics down to a 12-month level and I think that’s just going to be hard.’ We know that if we diagnose a kid at age 2 that that diagnosis is stable for 2 or 4 or 6 years, but we don’t have any idea with the diagnosis at 1 for a lot of kids would be like.’ Sad to say that I haven’t done it. I have done it twice.’ One 12-month-old was the infant sibling of a child with autism and another 13-month-old whose parents were completely unprepared for any news like that.
So there are a lot of problems. So we are going to talk about what a good diagnosis is, problems

with an early diagnosis and then what’s really good about an early diagnosis.’
Issues in Early Identification(Slide 39)
A good diagnosis is reliable and we’re not great at that yet.’ Between clinician and clinician, we’re not always consistent on whether we think a child is on the spectrum or not.’ A good diagnosis has predictive validity.’ That means if you diagnose at age 2, is that stable overtime; and generally it is.’ A good diagnosis proves useful in determining treatment and we hope that leads to improve prognosis. And we have to remember that we’re talking about a diagnosis in this context, it’s really the behavioral diagnosis of autism that we’re talking about.
Issues in Early Identification(Slide 40)
So the problems with early, going much under 2 is that we don’t have a lot of information with pure interactions.’ We really don’t know a lot more to expect than parallel play in kids under 2.’ So they don’t have much opportunity, too.’ A lot of kids aren’t even in daycare and they have never been in a setting with other children.’ Parents and physicians and people likely to see any children may have a limited awareness of what the relevant symptoms are in a young child. What are we looking for? Most kids with autism are healthy. Most kids meet their major motor milestones, so they walk by a year. So all those things that would be red flags; otherwise, really aren’t there.
Issues in Early Identification(Slide 41)
And development screeners are imperfect and underutilized. We also don’t know whether early identification will lead to better family support. We don’t know whether all these intensive therapies that we’ve developed for kids over 3 are applicable to kids under 2. We don’t know how much therapy is enough, how much is too much, we don’t know what the most important skills are to teach, and we really don’t know what alters outcome with the thing that takes probably 20 or 25 years to figure out if you know other physicians again.’ People like me we don’t like to be wrong. So going much under 2 years is going to make us wrong more often. And we prefer not to do that.
Issues in Early Identification(Slide 42)
And we really don’t want to cause harm by prematurely labeling a child by irreparably altering that child’s parent relationship. We don’t want to provide therapy that’s going to waste somebody’s time, and we don’t want to decrease attention that’s given to other siblings. So we don’t want to cause harm by alerting a family to our concern. But if you were to look at for early signs of an autism spectrum disorder, here are some of the things that you would see even in infancy.’ That means the first year of life.
Issues in Early Identification(Slide 43)
Typically, you’ll see extremes of temperament. So these babies are really either passive, too good, never cry or extremely irritable.’ The kind of babies who parents say cries all the time and they mean all the time. They’re very rarely happy. Babies’ parent ‘ and when parents feel lack of connectedness to their baby, that’s a very important sign. They feel like their baby isn’t really locked on to who they are. That’s a concern. There is precautious labeling prior to useful

language. So I’ve had kids who can identify ‘ again, all the letter of the alphabet by 1 year of age, but don’t have a word for ‘mama’. They may have ‘ and this is the most common thing ‘ delayed cooing, babbling or meaningful words despite normal hearing and that’s the most common presentation as delayed speech.
And they may have repetitive or unusual behaviors even as early as 6 to 9 months of age. They may have some wrist turning behaviors or something that looks weird to a family member but nobody knows what to make of it.’
Unit 6 – Advantages in Early Identification
Advantages in Early Identification(Slide 44)
Tina Iyama-Kurtycz: I’m going to give you two references about the very early autism phenotype. There was an entire issue of the Journal of Autism and Developmental Disorders that was devoted to this topic. A lot of people are trying to study the infant siblings of children with autism because they have a higher likelihood to develop autism. And this journal reported the first nine cases that they had followed from four months of age and it turns out that some children don’t have eye contact or social connectedness or smiling. Some babies do, but they don’t then roll over on time or sit up on time. So none of the babies they reported actually had a clean developmental history.
There is ‘ A lot of studies are saying at least by 12 to 14 months they’re able to tell whether the infant sibling will go on to have autism. Sometimes it’s early as four months in some studies that have to do with whether baby shift their visual attention in a typical way for a 4-month-old.
Advantages in Early Identification(Slide 45)
So that’s some of the interesting research that’s going on and then the Wilkins article is just ‘ Matson and Wilkins is just a very foot ‘ feet on the ground, ‘We really shouldn’t do this before two years of age’ article.
Advantages in Early Identification(Slide 46)
So the bottom line for early diagnosis is that there isn’t any magic age at which all children with autism can be diagnosed.
However, unusual development can be addressed without a diagnosis from birth. Children are the product of their genes, their prenatal environment and the interaction of their nervous system with experience and this shapes their developing brains. If you take any child and place him or her in adverse life circumstances where poverty, hunger and indifference limit their potential, you can aggravate developmental vulnerabilities.’ Children with autism are born with neuroanatomical pathways that are already set on a different course.
Perhaps they have something to do with a special subset of neurons that can’t recognize and relate to imitation. Maybe certain areas of the brain aren’t connected right. But either way, babies don’t take in the same experience ‘you’re going to have autism’, don’t take in the same experiences and model their brains in the same way. But what we’re hoping is that if we can alter really early experiences, maybe we can alter that vulnerable phenotype and so that’s what people are working on.

I do want to pause, though, and say that there are some children that are so severely affected by their autism that the size of the biological problem is so huge that you can give them everything we know how to do from a very early age and you may not alter that course. Amy Klin from Yale reported, on a 15-month-old they diagnosed very early, they put her into every kind of intervention, all of Yale Autism Child Program you had to do and still, she got more and more autistic over the intervention time period and she had severe autism. So sometimes a child’s biological problem is just very large.
I saw a family recently where this was the case and they came in, they had purchased early intervention services, they had done all of the right things, they’ve worked really hard and they’ve worked hard for two and a half years and this little girl is still very autistic. And they wanted to know what are the therapies they needed to know. And it was like, ‘You know, you did every therapy and you did your very best.’ And that’s what parents really need to know in the long run is that they did everything they could do. They did their very best. They did everything that they knew to do at the time because that’s how in 20 years you can live with yourself as a parent.
Advantages in Early Identification(Slide 47)
All right. So let’s talk about what’s good about early diagnosis. I think, if we can identify infants and young children who are at risk for autism, then we can provide intervention right then. For example, a six-month-old who doesn’t make eye contact and has normal vision is surely at risk for some kind of developmental disability. And maybe if we could provide a way for them to notice the parent and make the parent try more often,’ maybe we can shift that. So we can show parents about what we know about teaching joint attention and social skills, how to use visual strategies and how to teach imitation and then we don’t have to make a diagnosis until two years of age. And that may be the direction that we’re headed in.
Advantages in Early Identification(Slide 49)
So what I would like to do is help parents change a child’s behavior that seems repetitive or it seems as if the child might not be getting anything out of that. So even though it might be cute initially ‘ when nine-month-old spin everything that they find, really what I tell parents is, ‘You know, I don’t think he’s getting anything out of that.’ Or if they open a door repetitively, ‘You know, I don’t think he’s learning anything from that, so let’s change it up a little bit.’ And so yesterday I told a dad whose little guy spun himself in circles, you know, like make a Ring Around the Rosie, make it into something that has social meaning.
And I think we might at least alter the experience that that baby’s brain has with the world.
Advantages in Early Identification(Slide 48)
Autism, as I’ve mentioned, there are a people who want to screen the entire population for autism. And it doesn’t really meet the criteria we’ve established for other disorders. If we want to screen large populations of people, like for hypertension or for cervical cancer or for hearing loss in newborns.’ Those diseases are disorders that need to meet these criteria. And for example, the disease must be clearly defined, and that’s a huge stumbling block in autism.
Prevalence estimates need to be known. We need to know whether we can identify presymptomatic people before you develop ‘ just as you develop hypertension or just when you

develop changes on your cervical smears. We need screening tools that are validated on the general population and we must know that treatment will alter the course. And I think for autism, the big stumbling blocks are the disease must be clearly defined as you’ve seen it isn’t. And that’s ‘ we should be able to identify presymptomatic people and we can’t.
We can’t, but I think our next best thing is to identify as early as possible.
Advantages in Early Identification(Slide 50)
A really wonderful review of communication development and intervention for children with autism is by Rebecca Langdon and I’ve given you that reference.
Advantages in Early Identification(Slide 51)
So what I recommended to clinicians is that they just don’t worry about early labels but embrace early intervention because I think we can make a difference in the lives of children.
Advantages in Early Identification(Slide 52)
Unit 7 – Etiology of Autism and Theoretical Background
Etiology of Autism and Theoretical Background(Slide 53)
Now we’re going to turn to the topic, ‘What causes autism?’
You’ve probably heard a lot of things that people think about causing autism on popular media. There is a lot that we know about what causes autism and the things that you hear and the things that we know may not be the same thing. So I thought it was worthwhile taking the time to tell you and just review for you how we know what we know.
Etiology of Autism and Theoretical Background(Slide 54)
And we know what we know based on the scientific method and that is, scientists make observations and organize them. They draw conclusions. They develop a hypothesis about what might be going on. They design an experiment to test the hypothesis. They gather data and if the data doesn’t fit they have to go back and revise the hypothesis and go at that again.
Etiology of Autism and Theoretical Background(Slide 55)
And so science is a very slow process. It’s an accretion like building coral reefs. It’s like a little bit of knowledge here and a little bit of knowledge and it adds to a greater, broader conceptual idea. I tell parents that, ‘You know, I have no truth about autism. All I have is this accumulated evidence.’ And science is like human endeavor, but it’s the best way we have of figuring out actual causes and effective treatments for people with autism and their families. And if we ran after some of these other wilder ideas that have no basis and are unconnected to the actual body of science, we’re going to waste a lot of time and energy and money. And I think the biggest crime is that we’re going to waste children’s time and they don’t have time to spare.

Etiology of Autism and Theoretical Background(Slide 56)
Another principle about thinking about cause is that just because something happens on one day and then something else happens on the next day doesn’t mean that one thing caused the other. And this comes up a lot because parents are starting to recognize social and communication delays in the second year of life, between 12 and 24 months. Oh my gosh, a whole lot of immunizations happened then. And so people in the media fuel this by giving voice to some of these activist parents who believes that their child was harmed by an immunization.
Well it happens that, yes 18 months is when kids get immunizations and it is right about that time that parents start to notice changes in their children compared to other kids. Before that, we don’t have as many standards for social and communication. And it’s a coincidence and it doesn’t mean that it’s causal.’ Having been around for 30 years, I know that 25 years ago people were sure that a completely different immunization that we gave at 18 months was the cause of autism and it turned out not to be.
We have countrywide data to show that immunizations do not cause autism. When thymerizol, the mercury-containing component of many vaccines, was taken out of all immunizations in Denmark in 1992, there was absolutely no change in the rate of autism. That means on a public health scale, that was massive.’ They completely changed the carrier for their vaccine. Nothing changed the rate of autism. So in that ‘ and there is the same kind of data from Japan and huge sections of the US.
Etiology of Autism and Theoretical Background(Slide 57)
Here’s what does not cause autism. Refrigerator mothers, immunizations or mercury poisoning, diet, immune deficiencies, GI problems or lack of oxygen. Carl Sagan noted a scientist once said, ‘Extraordinary claims require extraordinary evidence.’ If you’re going to claim something that goes against what everyone knows about a particular condition or stars or whatever it is, if you’re going to claim something completely widely different, you have to have a tremendous amount of evidence in order to prove your point and get that accepted. And none of these conditions has anything near credible evidence.
One of the things I heard a mother say at a parent group was that these doctors just don’t acknowledge how sick our children really are and our children are really sick and we just don’t recognize them. Well you know, I see children who are inpatients at the American Family Children’s Hospital. Those are sick children. Those children are not my patients with autism who look quite healthy, who are growing very well, who may be fussy eaters but they do not have any recurrent illnesses or any problems.
Etiology of Autism and Theoretical Background(Slide 58)
And in fact, this was studied by Rosen and his colleagues at Kaiser Permanente Primary Care Pediatric Office. They reviewed 21,000 controls and 400 children with autism spectrum disorders and the kids ‘ and I looked their office visits and the number of illnesses and the kids with autism spectrum disorders were actually healthier than the kids in the general population and that would match my clinical impression as well.
Etiology of Autism and Theoretical Background(Slide 59)

So what does cause autism?
We have some really strong clues that there are genetic underpinnings to the development of autism. If you are an identical twin and you have autism, the chances that your other identical twin will have autism to that degree is 60%. The chances that you’ll both be on the spectrum are 90%. So it’s not 100%. So there is that little 10% wiggle room for other things to be happening, but 90% of identical twins both have autism. If you’re a fraternal twin, which is genetically like being a sibling, you’re rate drops to what it is about for siblings, in the 5% to 10% range.
The numbers we gave the parents who say, ‘We have a child with autism. What’s the chance for a second child to have autism?’ It’s 8%. It might be 10% to 15% for speech and language problem, but in general 8% to 10% is a probably reasonable number. There’s also information about what’s called the broader autism phenotype. And that is the idea that people ‘ parents or individuals who have autism ‘ have first-degree relatives, parents or siblings, who also have some of those characteristics.
Etiology of Autism and Theoretical Background(Slide 60)
And I learned of this from a wonderful pediatric neuropsychologist that I worked with who always said to me, ‘Oh, you know, apples don’t fall far from apple trees.’ And this was actually a great way to interview the families.
Etiology of Autism and Theoretical Background(Slide 61)
I sometimes ask them, ‘Do either of your parents tell you that this was just the way you were when you were a child?’ And I had a little three-year-old girl whose parents really did not believe the diagnosis until they started looking at mom’s history. And mother was treated as a child prodigy, a genius who played violin, I think. She was a musician and she also read ‘ she said, ‘You know, I read, but I didn’t really ever have any friends.’ And they went back and looked at that and was like, ‘Oh, maybe, you know, our little girl does have some of those characteristics.’
Etiology of Autism and Theoretical Background(Slide 62)
This was most beautifully clarified by Joe Piven in 1997. It was an old study, but it really illustrated the differences that parents with children with autism are from parents who have children with another kind of disability. He looked at the language sample of parents who had children with autism and compared the language to parents who have a child with Down syndrome. And on the slide you’ll get to see that there were 46 parents of kids with autism, 55 parents of kids with Down syndrome, and their language characteristics were very different. And this really does support kind of my clinical impression that getting a history from parents who have a child with autism is sometimes very difficult.
They may be too detailed or not detailed enough and they may fail to reference like they will say, ‘Well, Jodie told me this.’ And I don’t have any idea who Jodie is and they don’t know to tell me. Their accounts may be disorganized, they may fail to clarify and they may have language melody or rhythm problems similar to their children. So I think this broader autism phenotype concept is also important for looking at genetic underpinnings.
Etiology of Autism and Theoretical Background(Slide 63)

Now in this slide, these are few of the single genes or chromosomal disorders that caused autism. Tuberous sclerosis, Smith-Magenis, Rett syndrome ‘ These are all ‘ There are a lot of names, a lot of doctors’ names attached to syndrome that we know the cause of now. And we know that these children have a high risk of either mental retardation or autism or both. There are dozens of them and every once in a while you’ll read in the paper, ‘Oh, there’s a new gene for autism and they found that on chromosome 16 or 15 or whatever.’ And when you look at it - Those account for about 1% of cases.
So almost every chromosome has an autism hotspot. There are probably more than one, these are probably multiple genes that interact together and may interact with the environment to produce this autistic development.’ There’s a new test I wanted you to be aware of because in the past we’ve always done the test called chromosomes, we looked at and studied chromosomes and we look for fragile X syndrome which is the common cause of autistic development. And a lot of times those tests were negative. And we tell parents, ‘You know, we did everything we could.’
Etiology of Autism and Theoretical Background(Slide 64)
Well, there’s a new test that’s really changing how we look at these kids diagnostically and it’s called array comparative genoic hybridization or array CGH and it’s like having a Hubble telescope for the chromosomes. It’s like having this really powerful instrument to look at very small pieces of the chromosome that could be deleted or missing or duplicated. And any imbalance in chromosome gene number or copies can lead to developmental delays or autistic development. So we’re finding kids who we thought wouldn’t have a syndrome, but we’re identifying on array some abnormalities that we’ve never identified before.
Etiology of Autism and Theoretical Background(Slide 65)
So I think this is giving another 10% or 20% of parents an answer to why their child has a problem and kids, no matter how old they are, if they haven’t had this, they need to go back and probably see a medical geneticist to get that testing done.’ There are also ‘ After the genes are playing out their roles, there are also neurodevelopmental theories and you may have heard about theory of mind which has to do with the fact that kids with autism have difficulty seeing the world from another person’s point of view. So they have trouble with it, sort of understanding what another person might think. That’s theory of mind.
Etiology of Autism and Theoretical Background(Slide 66)
A few years ago, people were talking a lot about ‘broken mirror neurons’ and that is the ability ‘ The neurons that are responsible for our ability to map ourselves unto other people. If someone who’s watching a stage show and somebody was going to hit an actor with a sword and their right leg, the audience says, ‘Right leg pulls back’ because we know something’s going to happen. Children with autism tend not to do that. They tend not to understand that what they see other people do could happen to them or that they could do.
And this is why I think that kids with autism often have trouble learning sign language because they see their parents do this for more. And what they end up doing is grabbing their parents’ hands and putting it together because they know what they saw but they don’t know that they can do it and some people have wondered about ‘mirror neurons’ as responsible for this. But right now, I think probably the most attention is going to this idea of disconnection ‘ that areas

of the brain develop but they’re not connected to each other appropriately.
Etiology of Autism and Theoretical Background(Slide 67)
It’s not certainly proven, but the evidence is accumulating. That this disconnection between brain areas might lead to autistic development. And this is summarized in an article by Muller, The Study of Autism as a Distributed Disorder.
Etiology of Autism and Theoretical Background(Slide 68)
Probably, important developmental pathways are affected early in the development when you have autism. And as development progresses, there’s sort of an exponential effect on the rest of the brain because these new systems needed the old systems to be in place before new things could happen and if you miss something early, then it kind of multiplies in effect as development goes on.
When you go to a neurologist, there are three questions they ask, and one is, ‘Is this is a progressive or a static problem?’ And in autism it’s a static problem.’ There’s nothing going on in the brain that makes the child worse overtime. There are over 600 neurodegenerative diseases but autism isn’t one of them. So it’s a static problem. Then neurologists want to know, ‘Is this peripheral nervous system or central nervous system?’ And of course, autism is a developmental problem with brain development, so it’s a central problem.
And then once you get to the brain, neurologists want to know, ‘Is this localized or generalized?’ So they want to know is that localized to one area of the brain or is it diffuse and affects all areas of the brain and the answer is that for autism it is a generalized disorder. So it’s static, central and generalized.
Etiology of Autism and Theoretical Background(Slide 69)
And this was the idea of disconnection between areas of the brain was best illustrated by a dad, probably 20 years ago, who said to me, ‘My son has islands of intelligence but they don’t seem to be connected to each other.’
And that was before we knew anything about disconnection or how that word. He completely and succinctly said what every parent feels, like there are things that work in that brain but it’s not useful. The child can’t use that in everyday life. I had a little guy this past year who ‘ you know those little pin, where all those pins are hanging down, you put your hand up and you can see your handprint. Well, if parents took any state of the union, any country in Europe or Asia and put that puzzle piece up into the pins and he saw the outline. He could name the state or country.
And he was three and he didn’t have a word for ‘mama’ but he could go ‘New Hampshire,’ you know, ‘Texas’. And it was an amazing ability but it wasn’t connected and it wasn’t something he could use in other ways. What this also means is that there isn’t some normal child hiding underneath a lot of the autistic behaviors and that’s been something that people have felt, too. Just because a child has a spike area like state recognition or ABC recognition, it doesn’t generalize to generally general intelligence. And that’s a hard thing for parents to get but it is now consistent of what we’re understanding about these connections.
Etiology of Autism and Theoretical Background

(Slide 70)
For example, in autism, people are finding that the corpus collosum, which is the band of neurons that connects one side of the brain to the other side of the brain, that band is smaller in kids with autism. So there is not as much connection again. There’s also increased brain tissue, gray mater and white mater. There’s increased amounts in kids with autism. And that leads to some of these young kids having very large head sizes for their body size early in life. And so these are kids with macrocephaly or big heads because their brains have too many cells.
In normal development, what babies do is they are all born with a number of neurons they’re going to have; and then with experience, they prune down those connections. They make certain pathways more efficient and they prune down the number of cells and the number of connections that are present such that there’s a normal growth of the brain. And in autism, we’re thinking that there isn’t this normal pruning that goes on and that experience doesn’t make certain pathways more efficient; and therefore, maybe lots of pathways are open but it’s not an effective connection that leads to typical development.
Etiology of Autism and Theoretical Background(Slide 71)
So this is actually being worked on locally in Madison. One of our pediatric neurologists, David Chiu, is doing advanced scanning techniques on kids with autism and looking at this connectivity issue.’ It’s really ‘ It’s all calculus, I don’t understand these papers, but he explained it to me and it looks pretty promising and it does support what other people are finding in other major centers ‘ that there is just a lack of connection and inappropriate connections between areas of the brain and autism. So I think that’s going to be promising.
Etiology of Autism and Theoretical Background(Slide 72-74)
Unit 8 – Effective Interventions
Effective Interventions(Slide 75)
Now, I’d like to turn our attention to what we know about effective interventions in autism.
Effective Interventions(Slide 76)
And whether we like to acknowledge it or not, if we look at the evidence that we have, it is still a true statement that the only known effective intervention for autism is intensive behavioral therapy which is also known as Lovaaser Applied Behavioral Analysis.’ I have to tell you the story of this because Ivar Lovaas, who is a psychology professor at UCLA, he changed how we thought about autism.
Autism, before his paper came out, was hopeless. We would say, ‘You know, we’re really sorry.’ And actually it wasn’t mean at the time, but is a little bit before me. But you would say, ‘This is hopeless. There isn’t anything we can do. Your child has autism. I’m sorry, you know. You did the best you can.’ But Lovaas took 40 kids and he randomized them. So it’s a randomized group of children with autism, 20 ended up being in the control group who had whatever special education standards were at the time. That’s what they got. And then he took another 20 kids and he provided 40 hours per week of intensive behavioral ‘ positive stimulus, negative stimulus, and really intensively worked on these kids and half of those kids, 10 or 11,

had significant improvement to the point that they were mainstreamed into first and second grade classes.
And I remember, our child psychiatrist at the time told me, she said, ‘This changes everything. This means we’re not doing enough for kids with autism.’ And it was a sea change. It was a very landmark and important article. Now, it turns out that that was one of the best studies ever done. And it’s hard to prove that other things worked. But we have some information about psychotropic medication and it’s certainly not my first go-to thing especially with the young children. But I’ll give you an idea of the scope of how much it’s being used.
Effective Interventions(Slide 80)
And that is there is the University of Pennsylvania study that looked at over 60,000 children with an autism spectrum disorder diagnosis.
56% were on at least one medication, 20% were on three or more meds, 18% of kids under two were on medications. And fewer intercity kids because of lack of access to resources where psychiatrists were on medication. I mean, it’s a huge, huge number of people attempting to modify autism with medications.
Effective Interventions(Slide 81)
While there is one medication that is approved for irritability in autism and that is risperidone and Risperdal. It’s FDA-approved for autism. There are randomized controlled trials that showed that it’s better than placebo, that it modified symptoms in 75% of kids compared to 30% of placebo kids.
It has significant side effects of weight gain and sleepiness, sometimes extra uncontrollable involuntary movements. So it’s not risk free, but there is a roller for that in some kids who have autism and really irritable, over-reactive kind of states. But I don’t think I’ve ever used it in kids, 2 and under, and I think that’s probably a misreading of what is needed. But it’s really hard to evaluate effectiveness of treatments in autism and that’s because no matter what you do to a child who has autism, parents think they see an improvement.
Effective Interventions(Slide 78)
So we have studies, randomized controlled studies of medications like something called secretin which is very popular in the 1990s. People thought maybe this was going to help kids. Well, it turns out that when you do that randomized controlled trial and some kids get an injection of saline and some kids get an injection of the secretin, that parents whose kids got placebo actually thought their kid did better behaviorally afterwards than the kids who actually got the medications or the study drug.
And not only that, but once the parents were told that their kid got placebo and didn’t get the drug, parents still wanted the medication because they still had that belief that that was going to make a difference. This same kind of study was conducted in adults with developmental disabilities and the beautiful ‘ This is like one of my favorite studies in Lancet in 2008. And that is they randomized these people in supported living environments to either get a psychotropic medication or placebo, and depending on what the caretaker thought they got, the caretakers thought that their person or consumer was much better behaviorally.

Effective Interventions(Slide 79)
And placebo equaled drug treatment. So there was no difference, really, but just being told that something might help was helpful. It matches my clinical impression that people who prescribe psychotropic medications really easily often don’t fully investigate the cause of a disruptive behavior before turning to medications. Really, there are a lot of reasons. I saw ‘ OK, I have to tell you the story.’ I saw a kid yesterday. Seem like I saw a lot of kids yesterday, but I did. A 12-year-old boy that I had seen five years ago when he was seven. I didn’t see this family for five years. The mother came back, frantic. He was on five psychotropic meds. He had had three psych hospitalizations and everyone knew that his IQ was 48.
And so mother brought me his Math homework that he was supposed to be ‘ Sheets and sheets of double digit addition and subtraction problem and they said he has to do this and they said, ‘Well, we don’t care if he uses a calculator, but he has to finish this and if he didn’t finish them’’ They put him in like a timeout room without ‘ and he would become panicky and it’s because he was really a three- to four-year-old, cognitively. He would have hysterical disruptive behaviors and they would say, ‘Well, he’s a behavioral problem, you have to take him home.’
And so right now, he’s only going to school two hours ‘ I mean, this is foul. He’ll only be going to school two hours a day and they’re expecting him to finish his Math homework and when I gave him that puzzle that I just showed you ‘ and I just said, ‘So how many puzzle pieces are there?’ And he couldn’t count past five objects. So his number concept was at five, and they were giving him problems like 30 minus 30 equals. And it’s like ‘ I would have a tantrum, too.
And what happens whenever there is a gap between adult expectations and a child’s ability level, and that gap is significant, that child’s going to fill in that gap with behaviors. What else can they do? You don’t believe them that they can’t do this, so they’re just going to act out. And then what happens when they act out? They go to see somebody to get medications. And then that medication has side effects. And so this kid was wrenching through the house at night and looking for food because he was starving. ‘Well, he was on Seroquel.’ I said, ‘You know, the Seroquel’’ The mother said, ‘Well, he’s obsessed with food.’ And it was like, ‘No, he’s on Seroquel.’ And then she said, ‘Well, he’s tachycardic. His heart rate is always racing. He’s on stimulants.’
And so he had side effects plus people were not addressing his developmental abilities and if you don’t ‘ What he was doing was building failure upon failure upon failure. And he was the sweetest little boy. He came over to his mother. We started crying while we were talking, and he came over to her. He looked at her and he said, ‘Mom, are you sad?’ And she said yes, she was sad, and he came over to her and he gave her a hug and he said, ‘It’s OK. I love you.’ And it was like ‘ This kid is fine, if people would just adjust their expectations. And so we’re working on that. But I think that’s what triggers a lot of these medication trials without adequate investigation.
Effective Interventions(Slide 82)
So other treatments are what I’m going to call fad treatments, you might call complimentary and alternative treatments. They come and go and they come back and they never change the outcome. That’s a different talk and I’m going to be talking about complimentary and alternative interventions in autism in another segment.
Effective Interventions(Slide 83)

But, the bottom line is there’s no really one right way for all children. I think parents should have some options for their kids. They know their kid the best and better than anyone else and they need to work with people who have therapeutic interventions to offer that are reasonable and plausible.
Effective Interventions(Slide 77)
And I tried to help parents understand that there are interventions with both theoretical and evidence-based support. And these are better than interventions without either. So I use the term plausible therapies and implausible therapies. And I try to stir parents toward plausible therapies even if we don’t have a lot of data because the implausible ones are a waste of a child’s time.
Unit 9 – Services and Outcomes
Services and Outcomes(Slide 84)
I’m going to spend a few minutes on autism specific services namely, the early intervention, early intensive behavioral intervention, and I kind of titled the section, ‘The Myth of Autism Specific Services.
Services and Outcomes(Slide 85)
It’s hard to understand why someone working with your child 40 hours a week wouldn’t be helpful regardless of what was wrong with your child. Even for children with language delays, if somebody even spent 10 hours a week with them ‘ It’s not rocket science.
Services and Outcomes(Slide 86)
They would be better, but there is a belief that’s driven how services are provided in Wisconsin that only if you have an autistic spectrum disorder will you benefit from this intensive intervention. Right now, the state has supported through medical assistance dollars, about 200 or so families for up to three years to receive this intensive intervention. So what’s happened is this becomes a backlog of kids waiting for services. So now if a child gets a diagnosis at two, it was taking until they were four to get the kind of intensive services. No, it’s not that they weren’t getting any services.
Services and Outcomes(Slide 87)
I mean, early childhood programming is not nothing. I mean it’s certainly ‘ It’s positive and helpful and plausible, but it wasn’t with parents who were told they should seek. So what happened recently in Wisconsin that our governor signed a legislation that’s going to require Wisconsin-based insurance companies to cover autism interventions. We don’t know which kinds or how many or whether it covers ‘ Just Lovaas-type therapy or if it’s going to cover other kinds as well. But that’s going to relieve our backlog in Wisconsin, but every state has different sets of rules and regulations about these things.
What we really need is we need more studies to demonstrate the effectiveness of things like

parent training programs. I think if we could train parents on how to do these things, that they can incorporate this into their child’s everyday life and it could give them skills for the child’s lifetimes. Not only would it be probably less expensive and we could get to more people, but we could equip parents with what they need to know for many years instead of three.
And so there may be other ways to get to the right answer, but you know, they’re probably in this economy, it’s not going to happen rapidly. And that plays right into the whole questions of, ‘What happens to kids with autism? What are their outcomes?’ And we have to realize that what happens to kids with autism is partly what’s happening to us as a larger society. So our economy is better, unemployment’s high, it’s high for everyone and it’s going to be, I think, then higher people with developmental disabilities.
Services and Outcomes(Slide 88)
Services and Outcomes(Slide 89)
County-funded programs to support adults in the workplace and in living situations are getting cut back.’ There are people that are being forced back into group living and sheltered workshops, things that we thought we had gone past already and progressed beyond. But without any money, no program is going to be able to do what we know we can do for people. So outcome is going to be ‘ outcome studies are going to be affected about what’s happening in the larger society as a whole.
Services and Outcomes(Slide 90)
There have been several good long-term outcome studies. Christopher Gilberg is a long-time autism researcher who has done one with kids with birth dates as recently as the 1980s. And even for those kids whom you think that was - You know, only about 25 years ago. Even for those kids with required special education and therapy service and ‘ Their outcome, if you have average intelligence, only about 10% of that group, autism and average intelligence, had a good or fair outcome. I think it’s really ‘ outcome in autism is really impeded by the social skill issue.
Services and Outcomes(Slide 91)
And so that comes to my other outcome principle, and that is ‘ I hope this doesn’t sound rude, but being right isn’t as useful as being social. And I think I see that all the time with kids who have the IQ to do college or to do ‘ you know, whatever it is they want. But their social skill deficits are such that it makes it hard for other people to work with. They don’t understand other people’s point of view. It’s very hard for them to be as successful as a child with the same IQ. So social skills are probably our best predictor of adult happiness, at least, if not success.
Services and Outcomes(Slide 92)
Once in a while, for outcome, a child will fall off the autism spectrum entirely. One study was 1 in 30 kids, and another study 1 in 88 kids. In my own practice I’ve removed the diagnosis twice and all the kids that I’ve seen ‘ I just think, ‘You know, there’s nothing autistic about your development.’ And they’ve just outgrown it. One of those kids had a lot of appropriate intensive intervention. The other kid had a really wonderful family and maybe not as intensive intervention, but just moved away from autistic concerns. So what happens?

Debra Fine has done a study of kids who have had the intensive intervention and now are seven, eight, nine years old. And some of these kids are looking like they have trouble with executive function, that is organizing, planning and executing activities of daily life. So they’re looking more like they have attention deficit hyperactivity disorder than an autistic spectrum disorder and they don’t have cognitive delays. But they’re not quite clean. They’re not coming. They’re not completely living behind developmental concerns.
Services and Outcomes(Slide 93)
In the end, though, every child is a complex being ‘ a mix of strengths and weaknesses, and we all have the same hopes for our children. We want them to have a place to live in the community. We want them to have a job that they like doing. We want them to have friends and family who will support them and enjoy being with them. And we hope that everyone will see the unique value that each person brings to the world which gives us hope for them, sometimes in spite of the evidence. Thank you very much.
Conclusion(Slide 94)